

Abstract
The 2006 National Institutes of Health (NIH) Consensus paper presented recommendations by the Ancillary Therapy and Supportive Care Working Group to support clinical research trials in chronic graft-versus-host disease (GVHD). Topics covered in that inaugural effort included the prevention and management of infections and common complications of chronic GVHD, as well as recommendations for patient education and appropriate follow-up. Given the new literature that has emerged during the past 8 years, we made further organ-specific refinements to these guidelines. Minimum frequencies are suggested for monitoring key parameters relevant to chronic GVHD during systemic immunosuppressive therapy and, thereafter, referral to existing late effects consensus guidelines is advised. Using the framework of the prior consensus, the 2014 NIH recommendations are organized by organ or other relevant systems and graded according to the strength and quality of supporting evidence.
Keywords: Chronic graft-versus-host disease, Allogeneic hematopoietic cell transplantation, Supportive care, Consensus, Guidelines
INTRODUCTION
Chronic graft-versus-host disease (GVHD) is characterized by pleomorphic clinical manifestations with varying severity and clinical course. Prolonged systemic immunosuppressive treatment, including corticosteroids, is necessary to control disease severity and decrease the risk of nonrelapse mortality. Disease and treatment targeting the immune system causes delayed immune reconstitution with a high risk of infections and other related complications. Furthermore, the refractory nature of underlying fibrosis and limited success of systemic immunomodulatory treatments lead to significant persistence of morbidity for prolonged periods of time. Thus, ancillary therapy and supportive care become central components in the long-term management of chronic GVHD after allogeneic hematopoietic cell transplantation (HCT).
As in the 2005 National Institutes of Health (NIH) consensus framework, “ancillary therapy and supportive care” embraces the most frequent topical immunosuppressive or anti-inflammatory interventions and any other interventions directed at organ-specific control of symptoms or complications resulting from GVHD and its therapy. Also included in this definition are educational, preventive, and psychosocial interventions with this same objective. Several important aspects of good follow-up care, such as monitoring for and management of certain medication toxicities (eg, hypertension, hyperlipidemia, renal dysfunction, seizures, etc.) and problems not directly related to chronic GVHD (eg, iron overload, psychosocial adaptation) fall outside the scope of this document. General screening and preventive policies for survivors of HCT are summarized elsewhere [1,2].
METHODS
The working group searched the Medline (PubMed) database using a broad search strategy to identify studies related to prevention and management of infections, vaccinations, and common complications of chronic GVHD, patient education, and appropriate long-term follow-up and monitoring. The primary search was conducted using “graft-versus-host disease,” “chronic,” “blood and marrow transplantation,” and a variety of specific terms to capture pertinent organ-specific focus (eg, “ocular,” “oral,” etc.). Relevant references in the publications were also reviewed. In general, studies with cohorts including fewer than 20 patients, case reports, and studies of agents that are not commercially available were excluded from consideration.
Recommendations are organized according to an evidence-based system to reflect the strength of recommendations and the quality of evidence supporting them (Appendix 1). A version of this document posted on the Internet includes hyperlinks to Supplements 2–11 that provide additional organ-specific dispensary and other relevant information.
The 2014 international NIH Ancillary Therapy and Supportive Care Working Group was first subdivided into organ-specific subgroups, each of which was charged with the purpose of reviewing all new evidence since 2005. The subgroups subsequently came together to discuss all relevant new findings. Final recommendations were developed after discussion with the steering committee (Appendix 2). Overall, the percentages of level I and II evidence-based recommendations have not changed from 2006 to 2014 (Figure 1).
Figure 1.
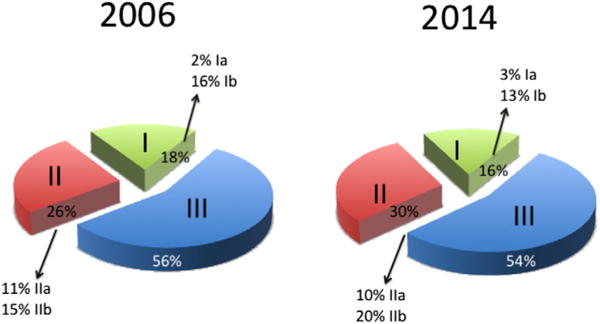
Distribution of NIH Consensus Ancillary and Supportive Care Recommendations based on quality of evidence compared to 2006 Consensus. The number of recommendations made in 2006 was 100 and in 2014, it was 123.
A summary of the major changes to the 2006 NIH Ancillary and Supportive Care Consensus Recommendations is shown in Supplement 1. The Working Group emphasizes that the recommendations in this document represent a wide variety of generally accepted current medical practices. Good clinical judgment and individual circumstances should determine appropriate interventions for specific patients.
SUMMARY OF RECOMMENDATIONS
Table 1 provides a summary of ancillary therapy and supportive care interventions, categorized by organ system. Table 2 provides a summary of general monitoring recommended for patients diagnosed with chronic GVHD.
Table 1.
Summary of Ancillary Therapy and Supportive Care Interventions
| Organ System | Organ-Specific Intervention*
|
|||
|---|---|---|---|---|
| Prevention | Treatment | |||
| Skin and appendages | Photoprotection e sun avoidance and physical sunblocks (eg, protective clothing, UVA, and UVB sunscreens). Avoidance of photosensitizing agents (eg, voriconazole). Surveillance for malignancy [2,3]. | For intact skin e topical emollients including urea containing products, corticosteroids, antipruritic agents, and others (eg, PUVA or narrow band UVB, calcineurin inhibitors). | ||
| For erosions/ulcerations e microbiologic cultures, topical antimicrobials, protective films or other dressings, debridement, hyperbaric oxygen, wound care specialist consultation. | ||||
| Mouth and oral cavity | Maintain good oral/dental hygiene. Routine dental cleaning and radiographs. Surveillance for infection and malignancy. Nutritional counseling, if needed. | Topical high and ultra-high potency corticosteroids and topical calcineurin inhibitors. Topical analgesics. Therapy for oral dryness (eg, salivary stimulants, sialogogues) and for prevention of related complications (ie, dental decay). | ||
| Eyes | Photoprotection. Surveillance for infection, cataract formation, and increased intraocular pressure. | Artificial tears, ocular ointments, topical corticosteroids or cyclosporine, punctal occlusion, humidified environment, occlusive eye wear, moisture chamber eyeglasses, cevimeline, pilocarpine, gas-permeable scleral contact lens, autologous serum, microbiologic cultures, topical antimicrobials, doxycycline. | ||
| Vulva and vagina | Surveillance for estrogen deficiency, infection (HSV, HPV, yeast, bacteria) and malignancy [3]. | Water-based or silicone lubricants, topical estrogens, topical corticosteroids or calcineurin inhibitors, dilators or vibrators, surgery for extensive synechiae or obliteration, early gynecology consultation. Avoid glycerin, paraben, fragrance, and other additive products, | ||
| Gastrointestinal tract and liver | Surveillance for infection (viral, bacterial, fungal, parasites) | Rule out other potential etiologies. Dietary modification, enzyme supplementation for pancreatic insufficiency, bile salt resins, gastroesophageal reflux management, esophageal dilatation, ursodeoxycholic acid, topical glucocorticoids, limitation of ethanol intake, avoidance of hepatotoxins. | ||
| Lungs | Surveillance for infection (Pneumocystis jiroveci, viral, fungal, bacterial). | Rule out other potential etiologies (eg, infection, gastroesophageal reflux). Inhaled corticosteroids, bronchodilators, supplementary oxygen, pulmonary rehabilitation. Consideration of lung transplantation in appropriate candidates. | ||
| Hematopoietic | Surveillance for infection (CMV, parvovirus) | Rule out other potential etiologies (eg, drug toxicity, infection). Hematopoietic growth factors, immunoglobulin for immune cytopenias | ||
| Neurologic | Calcineurin drug level monitoring. Seizure prophylaxis as indicated, including blood pressure control, electrolyte replacement, anticonvulsants. EMG monitoring and staging in symptomatic patients taking medications known to cause neuropathy. Close monitoring of distal extremities for wounds in insensate patients. | Occupational and physical therapy to prevent falls and improve function, treatment of neuropathic syndromes with tricyclic antidepressants, SSRI, or anticonvulsants [4]. Orthotics and assistive devices (canes and walkers). Bracing, splinting or surgical release for entrapment neuropathies. | ||
| Immunologic and infectious diseases | Immunizations and prophylaxis against Pneumocystis jirovecii, VZV, and encapsulated bacteria based on CDC guidelines. Consider immunoglobulin replacement based on levels and recurrent infections. Surveillance for infection (viral, bacterial, fungal, atypical). | Organism-specific antimicrobial agents. Empiric parenteral broad-spectrum antibacterial coverage for fever. | ||
| Musculoskeletal | Surveillance for decreased ROM, bone densitometry, calcium levels and 25-OH vitamin D. Physical therapy, calcium, vitamin D, and bisphosphonates. Flexion-extension x-rays to look for instability. | Physical therapy, bisphosphonates for osteopenia, and osteoporosis. Spinal orthosis for instability and/or intractable pain. Walking program, resistance training, core strengthening. | ||
SSRI indicates selective serotonin reuptake inhibitors; CDC, Centers for Disease Control.
In general, close serial monitoring of all organ systems is recommended to promote early detection and intervention directed toward reversing or preventing progression of chronic GVHD manifestations and treatment-associated toxicities. Ancillary and supportive care therapies are commonly employed in addition to systemic GVHD treatment, although in some cases their use may circumvent the need for systemic treatment or allow doses of systemic agents to be reduced.
Table 2.
Summary of Monitoring Recommendations*
| Parameter | Minimum Frequency (mo) During Systemic Immunosuppressive Therapy |
|---|---|
| Interval history with symptom assessment (including psychosocial symptoms) and medication review | 3 |
| Physical examination (by healthcare provider) | |
| General | 3 |
| Photographic ROM | 3–6 |
| Skin surveillance for secondary malignancy | 6–12 |
| Weight: | |
| Adults | 3 |
| Children | 1–3 |
| Height: | |
| Adults | 12 |
| Children | 3–6 |
| Nutritional assessment† | |
| Adults | 3–6 |
| Children | 1–6 |
| Tanner score (children and adolescents) | 6–12 |
| Developmental assessment (children and adolescents) | 3–6 |
| Laboratory monitoring | |
| Complete blood counts with differential | 3 |
| Chemistry panel including renal and liver function tests | 3 |
| Therapeutic drug monitoring | 3 |
| IgG level (until normal and independent of replacement) | 1–3‡ |
| Lipid profile (during treatment with corticosteroids or sirolimus). | 6 |
| Iron indices (if red cell transfusions are required or if iron overload has been documented previously) | 6–12 |
| Pulmonary function tests (PFT) | 3–6 |
| Endocrine function evaluation, eg, thyroid function tests, bone densitometry (if an abnormal result might change clinical management), calcium levels, 25-OH vitamin D | 12 |
| Subspecialty evaluations | |
| Ophthalmology | 3–12 |
| Dental assessment and oral cancer surveillance, including soft and hard tissues examination (radiographs as indicated); culture, biopsy or photographs of lesions (as clinically indicated); and professional dental hygiene. | 6 |
| Dermatology with assessment of extent and type of skin involvement, biopsy, or photographs (as clinically indicated). | 12* |
| Gynecology for vulvovaginal involvement (as clinically indicated). | 3–12 |
| Physiotherapy with assessment of ROM (if joint limitation is present). | 3–12 |
| Neuropsychological testing (as clinically indicated). | 12 |
All organ systems should be monitored at least annually and after immunosuppressive therapy is completed during extended survivorship [1,2]. The scope and frequency of monitoring should be individualized as clinically indicated. More frequent monitoring is strongly advised for those with active GVHD, especially during high-risk periods (eg, treatment taper or escalation).
Could be screened by health care provider and referred to nutritionist, if indicated.
Context dependent because post-transplantation immunoglobulin replacement during chronic GVHD therapy is not routine after the first post-transplantation year except when there are recurrent sinopulmonary infections or HCT for underlying primary immunodeficiency disease. See Table 11.
SKIN AND APPENDAGES
Ancillary and supportive care of the skin and appendages focuses on prevention, management of manifestations such as pruritus, rash, pain, dyspigmentation and limited range of motion (ROM), as well as topical care for erosions, ulcerations, and superinfection (Table 3). Topical therapy plays an important role in alleviating symptoms and treating complications caused by loss of skin integrity and immunosuppression. Because skin cancer incidence is increased in patients with chronic GVHD, vigilant monitoring is necessary so that early malignancies and premalignancies can be detected early and treated appropriately.
Table 3.
Ancillary Therapy and Supportive Care Recommendations for Skin GVHD
| Type of Intervention | Recommendation Rating |
|---|---|
| Preventive measures | |
| Photoprotection: UVA and UVB blockade including: | |
| Avoidance of sun exposure (especially between 10:00 am and 4:00 pm) | AIII |
| Use of sunscreens (>SPF 20 with broad-spectrum UVA and UVB protection) | AIII |
| Protective clothing | AIII |
| Avoidance of photosensitizing agents | AIII |
| Treatment | |
| Intact skin | |
| Symptomatic treatment with emollients and antipruritic agents | AIII |
| Topical corticosteroids | CIIb |
| Light therapy (PUVA, UVA1, UVB, narrow-band UVB) | CIIa |
| Topical calcineurin inhibitors (pimecrolimus, tacrolimus) | CIIa |
| Sclerotic manifestations with joint stiffness or contractures | |
| Deep muscle/fascial massage (Heller works) to improve ROM | CIII |
| Stretching exercises to improve ROM | BIII |
| Erosions and ulcerations | |
| Topical or oral antimicrobials | BIII |
| Wound dressings and debridement | CIII |
| Control of edema | BIII |
|
| |
| PEDIATRIC CONSIDERATIONS Systemic side effects of topical steroids and topical calcineurin inhibitors may occur more frequently in young children because of the larger skin surface area to body weight ratio. Although the least potent topical steroids (1% to 2.5% hydrocortisone) are safe, middle to upper mid-strength topical steroids should generally be used sparingly, and on limited areas, for no more than 3 to 4 wk. Topical steroids under occlusive dressings are not recommended. The use of potent or super-potent steroids on the face, or at any site in infants <1 yr of age, is not recommended. Avoid urea or menthol containing products in young children because they may cause skin irritation. | |
SPF indicates sun protective factor; PUVA, photochemotherapy.
Measures to Prevent the Development or Exacerbation of GVHD
Environmental ultraviolet radiation can cause exacerbation of cutaneous GVHD [5]. Photoprotection includes protective clothing, sun avoidance, physical sunblocks, and sunscreens. Topically applied agents should protect against both ultraviolet A (UVA) and ultraviolet B (UVB). Micronized zinc, micronized titanium dioxide, mexoryl SX, or Parsol 1789 (avobenzone; DSM, Basel, Switzerland) are useful additives to ensure adequate UVA protection. Laundry rinse cycle additives can enhance the ultraviolet barrier function of clothing.
Avoidance of Photosensitizing Agents
Several commonly prescribed medications have been associated with phototoxic drug eruptions that typically appear like severe sunburn, often associated with skin burning and/or pruritus. This list of such medications is extensive but voriconazole deserves special mention because of its particular dual association with phototoxicity and increased risk of squamous cell carcinoma [6].
Topical Care and Therapies for Intact Skin
Most patients with extensive rash will require systemic therapy, a topic beyond the scope of this review.
Regular lubrication of dry but intact skin with emollients may decrease pruritus and maintain skin integrity. Ointments and creams are better skin softeners than lotions and are less likely to sting when applied to erythematous skin. Moisturizers that contain 3% to 10% urea or glycerol are particularly efficacious for increasing skin hydration, but urea products can be more irritating to inflamed skin or in infants.
Topical steroids and emollients can improve cutaneous chronic GVHD, particularly nonsclerotic skin lesions without erosions or ulcerations (lichen-planus–like or papulosquamous plaques). Long-term use of topical steroids may be complicated by local skin atrophy and development of striae.
- General guidelines regarding topical steroid recommendations for skin GVHD:
- From the neck down: treatment should begin with mid-strength topical steroids (eg, triamcinolone 0.1% cream or ointment). In unresponsive cases, short-term occlusion of mid-strength steroids with damp towels (“wet wraps”) increases skin hydration and steroid penetration. When this is impractical, higher potency steroids (eg, fluocinonide 0.05% cream or ointment) may be helpful. The most potent topical steroids (eg, clobetasol dipropionate 0.05%, halobetasol propionate 0.05%) should not be used under occlusion. The use of wet wraps and high-potency steroids should be limited to less than 14 consecutive days, if possible.
- Face, axillae, and groin: lower potency steroids (hydrocortisone 1% to 2.5%, desonide 0.05%) are preferable for long-term use.
- Emollients: these may be used after the application of steroids. Emollients are occlusive and may increase the potency of steroids.
- Antipruritics: Although pruritus related to GVHD generally responds to immunosuppressive therapy, other adjuvant treatments may be useful.
- Topical: hydrocortisone/pramoxine or menthol-based creams/lotions.
