

Sir,
Uveitis is a rare adverse event of vaccination with a low incidence rate as about 10.5 per 100,000.[1] Vogt-Koyanagi-Harada Syndrome is a very rare adverse event of vaccination, and there is only one case report in worldwide.[2] We recently experienced a case of Vogt-Koyanagi-Harada Syndrome following vaccination of influenza, thus herein report the case.
A 52-year-old woman presented to our institution with bilateral red eyes and associated decrease in vision. There was no significant ocular or medical history. However, she had received the influenza vaccination 1 month previously. There was no history of trauma, and the presence of tinnitus was noted on review of the systems. On ocular examination, her best-corrected visual acuities were 20/30 (right) and 20/100 (left). Intraocular pressure was 15 mmHg bilaterally. She never suffered from uveitis previously. The anterior chamber revealed 2+ cells in the both eyes. The fundus appearances demonstrated multifocal serous retinal detachments, which were further confirmed with optical coherence tomography [Fig. 1]. Fluorescein angiography showed multiple hyperfluorescent spots [Fig. 2]. Laboratory examination showed that both IgM and IgG of cytomegalovirus (CMV), Epstein-Barr virus (EBV), and herpes simplex virus (HSV) were all negative in the serologic evaluation. Systemic steroid therapy was initiated promptly with intravenous methylprednisolone followed by systemic oral corticosteroids (1 mg/kg). Two months after treatment, anterior chamber got clear, and subretinal fluid disappeared. Her visual acuities were 20/20 (right) and 20/25 (left).
Figure 1.
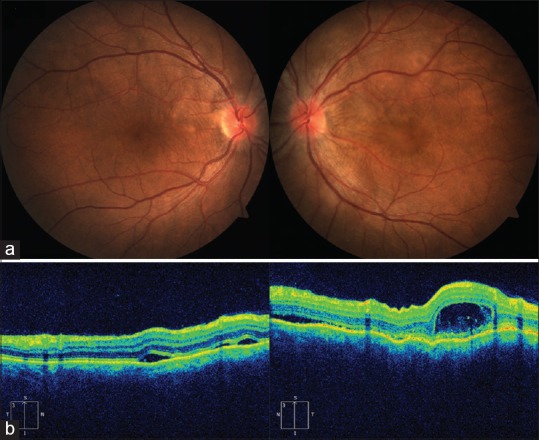
Fundus photographs showing bilateral multiple serous retinal detachments (a). Optical coherence tomography demonstrates serous retinal detachment in the both eyes (b)
Figure 2.
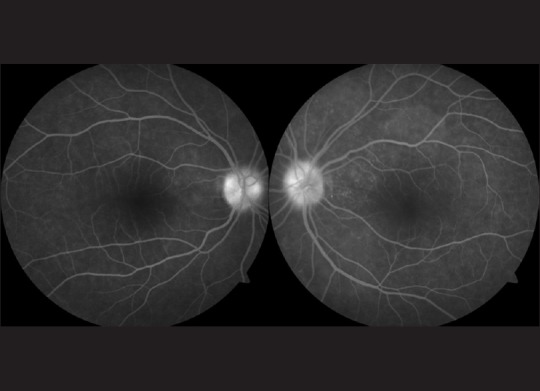
Fluorescein angiography showing multiple hyperfluorescent spots
This case is unusual in its etiology and presentation, with the development of Vogt-Koyanagi-Harada Syndrome in a woman who had received the influenza vaccination 1 month previously and the presentation of the syndrome with bilateral serous retinal detachments. That the negative finding of IgM and IgG of CMV, EBV, and HSV in the serum of a patient, and the effective use of systemic use of steroid, strongly suggested that the mechanism of uveitis and serous retinal detachments of the patient should be an autoimmune response rather than infectious. We encourage ophthalmologists, rheumatologists, and uveitis specialists to consider influenza vaccine as a cause of Vogt-Koyanagi-Harada Syndrome if the vaccine has been recently administered.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Klein NP, Ray P, Carpenter D, Hansen J, Lewis E, Fireman B, et al. Rates of autoimmune diseases in Kaiser Permanente for use in vaccine adverse event safety studies. Vaccine. 2010;28:1062–8. doi: 10.1016/j.vaccine.2009.10.115. [DOI] [PubMed] [Google Scholar]
- 2.Gallagher MJ, Yilmaz T, Foster CS. Vogt-Koyanagi-Harada Syndrome associated with bilateral serous macular detachments responsive to immunomodulatory therapy. Ophthalmic Surg Lasers Imaging. 2009;40:345–7. doi: 10.3928/15428877-20090430-25. [DOI] [PubMed] [Google Scholar]