

Abstract
The aim of this paper is to identify predictors of serum muscle damage marker (MDM) response following mixed martial arts (MMA) matches. Creatine kinase activity (CK) and myoglobin concentration (Mb) were measured in ten male elite MMA fighters (aged 28±5.7 years) prior to, 2 h, 24 h, and 96 h following 9 different MMA matches. The number of performed upright punches and kicks (UKF) that failed the opponent, the number of obtained hits to the upper and lower body (LBH), as well as the total fight duration (TFD) were evaluated as potential predictors from video recordings. CK peaked 24 h (829±753 U/L-1) and Mb peaked 2 h (210±122 µg/L-1) post matches. Almost 80% of the peak CK variance could be explained by LBH and UKF, whereas 87% of the Mb variation was explained by TFD and LBH. MMA result in a significant skeletal muscle damage, which largely depends on LBH. Furthermore, eccentric contractions to decelerate kicks that missed the opponent and the TFD seem to contribute to the MDM response.
Key words: Combat sports, mixed martial arts, muscle damage, creatine kinase, myoglobin
Introduction
Mixed Martial Arts (MMA) is a full contact combat sport that allows the athletes to use a broad range of fighting techniques from different martial arts like K1, kung fu, judo, wrestling and boxing. The idea to let unarmed opponents fight against each other using different techniques in order to find the most effective martial arts style, has its roots in the ancient Greece.1 Like in the modern MMA, fighters were not allowed to bite or to gouge the opponent’s eyes, mouth or nose.
Nevertheless, rules that allow athletes to punch the head of a downed opponent, let critics decry MMA as a dangerous barbaric blood sport which should be banned.2 By contrast, advocates argue that the mix of striking techniques with grappling is supposed to be less damaging. At least, there is evidence to suggest that MMA-contests are not associated with an extraordinary high injury rate. More concretely, the incidence of injuries is comparable with other full contact combat sports.1,3 However, these statistics usually focus on macroscopic injuries like orbital laceration, fractures and hematomas. By contrast, to the best knowledge of the authors, up to date no other study has analyzed the effect of MMA on microscopic damage of muscle tissue, measured as an altered level of muscle damage markers (MDM) in the blood.
Usually large intracellular molecules that are more or less specific for muscle tissue are used as damage markers. The muscle enzyme creatine kinase (CK) and the oxygen-binding protein myoglobin (Mb), rank among the most commonly used MDM in this context.4-6 Both markers have frequently been shown to increase following unaccustomed bouts of lengthening (eccentric) contractions7,8 and impact associated with collisions.9,10 However, more recent data indicate that metabolic stress may also induce muscle damage and would therefore contribute to the overall increase of MDMs in the blood.11-13
MMA competitions include all of the above listed stressors. Therefore, the major goal of the present study was to evaluate not only the response of MDM in the blood following MMA matches but also to identify which of these stressors serve as valuable predictors of the MDM response.
Materials and Methods
Subjects
A total of 10 healthy volunteer male elite MMA fighters aged between 22-40 years participated in the present study. Anthropometric values of the athletes can be found in Table 1. All athletes had a training experience of at least 5 years and competed in more than 1 national and/or international MMA events. None of the participants had any indication of musculoskeletal disorders or abnormality of liver or renal function. Written informed consent was obtained from all subjects prior to the enrolment. This study was approved by the local ethics board of the Heinrich Heine University Duesseldorf (Germany) and has therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki.
Table 1.
Anthropometric values of included athletes.
| Parameter (range) | Mean ± SD |
|---|---|
| Age, years (22-40) | 28±5.7 |
| Weight, kg (61-101) | 78±13.5 |
| Height, cm (169-191) | 181.5±7.13 |
| BMI, kg/m-2 (17.8-27.7) | 22.6±3.0 |
SD, standard deviation; BMI, body mass index.
Experimental procedures
The present study included 9 national MMA matches (including 4 title matches) that were organized between June 2013 and May 2014. Blood samples were drawn from the antecubital vein 20 min before (pre) and 2 h, 24 h, and 5 days post matches, after a resting period of 5 min. All blood samples were collected in 2 separate serum separator Vacutainer™ (BD, Franklin Lakes, NJ, USA) tubes. For every point of measurement, a total of 10 mL (5 mL each) was sampled. All blood samples were processed and subsequently transported at –10°C to the laboratory of the University Hospital Duesseldorf, Germany, where they were analyzed immediately. Measurements for CK activity were performed using an automated analyzer, Cobas 8000, Modul 701 (Roche Diagnostics GmbH, Basel, Switzerland). Mb concentration was determined by Nephelometer (Siemens Healthcare Diagnostics GmbH, Erlangen, Germany). The athletes were asked to avoid any strenuous exercises from three days prior to the competition until the end of follow-up measurements (i.e. 5 days after competition).