- Systemic: antihistamines (eg, diphenhydramine, hydroxyzine, ranitidine) may help, but severe pruritus rarely responds to standard dosing. Refractory symptoms may benefit from the addition of gabapentin.
- Others interventions:
- Psolaren with UVA [7–9] or UVA1 (340 to 400 nm) [10], UVB [11], or narrow-band UVB (311 to 313 nm) [12] can be effective, especially if sclerosis is not present. Phototherapy may be administered 2 to 3 times per week by dermatologists. Cautionary note: phototherapy is associated with an increased risk of phototoxicity and skin cancer.
Topical Care for Nonintact Skin
When appropriate, superficial or deep tissue culture should be obtained to test for bacterial, viral, fungal, or mycobacterial infection in eroded, ulcerated, or suspicious skin lesions. The differential diagnosis for noninfectious skin lesions includes vasculitis, recurrent malignancy, GVHD, hypersensitivity or drug reactions, dermatitis, and primary skin cancer. The general recommendations on wound care do not differ from those for patients without chronic GVHD.
For specific dispensing information, please see Supplement 2.
MOUTH AND ORAL CAVITY
Chronic GVHD can affect the oral cavity through lichen planus–like involvement of the mucosa, salivary gland involvement with subsequent hypofunction and xerostomia, and sclerotic involvement of the oral mucosa and surrounding skin tissues. Oral chronic GVHD can cause pain, sensitivity to various foods and beverages, taste impairment, dryness, dental caries, and decreased ROM. Infections including candidiasis and recrudescent herpes simplex virus (HSV) should be ruled out before initiating any form of therapy. When clinically indicated, viral and bacterial cultures, viral PCR, or biopsies should be performed. Drug-related conditions, such as sirolimus-associated aphthous-like ulcerations and calcineurin inhibitor–associated fibrovascular ulcerative lesions, must be considered.
Topical treatment may provide greater local benefits than systemic therapy alone (Table 4). When the oral cavity is the only site of chronic GVHD activity, and even when severe (eg, extensive ulcerations), intensive ancillary treatment might suffice to control the disease in the absence of systemic therapy.
Table 4.
Ancillary Therapy and Supportive Care Recommendations for Mouth and Oral Tissues
| Indication, Preparation*, Active agent, Concentration | Rating | |||
|---|---|---|---|---|
| Lichenoid-related symptoms/ulcers and erosions | Rinse | Clobetasol | 0.5 mg/mL (0.05%) | AIa |
| Budesonide | 0.3 mg/mL (0.03%) | BIIa | ||
| Dexamethasone | 0.1 mg/mL (0.01%) | AIII | ||
| Triamcinolone | 1 mg/mL (0.1%) | AIII | ||
| Tacrolimus | 0.1 mg/mL (0.01%) | BIIa | ||
| Prednisolone | 3 mg/mL (0.03%) | BIII | ||
| Clobetasol:tacrolimus 1:1 | Not specified | CIII | ||
| Gel, paste, ointment | Clobetasol gel | 0.05% | AIa | |
| Tacrolimus ointment | 0.1% | BIIa | ||
| Fluocinonide gel | 0.05% | BIII | ||
| Intralesional injection | Triamcinolone | 40 mg/mL, .5 mL/cm2 | CIIb | |
| Mucosal pain | Rinse | Lidocaine | 2% | BIII |
| Kaolinite pectin-diphenhydramine-lidocaine 1:1:1 | Not specified | BIII | ||
| Not applicable | CO2 laser for pain relief [30] | Not applicable | CIIIy | |
| Dry mouth | Gel, toothpaste | Fluoride | Per manufacturer | AIb |
| Rinse | Water sipping | Per need | AIII | |
| Gum, candy | Salivary stimulants | Per need | AIII | |
| Tablets | Pilocarpine | 5–10 mg 3–4/d | BIIa | |
| Cevimeline | 15–30 mg 3/d | BIII | ||
| Gastric reflux | Tablets | Proton pump inhibitor, antireflux measures | CIII | |
|
| ||||
| PEDIATRIC CONSIDERATIONS Behavioral: Children often don’t communicate symptoms of impaired speech, oral dryness or sensitivities, taste alteration, and dysphagia; reduced oral intake and increased drinking during eating or at night may be presenting symptoms. Specific approaches to help parents assist children with oral topical therapies may improve compliance. Prevention of caries: Bottle drinking should not be used as a pacifier for small children and cup drinking should be introduced as early as possible. Counsel the avoidance of refined carbohydrates including juices and soft drinks. Developmental: Fibrosis and limited mouth opening may contribute to the disruption of craniofacial growth. Pharmacologic considerations: While oral mucosal chronic GVHD generally responds well to topical steroids or calcineurin inhibitors, these agents may produce clinically relevant systemic drug levels in infants and small children. Viscous lidocaine may reduce the gag reflex, compromise swallowing and should be used with caution. Sialogogue use has been limited in children and dosing is not established. Orthodontic: Fixed braces should only be used after healing of acute inflammation. Specific guidelines for optimal force and pace of orthodontic management in chronic GVHD remain undefined. | ||||
The selection of a localized or generalized treatment depends on the extent of oral chronic GVHD.
Optional at centers experienced in the use of this therapy as it currently has limited availability.
All patients with oral chronic GVHD should be informed about their higher risk for developing oral squamous cell carcinoma and undergo annual screening by examination. In particular, patients with persistent or new changes in the oral mucosal color or texture or a growth should be evaluated for second primary cancer to avoid misdiagnosis as chronic GVHD. At the clinician’s discretion testing of the tissue sample for high-risk human papilloma virus (HPV) serotypes may be added. Atypical persistent oral lesions should be considered for a biopsy periodically to rule out progression to malignancy, especially if dysplasia was previously identified histopathologically. The response to high-potency topical steroids may assist in differentiating between oral lesions attributed to chronic GVHD and cancer. However, additional differential diagnoses that may not respond to topical steroids should be considered (eg, hyperplastic candidiasis, frictional keratosis).
Oral Mucosal, Gingival, and Lip Chronic GVHD
The mainstay of ancillary therapy for symptomatic oral mucosal or erythematous or ulcerative disease is the application of high-potency corticosteroid preparations, although evidence to guide the choice of specific agents is limited (Table 4) [15–17]. Solutions are used mainly when manifestations are generalized, whereas gels, creams, and ointments are used for localized lesions, with gels generally preferable due to their hydrophilic properties. Gels, creams, and ointments may be applied locally with a finger or applied to gauze, leaving the gauze in place against the lesion for 10 to 15 minutes before removing. It is important to educate patients on how to use steroid solution formulations. Alternative noncorticosteroid rinse formulations of tacrolimus or cyclosporine may also be effective. Various topical preparations may be used in combinations (eg, a corticosteroid and calcineurin inhibitor). The need for and intensity of these topical therapies are driven primarily by patient symptoms or presence of ulcers to re-establish integrity of the mucosal barrier. The application of topical calcineurin inhibitors is an alternative to locally applied corticosteroids [18,19]. Long-term use of topical steroids has been associated with atrophy of the lip vermillion but not of the oral mucosa. Therefore, treatment of the lips with topical tacrolimus 0.1% minimizes the risk of this adverse event. Intralesional injections of triamcinolone steroids have been used successfully in patients with discrete symptomatic ulcerative lesions that have not responded adequately to topical therapy [20].
All patients should be counseled about the relatively frequent side effect of oral candidiasis and the systemic effects that can result from long-term use of topical therapy with highly potent steroids. If candidiasis occurs, antifungal prophylaxis strategies are effective with continued ongoing topical steroid therapy.
Patients may need to avoid acidic, spicy, strongly flavored, and rough or crunchy foods and drinks because of sensitivity and discomfort. If toothpaste causes oral burning, patients should be instructed to use a children’s toothpaste. Topical analgesia is helpful when symptomatic mucosal GVHD impairs nutrition or communication. Viscous lidocaine may provide some relief. In situations when topical immunosuppressive therapy causes localized burning discomfort, addition of a small amount of viscous lidocaine can be effective in making the rinse more tolerable, although infrequent adverse events have been associated with the use of lidocaine rinses. It is worth remembering that reflux of acidic gastric contents in the context of inadequate salivary bicarbonate may contribute to oral mucosal symptoms; proton pump inhibitors and other antireflux measures might be helpful when symptoms of heartburn are present.
Salivary Gland Chronic GVHD
Patients with salivary gland involvement most frequently report dry mouth and present with signs of mucoid, viscous saliva, reduced or absence of moist film over the mucosal surfaces, absent floor of mouth pooling, accumulation of soft debris, and erythematous mucosal surfaces [21–23]. They may also develop mucoceles, which are recognized as generally painless but “annoying” blisters mostly on the palate and inside the lower lip [24,25]. Patients with salivary gland involvement may be at increased risk for developing dental caries, in particular along the gum line and contact areas. Even without use of intraoral topical steroids, patients with salivary gland chronic GVHD may develop recurrent candidiasis.
Ancillary care for dry mouth may include frequent water sipping, the use of gustatory and mechanical saliva stimulants (sugar-free gum and candy), oral moisturizing agents, and saliva substitutes. The milder flavored toothpastes marketed for children are often better tolerated. Caries can be prevented by home fluoride treatments before sleep. Even in patients without subjective oral dryness, mild salivary gland dysfunction can increase the risk of tooth decay, and topical fluoride should be considered as a decay prevention strategy [23,26]. If possible, avoidance of xerogenic medications such as tricyclic antidepressants, selective serotonin reuptake inhibitors, antihistamines, and opioids may help alleviate symptoms of dry mouth. Sialogogue therapy with cholinergic agonists (cevimeline, pilocarpine) may produce a significant enhancement of salivary secretion and may be offered in the absence of contraindications (eg, glaucoma, heart disease, or obstructive pulmonary disease) [27,28].
Sclerotic Manifestations of Oral Chronic GVHD
Topical therapy alone is insufficient for treating sclerosis of the perioral skin and surrounding tissues caused by chronic GVHD. In this situation, systemic treatment is required; however, the sclerosis is typically quite extensive once perioral skin is affected. In cases of focal intraoral mucosal sclerosis, typically affecting the posterior buccal mucosa, adjunctive intralesional steroid injections may be helpful, but long-term therapy is often required to maintain the response. Stretching exercises with or without the use of a physical therapy device to increase ROM of the mouth may be helpful.
Routine Dental Treatment
Patients with chronic GVHD should receive routine dental care, including regularly scheduled professional dental cleanings, and fluoride applications. The necessity for antibiotic prophylaxis in patients with chronic GVHD remains controversial. However, some centers follow The American Heart Association’s protocol for prevention of bacterial endocarditis [27]. Extended antibiotic therapy should be determined by the transplantation physician based on the dental disease, the type of treatment, and the patient’s risk for infection.
Patients with chronic GVHD who are currently or have previously been treated with antiresorptive therapy (eg, bisphosphonates, denosumab) are at risk for developing medication-related osteonecrosis of the jaw [29]. Similar to dental screening before HCT, dental consultation and implementation of appropriate dental and oral hygiene measures should be initiated before antiresorptive therapy.
For specific dispensing information, please see Supplement 3.
EYES
The clinical spectrum of chronic ocular GVHD includes acute conjunctival inflammation, pseudomembranous and cicatricial conjunctivitis, and, most frequently, keratoconjunctivitis sicca (or KCS). KCS often accompanies chronic GVHD activity in other organs and may be a prominent disease manifestation. Conversely, dry eyes may occasionally be the only manifestation of chronic GVHD [31]. The diagnosis of KCS is made by the presence of appropriate symptoms, tear production averaging ≤ 5 mm (Schirmer’s test), and clinical signs of keratitis. Although ocular symptoms and external examination can be ascertained from a clinic visit, a slit lamp examination by an ophthalmologist is generally required to make the diagnosis of KCS. In all cases, infectious keratitis must be ruled out. Most ancillary treatment for ocular chronic GVHD is aimed at relief of dry eyes (Table 5). When the sole manifestations of chronic GVHD are ocular, systemic immunosuppressive therapy may need to be initiated (or resumed) when topical and other local measures are insufficient to control inflammation and symptoms.
Table 5.
Ancillary Therapy and Supportive Care Recommendations for Eye GVHD
| Therapy | Indication | Rating |
|---|---|---|
| Topical | Mild* | |
| AT, preservative free | AIb | |
| Viscous ointment at bedtime/viscous tears during the day | BIb | |
| Moderate/severe* | ||
| Cyclosporine eye drops | CIb | |
| Topical steroid drops | BIIIa | |
| Lacriserts (Valeant Pharmaceuticals) for patients that use AT more frequently than hourly | CIb | |
| Autologous serum eye drops (limited availability) | CIb/CIIa | |
| Oral | Moderate/severe* | |
| Cevimeline | CIb | |
| Pilocarpine | CIb | |
| Surgical | Moderate/severe* | |
| Punctal occlusion (temporary or permanent occlusion, using silicone plugs or thermal cautery) | BIb/IIa | |
| Superficial debridement of filamentary keratitis | CIII | |
| Partial tarsorrhaphy | CIIb | |
| Moderate/severe* | ||
| Eye wear/environmental strategy | Occlusive eye wear (www.dryeyepain.com www.panoptx.com) |
BIII CIII |
| Lid care/warm compress/humidified environment | CIII | |
| Bandage contact lens (used with caution) | CIII | |
| Gas-permeable scleral lens | CIIa | |
|
| ||
| PEDIATRIC CONSIDERATIONS Although severe ocular sicca is uncommon in children with chronic GVHD, measured tear production is reduced, and surveillance for keratoconjunctivitis sicca is necessary. Ocular sicca generally responds to ancillary measures in conjunction with systemic immunosuppression. Experience is limited and dosing is not established for many of the topical and oral medications for ocular GVHD. | ||
AT indicates artificial tears.
Definitions of severity follow the Diagnosis and Scoring report [47].
Symptoms include burning, irritation, pain, foreign body sensation, blurred vision, photophobia, and paradoxically, excessive tearing [32]. Other causes of dry eyes must be considered, such as medications with anticholinergic side effects (antihypertensives, antidepressants, psychotropics, antihistamines, decongestants) and previous treatments (such as total body irradiation, chemotherapy, history of autologous HCT).
Aqueous tear deficiency/lacrimal gland dysfunction may fluctuate during systemic GVHD. Although systemic immunosuppressive therapies for chronic GVHD generally do not lead to improvement in the Schirmer scores, especially in cases of longstanding lacrimal gland dysfunction, they can improve overall symptoms of ocular GVHD.
If possible, an ophthalmologist who is knowledgeable about GVHD should be involved to coordinate care in a multidisciplinary fashion. Ancillary and supportive care for the eye focuses on increasing ocular surface moisture (by lubrication and decreasing tear evaporation and tear drainage from the surface of the eye) and on decreasing ocular surface inflammation.
Decreasing Ocular Surface Inflammation
To decrease ocular surface inflammation, judicious use of topical steroids may be necessary. In general, this type of treatment should be reserved for the control of ocular GVHD exacerbation when systemic immunosuppression is being tapered [33]. Topical steroids have been used for cicatricial conjunctivitis in limited case series [34]. Pulsed topical steroids should be carefully supervised by an ophthalmologist, as steroid-related complications include increased intraocular pressure, cataract formation, and silent infectious keratitis. Topical cyclosporine can be prescribed to control immune responses at the ocular surface [35]. The benefit of topical cyclosporine on tear function in GVHD has not been documented, but this type of treatment increases Schirmer scores and decreases surface apoptosis in patients with other dry eye conditions. Ocular surface inflammation may also be improved with autologous serum, but this treatment is available in only a limited number of centers [36,37].
Lubrication
For lubrication, the range of adjunctive measures includes the use of preservative-free artificial tears to coat the ocular surface, thereby minimizing superficial punctuate keratopathy (dry spots on the cornea), reducing the ocular symptoms, and improving the quality of vision. Because patients may tolerate certain formulations better than others, they should be encouraged to test different brands to identify that which provides the most benefit.
For patients who may require application of artificial tears more than once every hour, the use of slowly dissolving 5 mg pellets of hydroxypropyl methylcellulose may be more convenient [38]. Lacriserts (Valeant Pharmaceuticals, Lakewood, NJ) are available by prescription and are inserted once or twice daily into the inferior cul-de-sac of the eye but may produce a constant foreign body sensation. Oral medications may be used to increase lubrication by stimulating aqueous tear flow with selective muscarinic agonists, such as cevimeline [39] or pilocarpine [40]. These have been shown to improve sicca symptoms in patients with Sjogren’s syndrome, but drug interactions and toxicities must be reviewed because contraindications include glaucoma, heart disease, and asthma.
Control of Drainage
To decrease drainage from the surface of the eye, temporary or permanent occlusion of the tear duct punctae may provide additional benefit for patients with severe ocular sicca syndrome (<5 mm tear wetting) [41–43]. Permanent punctal occlusion (via thermal cauterization) may be necessary, as the silicone plugs used for temporary occlusion fall out repeatedly. Repeated thermal cautery may be needed if punctae reopen.
