

Abstract
In late March of 2009, an outbreak of influenza in Mexico, was eventually identified as H1N1 influenza A. In June 2009, the World Health Organization raised a pandemic alert to the highest level. More than 214 countries have reported confirmed cases of pandemic H1N1 influenza A. In Korea, the first case of pandemic influenza A/H1N1 infection was reported on May 2, 2009. Between May 2009 and August 2010, 750,000 cases of pandemic influenza A/H1N1 were confirmed by laboratory test. The H1N1-related death toll was estimated to reach 252 individuals. Almost one billion cases of influenza occurs globally every year, resulting in 300,000 to 500,000 deaths. Influenza vaccination induces virus-neutralizing antibodies, mainly against hemagglutinin, which provide protection from invading virus. New quadrivalent inactivated influenza vaccine generates similar immune responses against the three influenza strains contained in two types of trivalent vaccines and superior responses against the additional B strain.
Keywords: Influenza, Pandemic, Vaccines
History of Influenza Pandemics
The pandemic influenza of 1918 and 1919, also referred to as the Spanish flu, is estimated to have resulted in 50 to 100 million deaths worldwide1. Death rates were especially high among healthy adults between 15 and 34 years, which is why the Spanish flu was one of the worst epidemics humankind has ever experienced2. The extremely severe consequences of the Spanish flu resulted from the emergence of an antigenic shift in both the hemagglutinin (H1) and the neuraminidase (N1) proteins of the influenza A virus3. The unparalleled pathogenicity of the 1918 pandemic influenza virus was well demonstrated in a mouse model using genetic recombination techniques. After infection in mice, the 1918 pandemic strain produced 39,000 times more virus copies in the lungs than contemporary H1N1 strains4. After the 1918 and 1919 influenza pandemic, there were several other major-scale pandemics due to influenza A virus. The H2N2/1957 and H3N2/1968 pandemic influenza viruses emerged via the exchange of genomic RNA segments between human and avian viruses. In 1957, the shift of the influenza A strain to H2 and N2 resulted in a severe pandemic which led to at least 1 million deaths worldwide5. In 1968, an antigenic shift occurred only in hemagglutinin (from H2N2 to H3N2), which explain why the 1968 pandemic was less extensive than that in 19576. The emergence of a novel H1N1 influenza virus in March 2009 in Mexico represents the most recent pandemic, and the pandemic H1N1 virus has continued to circulate the world ever since.
2009 Pandemic Influenza A/H1N1
In late March of 2009, an outbreak of influenza was detected in Mexico, which was eventually identified as H1N1 influenza A. In June 2009 the World Health Organization (WHO) raised its pandemic alert to the highest level ('phase 6'). More than 214 countries have reported confirmed cases of pandemic H1N1 influenza A7. The 2009 influenza pandemic was caused by an H1N1 virus that had not been previously recovered from animals or humans. This strain represented a quadruple, genetic reassortment of two swine strains, one human strain, and one avian strain of influenza8. Using a modeling study, the United States Centers for Disease Control and Prevention (CDC) estimated that approximately 61 million cases of pandemic H1N1 influenza occurred on US soil between April 2009 and April 10, 2010, resulting in 274,000 hospitalizations and 12,470 deaths9. It was estimated that the 2009 H1N1 influenza pandemic was associated with 100,000 to 400,000 respiratory deaths and 46,000 to 180,000 cardiovascular deaths10,11. The mortality rate of the 2009 pandemic influenza A infection in the United States was 0.12 deaths per 100,000 individuals12. Most deaths were related to respiratory failure resulting from severe pneumonia and acute respiratory distress syndrome13. The pandemic was declared to be over in August 2010.
