

Abstract
Previous studies suggest strong associations between exposure to weight conscious peer groups and increased levels of disordered eating. This association has been attributed to socialization effects (i.e., membership leads to disordered eating); however, selection effects (i.e., selecting into peer groups based on genetic and/or environmental predispositions toward disordered eating) could contribute to or even account for these associations. The current study was the first to use a co-twin control design to disentangle these types of selection factors from socialization effects. Participants included 610 female twins (ages 8–14) drawn from the Michigan State University Twin Registry. To comprehensively examine a range of eating pathology, several disordered eating attitudes and behaviors (e.g., body dissatisfaction, binge eating) were examined via self-report questionnaires. Questionnaires also were used to assess peer group emphasis on body weight and shape. Replicating previous results, significant individual-level associations were found between membership in weight conscious peer groups and disordered eating. However, co-twin control analyses indicated that these associations were largely due to genetic and/or shared environmental selection factors rather than pure socialization effects. Importantly, results remained unchanged when controlling for pubertal status, suggesting that effects do not vary across developmental stage. Overall, these findings question whether associations between weight conscious peer groups and disordered eating are due entirely to socialization processes. Future studies are needed to identify the specific genetic and/or shared environmental factors that may drive selection into weight conscious peer groups.
Keywords: selection, socialization, co-twin control, disordered eating, weight conscious peer groups
Prior research has demonstrated significant associations between weight conscious peer groups (e.g., groups that emphasize thin body weights/shapes, dieting, and appearance) and levels of disordered eating. Multiple cross-sectional studies have shown associations between peer groups’ emphasis on body weight and excessive weight concerns, dieting and body dissatisfaction in girls (Levine & Smolak, 1992; Taylor et al., 1998; Vander Wal & Thelen, 2000; Wertheim, Paxton, Schutz, & Muir, 1997). Likewise, body image concerns, dietary restraint, the use of extreme weight-loss behaviors (Paxton, Schutz, Wertheim, & Muir, 1999), and binge eating (Goldschmidt et al., 2014) have been shown to be similar within friendship groups. Longitudinal studies have corroborated cross-sectional effects by demonstrating significant, prospective associations between peer groups’ initial level of weight concerns and disordered eating symptoms 6 months to 10 years later (Crandall, 1988; Haines, Neumark-Sztainer, Eisenberg, & Hannan, 2006; Keel, Forney, Brown, & Heatherton, 2013; Myer & Waller, 2001).
However, the mechanisms underlying these significant associations remain largely unknown. Researchers have proposed socialization effects (Crandall, 1988; Zalta & Keel, 2006), such that disordered eating attitudes and behaviors are learned through observing these cognitions/behaviors within peer groups. Two studies have indirectly examined these social explanations by exploring the convergence versus divergence of disordered eating within peer groups. Crandall (1988) found that, at the beginning of the academic year, a female college student’s level of binge eating was equally similar to her sorority friends as to her sorority as a whole, whereas at the end of the year, the student’s level of binge eating was significantly more correlated with members of her sorority friendship group. Likewise, Zalta and Keel (2006) found that college roommates who cohabited during the academic year became less similar to each other in bulimic symptoms (i.e., the EDI bulimia subscale; Garner, 1991) over their summer break away. These studies indirectly support socialization theories, as they suggest that time together increases similarity in disordered eating symptoms amongst peers (Crandall, 1988), while time apart decreases peers similarity in these symptoms (Zalta & Keel, 2006).
However, other studies suggest that pre-existing factors (i.e., selection effects - see Burt et al., 2010; McGue, Osler & Christesen, 2010) may also contribute to associations between weight conscious peer groups and increased disordered eating. Selection occurs when individuals seek out peer groups that are in line with their own attitudes and beliefs. In the case of disordered eating, girls who strongly value thin body weights and shapes might seek out peer groups who also focus on these characteristics. These weight conscious peer groups may then reinforce and strengthen their underlying beliefs and lead to increased disordered eating within the group. In this case, selection effects may drive the association between weight conscious peers and disordered eating by grouping like-minded individuals, rather than this association being driven solely by exposure to a particular set of peers.
Three studies have examined this possibility, and two found evidence for possible selection effects. Myer and Waller (2001) investigated convergence/divergence of bulimic symptoms in unselected college roommates across three time points (i.e., 1 week after move in, and then 10 and 24 weeks later). Unselected roommates did not become more similar to each other in bulimic symptoms; in fact, they became more dissimilar, as evidenced by a divergence in bulimic symptoms over the course of the study (Myer & Waller, 2001). Rayner et al. (2013) examined whether adolescents’ (ages 12 to 14) similarity to their peer groups in weight/shape concerns was prospectively associated with an increased likelihood of staying in that peer group across 12 and 24 months. Results indirectly support the presence of selection effects, as girls were more likely to stay in friendship groups that were more similar in body dissatisfaction and bulimic behaviors. Importantly, one study failed to find peer selection effects, as female college students who selected their roommates were not more similar in their levels of drive for thinness, body dissatisfaction, or bulimic symptoms than students who were unselected (i.e., randomly paired; Gilbert & Myer, 2004).
Overall, findings are mixed as to whether socialization or selection accounts for peer group/disordered eating associations, as an equal number of studies support each type of process (N = 2 for each). However, a relatively small number of studies have been conducted, and most have not simultaneously examined both socialization and selection factors. Indeed, although Crandall (1988) and Zalta and Keel (2006) showed socialization effects, they did not examine/control for initial selection into those peer groups. Thus, it remains unknown whether socialization alone, or socialization that is dependent upon initial selection into like-minded peer groups, accounts for associations between weight conscious peer groups and disordered eating.
One approach for simultaneously examining both processes is the co-twin control study. The co-twin control design is based on the counterfactual model (McGue et al., 2010) that states that the best way to determine whether a risk factor (e.g., exposure to weight conscious peers) is causal for a particular outcome (versus due to selection processes) is to examine the outcome when the individual is exposed to the risk factor and when the individual is not exposed. If the outcome is the same regardless of whether the individual is exposed or not-exposed, then the risk factor is not causal (i.e., it does not affect the outcome). However, if the individual’s outcome is different depending on whether he/she was exposed, then it is likely that the risk factor does lead to the outcome and risk factor/outcome associations are not due to selection factors. Unfortunately, for most risk factors, it is impossible to observe an outcome for both exposure and non-exposure simultaneously in one person. Consequently, the counterfactual model attempts to get as close as possible to this ideal situation by comparing exposed and unexposed groups who are matched on as many key characteristics and potential selection factors as possible. This matching ensures that exposure to the risk factor is not based on selection via pre-existing traits, as the two groups are matched on traits that could lead to selection into the exposed group.
Importantly, the co-twin control method provides a valuable extension of the counterfactual model by using co-twin discordance on a risk factor as a predictor of an outcome. This method eliminates the need for matching since twins are already matched on key demographic characteristics (i.e., age, socioeconomic status, rearing family, etc.). Moreover, the model improves upon the typical counterfactual model by matching twins on shared environmental influences (i.e., environmental influences shared by siblings, e.g., parental divorce, parental discipline, etc.) and genetic predispositions, as twins reared together share 100% of their shared environment, and ~50% (for dizygotic [DZ] twins) or 100% (for monozygotic [MZ] twins) of their segregating genes. The ability to control for and model genetic risk is particularly important for disordered eating, as twin and adoption studies show significant genetic influences (i.e., heritability ≥ 50%) on clinical eating disorders and their symptoms (Bulik, Sullivan & Kendler, 1998; Kaye, Klump, Frank, & Strober, 2000; Klump, Burt, Spanos, McGue, Iacono, & Wade, 2010; Klump et al., 2003; Klump, Miller, Keel, McGue, & Iacono, 2001).
Capitalizing on the use of twins, the co-twin control study compares three different sets of regression results: (1) individual-level effects (i.e., the extent to which a twin’s exposure to weight conscious peers predicts her own level of disordered eating), (2) effects in DZ twin pairs only (i.e., the extent to which co-twin discordance on exposure to weight conscious peers predicts each DZ twin’s level of disordered eating), and (3) effects in MZ twins only (i.e., the extent to which co-twin discordance on exposure to weight conscious peers predicts each MZ twin’s level of disordered eating). The presence of significant individual-level effects would be similar to what has been shown in previous cross-sectional research - they simply show significant associations between the exposure and outcome, not differentiating socialization from selection effects.