Control of Evaporation
Scleral lenses are beneficial in severe cases and are becoming more widely available [44–46]. These gas-permeable lenses are larger in diameter than regular contact lenses. By fitting on the sclera, they can often be worn by patients who are otherwise contact lens intolerant. In situ, scleral lenses continuously bath the cornea via a fluid reservoir of saline and/or artificial tears, which helps rejuvenate ocular surfaces. This fluid reservoir cushion covers distorted corneal surfaces, improves vision, and reduces pain and photosensitivity.
For specific dispensing information, please see Supplement 4.
GENITALIA
General Hygiene, Routine Surveillance, and Vulvovaginal Atrophy
General hygiene, routine gynecologic evaluations, as well as management of vulvar and vaginal atrophy are important to integrated care but are beyond the scope of this article. (See also Supplement 5).
Vulva and Vaginal Mucosa
The incidence of vulvovaginal chronic GVHD ranges between 20% and 50% based on gynecological surveillance evaluations up to 2 years after transplantation, with a higher risk in recipients of a peripheral blood graft [48–50]. The diagnosis of vulvovaginal GVHD relies on symptoms and physical findings. Histological confirmation is strongly recommended in the absence of diagnostic manifestations of chronic GVHD in other organs. Estrogen deficiency and infections (HPV, HSV, yeast, bacteria, or other recognized gynecological pathogens) must be ruled out at the time of initial diagnosis and periodically during management of vulvar or vaginal GVHD.
Chronic GVHD of the vulva and vagina presents with abnormalities of the mucosa or manifestations of sclerotic changes. Symptoms may include dysuria, dryness, tenderness to touch, and dyspareunia. Mild chronic GVHD of the vulva may occasionally be asymptomatic and detected only by examination. Mild to very active vaginal chronic GVHD can be asymptomatic. Physical findings of the vulva include erythematous patches (mucositis), retiform leucokeratosis (lichen-planus–like lesions), vestibular tenderness, agglutination of vulvar structures with thin adhesions or dense fibrosis between the clitoris and prepuce, or across the interlabial sulcus, and less often, ulcers. Vaginal findings include mucositis, ulcers, a yellow or green discharge, phimosis, and dense fibrotic changes that commonly involve the cervival-vaginal sulcus. Sclerosis of vulvar and vaginal tissues can lead to narrowing of the introitus, shortening, and even complete obliteration of the vaginal canal. Adhesions and fibrosis that involve the upper vagina or cervix may lead to hematometra. Although most patients with vulvar or vaginal GVHD have involvement of the mouth or other sites, vulvovaginal manifestations may sometimes be the only sign of chronic GVHD [48,49,51].
Post-HCT females of appropriate age, and especially those who are symptomatic, should be evaluated and followed by a gynecologist with experience in GVHD, and if not available, by practitioners with experience in non-neoplastic inflammatory diseases of the genital tissues, such as lichen planus.
Vulvovaginal GVHD
When the vulvovaginal region represents the only clinical manifestation of chronic GVHD activity, topical immunosuppressive agents might constitute an adequate primary therapy for controlling mild clinical manifestations (Table 6). Application of ultra-high potency corticosteroid is the mainstay of therapy, whereas topical calcineurin ointments also have efficacy [48,49,51–55]. The anti-inflammatory antibiotic clindamycin has been used successfully as an intravaginal therapy, often applied together with corticosteroids [56]. Patients may develop candidiasis or experience recurrence of HSV or HPV during immunosuppressive therapy and must be counseled to monitor for symptoms.
Table 6.
Ancillary Therapy and Supportive Care Recommendations for Vulvar and Vaginal GVHD
| Type of Intervention | Rating |
|---|---|
| Vulvar hygiene to minimize irritation | |
| Avoid skin contact with chemical irritants (eg, soap and feminine wash products) and synthetic clothing | BIII |
| Cleanse genital area with warm water, allow air circulation, and wipe front to back, use cotton underwear | BIII |
| Sparing use of simple emollients to vulva (not vagina) | BIII |
| Personal lubricants | BIII |
| Vulvovaginal atrophy | |
| Topical intravaginal or systemic estrogen ± progestin therapy as indicated based on patient-specific considerations | BIII |
| Topical therapy for vulvar GVHD | |
| Clobetasol gel 0.05% (vagina) | BIIa |
| Betamethasone dipropionate 0.05% ointment | BIII |
| Tacrolimus ointment 0.1% (vulva) | BIIb |
| Topical therapy for vaginal GVHD | |
| Hydrocortisone (10%) in 2% clindamycin base (apply 5 g with vaginal applicator nightly) | BIII |
| Clobetasol gel 0.05% applied twice daily | BIIa |
| Betamethasone dipropionate augmented gel | BIII |
| Tacrolimus vaginal suppositories 0.1% nightly (2 mg tacrolimus per 2 g suppository) | BIIb |
| Surgical therapy | |
| Surgical lysis with or without vaginal reconstruction followed by 6 mo of dilator therapy may be necessary for treatment of extensive synechiae and complete obliteration of the vaginal canal. | BIII |
|
| |
| PEDIATRIC CONSIDERATIONS Vulvar or vaginal GVHD needs to be considered as soon as physical development has progressed beyond thelarche and into pubarche. Vulvovaginal GVHD has been observed infrequently in prepubertal girls. Evaluation by an adolescent gynecologic practitioner is recommended when a diagnosis of vulvovaginal GVHD is being considered. | |
Sclerotic features of vaginal GVHD should be treated aggressively with topical corticosteroids and dilators. Surgical lysis with or without vaginal reconstruction is necessary for patients with extensive synechiae and complete obliteration of the vaginal canal. Topical treatment with calcineurin inhibitors has been used successfully to avoid surgery in some cases. These agents have also been used post-operatively with resumption of vaginal intercourse [53].
Penis and Foreskin
Only a few cases of male genital chronic GVHD have been reported, including lichenoid genital lesions on the foreskin or glans penis, phimosis, lichen sclerosis, and contracture secondary to Peyronie’s disease [57]. Routine assessment as part of the history and physical is essential for early detection of this rare but treatable manifestation of GVHD.
GASTROINTESTINAL TRACT AND LIVER
Gastrointestinal manifestations occur frequently in patients with chronic GVHD. These include dysphagia, odynophagia, heartburn, anorexia, nausea, vomiting, abdominal pain, diarrhea, weight loss, malnutrition, and jaundice. Each of these symptoms has a specific differential diagnosis that includes chronic GVHD, protracted acute GVHD, infection, biliary stone disease, medication side effects, and fibrotic complications of a previous injury (eg, intestinal strictures and hepatic fibrosis). The diagnosis of 1 cause of symptoms does not preclude the presence of other causes. Therefore, it is important to confirm the diagnosis of chronic GVHD before beginning treatment [58,59].
Odynophagia and Dysphagia
Lubrication can ease swallowing discomfort due to xerostomia. Other possible causes of odynophagia or dysphagia include esophageal webs, rings, strictures, dysmotility, or nonchronic GVHD diagnoses, such as pill esophagitis, infection, radiation esophagitis, and strictures caused by peptic reflux. Endoscopy is usually needed to exclude or confirm these diagnoses. Esophageal dilation may be helpful in patients with documented webs or strictures, but this procedure can cause perforation and should be performed by an experienced gastroenterologist (Table 7).
Table 7.
Ancillary Therapy and Supportive Care Recommendations for GI/Liver GVHD
| Type of Intervention | Rating |
|---|---|
| Esophageal dilation for webs or stricture | BIII |
| Dietary modifications for carbohydrate, fat malabsorption | BIII |
| Pancreatic enzyme replacement for insufficiency | BIIa |
| Ursodeoxycholic acid if cholestasis | BIIa |
| Lactase tablets or lactase-containing dairy products | BIII |
| Topical glucocorticoid formulations for late acute GVHD | CIa |
| Bile acid binding resins if bile salt malabsorption (eg, cholestyramine) | CIII |
|
| |
| PEDIATRIC CONSIDERATIONS No substantive differences. | |
Diarrhea
Patients presenting with acute diarrhea should have a standard infectious screen depending on severity and epidemiologic considerations (eg, enteric bacterial and viral pathogens, Clostridium difficile toxin, cytomegalovirus [CMV], adenovirus). Protracted diarrhea during treatment with immunosuppressive medications requires a broad search for gut pathogens, including norovirus, rotavirus, astrovirus, cryptosporidia, giardia lamblia, microsporidia, and others, depending on geographic conditions. The differential diagnosis also includes noninfectious, causes such as intestinal mucosal disease, pancreatic insufficiency, magnesium and other medication side effects. Of note, CMV enteritis can be present without CMV viremia. Pancreatic atrophy, an indication for enzyme supplementation, occurs rarely in patients with prolonged chronic GVHD. Mycophenolate mofetil may also cause enteritis with manifestations similar to GVHD. Acute GVHD of the gastrointestinal tract may benefit from the addition of oral topical glucocorticoids. Judicious use of loperamide or diphenoxylate for diarrhea, nortriptyline or dicyclomine for symptoms of irritable bowel syndrome, or pancreatic enzymes for fat malabsorption symptoms can be considered in the right clinical circumstances.
Abnormal Liver Tests
Liver disorders in patients with chronic GVHD may present in several ways: abnormalities of blood tests (alanine aminotransferase [ALT], alkaline phosphatase [AP], gammaglutamyl transpeptidase [GGT], bilirubins, iron/ferritin); development of signs of portal hypertension and end-stage liver disease; and abnormalities on hepatobiliary imaging (ultrasound, computed tomography, magnetic resonance imaging). Each presentation has a specific differential diagnosis and treatments depend on accurate diagnoses, which in turn depend on a careful history, liver imaging, viral tests, and in some patients, liver histology. Liver GVHD presentations may be hepatitic (elevated serum aspartate and alanine aminotransferases, AST/ALT) and cholestatic. Significant ALT elevations and any degree of jaundice require systemic treatment with immunosuppressive medications and ursodeoxycholic acid if the cause is GVHD. Treatment of iron overload is also indicated when present. Multiple causes of liver dysfunction can be present simultaneously. Causes of portal hypertension are investigated with cardiac, hepatic vein, and liver imaging, along with liver elastography and histology in some cases.
Management of liver GVHD with persistent cholestasis, chronic viral hepatitis, iron overload, or end-stage liver disease is beyond the scope of this manuscript.
Weight Loss
Chronic GVHD is an important risk factor for low body mass index and lean body mass [60], but the mechanisms can be complex. Oral caloric intake is limited by oropharyngeal and esophageal pathology. In addition, upper gastrointestinal GVHD is frequently accompanied by anhedonia for food, anorexia, and satiety. Immunosuppressive medications such as calcineurin inhibitors, mycophenolate mofetil, azoles, and trimethoprim/sulfamethoxazole (TMP/ SMX) commonly cause nausea. Weight loss in patients with extensive chronic GVHD may also be caused by increased action of glucagon and norepinephrine, resulting in an increase in resting energy expenditure and alterations in fat and carbohydrate oxidation rates [61]. Nutritional support is very important as around 30% of adults [62,63] and up to 40% of children with chronic GVHD are malnourished [64]. The input of a nutritionist can be very helpful in addressing weight loss, as some patients will need total parenteral nutrition or tube feedings. A multidisciplinary team including a gastroenterologist, nutritionist, and oncologist may help to ensure adequate nutrition.
For specific dispensing information, please see Supplement 6.
LUNG
The currently recognized noninfectious pulmonary manifestations of chronic GVHD are bronchiolitis obliterans syndrome (BOS) and its earlier precursor, which is lesser degrees of airflow obstruction [65]. Dyspnea, wheeze, or cough occur frequently in chronic GVHD and clinical examination, pulmonary function tests (PFTs) [66–68], radiologic studies, and bronchoalveolar lavage help to distinguish BOS from other pulmonary diseases (eg, pulmonary thromboembolism, cryptogenic-organizing pneumonia, radiation-induced lung injury), extrapulmonary diseases (eg, effusions, subcutaneous sclerosis), and lung infections. Air trapping and bronchiectasis may result from advanced BOS, infections, or both. Pneumothorax, pneumomediastinum, or subcutaneous emphysema might cause respiratory deterioration independently or may complicate BOS. Common diseases that may contribute to lung function deterioration (with or without BOS) should be investigated and treated, including chronic postnasal drip, recurrent sinus infections, or gastroesophageal reflux disease [65].
Because the prognosis of BOS remains poor, early diagnosis and treatment are considered essential. Limited data are available to guide the frequency of post-transplantation PFT monitoring in asymptomatic patients, those with chronic GVHD, or those with established BOS. Because patients may have subclinical changes in pulmonary function before a diagnosis of chronic GVHD or BOS has been made, frequent monitoring of PFTs or at least limited spirometry every 3 months is recommended for high-risk patients during the first 1 to 2 years by some experts [65,69,70], followed by additional evaluations in the setting of unexplained irreversible decline of forced expiratory volume in 1 second (FEV1) >10% [69]. More data are needed to further define the role of bronchoscopy or chest imaging in monitoring pulmonary complications after HCT, including new diagnostic tools such as parametric response mapping [71].
In established BOS, small retrospective studies suggest a beneficial effect on symptoms, stabilization of FEV1 and reduced systemic prednisone exposure, when inhaled corticosteroids are added either alone [72] or in combination with bronchodilatators [73] or azithromycin and montelukast [74] (Table 8). Combination therapy with fluticasone, azithromycin, and montelukast is tolerable and may benefit newly diagnosed BOS. Pulmonary rehabilitation programs may be beneficial in BOS [75], as has been shown in chronic obstructive pulmonary disease. Standard 6-minute walk tests [76] help to better characterize physical performance and identify patients who need supplemental oxygen based on having pulse oximeter oxygen saturation (SpO2) <87% while breathing room air.
Table 8.
Ancillary Therapy and Supportive Care Recommendations for Lung GVHD
| Type of Intervention | Rating |
|---|---|
| Inhaled corticosteroids and bronchodilators | CIb |
| Fluticasone, azithromycin, montelukast | CIII |
| Prophylactic IVIG | DIa |
| Pulmonary rehabilitation | CIII |
| Supplementary oxygen | AIII |
|
| |
| PEDIATRIC CONSIDERATIONS Formal spirometry, lung volumes and diffusing capacity are not measurable in children < 7 yr of age, but negative plethysmography is an option. Actual measured PFT values must be carefully considered in pediatric patients, because predicted normal values vary with age, weight, and height. Therefore, percent predicted values might spuriously show serial decrease over time without substantive decline in absolute values. | |
Respiratory infections may aggravate respiratory impairment and should be treated urgently. Bronchoalveolar lavage is highly recommended, as the only manifestation of a significant lung infection may be a decline in FEV1 or forced vital capacity. Patient education for preventive measures against transmission of respiratory infections and avoidance of inhaled pulmonary toxins from cigarettes, marijuana, and dust should be emphasized. Interventions pioneered in lung transplantation and management of cystic fibrosis, such as inhaled amphotericin, tobramycin, and rotating antibiotics have not been tested in chronic GVHD but might be considered for individual patients with frequent repetitive infections.
Lung transplantations have been performed in a small number of patients for the treatment of severe BOS and reports suggest the resulting BOS recurrence rates have been low. Therefore, it is reasonable to discuss this option with a thoracic transplantation specialist for HCT recipients whose underlying malignancy is in remission or if transplantation was done for non-malignant indications.
For specific dispensing information, please see Supplement 7.
HEMATOPOIETIC SYSTEM
Cytopenias may be caused by stromal damage, graft failure, drug toxicity, infection, relapse of underlying disease, CMV infection, hemolysis, the anemia of chronic disease, and autoimmune processes, including GVHD [77–80]. Intravenous immunoglobulin may be effective in certain cytopenias that have not improved after steroid treatment [78,80] (Table 9). Growth factor use has not been formally evaluated in chronic GVHD patients with persistent cytopenias. Thrombocytopenia at the time of diagnosis of chronic GVHD is associated with poor prognosis [81,82] but may also be caused by autoantibodies that would respond to treatment with steroids or rituximab. Eosinophilia can occur with either acute or chronic GVHD [83,84]. In patients with chronic GVHD, eosinophilia has been associated with elevated serum levels of IL-5 [85] and can herald or represent disease activity [86]. Emerging data suggest that the terminal complement inhibitor eculizumab could have a role in the treatment of HCT-associated thrombotic microangiopathy [87,88].
Table 9.
Ancillary Therapy And Supportive Care Recommendations for the Hematopoietic System
| Type of Intervention | Rating |
|---|---|
| Growth factors (G-CSF, GM-CSF, erythropoietin) | CIII |
| Immunoglobulin for cytopenias | CIII |
| Eculizumab for thrombotic microangiopathy | CIII |
|
| |
| PEDIATRIC CONSIDERATIONS No substantive differences. | |
G-CSF indicates granulocyte colony–stimulating factor; GM-CSF, granulocyte macrophage colony–stimulating factor.
