

Ribavirin plus pegylated interferon (iFNα) is currently the standard therapy for treating chronic hepatitis C (HCV). Addition of first-generation protease inhibitors such as telaprevir and boceprevir to standard therapy is also recommended for chronic HCV genotype 1 infections.1 Despite the recent advances in the treatment modalities for chronic HCV, adherence to treatment has been limited by contraindications to iFNα-based regimens, numerous side effects (e.g influenza-like symptoms, depression, fatigue, cytopenias), and the requirement of weekly subcutaneous injections.2 Sofosbuvir is a nucleotide polymerase inhibitor that has recently been approved in combination with ribavirin for chronic HCV genotypes 2 and 3 infections.3 With the aim of providing more epidemiologic evidence, we have systematically evaluated and summarized in a meta-analysis available data on this topic.
A comprehensive search of the Cochrane library, PUBMED, and Scopus from January 1980 to November 2013 was conducted. The outcome of interest was sustained virological response (SVR) at 12 weeks. Only trials reporting SVR for HCV patients who received sofosbuvir-ribavirin duo therapy were eligible for inclusion. Subgroup analyses were performed by HCV genotype and for patients who were naive, experienced, or nonresponders to previous treatment with standard regimen. This meta-analysis was performed by calculating pooled SVRs. First, the individual study SVR was transformed into a quantity using the Freeman–Tukey variant of the arcsine square root transformed proportion. The pooled SVR is calculated as the back transform of the weighted mean of the transformed SVRs, using inverse arcsine variance weights for the fixed effects model and DerSimonian–Laird weights for the random effects model.4,5 The effect of publication and selection bias on the summary estimates were tested by both the Egger bias indicator and Begg–Mazumdar bias indicator.6
We included six trials7-11 involving 636 patients in the analyses (Table 1). HCV Genotype 1 patients had an overall 12-week SVR of 66% (95% CI: 57%-73%) after 12 weeks of treatment (Figure 1A). The outcome was better for treatment naive patients (70%; 95% CI: 61%-77%; Figure 1B) compared to treatment experienced (nonresponders) which was 10%. However, for HCV Genotype 2 and 3, there were similar 12-week SVRs for both treatment naïve and treatment experienced patients. The overall 12-week SVR after 12 weeks of treatment was 75 % (95% CI: 71%-78%; Figure 2A). Subgroup analysis limited to treatment experienced patients was equally high (75%; 95% CI: 71%-79%; Figure 2B). There was no evidence of heterogeneity or publication bias in these analyses. Begg–Mazumdar bias indicator gave Kendall's tau=-0.02 (P=0.86), and the Egger bias was -1.25 (95 % CI=-4.23 to 1.74, P=0.36).
Table 1. Characteristics of Included Studies.
| Trial | Region | HCV Genotype | Subgroup | No. Patients | Treatment duration (weeks) | Sofosbuvir dose (mg once daily) | Ribavirin dose (mg/day) | SVR at 12 weeks (%) |
|---|---|---|---|---|---|---|---|---|
| Quantum | Europe | 1 | Naive | 25 | 12 | 400 | 1,000-1,200 | 56 |
| Electron | Europe | 1 | Naive | 25 | 12 | 400 | 1,000-1,200 | 88 |
| NIH Spare | North America | 1 | Naive | 10 | 12 | 400 | 600-1,000 | 90 |
| Electron | Europe | 1 | Experienced | 10 | 12 | 400 | 1,000-1,200 | 10 |
| Fission | North America | 2 and 3 | Naive | 256 | 12 | 400 | 1,000-1,200 | 67 |
| Fusion | North America | 2 and 3 | Experienced | 103 | 12 | 400 | 1,000-1,200 | 50 |
| Positron | North America | 2 and 3 | Experienced | 207 | 12 | 400 | 1,000-1,200 | 78 |
Figure 1.
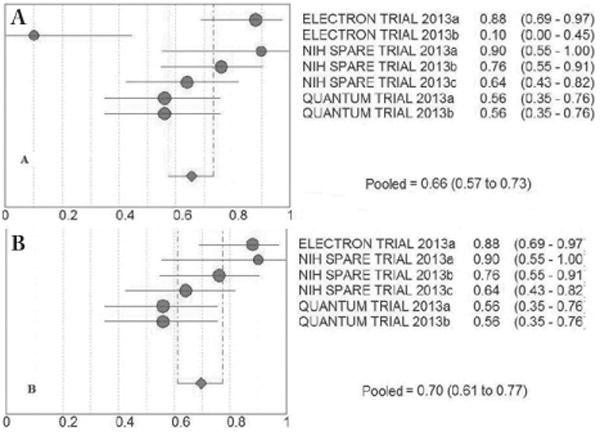
A) Overall 12-week SVR for HCV Genotype 1 patients; B) 12-week SVR for treatment naive Genotype 1 patients.