By contrast, the MZ and DZ twin pair estimates help determine if individual-level associations are due to socialization or selection effects. Because MZ and DZ co-twins share 100% of their shared environment, discordance between them on the exposure variable cannot be due to shared environmental selection effects. Thus, if shared environmental factors (e.g., socioeconomic status, parenting style) are important for selection into weight conscious peer groups, significant associations between exposure and disordered eating in either discordant MZ or DZ twins will not be observed1. If genetic factors are important for selection into weight conscious peer groups, then significant associations between exposure to weight conscious peers and disordered eating in discordant DZ twins will be observed, since these twins only share 50% of their genes. By contrast, an association in discordant MZ twin pairs would not be observed, since these twins share 100% of their genes – in this case, discordance in exposure to weight conscious peers cannot be due to differences in genetic factors between MZ co-twins.
Figure 1 provides a summary of expected results if socialization and/or selection effects are present. Scenario A shows expected results if associations between exposure to weight conscious peers and disordered eating are due entirely to socialization processes. In this case, there are significant associations with similar magnitude within individual-level and within discordant MZ and DZ twin pairs, suggesting that exposure to weight conscious peers increases disordered eating on the individual level and within-twin pairs even when shared environmental and genetic selection processes are controlled. Scenarios B and C show expected results if selection is present. In both cases, the association between exposure to weight conscious peer groups and disordered eating in discordant twins is attenuated, suggesting that the association is due to either genetic and/or shared environment selection effects. Scenario B would suggest genetic selection effects only, as there is still an association for DZ twins who share less genetic material than MZ twins. Scenario C would suggest shared environmental and/or genetic and shared environmental selection effects, since associations are no longer significant or are reduced in magnitude when controlling for shared environmental and genetic selection processes. Since no portion of our sample controls for 100% of genetic influences and 0% of shared environmental influences (MZ twins reared apart would be one such sample), we are unable to detect if selection effects identified in Scenario C are due completely to shared environmental effects or to both genetic and shared environmental effects. Nonetheless, the ability to separate socialization, selection due to genetic effects only, and selection due to genetic and/or shared environmental effects represents a significant advance over prior studies.
Figure 1. Summary of Potential Results of Co-Twin Control Analysis.
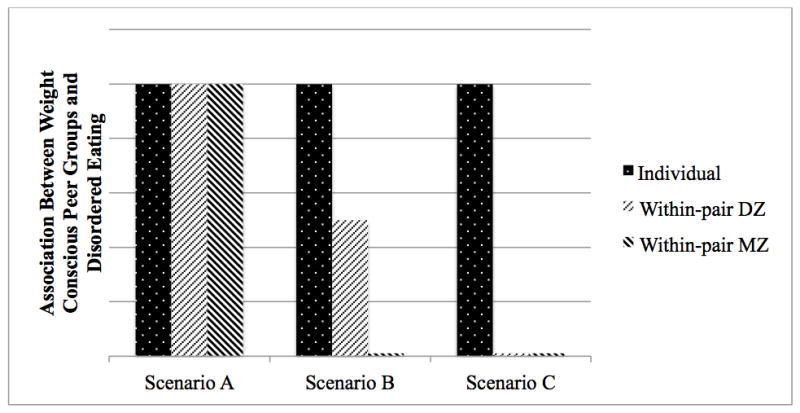
Scenario A would indicate that the association between weight conscious peer groups and disordered eating are due completely to socialization processes, as there are significant associations on the individual-level and within discordant MZ and DZ twin pairs. Scenario B would indicate genetic selection effects only, as there is still an association for DZ twins who share less genetic material (approximately 50%) than MZ twins (approximately 100%). Scenario C would suggest genetic and/or shared environment selection effects, since when controlling for these types of influences, associations are non-significant or reduced in magnitude.
Using the co-twin control method, the present study directly explored socialization versus selection effects in associations between weight conscious peer groups and disordered eating in pre-adolescent and young adolescent female twins. Although previous research has primarily focused on college-aged women, peer groups become more developmentally important in early adolescence (e.g., ages 10–14; Steinberg & Monahan, 2007) when disordered eating often begins. Our focus on this younger age group therefore may highlight patterns of effects that are unique to the early (and critical) stages of disordered eating development. Nonetheless, because of our younger age range, we focus our analyses on a variety of disordered eating attitudes and behaviors (rather than clinical disorders) in order to maximize power and examine the full spectrum of eating pathology.
Methods
Participants
The current study used archival twin data (N = 610 female twins ages 8–14 years, M = 11.63, SD = 2.10; 52.8% MZ, 47.2% DZ) from the Twin Study of Mood, Behavior, and Hormones during Puberty (MBHP). This study recruits all of its twins from the Michigan Twins Project (MTP), a population-based recruitment database within the Michigan State University Twin Registry (MSUTR; Burt & Klump, 2013; Klump & Burt, 2006) that recruits twins ages 3–25 and 30–50 years using birth records in collaboration with the Michigan Department of Community Health (see Burt & Klump (2013) for recruitment details). Although the MTP is an on-going project, the current response rate (57%) is on par or better than that of other twin registries using similar recruitment methods (Burt & Klump, 2013; Iacono & McGue, 2002), and participating twins are representative of the broader population in terms of racial/ethnic diversity, family income, parental education, and a range of other variables (including emotional problems – see Burt & Klump, 2013).
The primary aim of the on-going MBHP study is to investigate the influence of ovarian hormones on phenotypic and genetic risk for disordered eating during puberty. Thus, several inclusion/exclusion criteria were used (e.g., no recent psychotropic, steroid, or other medication use that is known to influence hormone functioning) that could conceivably alter the composition and disordered eating characteristics of the recruited sample. Notably, however, twins who were assessed for the MBHP were not significantly different from non-participating MTP families in terms of overall disordered eating symptoms (e.g., body dissatisfaction, dieting, binge eating) (t(391)= −0.95 p = 0.35) or BMI (t(375)= −0.84 p = 0.40). The recruited MBHP was also highly representative of the MTP sample and the general population of Michigan in terms of ethnic/racial distributions, with 4% of pairs identifying as Hispanic and 81.5% identifying as Caucasian, 8.3% as African American, 0.2% as American Indian/Alaskan Native, and 9.3% as multiple races.
Zygosity Determination
The MSUTR determines zygosity using a well-validated physical similarity questionnaire (Lykken, Bouchard Jr, McGue, & Tellegen, 1990) that has been shown to be 95% accurate when compared to genotyping (Peeters, Van Gestel, Vlietinck, C. Derom, & R. Derom, 1998). For the MSUTR sample used in this study, both twins, their mother, and two research assistants evaluated the physical similarities independently. Reports were then compared and any discrepancies were resolved through review of questionnaire data and twin photographs by one of the principal investigators (KLK) or by examination of DNA markers (Burt & Klump, 2013; Klump & Burt, 2006).
Measures
All measures were completed by the twins. Although we did not have parental reports of weight-conscious peer groups, we did have parental reports of twin disordered eating (via a parent report version of the Minnesota Eating Behavior Survey see description below). However, similar to previous studies (Kolko & Kazdin, 1993), the parental reports did not significantly correlate with the twin’s report of disordered eating (r’s mainly <.16), and individual-level associations between parental reported disordered eating and twin reported weight-conscious peer groups were small in magnitude (average r = .13). These non-significant associations likely reflect the lack of information parents have about their child’s eating disorder symptoms, particularly the cognitive symptoms (e.g., weight preoccupation) and behavioral symptoms that children often hide (e.g., purging). Thus, in the current study, we focus on twin reported symptoms in all analyses.
Exposure to Weight Conscious Peer Groups
As described below, we used several measures to assess exposure to weight conscious peer groups, many of which seem to tap related constructs. Although intercorrelations between scores on peer exposure questionnaires were significant and positive (rs = .31–.56, Mean = .42), all correlations were small-to-moderate in magnitude, with only 10–31% shared variance. This relatively limited amount of shared variance suggests that the questionnaires tap different aspects of weight conscious peer group exposure. Thus, all analyses were conducted separately for each questionnaire. Notably, these questionnaires have been studied much less frequently than those used to assess disordered eating, and so psychometric data is limited (but is still described below).
The Perceived Friend Preoccupation with Weight and Dieting Scale (Schutz, Paxton, & Wertheim, 2002) is a 9-item questionnaire aimed at assessing twins’ perceptions of the frequency of weight- and dieting- related thoughts and behaviors among their friends. This self-report questionnaire has participants rate their response on a 5-point scale from 1 (never) to 5 (very often), with high scores representing more perceived importance of weight and dieting among friendship groups. Factor analysis found all items load on a single factor with item-total correlations ≥ .52 (Schutz et al., 2002). Cronbach’s alpha in a sample of adolescent girls in grades 7, 8, and 10 was excellent at .87 (Schutz et al., 2002). Similarly, Cronbach’s alpha in the present study was excellent at .86.