NEUROLOGIC SYSTEM
Chronic GVHD of the nervous system is rare but can present as polyneuropathy, myositis and myasthenia [89]. Symptoms may include muscle weakness and wasting, pain, burning, dysesthesias, and parasthesias. Less clearly associated with chronic GVHD are central nervous system manifestations, such as cerebral angiitis and vasculitis or encephalitis-like disease [90,91]. In contrast, muscle cramps are a relatively common symptom but not necessarily directly attributable to chronic GVHD.
Neuropathy and Myopathy
Painful neuropathy and myopathy can occur in patients with chronic GVHD [89]. Consideration of chronic inflammatory demyelinating polyneuropathy may require cerebrospinal fluid examination, electromyography (EMG) studies, and sural nerve biopsy if symptoms present without other evidence of chronic GVHD [89,92]. EMG, including nerve conduction studies, is also useful in measuring the severity and progress of peripheral neuropathy. Neuropathic pain can occur in a dermatomal distribution in the absence of rash during the prodromal phase of varicella zoster virus (VZV) reactivation. Specific interventions for painful peripheral neuropathies may include the use of tricyclic antidepressants [93], selective serotonin reuptake inhibitors [94], and anticonvulsants [95] (Table 10). Opioid analgesics are poorly effective as a solitary approach for relieving neuropathic pain, but they may provide some relief and can be an important adjunct to treatment when other approaches provide inadequate relief [96]. Because of untoward side effects, such as sedation, these medications may need to be titrated up slowly, as tolerated by the patient, until symptoms are adequately controlled. Rehabilitation medicine consultation with physical and occupational therapy should be considered for all patients who have a decreased ability to perform activities of daily living or impaired quality of life because of pain or muscle weakness. Falls are more prevalent among patients with proximal myopathy or those with distal weakness and poor proprioception due to neuropathy; the latter may require orthotic support [97]. Insensate distal extremities are also at risk for skin breakdown and wound infection from trauma, even mild, that goes unnoticed. Therefore, when distal sensory loss is present, frequent skin checks are advised either by the patient, a caregiver, or the medical team.
Table 10.
Ancillary Therapy and Supportive Care Recommendations for Neurologic Syndromes of GVHD
| Type of Intervention | Rating |
|---|---|
| Neuropathies: | |
| Tricyclic antidepressants (eg, amitriptyline) | BIIb |
| SSRI (eg, citalopram) | CIIb |
| Anticonvulsants (eg, gabapentin, pregabalin) | BIb |
| Bracing/splinting [102] | BIb |
| Surgical release | BIb |
| Muscle cramps: | |
| Baclofen | CIII |
| Clonazepam or diazepam (in the evening or at bedtime) | CIII |
| Cyclobenzoprine (short term use: 2–3 wk) | CIII |
| Ropinirole (1–3 hours before bedtime) | CIII |
| Quinine sulfate (FDA blackbox warning 11/2009) | EIIb |
| Neuropathies/myopathies/CNS disease | |
| Rehabilitation medicine (PM&R, PT/OT, orthotics) [103,104] | CIII |
| Plasmapheresis for TTP | BIIb |
| IVIG | BIIb |
|
| |
| PEDIATRIC CONSIDERATIONS Drugs of the SSRI antidepressant class should generally be used under expert supervision because of the increased risk of suicidal tendencies associated with their use in children. Gabapentin may be used with success for treating extremity dysesthesias or muscle cramps but experience is very limited with other agents for muscle cramps. | |
FDA indicates Food and Drug Administration; CNS, central nervous system; PT, physical therapy; OT, occupational therapy; TTP, thrombotic thrombocytopenic purpura.
GVHD also places patients at risk for entrapment mononeuropathies due to sclerosis and associated contractures, fasciitis, and decreased tissue coverage (muscle, adipose tissue) over pressure-sensitive areas. Patients should be monitored for symptoms of carpal tunnel syndrome, ulnar neuropathy at the elbow, and peroneal neuropathy at the fibular head. EMG and nerve conduction studies can diagnose and grade the severity of these mononeuropathies. Treatment may include bracing and splinting, off-loading the affected area, or surgical release.
Exercise should be encouraged based on physician recommendations or through a cancer-trained group program to maintain muscle strength. This requires strength training, not only aerobics.
Myasthenia Gravis and Polymyositis
Myasthenia gravis occurs rarely in chronic GVHD. The diagnosis is suggested by the syndrome of ptosis, extraocular muscle weakness, and proximal limb and facial weakness in the presence of antiacetylcholine receptor antibodies [98].
Polymyositis can present with proximal muscle weakness that is often painful and associated with an elevated serum concentration of creatinine phosphokinase and aldolase [99]. Isolated polymyositis occurs rarely as the sole manifestation of chronic GVHD and muscle biopsy may be required to establish the diagnosis [100,101].
Muscle Cramps
Skeletal muscle cramps of the extremities and severe carpopedal spasms, with impairment of fine motor functions, are often observed in patients with chronic GVHD. Generally, conventional muscle relaxants and analgesics are ineffective. It is important to exclude electrolyte disturbances, particularly hypomagnesemia. Various interventions have been tested (Table 10) but must be implemented in a way that accounts for the specific situation in each individual; a careful review of risks and benefits is strongly advised.
For specific dispensing information, please see Supplement 8.
IMMUNOLOGIC AND INFECTIOUS DISEASES
Infection is the most common cause of mortality in patients with chronic GVHD and infection prophylaxis requires special emphasis. The immune defects in chronic GVHD are broad, encompassing macrophage function, antibody production, and T cell function. Prevention, early diagnosis, and prompt treatment of infections are essential to the supportive care of patients with chronic GVHD. Recommendations supported by published evidence are more often based on results from studies with patients who had conditions other than chronic GVHD. Comprehensive guidelines for the prevention of opportunistic infections after HCT have been published in collaboration by the Center for Disease Control, the Infectious Disease Society of America, and the American Society of Blood and Marrow Transplantation [105,106].
Antibacterial Prophylaxis
Patients with chronic GVHD are considered at risk for infection with encapsulated bacteria, particularly Streptococcus pneumoniae, but also Haemophilus influenzae and Neisseria meningitides. Encapsulated organism prophylaxis should be given to all patients with chronic GVHD while systemic immunosuppressive treatment is being given (Table 11). Optimal selection of prophylaxis considers local patterns of pneumococcal resistance and individual allergies or toxicities associated with available antibiotic choices that include penicillin, cotrimoxazole, second-generation cephalosporins, quinolones, and azithromycin. None of these strategies have been tested in randomized trials but historical data indicate that fulminant septic events can occur without prophylaxis due to the profound immunosuppression. When pneumococcal resistance patterns permit, a daily cotrimoxazole regimen can provide prophylaxis against Pneumocystis jirovecii pneumonia (PJP), pneumococcus, and to some extent toxoplasmosis and nocardia.
Table 11.
Ancillary Therapy and Supportive Care Recommendations for Immunologic and Infectious Complications of Chronic GVHD
| Type of Intervention | Recommendation Rating |
|---|---|
| Antibacterial prophylaxis | |
| Antibiotic prophylaxis for encapsulated organisms: | |
| Penicillin Vee-K (if supported by resistance patterns) | BIIb |
| Alternatives: cotrimoxazole, second generation cephalosporins, quinolones and azithromycin | CIII |
| Pneumococcal vaccine | BIIb |
| Hib vaccine | BIIb |
| IVIG routinely after allogeneic HCT | D |
| IVIG in patients with severe hypogammaglobulinemia and repeated sinopulmonary infections | CIII |
| Antibiotic prophylaxis before dental extractions and other invasive procedures | CIII |
| Antifungal prophylaxis | |
| Prophylaxis for Candida infection | CIII |
| Primary prophylaxis with agents with activity against mould if prednisone >0.5–1 mg/kg/day | AIa |
| Secondary prophylaxis with pathogen specific agent for prior history of mold | CIII |
| Pneumocystis jirovecii antibiotic prophylaxis | AIb |
| Antiviral prophylaxis | |
| HSV prophylaxis | D |
| VZV prophylaxis | CIa |
| CMV prophylaxis in seropositive cord blood recipients during the first year after transplantation | CIIa |
| Influenza vaccination with killed vaccine | BIII |
| Early empirical treatment with oseltamivir during influenza outbreaks | CIII |
|
| |
| PEDIATRIC CONSIDERATIONS Children undergoing HCT have frequently missed routine childhood immunizations. Review of immunization history and patient-specific vaccination is indicated. Heptavalent conjugated pneumococcal vaccine is recommended at 12 and 14 mo after HCT for patients less than or equal to 5 yr of age. It is also recommended that children between 2–5 yr of age receive one dose of the 23-valent pneumococcal vaccine 2 mo after the last dose of the heptavalent conjugated vaccine. Patients with primary immunodeficiency diseases (examples: severe combined immunodeficiency disease, Wiskott Aldrich syndrome, IPEX syndrome, and chronic granulomatous disease), regardless of their serum immunoglobulin levels, have never completed a primary immunization series at the time of transplantation. Defects in T cell and B cell collaboration often exist such that serum immunoglobulins may be functionally defective. After transplant, B cell numbers are variably restored; mixed donor T and B cell chimerism may also complicate restoration of functional immunoglobulins. Centers that specialize in HCT for PID typically advocate maintaining serum trough IgG levels of 600 to 800 mg/dL. | |
Hib indicates Haemophilus influenzae type b.
Antibiotic prophylaxis before dental extractions and other invasive procedures in patients with chronic GVHD has not been studied and consensus on this subject has not been reached (see also above under “Routine dental cleaning”).
Vaccinations
Although no studies have evaluated the degree of protection provided by vaccination against encapsulated organisms in patients with chronic GVHD, expert consensus opinion advocates their use beginning as early as 3 to 6 months after transplantation, as the T cell–dependent conjugated vaccines are more effective than the older polysaccharide vaccines and the risk of adverse outcomes with vaccination is low [105,106]. Nonetheless, some centers require an arbitrary numeric level of immune reconstitution if vaccinations for pneumococcus, H. influenzae type b, and N. meningitides are given before 1 year after transplantation (eg, serum IgG level > 400 mg/dL, CD4 T cells > 200/μL, and CD19 B cells > 20/μL). Vaccination with trivalent influenza vaccine but never the live attenuated influenza vaccine is advised for all recipients who are at least 6 months out from HCT, and in the midst of an influenza epidemic, as early as 4 months after HCT. Inactivated influenza vaccine is also recommended for all close contacts. No live virus vaccine should be given, including the live attenuated measles, mumps, rubella, varicella, and zoster vaccines. Household contacts should not be given oral polio vaccine.
Intravenous Immunoglobulin
Universal administration of intravenous immunoglobulin (IVIG) after HCT has not been shown to confer clinical benefit and should be avoided [107,108]. In patients with hypogammaglobulinemia caused by other disorders, administration of IVIG to maintain IgG levels above 400 mg/dL has been associated with a reduced incidence of severe bacterial infections [109–111]. IVIG may be considered for patients who have recurrent sinopulmonary infections and serum IgG levels < 400 mg/dL > 90 days after HCT. Some experts recommend monitoring IgG levels and administering IVIG routinely in chronic GVHD, but there are no data demonstrating that this approach improves outcomes.
Antifungal Prophylaxis
Invasive mold infections are a significant risk for patients with severe cell-mediated immunodeficiency caused by chronic GVHD and its treatment. Although controversies remain about the appropriate duration of therapy, dosing and drug levels, drug interactions, and resistant breakthrough infections, many centers prescribe primary prophylaxis with posaconazole [112] or voriconazole for patients considered at high-risk for invasive mold infections, such as those with chronic GVHD treated with higher doses of steroids (>0.5 to 1.0 mg/kg/day). Most centers also prescribe secondary prophylaxis during systemic corticosteroid therapy for chronic GVHD. Selection of an appropriate prophylactic drug is based on the specific pathogen that caused the previous invasive mold infection and the response to antifungal therapy during that episode.
Pneumocystis Jirovecii Prophylaxis
PJP more than 6 months after HCT is strongly associated with chronic GVHD. All patients should receive PJP prophylaxis during immunosuppressive treatment after allogeneic HCT [106]. The optimal duration of continued prophylaxis after stopping immunosuppression has not been defined, and practices vary widely among centers. The first choice of prophylaxis for PJP is trimethoprim-sulfamethoxazole. Alternatives include dapsone, atovaquone, and aerosolized or intravenous pentamidine, although pentamidine has appeared inferior to other regimens [113].
Antiviral Prophylaxis
Approximately 30% to 60% of patients experience an episode of zoster during the first year after discontinuing post-transplantation prophylaxis [114]. Some experts use long-term antiviral prophylaxis to prevent recurrent HSV and VZV infection among HCT recipients with severe, long-term immunodeficiency [115–117], but current evidence does not support routine administration of antiviral prophylaxis for HSV in patients with chronic GVHD. If a patient with chronic GVHD is exposed to varicella (either primary or post-vaccination illness), VZV immunoglobulin, if available, should be given within 96 hours, or valacyclovir may be given until 22 days from exposure.
The optimal strategy to monitor and treat CMV after day +100 has not been defined. Patients who begin chronic GVHD therapy who also have lymphopenia and/or a history of CMV reactivation during the first 3 months after HCT are at higher risk of late CMV reactivation and death [118]. Some centers continue to monitor for CMV viremia after day 100 by weekly or every other week PCR testing based on individual risks, followed by pre-emptive therapy, as follows:
CMV seronegative (both donor and recipient): no prophylaxis or viremia checks.
- CMV seropositive (either donor or recipient)
-
○No prior history of CMV infection: CMV viremia testing every 1 to 4 weeks
-
○History of CMV infection or disease: weekly CMV viremia testing and pre-emptive treatment as during the first 100 days
-
○Because of the high risk for CMV reactivation among seropositive cord blood recipients, some centers recommend prophylaxis with valganciclovir after day 100 until 1 year after transplantation [119].
-
○
Some investigators advocate early empirical treatment of influenza with neuraminidase inhibitors during influenza outbreaks, using prediction rules based on symptoms and signs [120,121] although no evidence is available to support this practice.
For specific dispensing information, please see Supplement 9.
MUSCULOSKELETAL
Musculoskeletal complications after HCT are caused by chronic GVHD and its treatment with corticosteroids. The most frequent problems include fasciitis, sclerotic contractures and limitation in the ROM, steroid-induced myopathy, and osteoporosis. The topic of fasciitis and sclerotic changes has been partially covered under Skin and Appendages.
This section will focus on rehabilitation for disorders of mobility associated with fasciitis, contractures, and steroid myopathy, and on prevention and management of osteopenia/osteoporosis and avascular necrosis.
Rehabilitation in Patients with Chronic GVHD
Impairments such as joint contractures, limb swelling, muscle atrophy, and weakness are often seen in chronic GVHD. Functional loss associated with these impairments includes decreased mobility, fatigue, decreased ability to perform activities of daily living or work-related activities [122,123]. Assessment of the patient depends on comprehensive neuromusculoskeletal examination testing strength, ROM of affected joints, limb girth, pain, mobility, stamina, activities of daily living, and subjective measures of disability (Table 12). Whenever possible, treatment should be aimed at early intervention and prevention of severe joint contractures and deconditioning. Restoration of ROM, strength, and mobility and relief of pain are some of the essential rehabilitation goals [124–126]. Options include aggressive physical therapy and a home-based exercise program, along with strong encouragement and provision of resources for regular strength training and aerobics. These considerations emphasize the importance of multidisciplinary teams in managing chronic GVHD, with important contributions sometimes being needed from physical medicine and rehabilitation (PM&R), as well as physical and occupational therapy.
Table 12.
Ancillary Therapy and Supportive Care Recommendations for Fasciitis, Contractures, Steroid Myopathy, and Avascular Necrosis
| Type of Intervention | Rating |
|---|---|
| Fasciitis/Contractures | |
| Refer to PT for quantitative ROM measurements, to provide the patient with stretching exercises and to monitor progress. | AIII |
| Evaluation of ROM at each clinic visit. | AIII |
| Daily stretching exercises at home | AIII |
| PT stretching 2–3 times a wk (severe impairment) | AIII |
| Surgical release | DIII |
| Steroid myopathy and deconditioning | |
| Strengthening: isometric, isotonic, isokinetic exercise | AII |
| Decreased stamina: aerobic exercise should be progressive with increase in duration and resistance to achieve elevated heart rate | AIII |
| Avascular necrosis | |
| Nonoperative management in more advanced cases (bracing, crutches, intra-articular steroids, oral medications) | DIIb |
| Surgical management, including joint replacement | BIIb |
|
| |
| PEDIATRIC CONSIDERATIONS In children, a major goal is to avoid early replacement with artificial joints that have a finite lifespan. Therefore, therapy for moderate to severe AVN in children involves appropriate chronic analgesia and a variety of temporizing surgical interventions including core decompression, partial or total hip resurfacing at centers specializing in these approaches. | |
Patients with chronic glucocorticoid use are at risk of developing avascular necrosis (AVN), with the femoral and humeral heads being commonly involved. AVN results from the destruction of the bony vasculature, and damage that involves collapse of the articular surface is generally progressive and permanent. Plain films of the joints can be diagnostic, whereas magnetic resonance imaging is more sensitive and typically the investigation of choice in the setting of high clinical suspicion and normal x-ray findings. AVN can lead to painful joints with restricted ROM. Nonsurgical interventions are generally ineffective, except for in patients with asymptomatic AVN and less than 15% bony involvement on radiographs. In patients who are healthy enough to tolerate surgery, joint replacement should be considered [127].