2009 Pandemic Influenza A/H1N1 in Korea
In Korea, the first case of pandemic influenza A/H1N1 infection was reported on May 2, 2009. Influenza activity peaked in November and it declined rapidly to below baseline levels in February 2010. Between May 2009 and August 2010, there were 750,000 cases of pandemic influenza A/H1N1 that were confirmed by laboratory tests. The number of H1N1-related deaths was estimated at 252. Therefore, the case-fatality of the 2009 pandemic influenza A/H1N1 in Korea is 0.03%14. When the infection by H1N1 was associated with pneumonia, however, admission to an intensive care unit was necessary in 36.1% of all individuals and 10.4% required mechanical ventilation. Despite the administration of antiviral and antibacterial agents, the mortality rate of H1N1-assocated pneumonia was 7.2%15. The clinical outcomes of admitted H1N1 patients are consistent with those of the United States (of 272 hospitalized H1N1 patients, 25% were admitted to intensive care unit [ICU] and 7% died) and those of Australia and New Zealand (of 722 H1N1 patients admitted to ICU, the mortality rate was 14.3%)16,17. Younger generation does not seem to be more severely affected by 2009 H1N1. In a study which investigated the clinical characteristics of 3,777 pediatric cases of 2009 H1N1 influenza in southern part of Korea, 221 patients (5.9%) were hospitalized. Ten of the admitted patients (4.5%) were admitted to the ICU, and eight (3.6%) required mechanical ventilation18. The annual socioeconomic costs of the 2009 pandemic influenza A/H1N1 were estimated at a total of US $1.09 billion (0.14% of the national GDP of Korea), based on direct costs US $428.0 million (39.3%) and indirect costs US $662.5 million (60.8%)19.
Influenza
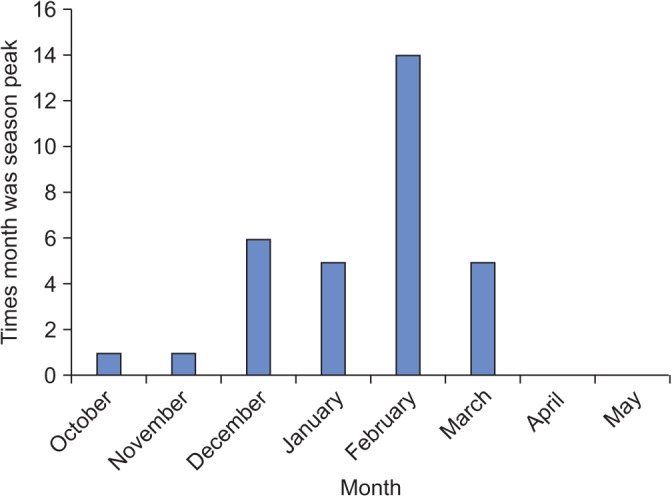
Influenza is an acute respiratory disease and human infections are predominantly caused by influenza A or B viruses. Influenza occurs in epidemics mainly during the winter season in temperate climates and throughout the year in the tropics (Figure 1)20. Usually, two to three different strains of influenza circulate concurrently during a given influenza season. It is estimated that more than one billion cases of influenza occurs globally every year, which results in 3 to 5 million cases of severe illness and 300,000 to 500,000 deaths21. This huge burden and epidemiologic pattern of influenza is caused by the changing nature of the antigenic properties of influenza viruses. Influenza A viruses have the special ability to undergo periodic modifications in the antigenic characteristics of their envelope glycoproteins, the hemagglutinin and the neuraminidase. Among the different influenza A viruses subtypes, three major hemagglutinin subtypes (H1, H2, and H3) and two neuraminidase subtypes (N1 and N2) have evolved to human species-specific subtypes. Influenza viruses have eight RNA filaments of segmented genome that can be reassorted at high rates among coinfecting viruses. Reassortment between animal and human influenza viruses may result in the emergence of new strains, which is called antigenic shift22. Antigenic shift induced the emergence of new viruses that caused the pandemics of 1908, 1957, 1968, and 2009. Antigenic drifts arise from point mutations in the RNA gene segments that code for the hemagglutinin or the neuraminidase. Outbreaks due to antigenic drifts are usually less extensive and severe. Antigenic drift accounts for the variable extent and severity of influenza outbreaks between the years of antigenic shift23. Influenza B viruses have a lower propensity for antigenic changes and only antigenic drifts in hemagglutinin have been described. In contrast to influenza A viruses, influenza B viruses have attracted relatively little attention. Nonetheless, influenza B has a large impact on public health causing 22.6% of the global total influenza cases between 2000 and 201324.
Figure 1. Peak month of flu activity from 1982–1983 through 2013–2014 in the United States. Adopted from Centers for Disease Control and Prevention, according to Creative Commons Licenses20.