The Appearance Conversations with Friends (Jones, Vigfusdottir, & Lee, 2004) is a 5-item questionnaire modified from the original Magazines as a Source of Influence Scale (Levine, Smolak, & Hayden, 1994). The current scale assesses the frequency of discussions about current and desired body shape with friends (e.g., “My friends and I talk about what we would like our bodies to look like”). Cronbach’s alpha of .85 indicated excellent reliability for a sample of adolescent females in grades 7, 8, 9, and 10 (Jones et al., 2004). Cronbach’s alpha in the present study was .88.
The Friends as a Source of Influence Scale (Paxton et al. 1999) is a 5-item questionnaire that asks participants to rate how important their friends are in influencing their opinions of the perfect body, diet products, exercise, and dieting (e.g. “Your idea of the perfect body”) on a 5-point scale from 1 (Not at all important) to 5 (Very important). Cronbach’s alpha of .87 indicates good internal consistency in a study of 10th grade girls (mean age = 15.5) (Paxton et al., 1999). In the present study, the Cronbach’s alpha was .84.
The Peer Attribution Scale (Lieberman, Gauvin, Bukowski, & White, 2001) includes 8-items assessing appearance-related attributions (e.g., “My friends would like me more if I lost weight) from friends on a 6-point Likert scale (ranging from “false” to “true”). The original scale includes items referring to same-sex and opposite-sex friends; however, in the current sample, we used a modified version (Shroff & Thompson, 2006) that refers to any friend (same- or opposite-sex) and deletes items that are specific to opposite-sex friends only (e.g., “If I was thinner, boys would be more attracted to me”). This modified scale exhibited a Cronbach’s alpha of .85 in past research (Shroff & Thompson, 2006) and .80 in the current sample.
Disordered Eating
The Minnesota Eating Behavior Survey (MEBS; von Ranson, Klump, Iacono & McGue, 2005)2 is a 30-item questionnaire made up of true/false questions that assesses a range of disordered eating symptoms. This measure was developed for use with children as young as 10-years-old. Previous factor analyses (Klump, McGue, & Iacono, 2000; von Ranson et al., 2005) produced four factors: Body Dissatisfaction (i.e., assessing discontent with body size and shape), Compensatory Behaviors (i.e., assessing the use of, and thoughts of using, self-induced vomiting and other inappropriate compensatory behaviors to control weight), Binge Eating (i.e., assessing thinking about binge eating as well as engaging in binge eating and/or secretive eating) and Weight Preoccupation (i.e., assessing preoccupation with weight, eating, and dieting). The current study focused on the Body Dissatisfaction, Binge Eating and Weight Preoccupation subscales, as well as the MEBS Total Score (i.e., a measure of overall levels of disordered eating that is the sum of all 30 items on the questionnaire). The Compensatory Behaviors subscale was excluded from analyses due to the low prevalence of compensatory behaviors in the sample (i.e., 90% of participants scored a “0” on this subscale).
The MEBS subscales that were examined demonstrate good three-year stability (r = 0.32–0.59) in adolescents (age 11–14) with the Total score being the most stable (r = 0.59) followed by the scales measuring attitudes (i.e., Weight Preoccupation and Body Dissatisfaction; r = 0.51 and r = 0.53, respectively) and then behaviors (i.e., Binge Eating; r = 0.32) (von Ranson et al., 2005). The MEBS subscales also demonstrate adequate convergent validity with similar types of scales from the Eating Disorder Examination Questionnaire (EDE-Q; Fairburns & Beglin, 1994), with inter-scale correlations ranging from .74–.83 (von Ranson et al., 2005). Good criterion-related validity is present for the MEBS as well, as girls with eating disorders (i.e., either anorexia nervosa [AN] or bulimia nervosa [BN]) were shown to have significantly higher scores on the Body Dissatisfaction subscale, Weight Preoccupation subscale, and Total Score than controls (von Ranson et al., 2005). Additionally, participants with BN had significantly higher scores on the Binge Eating subscale than controls (von Ranson et al. 2005). Finally, internal consistencies in previous studies have ranged from 0.70–0.85 (von Ranson et al., 2005) and were 0.68–0.88 in the current study.
The Eating in the Absence of Hunger for Children and Adolescents (EAH-Child; Tanofsky-Kraff et al., 2008) is a 14-item questionnaire developed to assess precipitants to eating when not hungry in children and adolescents ages 6 through 19. This questionnaire includes five emotional precipitants to eating when one is not hungry (i.e., feeling sad or depressed, angry or frustrated, anxious or nervous, tired, bored) and two external precipitants (i.e., sensory cues, social cues). Using a 5-point Likert scale with answers ranging from 1 (“Never”) to 5 (“Always”), participants are asked to select the frequency in which they eat beyond satiation and in the absence of hunger in response to each of the 7 precipitants. Factor analysis generated three subscales on this measure Negative Affect (i.e., eating in the absence of hunger in response to feeling sad or depressed, angry or frustrated, or anxious or nervous), External Eating (i.e., eating in absence of hunger when food looks, tastes, or smells good and when others are eating), and Fatigue/Boredom (i.e., eating in absence of hunger when feeling tired or bored) (Tanofsky-Kraff et al., 2008). Significant test-retest correlations (r = 0.65–0.70) have been observed for these scales across 5–565 days (M = 150 days, SD = 130), and they show good convergent validity with interview-based reports of loss of control over eating (Tanofsky-Kraff, et al., 2008). Finally, internal consistency was excellent for all subscales in past studies (0.80–0.88; Tanosky-Kraff et al., 2008) and the current sample (0.75–0.84).
The Emotional Eating Scale- Adapted for Children and Adolescents (EES-C; Tanofsky-Kraff et al., 2007) is a 26-item, self-report questionnaire designed to assess the urge to cope with negative affect through eating. Participants are presented with a list of emotions (e.g., resentful, discouraged, worn out) and asked to rate their desire to eat in the presence of each emotion on a 5-point scale from “I have no desire to eat” to “I have a very strong desire to eat.” A factor analysis generated three subscales that included: 1) eating in response to anxiety, anger, and frustration (e.g., furious, worried); 2) eating in response to depressive symptoms (e.g., down, sad); and 3) eating in response to feeling unsettled (e.g., excited, resentful). Good temporal stability was observed over an average of three months with intraclass correlations ranging from 0.59–0.74, depending upon the subscale (Tanofsky-Kraff et al., 2007). All subscales exhibited excellent internal consistency in prior work (0.83–0.93; Tanosky-Kraff et al, 2007) and the current study (0.72–0.92).
Covariate
Pubertal status was included in the models to ensure that associations between exposure to weight conscious peer groups and disordered eating were not due to this potentially confounding factor3. Indeed, past research has demonstrated that pubertal development is related to both phenotypic (Klump et al., 2013) and genetic risk (Culbert, Burt, McGue, Iacono, & Klump, 2009; Klump et al., 2000; Klump, Burt, McGue, & Iacono, 2007; Klump, McGue, & Iacono, 2003) for disordered eating symptoms. Further, a positive association was found between pubertal development and disordered eating within the current study (average r = 0.15), as well as pubertal development and exposure to weight conscious peer groups (average r = 0.28).
Pubertal development was assessed using the self-report Pubertal Development Scale (PDS; Peterson, Crockett, Richards, & Boxer, 1988). The PDS which asks participants to assess their pubertal development based on physical markers of puberty (i.e., height spurts, body hair growth, skin changes, breast development, onset of menarche). Participants rated the development of these physical markers on a 4-point scale: (1) development has not yet begun; (2) development has barely started; (3) development is definitely underway; and (4) development seems completed. An exception to this 4-point scale was the coding for menses, which was coded dichotomously as either absent (1) or present (4). The ratings of each physical marker are summed and averaged to obtain an overall PDS score, with higher scores representing more advanced pubertal development. The PDS correlates highly (r = .61–.67) with physician ratings of pubertal development (Peterson et al., 1988) and exhibited good internal consistency (alpha = .77) in the present sample.
Statistical Analyses
Data Preparation
Disordered eating and weight conscious peer group data were log transformed prior to analyses to control for positive skew. All scores were also standardized for the co-twin control analyses in order to allow for comparisons of effects across measures and analyses.
Initial Associations
Before examining associations between exposure to weight conscious peer groups and disordered eating, we first examined the extent of “discordance” in peer group exposure in MZ and DZ twins to ensure adequate variability in the independent variable. We calculated within-pair difference scores (i.e., absolute value of the difference between Twin 1’s and Twin 2’s score) for the peer exposure variables and compared the scores for MZ versus DZ twins using independent samples t-tests.