Prevention and Management of Osteoporosis
Bone mineral metabolism is disturbed following allogeneic HCT, even beyond 6 years [128–131]. Abnormalities include increased bone resorption and decreased bone formation, with consequent osteopenia and, less frequently, osteoporosis [132–134]. The recommendations for prevention and treatment of osteoporosis in patients with chronic GVHD are based on experience with osteoporosis in other diseases such as breast and prostate cancer, and on expert consensus (Table 13).
Table 13.
Recommendations for Prevention and Management of Osteoporosis
| Recommendation | Rating |
|---|---|
| Calcium and vitamin D replacement in deficient states, post-menopausal women, and all at high risk of deficiency | AIb |
| Antiresorptive therapy when prolonged corticosteroid administration (>3 mo) | AIIb |
| Antiresorptive therapy | |
| In patients off steroids, T-score ≤ −1.5 with other potential fracture risks (consider FRAX or FORE risk calculators) | AIIb |
| In patients with higher T-scores | DIII |
| Weight-bearing exercise | AIIb |
| Spinal orthosis for unstable compression fractures | AIIb |
|
| |
| PEDIATRIC CONSIDERATIONS The definition of reduced BMD in children uses age and sex- normalized standard-deviation scores (Z-scores) rather than T scores. The diagnosis of osteoporosis requires the presence of clinically significant fracture history and a BMD Z-score < −2.0. The incorrect application of T-scores to children may lead to inappropriate misdiagnosis and over-treatment. The use of bisphosphonates in children remains controversial because of inadequate long-term efficacy and safety data. Therefore, many experts limit their use to those children with reduced BMD, recurrent extremity fractures, and/or symptomatic vertebral collapse; most experience is with pamidronate. | |
In patients with chronic GVHD, a baseline calcium (total and ionized) and vitamin D level should be measured. These tests should be repeated at least annually when normal or as clinically indicated when abnormal or predicted to become abnormal. The consideration of secondary causes of osteoporosis at this stage is also critical. Referral to an endocrinologist is warranted whenever an endocrine, secondary cause of osteoporosis, such as hyperparathyroidism, is suspected [130].
Bone mineral density (BMD) measurement by dual-energy x-ray absorptiometry scans is recommended in patients with chronic GVHD. The resulting T score indicates the number of standard deviations above or below the average BMD for average healthy young adults. T scores < −1.5 indicate osteopenia, and T scores < −2.5 indicate osteoporosis. BMD studies should be repeated yearly for the first 3 years after HCT, and if BMD is stable, every 2 to 3 years thereafter [130]. The online “FRAX” or “FORE” 10-year fracture risk calculators are available to help guide the need for antiresorptive therapy in adults, but these have not been validated specifically for the HCT population: FRAX (http://www.shef.ac.uk/FRAX/tool.aspx), FORE (https://riskcalculator.fore.org).
Management consists of calcium and vitamin D supplementation and antiresorptive therapy.
Calcium and vitamin D
Replacement is justified in deficient states or when patients are post-menopausal or at high risk of developing deficiency [135,136] but is not adequate in patients with osteoporosis [137].
Antiresorptive therapy
In patients where steroid therapy is expected to last more than 3 months, a BMD study should be performed and antiresorptive therapy should strongly be considered especially in adults at high risk for fractures (see aforementioned dental considerations in oral section). Preferred antiresorptive therapy includes hormonal replacement in those who are deficient and, in females between menarche and approximately 50 years of age, or bisphosphonates [137–139]. Secondary options include raloxifene or calcitonin [137]. Newer agents include teriparatide, for which there is randomized controlled data in non-HCT settings [140], and denosumab, for which there are randomized trials in non-cancer patients and phase II trials in cancer patients [141]. However, the lack of experience after HCT led the working group to recommend endocrine consultation when preferred options cannot be used.
In patients who are not taking steroids for extended periods of time, recommendations are based on BMD T scores. Antiresorptive therapy is frequently indicated if the BMD T score is < −1.5. Patients with T scores > −1.5 should be followed closely with BMD studies yearly for 3 years, and if stable, every 2 to 3 years thereafter.
Weight-bearing exercise
Weight-bearing exercise, such as walking in 20- to 30-minute bursts with rest periods in between, improves bone density in osteopenic and osteoporotic patients [142]. Referral to a physical therapist or PM&R physician should be considered in patients who cannot perform this routine independently.
Vertebral compression fractures
Spinal orthotic bracing should be initiated if intractable pain or evidence of neurologic compromise are present or if the spine is unstable. Early mobilization with the brace and tight pain control are the first priority in management of these patients. A consult with a spine surgeon and PM&R physician should be strongly considered.
For specific dispensing information, please see Supplement 10.
PSYCHOSOCIAL
Studies of late effects in patients after allogeneic HCT suggest that chronic GVHD produces deleterious consequences for multidimensional functioning and quality of life [143–145]. Patients with chronic GVHD report significantly more fatigue, pain, bowel changes, and dyspareunia than those without chronic GVHD [145,146]. Lower physical, sexual, and psychosocial functioning [144,145,147,148], along with a lower likelihood of returning to work, are common in patients with chronic GVHD, and patients with more severe chronic GVHD have impaired physical and psychosocial recovery both at 1 year after HCT [149] and long term [150].
Chiodi et al. [151] reported that chronic GVHD was the most important factor influencing diminished vocation and domestic role function, negatively affecting family interactions and social activities. Corticosteroid treatment was independently associated with global distress [152]. Some of the more prevalent psychosocial domains associated with chronic GVHD include neurocognitive impairment, depression, anxiety, altered body image, sexual dysfunction, and fatigue [145,152–154].
Neurocognitive Functioning, Depression, and Anxiety
Neurocognitive performance for motor dexterity, processing speed, executive functioning, and memory [155] is below population averages in 20% to 40% of adults immediately before HCT. Cognitive performance usually declines further shortly after HCT yet recovers to its immediate pre-transplantation levels in most patients by 1 year [154]. However, by 5 years after transplantation, 38% continue to show mild impairment and 3% moderate impairment, primarily in motor dexterity, verbal learning, and memory [154]. Chronic GVHD has not been associated with any specific intellectual function deficits, and immunosuppressive medications have not been specifically examined as risk factors. The research on pediatric neurocognitive performance is mixed. Some studies document no cognitive effects of transplantation, whereas others point to immediate or slowly evolving impairment over time, mostly in processing speed, attention, visual memory, and fine motor coordination [156–160]. Contributing factors may include total body irradiation conditioning regimen, young age at HCT, and severity of GVHD [161].
Neuropsychological assessment may be helpful when individuals perceive cognitive impairment in a nonspecific way and clarity is needed to guide rehabilitative efforts. However, consensus on the recommended test battery has not yet been reached [162]. Because self-reported neurocognitive function does not correlate reliably with objective measures [163], adults should be referred for full neuropsychological evaluation if warranted by initial screening or by persisting concerns that cognition is disrupting functioning rather than for general complaints of impaired cognition (Table 14). For children, HCT potentially interrupts development and even mild impairment may be compounded over time by chronic GVHD or illness-related lack of opportunity to learn and practice skills. Therefore, in children, neuropsychological evaluation at 1 year and annual targeted brief screenings thereafter are advisable if any cognitive or learning deficits are identified.
Table 14.
Ancillary Therapy and Supportive Care Recommendations for Psychosocial Issues
| Type of Intervention | Rating |
|---|---|
| Brief neuropsychological testing if symptoms of cognitive deficits disrupt daily activities and safety | BII |
| Depression, anxiety and transplantation-related worry or distress: screen before transplantation, at 6 and 12 mo, and then annually with referral for cognitive, behavioral interventions, or psychiatry assessment if indicated. | BII |
| Education for all adults at discharge on the importance of return to sexual activity, use of lubricants for women, and regular exercise for management of sexual functioning, body image, sleep, fatigue and musculoskeletal symptoms. Query at 6 and 12 mo, then annually with medical evaluation or referral to supportive and cognitive behavioral interventions if indicated. | CIII |
| Regularly assess level of caregiver psychological adjustment and functioning. | CIII |
|
| |
| PEDIATRIC CONSIDERATIONS Neuropsychological evaluation is recommended if cognitive deficits are suspected. For mood, behavioral, academic, and adaptive functioning difficulties, screen before transplantation, at 6 and 12 mo, and then annually with referral for cognitive behavioral interventions as indicated. For body image issues and fatigue, query at 6 and 12 mo, and then annually with referral for cognitive behavioral and supportive interventions as indicated. Attend to timing for addressing sexual function needs as adolescents develop. | |
Depressive symptoms are associated with chronic GVHD and are more severe and longer term among those with extensive chronic GVHD [145]. Depressed mood warrants careful regular monitoring because it is the principal factor associated with suicidal ideation, it is associated with multiple other negative outcomes, and can be effectively treated [152]. The risk of suicide is greater in HCT survivors compared with that in the general population, and among allogeneic HCT survivors, chronic GVHD increases this risk by almost 3-fold [164,165].
Sexual Dysfunction
Many patients acknowledge interruption of sexual activity and sexual difficulties for prolonged periods of time after HCT. Recovery of sexual activity and quality of sexual function generally occurs within 2 years after HCT for men but may persist longer or be permanent for women and for some men [166]. Over 40% of females remain sexually inactive even 5 years after treatment [167], and chronic GVHD increases this risk for both men and women [168]. Contributing factors include GVHD of the skin and genitalia, hormonal changes, and glucocorticoid therapy [147,169]. Phosphodiesterase type 5 inhibitors for men and brief therapeutic options for sexual dysfunction in this population are understudied but are beginning to demonstrate efficacy in other cancer populations [170–172]. Education on use of lubricants should be universal for women after HCT. Dilators or vibrators may be necessary to maintain or improve vaginal dilation in women with chronic GVHD. Encouraging gradual resumption of sexual activities is also important. Behavioral treatments help to address a variety of problems. These treatments can improve communication and intimacy and help overcome anxiety about sexual desirability and concerns about performance [147]. Hormone evaluation and the need for hormone therapy warrant consultation with gynecology or endocrinology as indicated.
Fatigue and Musculoskeletal Symptoms
Although the biochemical, physiological, psychological, and behavioral mechanisms of fatigue are not fully understood [173], fatigue is a prevalent and distressing symptom for many years after allogeneic HCT [150,174]. Over two thirds of 5-year transplantation survivors report moderate to severe fatigue, muscle weakness or myalgias, and muscle cramps [175] (see also Table 10). Patients with ongoing chronic GVHD have significantly worse fatigue than those without a history of GVHD or those whose GVHD had resolved, in the absence of significant differences in sleep disturbance between groups [146]. Immunosuppressive agents used to treat or prevent GVHD may differentially contribute to fatigue [176].
Management of fatigue and musculoskeletal symptoms includes a gradually increasing exercise regimen, activity pacing, other cognitive behavioral strategies, and sometimes medication. Detailed recommendations are available in the National Comprehensive Cancer Network Clinical Practice Cancer Survivorship Guidelines [177].
Behavioral Interventions
Survivors with chronic GVHD often have unrecognized psychological, functional, or adjustment difficulties. The small evidence base for interventions for psychosocial issues after HCT is limited to cognitive-behavioral interventions [178,179], which have demonstrated efficacy [179]. Mindfulness and cognitive behavioral stress-reduction interventions have shown promise in cancer patients [180,181] in general and could be helpful for patients coping with chronic GVHD.
Supplementary Material
Acknowledgments
This project was supported by the National Institutes of Health’s (NIH) National Cancer Institute, Center for Cancer Research, Intramural Research Program and Division of Cancer Treatment and Diagnosis, Cancer Therapy Evaluation Program; Office of Rare Disease Research, National Center for Advancing Translational Sciences; Division of Allergy, Immunology and Transplantation, National Institute of Allergy and Infectious Disease; National Heart, Lung, and Blood Institute, Division of Blood Diseases and Resources. The authors want to acknowledge the following individuals and organizations that, by their participation, made this project possible: American Society for Blood and Marrow Transplantation, Center for International Bone and Marrow Transplant Research, US Chronic GVHD Consortium (supported by ORD and NCI), German-Austrian-Swiss GVHD Consortium, National Marrow Donor Program, the Health Resources and Services Administration, Division of Transplantation, US Department of Human Health and Services, Canadian Blood and Marrow Transplant Group, European Group for Blood and Marrow Transplantation, Pediatric Blood and Marrow Transplant Consortium, and the representatives of the Brazilian Chronic GVHD consortium (Drs. Maria Claudia Moreira, Marcia and Vaneuza Funke) and Deutsche José Carreras Leukämie-Stiftung. The organizers are in debt to patients and patient and research advocacy groups, who made this process much more meaningful by their engagement. Acknowledgement goes to the Meredith Cowden GVHD foundation for facilitating the initial planning meeting in Cleveland in November of 2013 in conjunction with the National GVHD Symposium. The project group also recognizes the contributions of numerous colleagues in the field of blood and marrow transplantation in the US and internationally, medical specialists and consultants, the pharmaceutical industry, and the NIH and US Food and Drug Administration professional staff for their intellectual input, dedication, and enthusiasm on the road to completion of these documents. Project participants also recognize Drs. Joseph Antin and Gerard Socie for their independent expert reviews and comments on final documents at the June 2014 meeting.
APPENDIX 1. EVIDENCE-BASED RATING SYSTEM FOR ANCILLARY THERAPY AND SUPPORTIVE CARE GUIDELINES IN CHRONIC GVHD
| Strength of the Recommendation: | |
| Category | Definition |
| A | Should always be offered. |
| B | Should generally be offered. |
| C | Evidence for efficacy is insufficient to support a recommendation for or against, or evidence for efficacy might not outweigh adverse consequences, or cost of the approach. Optional. |
| D | Moderate evidence for lack of efficacy or for adverse outcome supports a recommendation against use. Should generally not be offered. |
| E | Good evidence for lack of efficacy or for adverse outcome supports a recommendation against use. Should never be offered. |
| Quality of Evidence Supporting the Recommendation: | |
| Category | Definition |
| I | Evidence from at least one properly randomized, controlled trial. |
| II | Evidence for at least one well-designed clinical trial without randomization, from cohort or case-controlled analytic studies (preferable from more than one center) or from multiple time-series or dramatic results from uncontrolled experiments. |
| III | Evidence from opinions of respected authorities based on clinical experience, descriptive. |
| Qualifier for Categories I and II | |
| a | Evidence derived directly from study(s) in GVHD |
| b | Evidence derived indirectly from study(s) in analogous or other pertinent disease |
APPENDIX 2. NATIONAL INSTITUTES OF HEALTH CONSENSUS-DEVELOPMENT PROJECT ON CRITERIA FOR CLINICAL TRIALS IN CHRONIC GVHD STEERING COMMITTEE
Members of this committee included: Steven Pavletic, Georgia Vogelsang and Stephanie Lee (project chairs), Mary Flowers and Madan Jagasia (Diagnosis and Staging), David Kleiner and Howard Shulman (Histopathology), Kirk Schultz and Sophie Paczesny (Biomarkers), Stephanie Lee and Steven Pavletic (Response Criteria), Dan Couriel and Paul Carpenter (Ancillary and Supportive Care), Paul Martin and Corey Cutler (Design of Clinical Trials), Kenneth Cooke and David Miklos (Chronic GVHD Biology), Roy Wu, William Merritt, Linda Griffith, Nancy DiFronzo, Myra Jacobs, Susan Stewart, Meredith Cowden (members).
Footnotes
Disclaimer: The opinions expressed here are those of the authors and do not represent the official position of the NIH, FDA or the United States Government.
Financial disclosure: The authors have nothing to disclose.
Conflict of interest statement: There are no conflicts of interest to report.
SUPPLEMENTARY DATA
Supplementary data related to this article can be found at http://dx.doi.org/10.1016/j.bbmt.2015.03.024.