Match analyses
To estimate the amount of damaging events that were experienced by the enrolled athletes during the MMA matches, video recordings were analyzed by two experienced, independent raters. Any disagreements between those two raters were resolved by a third rater. Potential predictors of MDM level in the blood were defined as follows: i) eccentric contractions: number of performed upright punches (UPF) and kicks (UKF) that failed the opponent so that the respective limb had to be decelerated by the antagonistic musculature; ii) obtained attacks: number of obtained punches and kicks to the upper (UBH) and lower body (LBH); iii) duration of physical activity: total fight duration (TFD).
Statistics
Statistical differences between variables at different measurement time points were calculated by using repeated analyses of variance (ANOVA), while stepwise linear regression analyses were performed to estimate the impact of selected predictor variables (UPF, UKF, UBH, LBH, TFD) on the MDM response in the blood. The stepwise regression analysis was performed separately for the peak CK (24 h) and Mb (2 h) values. All statistical analyses were performed SPSS 22.0 (SPSS Inc., Chicago, IL, USA). For all analyses, P<0.05 was considered to be statistically significant.
Results
From the included MMA fights all matches were finished without knock outs. No fighter experienced a major cut or a macroscopic injury. No match had to be finished by the referee due to forbidden punches.
Muscle damage markers
Compared to the pre-test level (236±190 U/L-1), CK slightly increased 2 h post match (367±254 U/L-1), and significantly increased 24 h after the MMA competitions (829±753 U/L-1). At the last follow-up measurement (96 h) CK values returned to the baseline level (222±135 U/L-1). The mean Mb concentration already peaked 2 h after the fights (210±122 µg/L-1), which was significantly higher as the pretest level (29±5 µg/L-1). Thereafter, Mb concentrations decreased (24 h: 92±27) to show an almost complete recovery 96 h after the fight (35±11 µg/L-1).
Stepwise regression analysis
The mean number of UPF, UKF, UBH, and LBH were 31.11±43.26, 2.00±2.83, 4.22±6.04, 1.78±3.87, respectively. The mean TFD of all fights was 5.88±4.89 min. In the case of peak CK, it turned out that 80% of its variance could be explained by the predictors LBH and UKF. By contrast, 87% of the peak Mb variance could be predicted by the variables TFD and LBH. The results are summarized in Table 2.
Table 2.
Summary of the stepwise regression for the creatine kinase (CK) and the myoglobin (Mb) response.
| Dependent variable | Variables in the model | B (SE) | Standardized β | P | R2 of the model |
|---|---|---|---|---|---|
| CK 24h (peak) | LBH | 165.29 (38.29) | 0.82 | 0.01 | 0.80 |
| UKF | 160.50 (52.33) | 0.58 | 0.02 | ||
| Mb 2h (peak) | TFD | 0.34 (0.06) | 0.78 | 0.001 | 0.86 |
| LBH | 12.45 (5.00) | 0.35 | 0.04 |
SE, standard error; UPF, upright punches that failed the opponent; UKF, upright kicks that failed the opponent; UBH, number of obtained punches and kicks to the upper body; LBH, number of obtained punches and kicks to the lower body; TFD, total fight duration.
Discussion
The present results indicate that MMA matches are associated with severe muscle damage as evident by the significant increase of the indirect indicators of muscle damage CK and Mb (Figures 1 and 2). The earlier peak of Mb likely reflects the ability of these small molecules (17kDa) to directly enter the bloodstream from the extracellular space via the transepithelial pathway.14 By contrast, CK molecules (86 kDa) are slowly transported by the lymphatic system before leaking into the junction of the left subclavian vein and left jugular vein.15 Both markers are commonly used to estimate the amount of muscle damage and to judge, if patients need to be hospitalized in order to prevent renal failure.16 The underlying mechanisms for this complication include a renal vasoconstriction, an intraluminal cast formation and the direct toxic effects of myo-globin.17 Surprisingly, it has been stated that the risk for renal failures is low in the absence of nephrotoxic cofactors.18 Clarkson et al.16 reported that even marked exercise induced CK elevations of over 20,000 U/L-1 did not require any treatment to prevent renal compromise. However, dehydration is known to be a key factor that increases the risk of renal injury by decreasing the Mb’s solubility - and dehydration is common issue in MMA.18 Jelton et al.,19 who investigated the hydration status of 40 male MMA fighters, reported that 39% of these individuals presented a serious dehydration prior to competition and some of them failed to sufficiently rehydrate before the match. From this perspective, weight management in MMA must urgently be revised.