Pearson correlations were used to investigate within-person associations between exposure to weight conscious peer groups and disordered eating. These analyses were essentially replications of cross-sectional studies that examine whether individuals with weight conscious peer groups have significantly higher levels of disordered eating.
Co-Twin Control Analyses
Co-twin control analyses were then used to examine whether phenotypic associations between exposure to weight conscious peer groups and disordered eating symptoms were due to purely socialization factors (i.e., higher weight conscious peer groups lead to higher disordered eating) or selection (i.e., individuals who are more inclined towards disordered eating are more likely to choose weight conscious peer groups). We used mixed linear models (MLMs) to examine these possibilities and also to control for the non-independence of the twin data (by nesting a level-1 variable (individual twin) within a level-2 unit (twin pair)).
Separate MLMs were used to examine individual-level effects (i.e., associations between exposure to weight conscious peer groups and disordered eating within each twin) versus within-twin pair effects (i.e., associations between co-twin discordance in exposure to weight conscious peer groups and disordered eating in each twin). More specifically, the individual-level effects were estimated in models that regressed the disordered eating scores onto the exposure variable using the following equation:
where Yij is the observed outcome (i.e., disordered eating) for the jth twin (j= 1 or 2) in the ith twin pair (i= 1,2,…, N), β0 is the intercept term, β1 is the individual-level effect of exposure (i.e., weight conscious peer groups) on outcome (i.e., disordered eating), xij is the level of exposure for the jth twin in the ith twin pair, and εij is the residual (correlated across two members of a twin pair).
By contrast, the within-pair effects were modeled using both a within-pair (βW) and a between-pair (βB) effect that were estimated using the following regression model:
where, βW is the within-pair effect of exposure to weight conscious peer groups, xij is the level of exposure for the jth twin in the ith twin pair, xi is the mean exposure index for the ith twin pair, βB is the between-pair effect of exposure. In order to appropriately model all of these effects, the MLMs for the within-pair analyses included five predictor variables and one covariate (i.e., pubertal status): 1) each twin’s score on the exposure to weight conscious peers scale (i.e., the individual-level effect); 2) the difference between each co-twin’s score on the weight conscious peers scale and the pair’s mean on the scale (i.e., the within-pair effect); 3) a dummy coded zygosity variable that identifies MZ versus DZ twins; 4) pubertal status; 5) an interaction between the zygosity variable and the twin’s score on the weight conscious peers scale; 6) an interaction between the zygosity variable and the within-twin pair difference score. These latter interaction variables estimated the between-family effects (i.e., zygosity x exposure to weight-conscious peers) and tested for significant differences in within-pair effects between MZ and DZ twins (i.e., zygosity x within-twin pair difference scores). Notably, in order to obtain estimates of all effects in MZ and DZ twins separately, we ran two sets of MLMs – one in which zygosity was coded with the DZ twins as the control (i.e., MZ twins = 2 and DZ twins = 1), and the other with MZ twins as the control (i.e., MZ twins = 1, DZ twins = 2). The first model provided estimates of within-pair exposure for the MZ twins, while the second model provided these same estimates for DZ twins.
We conducted individual models for each of the disordered eating outcome variables (e.g., Body Dissatisfaction, Binge Eating, etc.) with each peer group exposure questionnaire (e.g., Perceived Friend Preoccupation with Weight and Dieting, etc.). Due to the relatively large number of models examined, a conservative p value of .01 was used for all analyses.
Results
Preliminary Analyses
A range of disordered eating attitudes and behaviors and exposure to weight conscious peer groups was present in our sample (see Table 1). A total of 3.9% of twins scored above the clinical cut-off (score = 15.55) for the MEBS Total Score (von Ranson et al., 2005), which is a relatively high percentage, given the lower age range of our sample (M = 11.63; SD = 2.10). Moreover, a wide range of scores were present on the exposure to weight conscious peer groups scales, as 10.9%–14.4% of twins scored ≥1 SD above the mean on these scales.
Table 1.
Descriptive Statistics for Disordered Eating and Peer Exposure Measures (N = 538–609).
| Measures | Mean | SD | Range in Sample |
|---|---|---|---|
| Disordered Eating Measures | |||
| Minnesota Eating Behavior Survey (MEBS) | |||
| Total Score (Possible range 0–30) | 4.29 | 4.67 | 0–27 |
| Body Dissatisfaction (Possible range 0–6) | 0.94 | 1.50 | 0–6 |
| Binge Eating (Possible range 0–7) | 0.84 | 1.30 | 0–7 |
| Weight Preoccupation (Possible range 0–8) | 1.66 | 1.98 | 0–8 |
| Eating in the Absence of Hunger (EAH) | |||
| Negative Affect (Possible range 1–5) | 1.19 | 0.41 | 1.00–3.50 |
| External Eating (Possible range 1–5) | 2.03 | 0.74 | 1.00–4.75 |
| Fatigue/Boredom (Possible range 1–5) | 1.44 | 0.61 | 1.00–5.00 |
| Emotional Eating Survey(EES) | |||
| Anxiety, Anger, & Frustration (Possible range 1–5) | 1.46 | 0.60 | 1.00–4.25 |
| Depression (Possible range 1–5) | 1.65 | 0.69 | 1.00–4.57 |
| Unsettled (Possible range 1–5) | 1.59 | 0.67 | 1.00–5.00 |
| Peer Exposure Questionnaires | |||
| Perceived Friend Preoccupation with Weight and Dieting (Possible range 9–45) | 14.45 | 5.49 | 9–37 |
| Appearance Conversations with Friends (Possible range 5–25) | 9.00 | 4.28 | 5–25 |
| Friends as a Source of Influence (Possible range 5–25) | 7.54 | 3.51 | 5–25 |
| Peer Attribution Scale (Possible range 4–24) | 6.04 | 3.47 | 4–24 |
Note. MEBS = Minnesota Eating Behaviors Survey; EAH = Eating in the Absence of Hunger; EES= Emotional Eating Scale
Within-pair difference scores for peer exposure variables are presented in Table 2. Interestingly, and similar to previous research (Rushton & Bons, 2005), significantly smaller differences in exposure to weight conscious peer groups were observed in MZ as compared to DZ pairs. However, effect sizes were small (d’s = 0.11 to 0.21), suggesting that overall, the degree of co-twin “discordance” in peer groups was relatively similar in MZ and DZ twins.
Table 2.
Means and Standard Deviations for Co-Twin Difference Scores on Weight Conscious Peer. Group Scales (N=519–629)
| Peer Exposure Questionnaires: | MZ Pairs (N = 322) | DZ Pairs (N = 288) | t (df) | p | Cohen’s d |
|---|---|---|---|---|---|
| Perceived Friend Preoccupation with Weight and Dieting | 3.47 (4.15) | 3.91 (3.57) | −1.26 (493) | 0.21 | 0.11 |
| Appearance Conversation with Friends | 2.68 (2.94) | 3.30 (3.07) | −2.44 (542.2) | 0.02 | 0.21 |
| Friends as a Source of Influence | 2.45 (3.22) | 2.82 (3.00) | −1.40 (547) | 0.16 | 0.12 |
| Peer Attribution Scale | 1.92 (2.83) | 2.36 (2.96) | −1.77 (550) | 0.08 | 0.15 |
Note. Values are the mean (standard deviation) of the co-twin difference scores for the weight conscious peer group scales. Difference scores were calculated by taking the absolute value of Twin 1-Twin 2.
Initial Phenotypic Associations
Within-person, phenotypic associations between weight conscious peer groups and disordered eating are presented in Table 3. Significant positive associations were found between all disordered eating and peer group scores; however, correlations varied in magnitude depending upon the questionnaires. Stronger correlations were observed between weight conscious peer groups and the disordered eating symptoms assessed with the MEBS (r’s = .25–.48) as compared to symptoms assessed with the EAH-C and EES-C scales (r’s = .10–.32).
Table 3.