References
- 1.Majhail NS, Rizzo JD, Lee SJ, et al. Recommended screening and preventive practices for long-term survivors after hematopoietic cell transplantation. Rev Bras Hematol Hemoter. 2012;34:109–133. doi: 10.5581/1516-8484.20120032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Inamoto Y, Savani BN, Shaw BE, et al. Secondary solid cancer screening following hematopoietic cell transplantation. Bone Marrow Transplant. 2015 doi: 10.1038/bmt.2015.63. http://dx.doi.org/10.1038/bmt.2015.63. [Epub ahead of print] [DOI] [PMC free article] [PubMed]
- 3.Majhail NS, Rizzo JD, Lee SJ, et al. Recommended screening and preventive practices for long-term survivors after hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2012;18:348–371. doi: 10.1016/j.bbmt.2011.12.519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Smith EM, Pang H, Cirrincione C, et al. Effect of duloxetine on pain, function, and quality of life among patients with chemotherapy-induced painful peripheral neuropathy: a randomized clinical trial. JAMA. 2013;309:1359–1367. doi: 10.1001/jama.2013.2813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kitajima T, Imamura S. Graft-versus-host reaction enhanced by ultraviolet radiation. Arch Dermatol Res. 1993;285:499–501. doi: 10.1007/BF00376823. [DOI] [PubMed] [Google Scholar]
- 6.Patel AR, Turner ML, Baird K, et al. Voriconazole-induced phototoxicity masquerading as chronic graft-versus-host disease of the skin in allogeneic hematopoietic cell transplant recipients. Biol Blood Marrow Transplant. 2009;15:370–376. doi: 10.1016/j.bbmt.2008.12.491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Vogelsang GB, Wolff D, Altomonte V, et al. Treatment of chronic graft-versus-host disease with ultraviolet irradiation and psoralen (PUVA) Bone Marrow Transplant. 1996;17:1061–1067. [PubMed] [Google Scholar]
- 8.Leiter U, Kaskel P, Krahn G, et al. Psoralen plus ultraviolet-A-bath photochemotherapy as an adjunct treatment modality in cutaneous chronic graft versus host disease. Photodermatol Photoimmunol Photomed. 2002;18:183–190. doi: 10.1034/j.1600-0781.2002.00719.x. [DOI] [PubMed] [Google Scholar]
- 9.Hymes SR, Morison WL, Farmer ER, et al. Methoxsalen and ultraviolet A radiation in treatment of chronic cutaneous graft-versus-host reaction. J Am Acad Dermatol. 1985;12:30–37. doi: 10.1016/s0190-9622(85)70005-9. [DOI] [PubMed] [Google Scholar]
- 10.Wetzig T, Sticherling M, Simon JC, et al. Medium dose long-wavelength ultraviolet A (UVA1) phototherapy for the treatment of acute and chronic graft-versus-host disease of the skin. Bone Marrow Transplant. 2005;35:515–519. doi: 10.1038/sj.bmt.1704804. [DOI] [PubMed] [Google Scholar]
- 11.Enk CD, Elad S, Vexler A, et al. Chronic graft-versus-host disease treated with UVB phototherapy. Bone Marrow Transplant. 1998;22:1179–1183. doi: 10.1038/sj.bmt.1701460. [DOI] [PubMed] [Google Scholar]
- 12.Grundmann-Kollmann M, Martin H, Ludwig R, et al. Narrowband UV-B phototherapy in the treatment of cutaneous graft versus host disease. Transplantation. 2002;74:1631–1634. doi: 10.1097/00007890-200212150-00023. [DOI] [PubMed] [Google Scholar]
- 13.Elad S, Or R, Resnick I, Shapira MY. Topical tacrolimus–a novel treatment alternative for cutaneous chronic graft-versus-host disease. Transpl Int. 2003;16:665–670. doi: 10.1007/s00147-003-0594-2. [DOI] [PubMed] [Google Scholar]
- 14.Ziemer M, Gruhn B, Thiele JJ, Elsner P. Treatment of extensive chronic cutaneous graft-versus-host disease in an infant with topical pimecrolimus. J Am Acad Dermatol. 2004;50:946–948. doi: 10.1016/j.jaad.2004.02.010. [DOI] [PubMed] [Google Scholar]
- 15.Schubert MM, Correa ME. Oral graft-versus-host disease. Dent Clin North Am. 2008;52:79–109. viii–ix. doi: 10.1016/j.cden.2007.10.004. [DOI] [PubMed] [Google Scholar]
- 16.Mays JW, Fassil H, Edwards DA, et al. Oral chronic graft-versus-host disease: current pathogenesis, therapy, and research. Oral Dis. 2013;19:327–346. doi: 10.1111/odi.12028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Noce CW, Gomes A, Shcaira V, et al. Randomized double-blind clinical trial comparing clobetasol and dexamethasone for the topical treatment of symptomatic oral chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2014;20:1163–1168. doi: 10.1016/j.bbmt.2014.04.009. [DOI] [PubMed] [Google Scholar]
- 18.Eckardt A, Starke O, Stadler M, et al. Severe oral chronic graft-versus-host disease following allogeneic bone marrow transplantation: highly effective treatment with topical tacrolimus. Oral Oncol. 2004;40:811–814. doi: 10.1016/j.oraloncology.2004.02.003. [DOI] [PubMed] [Google Scholar]
- 19.Sanchez AR, Sheridan PJ, Rogers RS. Successful treatment of oral lichen planus-like chronic graft-versus-host disease with topical tacrolimus: a case report. J Periodontol. 2004;75:613–619. doi: 10.1902/jop.2004.75.4.613. [DOI] [PubMed] [Google Scholar]
- 20.Ohbayashi Y, Imataki O, Higuchi A, et al. Topical steroid injection for refractory oral chronic graft-versus-host disease. Rinsho Ketsueki. 2007;48:1508–1510. [PubMed] [Google Scholar]
- 21.Nagler R, Marmary Y, Krausz Y, et al. Major salivary gland dysfunction in human acute and chronic graft-versus-host disease (GVHD) Bone Marrow Transplant. 1996;17:219–224. [PubMed] [Google Scholar]
- 22.Schubert MM, Sullivan KM, Morton TH, et al. Oral manifestations of chronic graft-v-host disease. Arch Intern Med. 1984;144:1591–1595. [PubMed] [Google Scholar]
- 23.Woo SB, Lee SJ, Schubert MM. Graft-vs.-host disease. Crit Rev Oral Biol Med. 1997;8:201–216. doi: 10.1177/10454411970080020701. [DOI] [PubMed] [Google Scholar]
- 24.Nicolatou-Galitis O, Kitra V, Van Vliet-Constantinidou C, et al. The oral manifestations of chronic graft-versus-host disease (cGVHD) in paediatric allogeneic bone marrow transplant recipients. J Oral Pathol Med. 2001;30:148–153. doi: 10.1034/j.1600-0714.2001.300304.x. [DOI] [PubMed] [Google Scholar]
- 25.Treister N, Woo S, Lehmann LE, et al. Oral chronic graft-versus-host disease in pediatric patients following hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2005;11:721–731. doi: 10.1016/j.bbmt.2005.06.002. [DOI] [PubMed] [Google Scholar]
- 26.Schubert MM, Sullivan KM. Recognition, incidence, and management of oral graft-versus-host disease. NCI Monogr. 1990:135–143. [PubMed] [Google Scholar]
- 27.Nagler RM, Nagler A. Major salivary gland involvement in graft-versus-host disease: considerations related to pathogenesis, the role of cytokines and therapy. Cytokines Cell Mol Ther. 1999;5:227–232. [PubMed] [Google Scholar]
- 28.Nagler RM, Nagler A. Sialometrical and sialochemical analysis of patients with chronic graft-versus-host disease–a prolonged study. Cancer Invest. 2003;21:34–40. doi: 10.1081/cnv-120016401. [DOI] [PubMed] [Google Scholar]
- 29.Ruggiero SL, Dodson TB, Fantasia J, et al. American Association of Oral and maxillofacial Surgeon position paper on medication-related osteonecrosis of the jaw – 2014 update. J Oral Maxillofac Surg. 2014;72:1938–1956. doi: 10.1016/j.joms.2014.04.031. [DOI] [PubMed] [Google Scholar]
- 30.Elad S, Or R, Shapira MY, et al. CO2 laser in oral graft-versus-host disease: a pilot study. Bone Marrow Transplant. 2003;32:1031–1034. doi: 10.1038/sj.bmt.1704272. [DOI] [PubMed] [Google Scholar]
- 31.Jacobs R, Tran U, Chen H, et al. Prevalence and risk factors associated with development of ocular GVHD defined by NIH consensus criteria. Bone Marrow Transplant. 2012;47:1470–1473. doi: 10.1038/bmt.2012.56. [DOI] [PubMed] [Google Scholar]
- 32.Dietrich-Ntoukas T, Cursiefen C, Westekemper H, et al. Diagnosis and treatment of ocular chronic graft-versus-host disease: report from the German-Austrian-Swiss Consensus Conference on Clinical Practice in chronic GVHD. Cornea. 2012;31:299–310. doi: 10.1097/ICO.0b013e318226bf97. [DOI] [PubMed] [Google Scholar]
- 33.Marsh P, Pflugfelder SC. Topical nonpreserved methylprednisolone therapy for keratoconjunctivitis sicca in Sjogren syndrome. Ophthalmology. 1999;106:811–816. doi: 10.1016/S0161-6420(99)90171-9. [DOI] [PubMed] [Google Scholar]
- 34.Robinson MR, Lee SS, Rubin BI, et al. Topical corticosteroid therapy for cicatricial conjunctivitis associated with chronic graft-versus-host disease. Bone Marrow Transplant. 2004;33:1031–1035. doi: 10.1038/sj.bmt.1704453. [DOI] [PubMed] [Google Scholar]
- 35.Donnenfeld E, Pflugfelder SC. Topical ophthalmic cyclosporine: pharmacology and clinical uses. Surv Ophthalmol. 2009;54:321–338. doi: 10.1016/j.survophthal.2009.02.002. [DOI] [PubMed] [Google Scholar]
- 36.Kojima T, Ishida R, Dogru M, et al. The effect of autologous serum eyedrops in the treatment of severe dry eye disease: a prospective randomized case-control study. Am J Ophthalmol. 2005;139:242–246. doi: 10.1016/j.ajo.2004.08.040. [DOI] [PubMed] [Google Scholar]
- 37.Ogawa Y, Okamoto S, Mori T, et al. Autologous serum eye drops for the treatment of severe dry eye in patients with chronic graft-versus-host disease. Bone Marrow Transplant. 2003;31:579–583. doi: 10.1038/sj.bmt.1703862. [DOI] [PubMed] [Google Scholar]
- 38.Hill JC. Slow-release artificial tear inserts in the treatment of dry eyes in patients with rheumatoid arthritis. Br J Ophthalmol. 1989;73:151–154. doi: 10.1136/bjo.73.2.151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Ono M, Takamura E, Shinozaki K, et al. Therapeutic effect of cevimeline on dry eye in patients with Sjogren’s syndrome: a randomized, double-blind clinical study. Am J Ophthalmol. 2004;138:6–17. doi: 10.1016/j.ajo.2004.02.010. [DOI] [PubMed] [Google Scholar]
- 40.Papas AS, Sherrer YS, Charney M, et al. Successful treatment of dry mouth and dry eye symptoms in Sjogren’s syndrome patients with oral pilocarpine: a randomized, placebo-controlled, dose-adjustment study. J Clin Rheumatol. 2004;10:169–177. doi: 10.1097/01.rhu.0000135553.08057.21. [DOI] [PubMed] [Google Scholar]
- 41.Hutnik CM, Probst LE. Argon laser punctal therapy versus thermal cautery for the treatment of aqueous deficiency dry eye syndrome. Can J Ophthalmol. 1998;33:365–372. [PubMed] [Google Scholar]
- 42.Sabti S, Halter JP, Braun Frankl BC, Goldblum D. Punctal occlusion is safe and efficient for the treatment of keratoconjunctivitis sicca in patients with ocular GvHD. Bone Marrow Transplant. 2012;47:981–984. doi: 10.1038/bmt.2011.205. [DOI] [PubMed] [Google Scholar]
- 43.Altan-Yaycioglu R, Gencoglu EA, Akova YA, et al. Silicone versus collagen plugs for treating dry eye: results of a prospective randomized trial including lacrimal scintigraphy. Am J Ophthalmol. 2005;140:88–93. doi: 10.1016/j.ajo.2005.02.031. [DOI] [PubMed] [Google Scholar]
- 44.Jacobs DS, Rosenthal P. Boston scleral lens prosthetic device for treatment of severe dry eye in chronic graft-versus-host disease. Cornea. 2007;26:1195–1199. doi: 10.1097/ICO.0b013e318155743d. [DOI] [PubMed] [Google Scholar]
- 45.Takahide K, Parker PM, Wu M, et al. Use of fluid-ventilated, gas-permeable scleral lens for management of severe keratoconjunctivitis sicca secondary to chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2007;13:1016–1021. doi: 10.1016/j.bbmt.2007.05.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Schornack MM, Baratz KH, Patel SV, Maguire LJ. Jupiter scleral lenses in the management of chronic graft versus host disease. Eye Contact Lens. 2008;34:302–305. doi: 10.1097/ICL.0b013e318188e205. [DOI] [PubMed] [Google Scholar]
- 47.Filipovich AH, Weisdorf D, Pavletic S, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biol Blood Marrow Transplant. 2005;11:945–956. doi: 10.1016/j.bbmt.2005.09.004. [DOI] [PubMed] [Google Scholar]
- 48.Spinelli S, Chiodi S, Costantini S, et al. Female genital tract graft-versus-host disease following allogeneic bone marrow transplantation. Haematologica. 2003;88:1163–1168. [PubMed] [Google Scholar]
- 49.Zantomio D, Grigg AP, MacGregor L, et al. Female genital tract graft-versus-host disease: incidence, risk factors and recommendations for management. Bone Marrow Transplant. 2006;38:567–572. doi: 10.1038/sj.bmt.1705487. [DOI] [PubMed] [Google Scholar]
- 50.Flowers ME, Parker PM, Johnston LJ, et al. Comparison of chronic graft-versus-host disease after transplantation of peripheral blood stem cells versus bone marrow in allogeneic recipients: long-term follow-up of a randomized trial. Blood. 2002;100:415–419. doi: 10.1182/blood-2002-01-0011. [DOI] [PubMed] [Google Scholar]
- 51.Hirsch P, Leclerc M, Rybojad M, et al. Female genital chronic graft-versus-host disease: importance of early diagnosis to avoid severe complications. Transplantation. 2012;93:1265–1269. doi: 10.1097/TP.0b013e31824f3dcd. [DOI] [PubMed] [Google Scholar]
- 52.Stratton P, Turner ML, Childs R, et al. Vulvovaginal chronic graft-versus-host disease with allogeneic hematopoietic stem cell transplantation. Obstet Gynecol. 2007;110:1041–1049. doi: 10.1097/01.AOG.0000285998.75450.86. [DOI] [PubMed] [Google Scholar]
- 53.Spiryda LB, Laufer MR, Soiffer RJ, Antin JA. Graft-versus-host disease of the vulva and/or vagina: diagnosis and treatment. Biol Blood Marrow Transplant. 2003;9:760–765. doi: 10.1016/j.bbmt.2003.08.001. [DOI] [PubMed] [Google Scholar]
- 54.Anderson M, Kutzner S, Kaufman RH. Treatment of vulvovaginal lichen planus with vaginal hydrocortisone suppositories. Obstet Gynecol. 2002;100:359–362. doi: 10.1016/s0029-7844(02)02117-8. [DOI] [PubMed] [Google Scholar]
- 55.Cribier B, Frances C, Chosidow O. Treatment of lichen planus. An evidence-based medicine analysis of efficacy. Arch Dermatol. 1998;134:1521–1530. doi: 10.1001/archderm.134.12.1521. [DOI] [PubMed] [Google Scholar]
- 56.Sobel JD, Reichman O, Misra D, Yoo W. Prognosis and treatment of desquamative inflammatory vaginitis. Obstet Gynecol. 2011;117:850–855. doi: 10.1097/AOG.0b013e3182117c9e. [DOI] [PubMed] [Google Scholar]
- 57.Yared J, Gojo I, Akpek G. Glans penis involvement: an under-recognized manifestation of chronic GVHD. Bone Marrow Transplant. 2012;47:1006–1007. doi: 10.1038/bmt.2011.209. [DOI] [PubMed] [Google Scholar]
- 58.Applebaum FR, Forman SJ, Negrin RS, Antin JH, editors. Thomas’ Hematopoietic Cell Transplantation. 5th. Hoboken: Wiley-Blackwell; 2015. [Google Scholar]
- 59.Kida A, McDonald GB. Gastrointestinal, hepatobiliary, pancreatic, and iron-related diseases in long-term survivors of allogeneic hematopoietic cell transplantation. Semin Hematol. 2012;49:43–58. doi: 10.1053/j.seminhematol.2011.10.006. [DOI] [PubMed] [Google Scholar]
- 60.Inaba H, Yang J, Kaste SC, et al. Longitudinal changes in body mass and composition in survivors of childhood hematologic malignancies after allogeneic hematopoietic stem-cell transplantation. J Clin Oncol. 2012;30:3991–3997. doi: 10.1200/JCO.2011.40.0457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Zauner C, Rabitsch W, Schneeweiss B, et al. Energy and substrate metabolism in patients with chronic extensive graft-versus-host disease. Transplantation. 2001;71:524–528. doi: 10.1097/00007890-200102270-00007. [DOI] [PubMed] [Google Scholar]
- 62.Lenssen P, Sherry ME, Cheney CL, et al. Prevalence of nutrition-related problems among long-term survivors of allogeneic marrow transplantation. J Am Diet Assoc. 1990;90:835–842. [PubMed] [Google Scholar]