Figure 1.
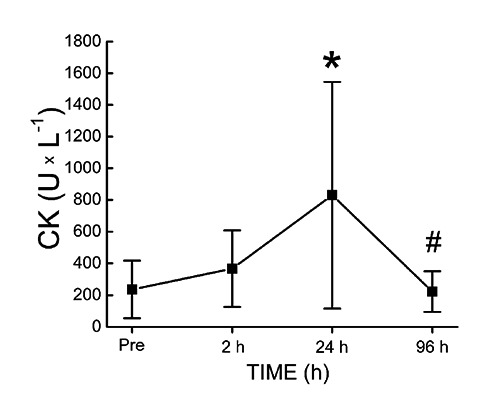
Creatine kinase (CK) activity was measured as described in the method section. CK activity increased slightly and reached its maximum at 24 h post match. After 5 days a complete recovery could be observed. *P<0.05 vs. pre. #P<0.05 vs. 24 h.
Figure 2.
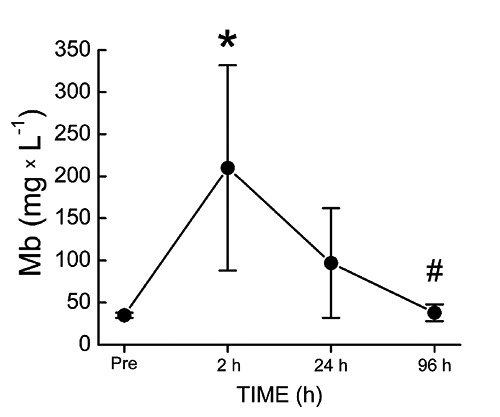
Myoglobin (Mb) concentration was measured as mentioned in the method section. The concentration of Mb increased after 2 h post match significantly, with peak values approximately 7 fold higher as compared to baseline values. A complete recovery could be observed 5 days after the matches. *P<0.05 vs. pre. #P<0.05 vs. 2 h.
Unfortunately comparative data on MDM after martial arts competitions are rare. The only other study found by the authors investigating MDM responses after a competition of martial arts that included boxing and kicking was that published by Saengsirisuwan et al.20 These authors reported that 12 h after Thai boxing competitions, the CK activity increased to 378.5±95 U/L-1. However, due to the fact that CK usually continues to increase for several days after the damaging event,21 the 12 h values of that study are not comparable to the present results. The comparability is further aggravated by the fact that the Thai boxers investigated by Saengsirisuwan et al.20 largely differed in mean body mass (40.0±2.1 kg) from the investigated athletes of the present study (78±13.5 kg).
The peak CK value of 829±753 U/L-1, measured 24 h after the fights included in the present study is comparable to CK activities reported by Takarada [10] after competitive rugby matches (1081±159 U/L-1). Noteworthy, this author found the extent of muscle damage to be highly correlated with the number of tackles (CK vs. number of tackles: r=0.85, P<0.01; Mb vs. number of tackles: r=0.92, P<0.01). Similarly, McLellan et al.,22 who found that CK activity peaked 24 h after an elite rugby league play in forwards (979±415 U/L-1) and backs (922±380 U/L-1), reported that the number of heavy collisions (>8.1 G) during an elite rugby league match play was an important predictor of the observed CK response. These data and others indicate that blunt force traumata are capable to induce a significant CK release.9,23,24 This assumption is supported by the results of the present study as the number of obtained punches and kicks to the lower body (LBH) significantly contributed to the variance of peak CK and Mb levels in MMA fighters. Therefore, it can reasonably be assumed that MDM response after MMA matches can partially be attributed to the number of obtained blunt force traumata.