Pearson Correlations examining Within-Person Associations between Weight Conscious Peer Groups and Disordered Eating.
| Weight Conscious Peer Group Measures | ||||
|---|---|---|---|---|
|
| ||||
| Disordered Eating Measures | Perceived Friend Preoccupation with Weight and Dieting (N=535–561) | Appearance Conversations with Friends (N=569–596) | Friends as a Source of Influence (N=566–592) | Peer Attribution Scale (N=566–593) |
| Minnesota Eating Behavior Survey (MEBS) | ||||
| Total Score | 0.43** | 0.36** | 0.43** | 0.50** |
| Weight Preocc. | 0.37** | 0.31** | 0.41** | 0.41** |
| Body Diss. | 0.39** | 0.31** | 0.27** | 0.44** |
| Binge Eating | 0.35** | 0.29** | 0.32** | 0.36** |
| Eating in the Absence of Hunger (EAH) | ||||
| Negative Affect | 0.27** | 0.23** | 0.30** | 0.26** |
| External Eating | 0.27** | 0.22** | 0.21** | 0.20** |
| Fatigue/Boredom | 0.31** | 0.24** | 0.23** | 0.30** |
| Emotional Eating Survey (EES) | ||||
| Anxiety, Anger and Frustration | 0.13* | 0.18** | 0.22** | 0.18** |
| Depression | 0.25** | 0.27** | 0.25** | 0.25** |
| Unsettled | 0.12* | 0.11* | 0.16** | 0.13* |
p< 0.05,
p<0.01
Co-Twin Control Analyses
Overall, findings from the co-twin control analyses suggested that the vast majority of within-person associations observed in Table 3 were accounted for by effects that are consistent with genetic and/or environmental selection (i.e., Scenario C). Table 4 displays results for all associations showing Scenario C. In many cases, the MZ and/or DZ within-pair estimates were not significantly different from zero, suggesting minimal associations between twin discordance in weight-focused peer groups and disordered eating when controlling for genetic and/or shared environmental factors. At times, a within-pair estimate was statistically significant (e.g., the MZ within-pair estimate for associations between MEBS Body Dissatisfaction and Perceived Friend Preoccupation), but in all cases, there were no significant differences between the MZ and DZ within-pair estimates (i.e., the “Ex x Zyg” interaction was non-significant), and all within-pair estimates were significantly reduced in magnitude (p < .05) as compared to the individual-level estimates (see Cumming (2009) for methods for beta comparisons). All of these results suggest the presence of Scenario C (i.e., genetic and/or shared environmental selection), as associations between exposure to weight-focused peers and disordered eating are significantly diminished when controlling for genetic and/or shared environmental factors.
Table 4.
Results from Co-Twin Control Results that Resemble Scenario C (i.e., Genetic and/or Environmental Selection).
| Exposure Questionnaires | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Perceived Friend Preoccupation
with Weight and Dieting (N=535–561) |
Appearance Conversations with
Friends (N=569–596) |
Friends as a Source of Influence (N=566–592) | Peer Attribution Scale (N=566–593) | |||||||||||||||||
|
| ||||||||||||||||||||
| Outcome Measures |
Ind. MZ (β) |
Ind. DZ (β) |
Within- Pair MZ (β) |
Within- Pair DZ (β) |
Ex x Zyg (β) |
Ind. MZ (β) |
Ind. DZ (β) |
Within- Pair MZ (β) |
Within- Pair DZ (β) |
Ex x Zyg (β) |
Ind. MZ (β) |
Ind. DZ (β) |
Within- Pair MZ (β) |
Within- Pair DZ (β) |
Ex x Zyg (β) |
Ind. MZ (β) |
Ind. DZ (β) |
Within- Pair MZ (β) |
Within- Pair DZ (β) |
Ex x Zyg (β) |
| Minnesota Eating Behaviors Survey | ||||||||||||||||||||
| Total Score | -- | -- | -- | -- | -- | 0.35* | 0.23* | 0.19* | 0.07 | 0.11 | 0.35* | 0.35* | 0.15* | 0.09 | 0.07 | -- | -- | -- | -- | -- |
| Body Diss | 0.29* | 0.23* | 0.13* | <0.01 | 0.13 | 0.23* | 0.14† | 0.10 | <0.01 | 0.10 | 0.21* | 0.25* | 0.08 | 0.02 | 0.06 | 0.26* | 0.46* | 0.07 | 0.14* | 0.07 |
| Binge Eating | 0.37* | 0.25* | 0.17* | 0.06 | 0.11 | -- | -- | -- | -- | -- | 0.30* | 0.30* | 0.11 | 0.13* | 0.01 | 0.18* | 0.43* | 0.10 | 0.19* | 0.09 |
| Weight Preocc | -- | -- | -- | -- | -- | 0.35* | 0.23* | 0.18* | 0.07 | 0.11 | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- |
| Eating in the Absence of Hunger | ||||||||||||||||||||
| Neg Affect | 0.29* | 0.24* | 0.12 | 0.10 | 0.03 | 0.15† | 0.23* | 0.08 | 0.13 | 0.05 | 0.28* | 0.27* | 0.10 | 0.09 | <0.01 | -- | -- | -- | -- | -- |
| External Eating | 0.23* | 0.28* | 0.01 | 0.12 | 0.11 | 0.16† | 0.24* | 0.10 | 0.07 | 0.02 | 0.16* | 0.26* | <0.01 | 0.12 | 0.12 | -- | -- | -- | -- | -- |
| Fatigue | 0.35* | 0.17† | 0.14 | −0.02 | 0.15 | .18* | 0.16† | 0.01 | 0.06 | 0.05 | 0.20* | 0.21* | 0.08 | 0.04 | 0.04 | -- | -- | -- | -- | -- |
| Emotional Eating Scale | ||||||||||||||||||||
| Anger, Anx, & Frustration | 0.16† | 0.15† | 0.07 | 0.10 | 0.03 | 0.19* | 0.22* | 0.10 | 0.11 | 0.01 | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- |
| Depression | 0.24* | 0.21* | 0.09 | 0.10 | <0.01 | 0.18* | 0.27* | 0.08 | 0.12 | 0.04 | -- | -- | -- | -- | -- | 0.15* | 0.34* | 0.10 | 0.17* | 0.08 |
| Unsettled | 0.15† | 0.12 | 0.04 | 0.07 | 0.03 | -- | -- | -- | -- | -- | 0.19* | 0.17† | 0.13 | 0.10 | 0.04 | -- | -- | -- | -- | -- |
Note. β = fixed effects beta estimates from the mixed linear models that index how effectively exposure to weight conscious peer groups can predict the outcome (i.e., disordered eating) in each set of analysis; “Ind. MZ” = individual-level associations between weight conscious peer groups and disordered eating for MZ pairs; “Ind. DZ” = individual-level associations between weight conscious peer groups and disordered eating for DZ pairs. “Within-Pair MZ” = within-pair association (i.e., the ability of within-pair differences in peer exposure to weight conscious peer groups to predict each twin’s level of disordered eating) for MZ pairs; “Within-Pair DZ = within-pair associations for DZ pairs only; “Ex x Zyg” = test of whether there are significant differences in within-pair effects for MZ versus DZ twins.
p< .01,
p<.05
Notably, there were a few associations that showed Scenario B (genetic selection), or a mix of Scenario A and C (socialization and selection) (see Table 5). One association showed strong evidence in support of Scenario B - the association between the Emotional Eating Scale- Unsettled and Appearance Conversations with Friends (see double lined cell in Table 5). A significant DZ within-pair effect and no significant MZ within-pair effect was observed for this association, the within-pair DZ effect was significantly greater than the MZ effect, and the within-pair DZ effect was similar in magnitude to the DZ individual-level estimate. These findings suggest genetic selection effects only, as when genetic effects were completely controlled (i.e., within MZ twins), the association was not observed.
Table 5.
Results from Co-Twin Control Results that Resemble Scenario B (Genetic Selection) or Mixture of Scenarios A and C (Socialization and Selection).

|
Note. β = fixed effects beta estimates from the mixed linear models that index how effectively exposure to weight conscious peer groups can predict the outcome (i.e., disordered eating) in each set of analysis; “Ind. MZ” = individual-level associations between weight conscious peer groups and disordered eating for MZ pairs; “Ind. DZ” = individual-level associations between weight conscious peer groups and disordered eating for DZ pairs; “Within-Pair MZ” = within-pair association (i.e., the ability of within-pair differences in peer exposure to weight conscious peer groups to predict each twin’s level of disordered eating) for MZ pairs; “Within-Pair DZ” = within-pair associations for DZ pairs only; “Ex x Zyg” = test of whether there are significant differences in within-pair effects for MZ versus DZ twins. Cells that are outlined with a single line resemble a mix of Scenarios A and C, whereas cells that are outlined with a double line resemble Scenario B. Cells outlined in a dotted line were cases where the interpretation is slightly ambiguous, however, these cases were interpreted as Scenario B.
p< .01
By contrast, a few associations showed a mix of Scenarios A and C (see solid line cells in Table 5). In some of these cases (e.g., associations between Weight Preoccupation and Friends as a Source of Influence), the within-pair estimates were significant for both MZ and DZ twins, and these estimates were not significantly different from each other (e.g., the Ex x Zyg interaction was non-significant), suggesting Scenario A. However, the MZ and DZ within-pair associations were either significantly reduced in magnitude (p < .05) as compared to their corresponding individual-level effects, or they were substantially reduced (e.g., nearly half of the within-individual estimate – see MEBS Binge Eating with the Appearance Conversations with Friends scale). These reductions suggest that Scenario C is also present, since controlling for genetic and shared environmental selection factors attenuates associations between weight conscious peer groups and disordered eating (see Figure 2). Another example of associations that resembled both Scenarios A and C included situations where the MZ twin estimate was statistically significant, the DZ twin estimate was non-significant, and there were significant differences between the MZ and DZ estimates (see the MEBS Weight Preoccupation with Perceived Friend Preoccupation with Weight and Dieting). In these cases, the non-significant DZ pair estimate suggests the presence of selection (i.e., Scenario C), but the ability for exposure to predict results even when controlling for genetic and/or shared environmental influences with the MZ twins also suggests that socialization effects may be present (i.e., Scenario A).