- 63.Bassim CW, Fassil H, Dobbin M, et al. Malnutrition in patients with chronic GVHD. Bone Marrow Transplant. 2014;49:1300–1306. doi: 10.1038/bmt.2014.145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Jacobsohn DA, Margolis J, Doherty J, et al. Weight loss and malnutrition in patients with chronic graft-versus-host disease. Bone Marrow Transplant. 2002;29:231–236. doi: 10.1038/sj.bmt.1703352. [DOI] [PubMed] [Google Scholar]
- 65.Chien JW, Martin PJ, Gooley TA, et al. Airflow obstruction after myeloablative allogeneic hematopoietic stem cell transplantation. Am J Respir Crit Care Med. 2003;168:208–214. doi: 10.1164/rccm.200212-1468OC. [DOI] [PubMed] [Google Scholar]
- 66.American Thoracic Society. Single-breath carbon monoxide diffusing capacity (transfer factor). Recommendations for a standard technique–1995 update. Am J Respir Crit Care Med. 1995;152:2185–2198. doi: 10.1164/ajrccm.152.6.8520796. [DOI] [PubMed] [Google Scholar]
- 67.Crapo RO, Morris AH, Gardner RM. Reference spirometric values using techniques and equipment that meet ATS recommendations. Am Rev Respir Dis. 1981;123:659–664. doi: 10.1164/arrd.1981.123.6.659. [DOI] [PubMed] [Google Scholar]
- 68.Hsu KH, Jenkins DE, Hsi BP, et al. Ventilatory functions of normal children and young adults–Mexican-American, white, and black. I. Spirometry. J Pediatr. 1979;95:14–23. doi: 10.1016/s0022-3476(79)80075-x. [DOI] [PubMed] [Google Scholar]
- 69.Williams KM, Chien JW, Gladwin MT, Pavletic SZ. Bronchiolitis obliterans after allogeneic hematopoietic stem cell transplantation. JAMA. 2009;302:306–314. doi: 10.1001/jama.2009.1018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Thompson PA, Lim A, Panek-Hudson Y, et al. Screening with spirometry is a useful predictor of later development of noninfectious pulmonary syndromes in patients undergoing allogeneic stem cell transplantation. Biol Blood Marrow Transplant. 2014;20:781–786. doi: 10.1016/j.bbmt.2014.02.011. [DOI] [PubMed] [Google Scholar]
- 71.Galban CJ, Boes JL, Bule M, et al. Parametric response mapping as an indicator of bronchiolitis obliterans syndrome after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2014;20:1592–1598. doi: 10.1016/j.bbmt.2014.06.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Bashoura L, Gupta S, Jain A, et al. Inhaled corticosteroids stabilize constrictive bronchiolitis after hematopoietic stem cell transplantation. Bone Marrow Transplant. 2008;41:63–67. doi: 10.1038/sj.bmt.1705877. [DOI] [PubMed] [Google Scholar]
- 73.Bergeron A, Belle A, Chevret S, et al. Combined inhaled steroids and bronchodilatators in obstructive airway disease after allogeneic stem cell transplantation. Bone Marrow Transplant. 2007;39:547–553. doi: 10.1038/sj.bmt.1705637. [DOI] [PubMed] [Google Scholar]
- 74.Norman BC, Jacobsohn DA, Williams KM, et al. Fluticasone, azithromycin and montelukast therapy in reducing corticosteroid exposure in bronchiolitis obliterans syndrome after allogeneic hematopoietic SCT: a case series of eight patients. Bone Marrow Transplant. 2011;46:1369–1373. doi: 10.1038/bmt.2010.311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Tran J, Norder EE, Diaz PT, et al. Pulmonary rehabilitation for bronchiolitis obliterans syndrome after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2012;18:1250–1254. doi: 10.1016/j.bbmt.2012.01.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166:111–117. doi: 10.1164/ajrccm.166.1.at1102. [DOI] [PubMed] [Google Scholar]
- 77.Bierling P, Cordonnier C, Fromont P, et al. Acquired autoimmune thrombocytopenia after allogeneic bone marrow transplantation. Br J Haematol. 1985;59:643–646. doi: 10.1111/j.1365-2141.1985.tb07359.x. [DOI] [PubMed] [Google Scholar]
- 78.Hartert A, Willenbacher W, Gunzelmann S, et al. Successful treatment of thrombocytopenia and hemolytic anemia with IvIG in a patient with lupus-like syndrome after mismatched related PBSCT. Bone Marrow Transplant. 2001;27:337–340. doi: 10.1038/sj.bmt.1702774. [DOI] [PubMed] [Google Scholar]
- 79.Keung YK, Cobos E, Bolanos-Meade J, et al. Evans syndrome after autologous bone marrow transplant for recurrent Hodgkin’s disease. Bone Marrow Transplant. 1997;20:1099–1101. doi: 10.1038/sj.bmt.1701017. [DOI] [PubMed] [Google Scholar]
- 80.Khouri IF, Ippoliti C, Gajewski J, et al. Neutropenias following allogeneic bone marrow transplantation: response to therapy with high-dose intravenous immunoglobulin. Am J Hematol. 1996;52:313–315. doi: 10.1002/(SICI)1096-8652(199608)52:4<313::AID-AJH12>3.0.CO;2-E. [DOI] [PubMed] [Google Scholar]
- 81.Akpek G. Clinical grading in chronic graft-versus-host disease: is it time for change? Leuk Lymphoma. 2002;43:1211–1220. doi: 10.1080/10428190290026268. [DOI] [PubMed] [Google Scholar]
- 82.Akpek G, Lee SJ, Flowers ME, et al. Performance of a new clinical grading system for chronic graft-versus-host disease: a multicenter study. Blood. 2003;102:802–809. doi: 10.1182/blood-2002-10-3141. [DOI] [PubMed] [Google Scholar]
- 83.Daneshpouy M, Socie G, Lemann M, et al. Activated eosinophils in upper gastrointestinal tract of patients with graft-versus-host disease. Blood. 2002;99:3033–3040. doi: 10.1182/blood.v99.8.3033. [DOI] [PubMed] [Google Scholar]
- 84.McNeel D, Rubio MT, Damaj G, et al. Hypereosinophilia as a presenting sign of acute graft-versus-host disease after allogeneic bone marrow transplantation. Transplantation. 2002;74:1797–1800. doi: 10.1097/00007890-200212270-00028. [DOI] [PubMed] [Google Scholar]
- 85.Masumoto A, Sasao T, Yoshiba F, et al. Hypereosinophilia after allogeneic bone marrow transplantation. A possible role of IL-5 overproduction by donor T-cells chronic GVHD. Rinsho Ketsueki. 1997;38:234–236. [PubMed] [Google Scholar]
- 86.Jacobsohn DA, Schechter T, Seshadri R, et al. Eosinophilia correlates with the presence or development of chronic graft-versus-host disease in children. Transplantation. 2004;77:1096–1100. doi: 10.1097/01.tp.0000118409.92769.fa. [DOI] [PubMed] [Google Scholar]
- 87.de Fontbrune FS, Galambrun C, Sirvent A, et al. Use of eculizumab in patients with allogeneic stem cell transplant-associated thrombotic microangiopathy: a study from the SFGM-TC. Transplantation. 2015 doi: 10.1097/TP.0000000000000601. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 88.Jodele S, Laskin BL, Dandoy CE, et al. A new paradigm: diagnosis and management of HSCT-associated thrombotic microangiopathy as multi-system endothelial injury. Blood Rev. 2014 doi: 10.1016/j.blre.2014.11.001. http://dx.doi.org/10.1016/j.blre.2014.11.001. [Epub ahead of print] [DOI] [PMC free article] [PubMed]
- 89.Openshaw HNS. Neurologic Complications. 2nd. Blackwell Science, Inc; 1999. [Google Scholar]
- 90.Ma M, Barnes G, Pulliam J, et al. CNS angiitis in graft vs host disease. Neurology. 2002;59:1994–1997. doi: 10.1212/01.wnl.0000038948.09158.a7. [DOI] [PubMed] [Google Scholar]
- 91.Padovan CS, Gerbitz A, Sostak P, et al. Cerebral involvement in graft-versus-host disease after murine bone marrow transplantation. Neurology. 2001;56:1106–1108. doi: 10.1212/wnl.56.8.1106. [DOI] [PubMed] [Google Scholar]
- 92.Sostak P, Padovan CS, Yousry TA, et al. Prospective evaluation of neurological complications after allogeneic bone marrow transplantation. Neurology. 2003;60:842–848. doi: 10.1212/01.wnl.0000046522.38465.79. [DOI] [PubMed] [Google Scholar]
- 93.Max MB, Culnane M, Schafer SC, et al. Amitriptyline relieves diabetic neuropathy pain in patients with normal or depressed mood. Neurology. 1987;37:589–596. doi: 10.1212/wnl.37.4.589. [DOI] [PubMed] [Google Scholar]
- 94.Sindrup SH, Gram LF, Brosen K, et al. The selective serotonin reuptake inhibitor paroxetine is effective in the treatment of diabetic neuropathy symptoms. Pain. 1990;42:135–144. doi: 10.1016/0304-3959(90)91157-E. [DOI] [PubMed] [Google Scholar]
- 95.Backonja M, Beydoun A, Edwards KR, et al. Gabapentin for the symptomatic treatment of painful neuropathy in patients with diabetes mellitus: a randomized controlled trial. JAMA. 1998;280:1831–1836. doi: 10.1001/jama.280.21.1831. [DOI] [PubMed] [Google Scholar]
- 96.Max MB, Schafer SC, Culnane M, et al. Association of pain relief with drug side effects in postherpetic neuralgia: a single-dose study of clonidine, codeine, ibuprofen, and placebo. Clin Pharmacol Ther. 1988;43:363–371. doi: 10.1038/clpt.1988.44. [DOI] [PubMed] [Google Scholar]
- 97.Richardson JK, Allet L, Kim H, Ashton-Miller JA. Fibular motor nerve conduction studies and ankle sensorimotor capacities. Muscle Nerve. 2013;47:497–503. doi: 10.1002/mus.23618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Lefvert AK, Bjorkholm M. Antibodies against the acetylcholine receptor in hematologic disorders: implications for the development of myasthenia gravis after bone marrow grafting. N Engl J Med. 1987;317:170. doi: 10.1056/NEJM198707163170315. [DOI] [PubMed] [Google Scholar]
- 99.Couriel DR, Beguelin GZ, Giralt S, et al. Chronic graft-versus-host disease manifesting as polymyositis: an uncommon presentation. Bone Marrow Transplant. 2002;30:543–546. doi: 10.1038/sj.bmt.1703711. [DOI] [PubMed] [Google Scholar]
- 100.Anderson BA, Young PV, Kean WF, et al. Polymyositis in chronic graft vs host disease. A case report. Arch Neurol. 1982;39:188–190. doi: 10.1001/archneur.1982.00510150058015. [DOI] [PubMed] [Google Scholar]
- 101.Parker P, Chao NJ, Ben-Ezra J, et al. Polymyositis as a manifestation of chronic graft-versus-host disease. Medicine (Baltimore) 1996;75:279–285. doi: 10.1097/00005792-199609000-00004. [DOI] [PubMed] [Google Scholar]
- 102.Gerritsen AA, de Vet HC, Scholten RJ, et al. Splinting vs surgery in the treatment of carpal tunnel syndrome: a randomized controlled trial. JAMA. 2002;288:1245–1251. doi: 10.1001/jama.288.10.1245. [DOI] [PubMed] [Google Scholar]
- 103.Hickson RC, Davis JR. Partial prevention of glucocorticoid-induced muscle atrophy by endurance training. Am J Physiol. 1981;241:E226–232. doi: 10.1152/ajpendo.1981.241.3.E226. [DOI] [PubMed] [Google Scholar]
- 104.Richardson JK, Sandman D, Vela S. A focused exercise regimen improves clinical measures of balance in patients with peripheral neuropathy. Arch Phys Med Rehabil. 2001;82:205–209. doi: 10.1053/apmr.2001.19742. [DOI] [PubMed] [Google Scholar]
- 105.Rubin LG, Levin MJ, Ljungman P, et al. 2013 IDSA clinical practice guideline for vaccination of the immunocompromised host. Clin Infect Dis. 2014;58:309–318. doi: 10.1093/cid/cit816. [DOI] [PubMed] [Google Scholar]
- 106.Tomblyn M, Chiller T, Einsele H, et al. Guidelines for preventing infectious complications among hematopoietic cell transplantation recipients: a global perspective. Biol Blood Marrow Transplant. 2009;15:1143–1238. doi: 10.1016/j.bbmt.2009.06.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Winston DJ, Antin JH, Wolff SN, et al. A multicenter, randomized, double-blind comparison of different doses of intravenous immunoglobulin for prevention of graft-versus-host disease and infection after allogeneic bone marrow transplantation. Bone Marrow Transplant. 2001;28:187–196. doi: 10.1038/sj.bmt.1703109. [DOI] [PubMed] [Google Scholar]
- 108.Cordonnier C, Chevret S, Legrand M, et al. Should immunoglobulin therapy be used in allogeneic stem-cell transplantation? A randomized, double-blind, dose effect, placebo-controlled, multicenter trial. Ann Intern Med. 2003;139:8–18. doi: 10.7326/0003-4819-139-1-200307010-00007. [DOI] [PubMed] [Google Scholar]
- 109.Intravenous immunoglobulin for the prevention of infection in chronic lymphocytic leukemia. A randomized, controlled clinical trial. Cooperative Group for the Study of Immunoglobulin in Chronic Lymphocytic Leukemia. N Engl J Med. 1988;319:902–907. doi: 10.1056/NEJM198810063191403. [DOI] [PubMed] [Google Scholar]
- 110.Intravenous immune globulin for the prevention of bacterial infections in children with symptomatic human immunodeficiency virus infection. The National Institute of Child Health and Human Developments Intravenous Immunoglobulin Study Group. N Engl J Med. 1991;325:73–80. doi: 10.1056/NEJM199107113250201. [DOI] [PubMed] [Google Scholar]
- 111.Magny JF, Bremard-Oury C, Brault D, et al. Intravenous immunoglobulin therapy for prevention of infection in high-risk premature infants: report of a multicenter, double-blind study. Pediatrics. 1991;88:437–443. [PubMed] [Google Scholar]
- 112.Ullmann AJ, Lipton JH, Vesole DH, et al. Posaconazole or fluconazole for prophylaxis in severe graft-versus-host disease. N Engl J Med. 2007;356:335–347. doi: 10.1056/NEJMoa061098. [DOI] [PubMed] [Google Scholar]
- 113.Vasconcelles MJ, Bernardo MV, King C, et al. Aerosolized pentamidine as pneumocystis prophylaxis after bone marrow transplantation is inferior to other regimens and is associated with decreased survival and an increased risk of other infections. Biol Blood Marrow Transplant. 2000;6:35–43. doi: 10.1016/s1083-8791(00)70050-4. [DOI] [PubMed] [Google Scholar]
- 114.Koc S, Leisenring W, Flowers ME, et al. Therapy for chronic graft-versus-host disease: a randomized trial comparing cyclosporine plus prednisone versus prednisone alone. Blood. 2002;100:48–51. doi: 10.1182/blood.v100.1.48. [DOI] [PubMed] [Google Scholar]
- 115.Perren TJ, Powles RL, Easton D, et al. Prevention of herpes zoster in patients by long-term oral acyclovir after allogeneic bone marrow transplantation. Am J Med. 1988;85:99–101. [PubMed] [Google Scholar]
- 116.Kanda Y, Mineishi S, Saito T, et al. Long-term low-dose acyclovir against varicella-zoster virus reactivation after allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplant. 2001;28:689–692. doi: 10.1038/sj.bmt.1703214. [DOI] [PubMed] [Google Scholar]
- 117.Boeckh M, Kim HW, Flowers ME, Meyers JD, Bowden RA. Long-term acyclovir for prevention of varicella zoster virus disease after allogeneic hematopoietic cell transplantation – a randomized double-blind placebo controlled study. Blood. 2006;107:1800–1805. doi: 10.1182/blood-2005-09-3624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Boeckh M, Leisenring W, Riddell SR, et al. Late cytomegalovirus disease and mortality in recipients of allogeneic hematopoietic stem cell transplants: importance of viral load and T-cell immunity. Blood. 2003;101:407–414. doi: 10.1182/blood-2002-03-0993. [DOI] [PubMed] [Google Scholar]
- 119.Milano F, Pergam SA, Xie H, et al. Intensive strategy to prevent CMV disease in seropositive umbilical cord blood transplant recipients. Blood. 2011;118:5689–5696. doi: 10.1182/blood-2011-06-361618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Sintchenko V, Gilbert GL, Coiera E, Dwyer D. Treat or test first? Decision analysis of empirical antiviral treatment of influenza virus infection versus treatment based on rapid test results. J Clin Virol. 2002;25:15–21. doi: 10.1016/s1386-6532(00)00182-7. [DOI] [PubMed] [Google Scholar]
- 121.Rothberg MB, Bellantonio S, Rose DN. Management of influenza in adults older than 65 years of age: cost-effectiveness of rapid testing and antiviral therapy. Ann Intern Med. 2003;139:321–329. doi: 10.7326/0003-4819-139-5_part_1-200309020-00007. [DOI] [PubMed] [Google Scholar]