Influenza Vaccination
Influenza viruses display high mutation rates, which compromises the efficient recognition of new variants by the immune system. As a consequence, new influenza vaccines need to be produced each year to match current circulating viruses. Influenza vaccination induces virus-neutralizing antibodies, mainly against hemagglutinin which provide protection to invading viruses25. The elderly and those with comorbidities are at increased risk to suffer from complication of influenza. Influenza vaccination not only reduces the risk of infection but also reduces the illness severity. The United States CDC and the WHO collaborate to track influenza virus strains isolated throughout the world and to predict the appropriate components for the annual influenza vaccine. There are two types of influenza vaccines, inactivated influenza vaccine and live-attenuated vaccine. The choice of vaccine formulation depends on several factors, including age, comorbidities, pregnancy, and risk of adverse reaction. The intranasally administered live-attenuated influenza vaccine is approved for healthy nonpregnant adults up to 49 years of age. Until recently, inactivated influenza vaccines were trivalent, containing two influenza A antigens (H3N2 and H1N1) and one influenza B virus antigen (Victoria or Yamagata strain). Two genetic lineages of influenza B viruses have circulated since the mid-1980s. Between 1999 and 2012, 42% of all influenza B infections were caused by viruses that were not covered in the trivalent vaccine of those seasons26. In August 2013, the Food and Drug Administration approved a quadrivalent inactivated influenza vaccine, Fluarix Tetra, which contains two influenza A antigens (H3N2 and H1N1) and two influenza B antigens (Victoria and Yamagata strain). Quadrivalent inactivated influenza vaccine generates similar immune responses against the three influenza strains contained in two types of trivalent vaccines and superior responses against the additional B strain27,28. In 2010, the United States Advisory Committee on Immunization Practice (ACIP) expanded the recommendation for influenza vaccination to include all individuals of 6 months of age and older. Vaccination to prevent influenza is particularly important for people who are at high risk of developing serious complications. When the vaccine supply is limited, vaccination efforts should focus on delivering vaccination to this specified group of people (Table 1)29.
Table 1. High-priority groups for flu vaccination during a vaccine shortage.
| When vaccine supply is limited, vaccination efforts should focus on delivering vaccination to the following people (no hierarchy is implied by order of listing): |
| - Children aged 6 months through 4 years (59 months) |
| - People aged 50 years and older |
| - People with chronic pulmonary (including asthma), cardiovascular (except hypertension), renal, hepatic, neurologic, hematologic, or metabolic disorders (including diabetes mellitus) |
| - People who are immunosuppressed (including immunosuppression caused by medications or by human immunodeficiency virus) |
| - Women who are or will be pregnant during the influenza season |
| - People who are aged 6 months through 18 years and receiving long-term aspirin therapy and who therefore might be at risk for experiencing Reye syndrome after influenza virus infection |
| - People who are residents of nursing homes and other chronic-care facilities |
| - American Indians/Alaska Natives |
| - People who are morbidly obese (body mass index is 40 or greater) |
| - Health-care personnel |
| - Household contacts and caregivers of children younger than 5 years and adults aged 50 years and older, with particular emphasis on vaccinating contacts of children aged younger than 6 months |
| - Household contacts and caregivers of people with medical conditions that put them at higher risk for severe complications from influenza |
Adopted from Centers for Disease Control and Prevention, according to Creative Commons Licenses29.
Footnotes
Conflicts of Interest: No potential conflict of interest relevant to this article was reported.