Figure 2. Examples of Scenario C and a Mixture of Scenarios A and C.
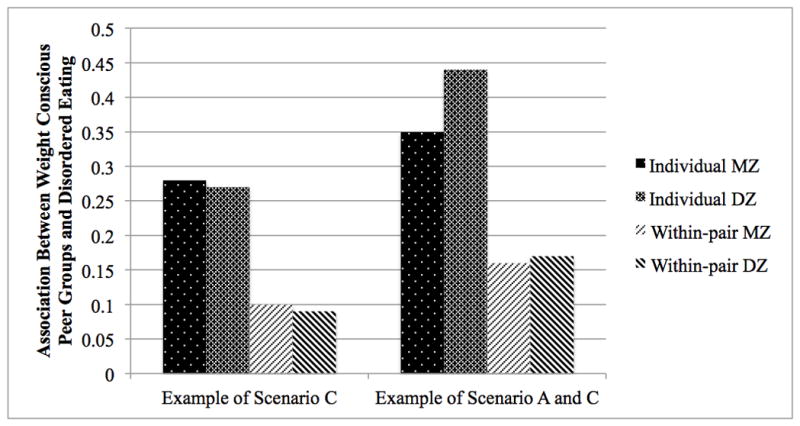
Associations between Friends as a Source of Influence and Eating in the Absence of Hunger-Negative Affect are displayed to demonstrate effects that resemble Scenario C (i.e., significant individual-level effects and non-significant DZ and MZ within-pair effects). Associations between Peer Attribution Scale and the Minnesota Eating Behavior Survey- Total Score are displayed to represent associations that resemble a mix of Scenario A and C (i.e., the within-pair associations are significant resembling Scenario A, but reduced compared to the individual-level effects resembling Scenario C).
Finally, there were a small number of associations in which the effects were more difficult to interpret (see dotted line cells in Table 5). In all of these cases, results were trending toward Scenario B, or genetic selection effects, in that the DZ within-pair estimate was statistically significant and it was not significantly reduced (p > .05) from the DZ within-individual estimate. Moreover, the MZ within-pair estimates were not statistically significant, and in some cases, even the MZ within-individual estimates were not significant. These results would clearly suggest Scenario B, except that the Ex x Zyg interaction was non-significant, leading to ambiguity around whether the MZ and DZ within-pair estimates were very different from each other. However, given the difficulty in detecting statistically significant interactions in regression and MLM models, and the bulk of evidence in support of Scenario B for these associations, we tentatively interpret these results to show Scenario B, genetic selection effects.
Discussion
Findings from this study are the first to suggest that associations between weight conscious peer groups and disordered eating may be due to genetic and/or shared environmental selection factors rather than pure socialization effects. Results showed that girls who exhibit more disordered eating (either due to genetic or shared environmental predispositions) appear to select into weight conscious peer groups rather than socialization within these peer groups leading to increased disordered eating. Support for these types of genetic and/or shared environmental selection effects persisted even when controlling for pubertal status. This pattern was consistently observed across multiple disordered eating constructs (i.e., body dissatisfaction, weight preoccupation, binge eating, eating in the absence of hunger, emotional eating) and multiple measures of peer group exposure. Overall, these findings question whether associations between weight conscious peer groups and disordered eating are due entirely to socialization processes.
Previously, researchers have suggested that socialization may be the mechanism at work in the association between weight conscious peer groups and disordered eating. Studies examining the convergence or divergence of disordered eating behaviors with exposure to peer groups have provided support for socialization, in that individuals who spend more time together become more similar in their level of disordered eating (Crandall, 1988; Zalta & Keel, 2006). However, these studies were unable to entirely control for selection effects, since neither study accounted for whether the individuals were friends prior to living together in the sorority (Crandall, 1988) or living together as roommates (Zalta & Keel, 2006). When peer groups were completely unselected, Myer and Waller (2001) observed a lack of convergence in bulimic behavior. Additional support for selection effects was found when Rayner et al. (2013) examined girls’ friendship groups across time and noted that girls tend to stay in friendship groups that are more similar to their own body dissatisfaction and bulimic behavior.
Results from our study corroborate these latter findings by supporting the presence of genetic and/or shared environmental selection effects. When genetic and shared environmental influences were controlled for using the co-twin control method, the association between exposure to weight conscious peer groups and disordered eating was either eliminated or significantly reduced. Aggregating findings across all studies then, it is possible that genetic and/or shared environmental selection effects may drive who one chooses to affiliate with initially (e.g., who decides to join a sorority), and then socialization may work to increase the similarity within a particular peer group (VanHuysse et al, submitted). This hypothesis would reconcile previous inconsistent findings and would help account for the small number of associations (~20%) in our study that showed both socialization and selection effects (i.e., Scenarios A and C).
Interestingly, another recent co-twin control study from the MSUTR examined associations between weight conscious peer groups and thin-ideal internalization in a sample that overlapped with the current one (i.e., 92% overlap; VanHuysse et al., submitted). This study found stronger support for socialization effects, although results also highlighted a complimentary role of selection (VanHuysse et al, submitted). Integration of the findings from VanHuysse et al. (submitted) and the current study seem to support the presence of both mechanisms. Specifically, genetic and/or environmental risk for disordered eating (and to a lesser extent thin-ideal internalization) may lead young girls to select into weight conscious peer groups. Within these peer groups, socialization effects may then work to increase thin-ideal internalization and, to a lesser extent, disordered eating symptoms (VanHuysse et al., submitted).
Moving forward, it will be important to identify the genetic and/or shared environmental influences contributing to selection into weight conscious peer groups. Although our co-twin control design advances prior research by providing evidence for selection effects, the design is unable to determine the degree to which genetic and/or shared environmental effects contribute to the selection processes. Future studies could use multivariate models (e.g., Cholesky decomposition models) to disentangle these genetic/shared environmental influences and advance our understanding of the underlying selection processes.
Ideally, these studies would also assess and examine the specific factors that may contribute to genetically and/or environmentally mediated selection into weight conscious peer groups. The current study controlled for pubertal development, suggesting that the selection effects observed in this study are independent of pubertal stage.3 These results were somewhat unexpected, as prior research has demonstrated increased genetic (and decreased shared environmental) risk for disordered eating with more advanced pubertal development (Culbert et al., 2009; Klump et al., 2000; Klump et al., 2007). Thus, we thought we might observe stronger genetic (and weaker shared environmental) selection effects in pubertal girls as opposed to pre-pubertal girls. The lack of differences suggests that there are stable genetic and/or shared environmental factors that drive selection into weight-conscious peer groups across development.
Two specific factors that might contribute to selection into weight focused peer groups are perfectionism and maternal disordered eating. Perfectionism is a personality trait that tends to develop early in life (prior to peer group selection), it is significantly heritable (.39 to .58; Jang, Livesley, Vernon, & Jackson, 1996; Tellegen et al., 1988), and it exhibits significant associations with a range of eating disorder symptoms (e.g., fasting, binge behaviors) and diagnoses (Forbush, Heatherton & Keel, 2007). As noted by Zalta and Keel (2006), it is possible that young girls who are raised in an environment with excessively high standards and/or who are genetically predisposed to perfectionistic qualities may select into peer groups with other girls who are self-critical and have high standards. These high standards could translate into an emphasis on society’s notion of the “ideal” body and an increased rate of disordered eating symptoms. Maternal disordered eating also could serve as a genetic and/or shared environmental selection factor, as girls who inherit genes of risk from their mother and/or observe maternal disordered eating could select into peer groups who also exhibit or emphasize these behaviors.