Figure 2.
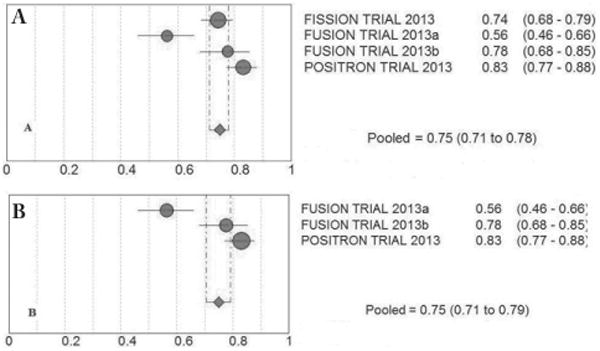
A) Overall 12-week SVR for HCV Genotype 2 and 3 patients; B) 12-week SVR for treatment experienced HCV Genotype 2 and 3 patients.
In conclusion, our results indicate that sofosbuvir-ribavirin duo therapy for 12 weeks is effective in treatment naïve HCV genotype 1 and in both treatment naïve and experienced HCV genotype 2 and 3 infections. However, prior nonresponders with HCV genotype 1 infection do not seem to benefit from this therapeutic option. Future studies should focus on side effects, including cost-analysis of this novel treatment combination compared to standard therapy in order to aid the decision process.
References
- 1.Ghany MG, Strader DB, Thomas DL, Seeff LB. Diagnosis, management, and treatment of hepatitis C: an update. Hepatology. 2009;49:1335–74. doi: 10.1002/hep.22759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Soriano V, Vispo E, Poveda E, Labarga P, Barreiro P. Treatment failure with new hepatitis C drugs. Expert Opin Pharmacother. 2012;13:313–23. doi: 10.1517/14656566.2012.653341. [DOI] [PubMed] [Google Scholar]
- 3. [Accessed November 25, 2013];FDA Antiviral Drugs Advisory Committee Meeting, October 25, 2013 FDA Web site. http://www.fda.gov/downloads/advisorycommittees/committeesmeetingmaterials/drugs/antiviraldrugsadvisorycommittee/ucm371876.pdf.
- 4.Stuart A, Ord JK. Kendall's Advanced Theory of Statistics. 6th. London: Edward Arnold; 1994. [Google Scholar]
- 5.DerSimonian R, Laird N. Meta-analysis in clinical trials. Controlled Clin Trials. 1986;7:177–88. doi: 10.1016/0197-2456(86)90046-2. [DOI] [PubMed] [Google Scholar]
- 6.Harbord RM, Egger M, Sterne JAC. A modified test for small-study effects in meta-analyses of controlled trials with binary endpoints. Stat Med. 2005;25:3443–57. doi: 10.1002/sim.2380. [DOI] [PubMed] [Google Scholar]
- 7.Lalezari JP, Nelson DR, Hyland RH, et al. Once daily sofosbuvir plus ribavirin for 12 and 24 weeks in treatment-naive patients with hCV infection: the Quantum study. J Hepatol. 2013;58:S236. [Google Scholar]
- 8.Gane EJ, Stedman CA, Hyland RH, et al. All-oral sofosbuvir-based 12-week regimens for the treatment of chronic HCV infection: the Electron study. J Hepatol. 2013;58:S6. [Google Scholar]
- 9.Osinusi A, Meissner EG, Lee YJ, et al. Sofosbuvir and ribavirin for hepatitis C genotype 1 in patients with unfavorable treatment characteristics: a randomized clinical trial. JAMA. 2013 Nov 13;310(18):1987. doi: 10.1001/jama.2013.109309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lawitz E, Mangia A, Wyles D, et al. Sofosbuvir for previously untreated chronic hepatitis C infection. N Engl J Med. 2013;368:1878–87. doi: 10.1056/NEJMoa1214853. [DOI] [PubMed] [Google Scholar]
- 11.Jacobson IM, Gordon SC, Kowdley KV, et al. Sofosbuvir for hepatitis C genotype 2 or 3 in patients without treatment options. N Engl J Med. 2013 May 16;368(20):1867–77. doi: 10.1056/NEJMoa1214854. [DOI] [PubMed] [Google Scholar]