References
- 1.Johnson NP, Mueller J. Updating the accounts: global mortality of the 1918-1920 "Spanish" influenza pandemic. Bull Hist Med. 2002;76:105–115. doi: 10.1353/bhm.2002.0022. [DOI] [PubMed] [Google Scholar]
- 2.Morens DM, Fauci AS. The 1918 influenza pandemic: insights for the 21st century. J Infect Dis. 2007;195:1018–1028. doi: 10.1086/511989. [DOI] [PubMed] [Google Scholar]
- 3.Taubenberger JK, Reid AH, Krafft AE, Bijwaard KE, Fanning TG. Initial genetic characterization of the 1918 "Spanish" influenza virus. Science. 1997;275:1793–1796. doi: 10.1126/science.275.5307.1793. [DOI] [PubMed] [Google Scholar]
- 4.Tumpey TM, Basler CF, Aguilar PV, Zeng H, Solorzano A, Swayne DE, et al. Characterization of the reconstructed 1918 Spanish influenza pandemic virus. Science. 2005;310:77–80. doi: 10.1126/science.1119392. [DOI] [PubMed] [Google Scholar]
- 5.Xu R, McBride R, Paulson JC, Basler CF, Wilson IA. Structure, receptor binding, and antigenicity of influenza virus hemagglutinins from the 1957 H2N2 pandemic. J Virol. 2010;84:1715–1721. doi: 10.1128/JVI.02162-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Masurel N, Marine WM. Recycling of Asian and Hong Kong influenza A virus hemagglutinins in man. Am J Epidemiol. 1973;97:44–49. doi: 10.1093/oxfordjournals.aje.a121483. [DOI] [PubMed] [Google Scholar]
- 7.World Health Organization. Pandemic (H1N1) 2009: update 112 [Internet] Geneva: World Health Organization; 2010. [cited 2010 Oct 4]. http://www.who.int/csr/don/2010_08_06/en/index.html. [Google Scholar]
- 8.Novel Swine-Origin Influenza A (H1N1) Virus Investigation Team. Dawood FS, Jain S, Finelli L, Shaw MW, Lindstrom S, et al. Emergence of a novel swine-origin influenza A (H1N1) virus in humans. N Engl J Med. 2009;360:2605–2615. doi: 10.1056/NEJMoa0903810. [DOI] [PubMed] [Google Scholar]
- 9.Shrestha SS, Swerdlow DL, Borse RH, Prabhu VS, Finelli L, Atkins CY, et al. Estimating the burden of 2009 pandemic influenza A (H1N1) in the United States (April 2009-April 2010) Clin Infect Dis. 2011;52(Suppl 1):S75–S82. doi: 10.1093/cid/ciq012. [DOI] [PubMed] [Google Scholar]
- 10.Dawood FS, Iuliano AD, Reed C, Meltzer MI, Shay DK, Cheng PY, et al. Estimated global mortality associated with the first 12 months of 2009 pandemic influenza A H1N1 virus circulation: a modelling study. Lancet Infect Dis. 2012;12:687–695. doi: 10.1016/S1473-3099(12)70121-4. [DOI] [PubMed] [Google Scholar]
- 11.Simonsen L, Spreeuwenberg P, Lustig R, Taylor RJ, Fleming DM, Kroneman M, et al. Global mortality estimates for the 2009 Influenza Pandemic from the GLaMOR project: a modeling study. PLoS Med. 2013;10:e1001558. doi: 10.1371/journal.pmed.1001558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Fowlkes AL, Arguin P, Biggerstaff MS, Gindler J, Blau D, Jain S, et al. Epidemiology of 2009 pandemic influenza A (H1N1) deaths in the United States, April-July 2009. Clin Infect Dis. 2011;52(Suppl 1):S60–S68. doi: 10.1093/cid/ciq022. [DOI] [PubMed] [Google Scholar]
- 13.Louie JK, Acosta M, Winter K, Jean C, Gavali S, Schechter R, et al. Factors associated with death or hospitalization due to pandemic 2009 influenza A(H1N1) infection in California. JAMA. 2009;302:1896–1902. doi: 10.1001/jama.2009.1583. [DOI] [PubMed] [Google Scholar]
- 14.Suh M, Kang DR, Lee DH, Choi YJ, Tchoe B, Nam CM, et al. Socioeconomic burden of influenza in the Republic of Korea,2007-2010. PLoS One. 2013;8:e84121. doi: 10.1371/journal.pone.0084121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Choi WI, Yim JJ, Park J, Kim SC, Na MJ, Lee WY, et al. Clinical characteristics and outcomes of H1N1-associated pneumonia among adults in South Korea. Int J Tuberc Lung Dis. 2011;15:270–275. [PubMed] [Google Scholar]