Despite the many strengths of this study (i.e., the ability to test for selection effects, the examination of multiple disordered eating measures, etc.), this study was not without limitations. First, the co-twin control study design is unable to control for every factor that may be important in selection into weight-focused peer groups (e.g., consumption of media that emphasizes the thin-ideal). Propensity score matching (Caliendo & Kopeinig, 2008) within a twin study design or other designs may be a promising approach for exploring additional matching variables. Moreover, the co-twin control design is unable to control for environmental factors that are different between twins, such as non-shared environmental factors that are specific to each co-twin (e.g., twins participating in different sports or after school activities). Since these unique experiences vary across the twin pair, it is impossible to match twins on these experiences and thus, they cannot be controlled for within the models. It is possible that these non-shared environmental factors are causing selection into peer groups with differing levels of focus on body weight and body shape (i.e., one co-twin plays soccer [a less weight-focused sport] while another takes ballet classes [a more weight-focused sport]).
Second, we used data from only one informant (e.g., twin’s self report). Associations between weight conscious peer groups and disordered could be inflated by shared method variance (e.g., similarities in response styles may lead to stronger associations between exposure and outcome variables; Podsakoff et al., 2003). Additional research is needed to explore associations using data from other informants (e.g., parental reports, peer reports) to ensure that results are unchanged. Further, the use of informant reports is also important given the possibility that individuals high in disordered eating might erroneously report a stronger emphasis on weight and shape in their peer groups than individuals lower in disordered eating.
Third, our participants were younger than those in most previous studies (Crandall, 1988 and Zalta & Keel, 2006; for an exception, see Rayner et al. (2013) who also identified selection effects in this age group). Although we would argue that adolescence is a critical time period when young girls are beginning to rely more on their peer groups (Steinberg, 1990), it remains unknown whether differences in results (between ours and previous studies’ results) are due to possible age differences in effects (e.g., selection effects being more important in adolescence; socialization being more important in young adulthood). Future studies should examine this possibility by examining effects across adolescent and young adult ages.
Fourth, since this study was conducted using a non-clinical sample, it is unknown if the findings from this study generalize to a clinical population. However, the disordered eating symptoms that were examined are precursors to full clinical eating disorders (Killen, et al., 1996; Stice & Shaw, 2002), which suggests it is likely that similar results might be found in a clinical sample. One challenge in conducting the present study using a clinical sample would be finding a sufficient number of twins with clinical eating disorders to conduct a well-powered twin analysis. Nonetheless, future research is needed to assess whether findings translate to individuals with clinical eating disorders.
Finally, our data are cross-sectional, and we therefore are limited in our ability to confirm causal associations. Indeed, while this study investigated whether peer group’s emphasis on weight and shape predicted disordered eating, it is possible that an individual’s disordered eating could lead to greater emphasis on body weight and shape within the peer group. Future longitudinal studies are needed to assess whether individuals at higher risk for disordered eating symptoms prospectively select into weight conscious peer groups. This design could then assess whether, after selecting into these peer groups, exposure leads to enhanced disordered eating symptoms across time (i.e., demonstrating socialization effects). This longitudinal design may also allow for identification of specific selection factors that may drive selection into weight conscious peer groups (e.g., perfectionism, maternal dieting, etc.).
General Scientific Summary.
This study suggests that selection effects may contribute to the association between weight conscious peer groups and increased levels of disordered eating, such that girls with a genetic and/or environmental predisposition for disordered eating may select into peer groups who are more body or weight focused.
Acknowledgments
This research was supported by grants from the National Institute of Mental Health (NIMH) (1 R01 MH082054) awarded to Dr. Klump.
Footnotes
Unfortunately, the co-twin control design is unable to control for non-shared environmental factors (e.g., twins participating in different sports or after-school activities). These factors are unique to each co-twin, making it is impossible to match twins on these experiences and thus, these factors cannot be controlled for within the co-twin control models.
The Minnesota Eating Behavior Survey (MEBS; previously known as the Minnesota Eating Disorder Inventory (M-EDI)) was adapted and reproduced by special permission of Psychological Assessment Resources, Inc., 16204 North Florida Avenue, Lutz, Florida 33549, from the Eating Disorder Inventory (collectively, EDI and EDI-2) by Garner, Olmstead, & Polivy (1983) Copyright 1983 by Psychological Assessment Resources, Inc. Further reproduction of the MEBS is prohibited without prior permission from Psychological Assessment Resources, Inc.
To ensure that results also did not vary by age or body weight, we ran analyses controlling for age (which correlates highly with pubertal development, r = .79) and body mass index (calculated from height and weight measurements). Results were identical to those described below, and thus, only analyses with pubertal development as a covariate are included herein.
In order to further ensure that results do not differ by pubertal status, we also examined pubertal status as a moderator (instead of covariate) in analyses. The sample was divided into pre-pubertal and pubertal groups (with a mean score of 2.5 on the PDS used as a cut-off). Co-twin control models were run separately in each group. The overall results were consistent between the pre-pubertal and pubertal groups, as they both continued to favor Scenario C, suggesting selection effects do not seems to vary by pubertal status.
Parts of this manuscript were presented at the 43rd Annual Meeting of Behavior Genetics Association, Marseille, France, June 28– July 2, 2013 and the 19th Annual Meeting of the Eating Disorders Research Society, Bethesda, Maryland, September 18–21, 2013.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIMH.
References
- Bulik CM, Sullivan PF, Kendler KS. Heritability of binge-eating and broadly defined bulimia nervosa. Biological Psychiatry. 1998;44(12):1210–1218. doi: 10.1016/s0006-3223(98)00280-7. [DOI] [PubMed] [Google Scholar]
- Burt SA, Donnellan MB, Humbad MN, Hicks BM, McGue M, Iacono WG. Does marriage inhibit antisocial behavior? An examination of selection vs causation via a longitudinal twin design. Archives of General Psychiatry. 2010;67(12):2010. doi: 10.1001/archgenpsychiatry.2010.159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burt SA, Klump KL. The Michigan State University Twin Registry (MSUTR): An update. Twin Research and Human Genetics. 2013;1(1):1–7. doi: 10.1017/thg.2012.87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caliendo M, Kopeinig S. Some practical guidance for the implementation of propensity score matching. Journal of Economic Surveys. 2008;22(1):31–72. [Google Scholar]
- Crandall CS. Social contagion of binge eating. Journal of Personality and Social Psychology. 1988;55(4):588–598. doi: 10.1037//0022-3514.55.4.588. [DOI] [PubMed] [Google Scholar]
- Culbert KM, Burt SA, McGue M, Iacono WG, Klump KL. Puberty and the genetic diathesis of disordered eating attitudes and behaviors. Journal of Abnormal Psychology. 2009;118(4):788–796. doi: 10.1037/a0017207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cumming G. Inference by eye: Reading the overlap of independent confidence intervals. Statistics in Medicine. 2009;28(2):205–220. doi: 10.1002/sim.3471. [DOI] [PubMed] [Google Scholar]
- Fairburn CG, Beglin SJ. Assessment of eating disorders: Interview or self-report questionnaire? International Journal of Eating Disorders. 1994;16:363–370. [PubMed] [Google Scholar]
- Forbush K, Heatherton TF, Keel PK. Relationships between perfectionism and specific disordered eating behaviors. International Journal of Eating Disorders. 2007;40:37–41. doi: 10.1002/eat.20310. [DOI] [PubMed] [Google Scholar]