Apart from the blunt force traumata resulting from physical collisions, we found that upright kicks that failed the opponent (UKF), contributed to the variance of the observed CK response. It is well documented in the literature that eccentric contractions are associated with increased membrane permeability, resulting in an efflux of MDM in the bloodstream.25 Furthermore, it has been demonstrated that fast velocity (210°/s-1) eccentric contractions result in a 4.5-fold higher CK response, when compared to slower (30°/s-1) eccentric contractions.26 Therefore, the contribution of UKF to the observed variance of the CK response is likely a function of the eccentric contractions of the antagonists needed to rapidly decelerate the leg. The fact that the number of performed punches, which failed the opponent did not turn out as a significant predictor of the CK and Mb response may be a result of the lower mass that needs to be decelerated and the lower mass of muscles that contracts eccentrically. Finally, the performed stepwise regression revealed that the total fight duration (TFD) was correlated with the peak Mb response measured 2 h after the MMA matches. A possible explanation for this observation is that the metabolic stress contributed to the increased membrane permeability, which allowed the Mb molecules to leak into the extracellular space. Research does indeed show that not only high mechanical forces, but also metabolic stress aggravates the amount of muscle damage, indicative by MDM in the blood.27 In this context, it was reported that shorter rest intervals between sets of eccentric contractions result in greater CK responses.28,29 Thus, despite the fact that shorter rest intervals resulted in a lower amount of work performed by participants, the higher metabolic stress resulted in a greater MDM leakage. In an animal model, it could be shown that even exhaustive swimming protocols that virtually lack any meaningful mechanical stress result in pronounced CK elevations.30 The reason why TFD partially predicted the variance of Mb but not the CK response remains unclear.
Study limitations
There are some limitations that need to be acknowledged and addressed regarding the present study. Firstly, the hydration status of the athletes was not assessed. Since the hydration status affects the blood volume, the activity and concentration measures of CK and Mb may be biased by concentration/dilution effects to an unknown extent. It has been reported previously that hypohydration is able to amplify the characteristic exercise induced MDM response in the blood.31 Additionally, our study was only observational, based on indirect markers of muscle damage. Therefore, the discussion on the underlying mechanisms that resulted in the MDM release had to be speculative in nature. Finally, we were not able to measure the severity of the physical collisions, which likely would have improved the accuracy of the obtained regression models.
Conclusions
The variety of injury patterns associated with MMA has been thoroughly reviewed by Walrod et al. in 2011.32 However, to the best knowledge of the authors up to date no other study investigated blood indices of muscle damage after competitive MMA matches. The present data demonstrate that MMA matches result in pronounced increase of CK and Mb in the blood. Further, it turned out that the number of obtained hits to the lower body, the number of eccentric contractions to decelerate the respective leg after kicks that missed the opponent, and the duration of the fights contributed to the observed MDM response.
References
- 1.McClain R, Wassermen J, Mayfield C, et al. Injury profile of mixed martial arts competitors. Clin J Sport Med 2014;24:497-501. [DOI] [PubMed] [Google Scholar]
- 2.White C. Mixed martial arts and boxing should be banned, says BMA. BMJ 2007;335 :469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bledsoe GH, Hsu EB, Grabowski JG, et al. Incidence of injury in professional mixed martial arts competitions. J Sports Sci Med 2006;5:136-42. [PMC free article] [PubMed] [Google Scholar]
- 4.Paul GL, DeLany JP, Snook JT, et al. Serum and urinary markers of skeletal muscle tissue damage after weight lifting exercise. Eur J of Appl Physiol Occup Physiol 1989;58:786-90. [DOI] [PubMed] [Google Scholar]
- 5.Tiidus PM, Ianuzzo CD. Effects of intensity and duration of muscular exercise on delayed soreness and serum enzyme activities. Med Sci Sports Exerc 1983;15:461-5. [PubMed] [Google Scholar]
- 6.Noakes TD. Effect of exercise on serum enzyme activities in humans. Sports Med 1987;4:245-67. [DOI] [PubMed] [Google Scholar]
- 7.Nosaka K, Clarkson PM. Effect of eccentric exercise on plasma enzyme activities previously elevated by eccentric exercise. Eur J of Appl Physiol Occup Physiol 1994;69:492-7. [DOI] [PubMed] [Google Scholar]