- 122.Courneya KS, Keats MR, Turner AR. Physical exercise and quality of life in cancer patients following high dose chemotherapy and autologous bone marrow transplantation. Psychooncology. 2000;9:127–136. doi: 10.1002/(sici)1099-1611(200003/04)9:2<127::aid-pon438>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]
- 123.Janin A, Socie G, Devergie A, et al. Fasciitis in chronic graft-versus-host disease. A clinicopathologic study of 14 cases. Ann Intern Med. 1994;120:993–998. doi: 10.7326/0003-4819-120-12-199406150-00004. [DOI] [PubMed] [Google Scholar]
- 124.Dimeo F, Bertz H, Finke J, et al. An aerobic exercise program for patients with haematological malignancies after bone marrow transplantation. Bone Marrow Transplant. 1996;18:1157–1160. [PubMed] [Google Scholar]
- 125.Dimeo FC, Stieglitz RD, Novelli-Fischer U, et al. Effects of physical activity on the fatigue and psychologic status of cancer patients during chemotherapy. Cancer. 1999;85:2273–2277. [PubMed] [Google Scholar]
- 126.Mello M, Tanaka C, Dulley FL. Effects of an exercise program on muscle performance in patients undergoing allogeneic bone marrow transplantation. Bone Marrow Transplant. 2003;32:723–728. doi: 10.1038/sj.bmt.1704227. [DOI] [PubMed] [Google Scholar]
- 127.Mont MA, Carbone JJ, Fairbank AC. Core decompression versus nonoperative management for osteonecrosis of the hip. Clin Orthop Relat Res. 1996:169–178. doi: 10.1097/00003086-199603000-00020. [DOI] [PubMed] [Google Scholar]
- 128.Castaneda S, Carmona L, Carvajal I, et al. Reduction of bone mass in women after bone marrow transplantation. Calcif Tissue Int. 1997;60:343–347. doi: 10.1007/s002239900240. [DOI] [PubMed] [Google Scholar]
- 129.Schimmer AD, Mah K, Bordeleau L, et al. Decreased bone mineral density is common after autologous blood or marrow transplantation. Bone Marrow Transplant. 2001;28:387–391. doi: 10.1038/sj.bmt.1703149. [DOI] [PubMed] [Google Scholar]
- 130.Schimmer AD, Minden MD, Keating A. Osteoporosis after blood and marrow transplantation: clinical aspects. Biol Blood Marrow Transplant. 2000;6:175–181. doi: 10.1016/s1083-8791(00)70040-1. [DOI] [PubMed] [Google Scholar]
- 131.Kerschan-Schindl K, Mitterbauer M, Fureder W, et al. Bone metabolism in patients more than five years after bone marrow transplantation. Bone Marrow Transplant. 2004;34:491–496. doi: 10.1038/sj.bmt.1704618. [DOI] [PubMed] [Google Scholar]
- 132.Kang MI, Lee WY, Oh KW, et al. The short-term changes of bone mineral metabolism following bone marrow transplantation. Bone. 2000;26:275–279. doi: 10.1016/s8756-3282(99)00265-3. [DOI] [PubMed] [Google Scholar]
- 133.Stern JM, Chesnut CH, 3rd, Bruemmer B, et al. Bone density loss during treatment of chronic GVHD. Bone Marrow Transplant. 1996;17:395–400. [PubMed] [Google Scholar]
- 134.Stern JM, Sullivan KM, Ott SM, et al. Bone density loss after allogeneic hematopoietic stem cell transplantation: a prospective study. Biol Blood Marrow Transplant. 2001;7:257–264. doi: 10.1053/bbmt.2001.v7.pm11400947. [DOI] [PubMed] [Google Scholar]
- 135.Chapuy MC, Meunier PJ. Prevention and treatment of osteoporosis. Aging (Milano) 1995;7:164–173. doi: 10.1007/BF03324331. [DOI] [PubMed] [Google Scholar]
- 136.Dawson-Hughes B, Harris SS, Krall EA, Dallal GE. Effect of calcium and vitamin D supplementation on bone density in men and women 65 years of age or older. N Engl J Med. 1997;337:670–676. doi: 10.1056/NEJM199709043371003. [DOI] [PubMed] [Google Scholar]
- 137.Delmas PD. Treatment of postmenopausal osteoporosis. Lancet. 2002;359:2018–2026. doi: 10.1016/S0140-6736(02)08827-X. [DOI] [PubMed] [Google Scholar]
- 138.Cauley JA, Robbins J, Chen Z, et al. Effects of estrogen plus progestin on risk of fracture and bone mineral density: the Women’s Health Initiative randomized trial. JAMA. 2003;290:1729–1738. doi: 10.1001/jama.290.13.1729. [DOI] [PubMed] [Google Scholar]
- 139.Delmas PD. The use of bisphosphonates in the treatment of osteoporosis. Curr Opin Rheumatol. 2005;17:462–466. doi: 10.1097/01.bor.0000163448.51661.87. [DOI] [PubMed] [Google Scholar]
- 140.Adler RA. Glucocorticoid-induced osteoporosis: management update. Curr Osteoporos Rep. 2010;8:10–14. doi: 10.1007/s11914-010-0003-6. [DOI] [PubMed] [Google Scholar]
- 141.Zaheer S, LeBoff M, Lewiecki EM. Denosumab for the treatment of osteoporosis. Expert Opin Drug Metab Toxicol. 2015;11:461–470. doi: 10.1517/17425255.2015.1000860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Asikainen TM, Kukkonen-Harjula K, Miilunpalo S. Exercise for health for early postmenopausal women: a systematic review of randomised controlled trials. Sports Med. 2004;34:753–778. doi: 10.2165/00007256-200434110-00004. [DOI] [PubMed] [Google Scholar]
- 143.Syrjala KL, Langer SL, Abrams JR, et al. Late effects of hematopoietic cell transplantation among 10-year adult survivors compared with case-matched controls. J Clin Oncol. 2005;23:6596–6606. doi: 10.1200/JCO.2005.12.674. [DOI] [PubMed] [Google Scholar]
- 144.Pidala J, Kurland B, Chai X, et al. Patient-reported quality of life is associated with severity of chronic graft-versus-host disease as measured by NIH criteria: report on baseline data from the Chronic GVHD Consortium. Blood. 2011;117:4651–4657. doi: 10.1182/blood-2010-11-319509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145.Syrjala KL, Langer SL, Abrams JR, et al. Recovery and long-term function after hematopoietic cell transplantation for leukemia or lymphoma. JAMA. 2004;291:2335–2343. doi: 10.1001/jama.291.19.2335. [DOI] [PubMed] [Google Scholar]
- 146.Pallua S, Giesinger J, Oberguggenberger A, et al. Impact of GvHD on quality of life in long-term survivors of haematopoietic transplantation. Bone Marrow Transplant. 2010;45:1534–1539. doi: 10.1038/bmt.2010.5. [DOI] [PubMed] [Google Scholar]
- 147.Yi JC, Syrjala KL. Sexuality after hematopoietic stem cell transplantation. Cancer J. 2009;15:57–64. doi: 10.1097/PPO.0b013e318198c758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 148.Wong FL, Francisco L, Togawa K, et al. Long-term recovery after hematopoietic cell transplantation: predictors of quality-of-life concerns. Blood. 2010;115:2508–2519. doi: 10.1182/blood-2009-06-225631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149.Syrjala KL, Chapko MK, Vitaliano PP, et al. Recovery after allogeneic marrow transplantation: prospective study of predictors of long-term physical and psychosocial functioning. Bone Marrow Transplant. 1993;11:319–327. [PubMed] [Google Scholar]
- 150.Kiss TL, Abdolell M, Jamal N, et al. Long-term medical outcomes and quality-of-life assessment of patients with chronic myeloid leukemia followed at least 10 years after allogeneic bone marrow transplantation. J Clin Oncol. 2002;20:2334–2343. doi: 10.1200/JCO.2002.06.077. [DOI] [PubMed] [Google Scholar]
- 151.Chiodi S, Spinelli S, Ravera G, et al. Quality of life in 244 recipients of allogeneic bone marrow transplantation. Br J Haematol. 2000;110:614–619. doi: 10.1046/j.1365-2141.2000.02053.x. [DOI] [PubMed] [Google Scholar]
- 152.Sun CL, Francisco L, Baker KS, et al. Adverse psychological outcomes in long-term survivors of hematopoietic cell transplantation: a report from the Bone Marrow Transplant Survivor Study (BMTSS) Blood. 2011;118:4723–4731. doi: 10.1182/blood-2011-04-348730. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Baker KS, Fraser CJ. Quality of life and recovery after graft-versus-host disease. Best practice & research. Clin Haematol. 2008;21:333–341. doi: 10.1016/j.beha.2008.03.002. [DOI] [PubMed] [Google Scholar]
- 154.Syrjala KL, Artherholt SB, Kurland BF, et al. Prospective neurocognitive function over 5 years after allogeneic hematopoietic cell transplantation for cancer survivors compared with matched controls at 5 years. J Clin Oncol. 2011;29:2397–2404. doi: 10.1200/JCO.2010.33.9119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 155.Friedman MA, Fernandez M, Wefel JS, et al. Course of cognitive decline in hematopoietic stem cell transplantation: a within-subjects design. Arch Clin Neuropsychol. 2009;24:689–698. doi: 10.1093/arclin/acp060. [DOI] [PubMed] [Google Scholar]
- 156.Kupst MJ, Penati B, Debban B, et al. Cognitive and psychosocial functioning of pediatric hematopoietic stem cell transplant patients: a prospective longitudinal study. Bone Marrow Transplant. 2002;30:609–617. doi: 10.1038/sj.bmt.1703683. [DOI] [PubMed] [Google Scholar]
- 157.Simms S, Kazak AE, Golomb V, et al. Cognitive, behavioral, and social outcome in survivors of childhood stem cell transplantation. J Pediatr Hematol Oncol. 2002;24:115–119. doi: 10.1097/00043426-200202000-00011. [DOI] [PubMed] [Google Scholar]
- 158.Barrera M, Atenafu E, Andrews GS, Saunders F. Factors related to changes in cognitive, educational and visual motor integration in children who undergo hematopoietic stem cell transplant. J Pediatr Psychol. 2008;33:536–546. doi: 10.1093/jpepsy/jsm080. [DOI] [PubMed] [Google Scholar]
- 159.Perkins JL, Kunin-Batson AS, Youngren NM, et al. Long-term follow-up of children who underwent hematopoietic cell transplant (HCT) for AML or ALL at less than 3 years of age. Pediatr Blood Cancer. 2007;49:958–963. doi: 10.1002/pbc.21207. [DOI] [PubMed] [Google Scholar]
- 160.Shah AJ, Epport K, Azen C, Killen R, et al. Progressive declines in neurocognitive function among survivors of hematopoietic stem cell transplantation for pediatric hematologic malignancies. J Pediatr Hematol Oncol. 2008;30:411–418. doi: 10.1097/MPH.0b013e318168e750. [DOI] [PubMed] [Google Scholar]
- 161.Armstrong FD. Acute and long-term neurodevelopmental outcomes in children following bone marrow transplantation. Front Biosci. 2001;6:G6–G12. doi: 10.2741/armstron. [DOI] [PubMed] [Google Scholar]
- 162.Denlinger CS, Ligibel JA, Are M, et al. Survivorship: cognitive function, version 1.2014. J Natl Compr Canc Netw. 2014;12:976–986. doi: 10.6004/jnccn.2014.0094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 163.Jacobs SR, Jacobsen PB, Booth-Jones M, et al. Evaluation of the functional assessment of cancer therapy cognitive scale with hematopoietic stem cell transplant patients. J Pain Symptom Manage. 2007;33:13–23. doi: 10.1016/j.jpainsymman.2006.06.011. [DOI] [PubMed] [Google Scholar]
- 164.Hoodin F, Zhao L, Carey J, et al. Impact of psychological screening on routine outpatient care of hematopoietic cell transplantation survivors. Biol Blood Marrow Transplant. 2013;19:1493–1497. doi: 10.1016/j.bbmt.2013.07.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 165.Tichelli A, Labopin M, Rovo A, et al. Increase of suicide and accidental death after hematopoietic stem cell transplantation: a cohort study on behalf of the Late Effects Working Party of the European Group for Blood and Marrow Transplantation (EBMT) Cancer. 2013;119:2012–2021. doi: 10.1002/cncr.27987. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 166.Thygesen KH, Schjodt I, Jarden M. The impact of hematopoietic stem cell transplantation on sexuality: a systematic review of the literature. Bone Marrow Transplant. 2012;47:716–724. doi: 10.1038/bmt.2011.169. [DOI] [PubMed] [Google Scholar]
- 167.Syrjala KL, Kurland BF, Abrams JR, et al. Sexual function changes during the 5 years after high-dose treatment and hematopoietic cell transplantation for malignancy, with case-matched controls at 5 years. Blood. 2008;111:989–996. doi: 10.1182/blood-2007-06-096594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 168.Wong FL, Francisco L, Togawa K, et al. Longitudinal trajectory of sexual functioning after hematopoietic cell transplantation: impact of chronic graft-versus-host disease and total body irradiation. Blood. 2013;122:3973–3981. doi: 10.1182/blood-2013-05-499806. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 169.Mueller SM, Haeusermann P, Rovo A, et al. Genital chronic GVHD in men after hematopoietic stem cell transplantation: a single-center cross-sectional analysis of 155 patients. Biol Blood Marrow Transplant. 2013;19:1574–1580. doi: 10.1016/j.bbmt.2013.07.010. [DOI] [PubMed] [Google Scholar]
- 170.Barsky Reese J, Porter LS, Regan KR, et al. A randomized pilot trial of a telephone-based couples intervention for physical intimacy and sexual concerns in colorectal cancer. Psychooncology. 2014;23:1005–1013. doi: 10.1002/pon.3508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 171.Denlinger CS, Carlson RW, Are M, et al. Survivorship: sexual dysfunction (female), version 1.2013. J Natl Compr Canc Netw. 2014;12:184–192. doi: 10.6004/jnccn.2014.0019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 172.Denlinger CS, Carlson RW, Are M, et al. Survivorship: sexual dysfunction (male), version 1.2013. J Natl Compr Canc Netw. 2014;12:356–363. doi: 10.6004/jnccn.2014.0037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 173.Payne JK. A neuroendocrine-based regulatory fatigue model. Biol Res Nurs. 2004;6:141–150. doi: 10.1177/1099800404268280. [DOI] [PubMed] [Google Scholar]
- 174.Hjermstad MJ, Knobel H, Brinch L, et al. A prospective study of health-related quality of life, fatigue, anxiety and depression 3–5 years after stem cell transplantation. Bone Marrow Transplant. 2004;34:257–266. doi: 10.1038/sj.bmt.1704561. [DOI] [PubMed] [Google Scholar]
- 175.Syrjala KL, Yi JC, Artherholt SB, et al. Measuring musculoskeletal symptoms in cancer survivors who receive hematopoietic cell transplantation. J Cancer Surviv. 2010;4:225–235. doi: 10.1007/s11764-010-0126-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 176.Jim HS, Evans B, Jeong JM, et al. Sleep disruption in hematopoietic cell transplantation recipients: prevalence, severity, and clinical management. Biol Blood Marrow Transplant. 2014;20:1465–1484. doi: 10.1016/j.bbmt.2014.04.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 177.Denlinger CS, Ligibel JA, Are M, et al. Survivorship: fatigue, version 1.2014. J Natl Compr Canc Netw. 2014;12:876–887. doi: 10.6004/jnccn.2014.0082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 178.Syrjala KL, Stover AC, Yi JC, et al. Development and implementation of an Internet-based survivorship care program for cancer survivors treated with hematopoietic stem cell transplantation. J Cancer Surviv. 2011;5:292–304. doi: 10.1007/s11764-011-0182-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 179.DuHamel KN, Mosher CE, Winkel G, et al. Randomized clinical trial of telephone-administered cognitive-behavioral therapy to reduce post-traumatic stress disorder and distress symptoms after hematopoietic stem-cell transplantation. J Clin Oncol. 2010;28:3754–3761. doi: 10.1200/JCO.2009.26.8722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 180.Carlson LE, Speca M, Faris P, Patel KD. One year pre-post intervention follow-up of psychological, immune, endocrine and blood pressure outcomes of mindfulness-based stress reduction (MBSR) in breast and prostate cancer outpatients. Brain Behav Immun. 2007;21:1038–1049. doi: 10.1016/j.bbi.2007.04.002. [DOI] [PubMed] [Google Scholar]
- 181.Witek-Janusek L, Albuquerque K, Chroniak KR, et al. Effect of mindfulness based stress reduction on immune function, quality of life and coping in women newly diagnosed with early stage breast cancer. Brain Behav Immun. 2008;22:969–981. doi: 10.1016/j.bbi.2008.01.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.