- 16.Jain S, Kamimoto L, Bramley AM, Schmitz AM, Benoit SR, Louie J, et al. Hospitalized patients with 2009 H1N1 influenza in the United States, April-June 2009. N Engl J Med. 2009;361:1935–1944. doi: 10.1056/NEJMoa0906695. [DOI] [PubMed] [Google Scholar]
- 17.ANZIC Influenza Investigators. Webb SA, Pettila V, Seppelt I, Bellomo R, Bailey M, et al. Critical care services and 2009 H1N1 influenza in Australia and New Zealand. N Engl J Med. 2009;361:1925–1934. doi: 10.1056/NEJMoa0908481. [DOI] [PubMed] [Google Scholar]
- 18.Lee MC, Kim HY, Kong SG, Kim YM, Park SE, Im YT, et al. Clinical characteristics of pandemic influenza A (H1N1) 2009 pediatric infection in Busan and Gyeongsangnam-do: one institution. Tuberc Respir Dis. 2012;72:493–500. doi: 10.4046/trd.2012.72.6.493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kim YW, Yoon SJ, Oh IH. The economic burden of the 2009 pandemic H1N1 influenza in Korea. Scand J Infect Dis. 2013;45:390–396. doi: 10.3109/00365548.2012.749423. [DOI] [PubMed] [Google Scholar]
- 20.Centers for Disease Control and Prevention. The flu season [Internet] Atlanta: Centers for Disease Control and Prevention; 2014. [cited 2015 Dec 11]. http://www.cdc.gov/flu/about/season/flu-season.htm. [Google Scholar]
- 21.Thompson WW, Shay DK, Weintraub E, Brammer L, Cox N, Anderson LJ, et al. Mortality associated with influenza and respiratory syncytial virus in the United States. JAMA. 2003;289:179–186. doi: 10.1001/jama.289.2.179. [DOI] [PubMed] [Google Scholar]
- 22.Webster RG, Wright SM, Castrucci MR, Bean WJ, Kawaoka Y. Influenza: a model of an emerging virus disease. Intervirology. 1993;35:16–25. doi: 10.1159/000150292. [DOI] [PubMed] [Google Scholar]
- 23.Webster RG, Kendal AP, Gerhard W. Analysis of antigenic drift in recently isolated influenza A (H1N1) viruses using monoclonal antibody preparations. Virology. 1979;96:258–264. doi: 10.1016/0042-6822(79)90189-2. [DOI] [PubMed] [Google Scholar]
- 24.Caini S, Huang QS, Ciblak MA, Kusznierz G, Owen R, Wangchuk S, et al. Epidemiological and virological characteristics of influenza B: results of the Global Influenza B Study. Influenza Other Respir Viruses. 2015;9(Suppl 1):3–12. doi: 10.1111/irv.12319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Uyeki TM. Preventing and controlling influenza with available interventions. N Engl J Med. 2014;370:789–791. doi: 10.1056/NEJMp1400034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Heikkinen T, Ikonen N, Ziegler T. Impact of influenza B lineage-level mismatch between trivalent seasonal influenza vaccines and circulating viruses, 1999-2012. Clin Infect Dis. 2014;59:1519–1524. doi: 10.1093/cid/ciu664. [DOI] [PubMed] [Google Scholar]
- 27.Domachowske JB, Pankow-Culot H, Bautista M, Feng Y, Claeys C, Peeters M, et al. A randomized trial of candidate inactivated quadrivalent influenza vaccine versus trivalent influenza vaccines in children aged 3-17 years. J Infect Dis. 2013;207:1878–1887. doi: 10.1093/infdis/jit091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Tinoco JC, Pavia-Ruz N, Cruz-Valdez A, Aranza Doniz C, Chandrasekaran V, Dewe W, et al. Immunogenicity, reactogenicity, and safety of inactivated quadrivalent influenza vaccine candidate versus inactivated trivalent influenza vaccine in healthy adults aged ≥18 years: a phase III, randomized trial. Vaccine. 2014;32:1480–1487. doi: 10.1016/j.vaccine.2014.01.022. [DOI] [PubMed] [Google Scholar]
- 29.Centers for Disease Control and Prevention. Vaccination: who should do it, who should not and who should take precautions [Internet] Atlanta: Centers for Disease Control and Prevention; 2015. [cited 2015 Dec 11]. http://www.cdc.gov/flu/protect/whoshouldvax.htm. [Google Scholar]