- 8.Sorichter S, Puschendorf B, Mair J. Skeletal muscle injury induced by eccentric muscle action: muscle proteins as markers of muscle fiber injury. Exerc Immunol Rev 1999;5:5-21. [PubMed] [Google Scholar]
- 9.McLellan CP, Lovell DI, Gass GC. Biochemical and endocrine responses to impact and collision during elite Rugby League match play. J Strength Cond Res 2011;25:1553-62. [DOI] [PubMed] [Google Scholar]
- 10.Takarada Y. Evaluation of muscle damage after a rugby match with special reference to tackle plays. Br J Sports Med 2003;37:416-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Suzuki K, Totsuka M, Nakaji S, et al. Endurance exercise causes interaction among stress hormones, cytokines, neutrophil dynamics, and muscle damage. J Appl Physiol 1999;87:1360-7. [DOI] [PubMed] [Google Scholar]
- 12.Peake J, Suzuki K. Neutrophil activation, antioxidant supplements and exercise-induced oxidative stress. Exerc Immunol Rev 2004;10:129-41. [PubMed] [Google Scholar]
- 13.Behringer M, Montag J, Franz A, et al. Exhaustive exercise: a near death experience for skeletal muscle cells? Med Hypotheses 2014;83:758-65. [DOI] [PubMed] [Google Scholar]
- 14.van de Vyver M, Myburgh KH. Cytokine and satellite cell responses to muscle damage: interpretation and possible confounding factors in human studies. J Muscle Res Cel. Motil 2012;33:177-85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lindena J, Kupper W, Trautschold I. Enzyme activities in thoracic duct lymph and plasma of anaesthetized, conscious resting and exercising dogs. Eur J Appl Physiol Occup Physiol 1984;52:188-95. [DOI] [PubMed] [Google Scholar]
- 16.Clarkson PM, Kearns AK, Rouzier P, et al. Serum creatine kinase levels and renal function measures in exertional muscle damage. Med Sci Sports Exerc 2006;38:623-7. [DOI] [PubMed] [Google Scholar]
- 17.Daher Ede F, Silva Júnior GB, Brunetta DM, et al. Rhabdomyolysis and acute renal failure after strenuous exercise and alcohol abuse: case report and literature review. São Paulo Med J 2005;123:33-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sinert R, Kohl L, Rainone T, et al. Exercise-induced rhabdomyolysis. Ann Emerg Med 1994;23:1301-6. [DOI] [PubMed] [Google Scholar]
- 19.Jetton AM, Lawrence MM, Meucci M, et al. Dehydration and acute weight gain in mixed martial arts fighters before competition. J Strength Con Res 2013:27:1322-6. [DOI] [PubMed] [Google Scholar]
- 20.Saengsirisuwan V, Phadungkij S, Pholpramool C. Renal and liver functions and muscle injuries during training and after competition in Thai boxers. Br J Sports Med 1998;32:304-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Brancaccio P, Maffulli N, Limongelli FM. Creatine kinase monitoring in sport medicine. British Medical Bulletin 2007;81:209-30. [DOI] [PubMed] [Google Scholar]
- 22.McLellan CP, Lovell DI, Gass GC. Creatine kinase and endocrine responses of elite players pre, during, and post rugby league match play. J Strength Cond Res 2010;24:2908-19. [DOI] [PubMed] [Google Scholar]
- 23.Smart DJ, Gill ND, Beaven CM. The relationship between changes in interstitial creatine kinase and game-related impacts in rugby union. Br J Sports Med 2008;42:198-201. [DOI] [PubMed] [Google Scholar]
- 24.Hoffman JR, Maresh CM, Newton RU. Performance, biochemical, and endocrine changes during a competitive football game. Med Sci Sports Exerc 2002;34:1845-53. [DOI] [PubMed] [Google Scholar]
- 25.Brancaccio P, Lippi G, Maffulli N. Biochemical markers of muscular damage. Clinical Chem and Lab Medicine 2010;48:757-67. [DOI] [PubMed] [Google Scholar]
- 26.Chapman D, Newton M, Sacco P. Greater muscle damage induced by fast versus slow velocity eccentric exercise. Int J Sports Med 2006;27:591-98. [DOI] [PubMed] [Google Scholar]
- 27.Koch AJ, Pereira R, Machado M. The creatine kinase response to resistance exercise. J Musc Neur Interact 2014;14:68-77. [PubMed] [Google Scholar]
- 28.Machado M, Willardson JM. Short recovery augments magnitude of muscle damage in high responders. Med Sci Sports Exerc 2010;42:1370-4. [DOI] [PubMed] [Google Scholar]
- 29.Rodrigues BM, Dantas E, Salles BF. Creatine kinase and lactate dehydrogenase responses after upper-body resistance exercise with different rest intervals. J Strength Cond Res 2010;24:1657-62. [DOI] [PubMed] [Google Scholar]
- 30.Chen Y, Serfass RC, Apple FS. Alterations in the expression and activity of creatine kinase-M and mitochondrial creatine kinase subunits in skeletal muscle following prolonged intense exercise in rats. Eur J Appl Physiol 2000;81:114-9. [DOI] [PubMed] [Google Scholar]
- 31.Fielding RA, Violan MA, Svetkey L, et al. Effects of prior exercise on eccentric exercise-induced neutrophilia and enzyme release. Med Sci Sports Exerc 2000;32:359-64. [DOI] [PubMed] [Google Scholar]
- 32.Walrod B. Current review of injuries sustained in mixed martial arts competition. Curr Sports Med Rep 2011;10:288-9. [DOI] [PubMed] [Google Scholar]