- Garner DM. Eating disorder inventory-2: Professional manual. Odessa, FL: Psychological Assessment Resources; 1991. [Google Scholar]
- Garner DM, Olmsted MP, Polivy J. Development and validation of a multidimensional eating disorder inventory for anorexia nervosa and bulimia. International Journal of Eating Disorders. 1983;2(2):15–34. [Google Scholar]
- Gilbert N, Meyer C. Similarity in young women’s eating attitudes: Self-selected versus artificially constructed groups. International Journal of Eating Disorders. 2004;36:213–219. doi: 10.1002/eat.20036. [DOI] [PubMed] [Google Scholar]
- Goldschmidt AB, Wall MM, Choo TJ, Bruening M, Eisenberg ME, Neumark-Sztainer D. Examining associations between adolescent binge eating and binge eating in parents and friends. International Journal of Eating Disorders. 2014;47(3):325–328. doi: 10.1002/eat.22192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haines J, Neumark-Sztainer D, Eisenberg ME, Hannan PJ. Weight teasing and disordered eating behaviors in adolescents: Longitudinal findings from project eat (eating among teens) Pediatrics. 2006;117(2):e209–e215. doi: 10.1542/peds.2005-1242. [DOI] [PubMed] [Google Scholar]
- Iacono WG, McGue M. Minnesota twin family study. Twin Research. 2002;5(5):482–487. doi: 10.1375/136905202320906327. [DOI] [PubMed] [Google Scholar]
- Jang KL, Livesley WJ, Vernon PA, Jackson DN. Heritability of personality disorder traits: A twin study. Acta Psychiatrica Scandinavica. 1996;94(6):438–444. doi: 10.1111/j.1600-0447.1996.tb09887.x. [DOI] [PubMed] [Google Scholar]
- Jones DC, Vigfusdottir TH, Lee Y. Body image and the appearance culture among adolescent girls and boys: An examination of friend conversations, peer criticism, appearance magazines, and the internalization of appearance ideals. Journal of Adolescent Research. 2004;19(3):323–339. [Google Scholar]
- Kaye WH, Klump KL, Frank GKW, Strober M. Annual Review of Medicine: Selected Topics in the Clinical Sciences. Vol. 51. Palo Alto, CA: Annual Reviews; 2000. Anorexia and bulimia nervosa. [DOI] [PubMed] [Google Scholar]
- Keel PK, Forney KJ, Brown TA, Heatherton TF. Influence of college peers on disordered eating in women and men at 10- year follow-up. Journal of Abnormal Psychology. 2013;122(1):105–110. doi: 10.1037/a0030081. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Killen JD, Taylor CB, Hayward C, Haydel KF, Wilson DM, Hammer L, Kraemer H, Blair-Greiner A, Strachowski D. Weight concerns influence the development of eating disorders: A 4-year prospective study. Journal of Consulting and Clinical Psychology. 1996;64(5):936–940. doi: 10.1037//0022-006x.64.5.936. [DOI] [PubMed] [Google Scholar]
- Klump KL, Burt SA. The Michigan State University Twin Registry (MSUTR): Genetic, environmental and neurobiological influences on behavior across development. Twin Research and Human Genetics. 2006;9(6):971–977. doi: 10.1375/183242706779462868. [DOI] [PubMed] [Google Scholar]
- Klump KL, Burt SA, McGue M, Iacono WG. Changes in genetic and environmental influences on disordered eating across adolescence: A longitudinal twin study. Archives in General Psychiatry. 2007;64(12):1409–1415. doi: 10.1001/archpsyc.64.12.1409. [DOI] [PubMed] [Google Scholar]
- Klump KL, Burt SA, Spanos A, McGue M, Iacono WG, Wade TM. Age differences in genetic and environmental influences on weight and shape concerns. International Journal of Eating Disorders. 2010;43:679–688. doi: 10.1002/eat.20772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klump KL, Keel PK, Burt SA, Racine SE, Neale MC, Sisk CL, Boker S. Ovarian hormones and emotional eating associations across the menstrual cycle: An examination of the potential moderating effects of body mass index and dietary restraint. International Journal of Eating Disorders. 2013 doi: 10.1002/eat.22084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klump KL, McGue M, Iacono WG. Age differences in genetic and environmental influences on eating attitudes and behaviors in preadolescent and adolescent female twins. Journal of Abnormal Psychology. 2000;109(2):239–251. [PubMed] [Google Scholar]
- Klump KL, McGue M, Iacono WG. Differential heritability of eating attitudes and behaviors in prepubertal versus pubertal twins. International Journal of Eating Disorders. 2003;33(3):287–292. doi: 10.1002/eat.10151. [DOI] [PubMed] [Google Scholar]
- Klump KL, Miller KB, Keel PK, McGue M, Iacono WG. Genetic and environmental influences on anorexia nervosa syndromes in a population based twin sample. Psychological Medicine. 2001;31:737–740. doi: 10.1017/s0033291701003725. [DOI] [PubMed] [Google Scholar]
- Kolko DJ, Kazdin AE. Emotional/behavioral problems in clinic and nonclinic children: Correspondence among child, parent and teacher reports. Journal of Child Psychology and Psychiatry. 1993;34(4):991–1006. doi: 10.1111/j.1469-7610.1993.tb01103.x. [DOI] [PubMed] [Google Scholar]
- Levine MP, Smolak L. Toward a model of the developmental psychopathology of eating disorders: The example of early adolescence. In: Crowther JH, Hobfoll SE, Tennenbaum DL, Stephens MAP, editors. The etiology of bulimia nervosa: The individual and family context. Washington, D.C: Hemisphere; 1992. pp. 59–80. [Google Scholar]
- Levine MP, Smolak L, Hayden H. The relation of sociocultural factors to eating attitudes and behaviors among middle school girls. Journal of Early Adolescence. 1994;14(4):471–490. [Google Scholar]
- Lieberman M, Gauvin L, Bukowski WM, White DR. Interpersonal influence and disordered eating behaviors in adolescent girls: The role of peer modeling, social reinforcement and body-related teasing. Eating Behaviors. 2001;2:215–236. doi: 10.1016/s1471-0153(01)00030-7. [DOI] [PubMed] [Google Scholar]
- Lykken DT, Bouchard TJ, Jr, McGue M, Tellegen A. The Minnesota Twin Family Registry: Some initial findings. Acta Geneticae Medicae et Gemellologiae. 1990;39(1):35–70. doi: 10.1017/s0001566000005572. [DOI] [PubMed] [Google Scholar]
- McGue M, Osler M, Christensen K. Causal inference and observational research: The utility of twins. Perspectives on Psychological Science. 2010;5(5):546–556. doi: 10.1177/1745691610383511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Myer C, Waller G. Social convergence of disturbed eating attitudes in young adult women. Journal of Nervous and Mental Disorders. 2001;189(2):114–119. doi: 10.1097/00005053-200102000-00007. [DOI] [PubMed] [Google Scholar]
- Paxton SJ, Schutz HK, Wertheim EH, Muir SL. Friendship clique and peer influences on body image concerns, dietary restraint, extreme weight-loss behaviors, and binge eating in adolescent girls. Journal of Abnormal Psychology. 1999;108(2):255–266. doi: 10.1037//0021-843x.108.2.255. [DOI] [PubMed] [Google Scholar]
- Peeters H, Van Gestel S, Vlietinck R, Derom C, Derom R. Validation of a telephone zygosity questionnaire in twins of known zygosity. Behavior Genetics. 1998;28(3):159–163. doi: 10.1023/a:1021416112215. [DOI] [PubMed] [Google Scholar]
- Petersen AC, Crockett L, Richards M, Boxer A. A self-report measure of pubertal status: Reliability, validity, and initial norms. Journal of Youth Adolescence. 1988;17(2):117–133. doi: 10.1007/BF01537962. [DOI] [PubMed] [Google Scholar]
- Podsakoff PM, MacKenzie SB, Lee J, Podsakoff N. Common method biases in behavioral research: A critical review of the literature and recommended remedies. Journal of Applied Psychology. 2003;88(5):879–903. doi: 10.1037/0021-9010.88.5.879. [DOI] [PubMed] [Google Scholar]
- Rayner KE, Schniering CA, Rapee RM, Taylor A, Hutchinson DM. Adolescent girls’ friendship networks, body dissatisfaction, and disordered eating: Examining selection and socialization processes. Journal of Abnormal Psychology. 2013;122(1):93–104. doi: 10.1037/a0029304. [DOI] [PubMed] [Google Scholar]
- Rushton JP, Bons TA. Mate choice and friendship in twins: Evidence for genetic similarity. Psychological Science. 2005;16(7):555–559. doi: 10.1111/j.0956-7976.2005.01574.x. [DOI] [PubMed] [Google Scholar]
- Schutz HK, Paxton SJ, Wertheim EH. Investigation of body comparison among adolescent girls. Journal of Applied Social Psychology. 2002;32(9):1906–1937. [Google Scholar]
- Shroff H, Thompson JK. Peer influences, body-image dissatisfaction, eating dysfunction and self-esteem in adolescent girls. Journal of Health Psychology. 2006;11(4):533–551. doi: 10.1177/1359105306065015. [DOI] [PubMed] [Google Scholar]
- Smolak L, Levine M, Schermer F. Parental input and weight concerns among elementary school children. International Journal of Eating Disorders. 1999;25:339–343. doi: 10.1002/(sici)1098-108x(199904)25:3<263::aid-eat3>3.0.co;2-v. [DOI] [PubMed] [Google Scholar]
- Steinberg L. Autonomy, conflict, and harmony in the family relationship. In: Feldman S, Elliot G, editors. At the threshold: The developing adolescent. Cambridge, MA: Harvard University Press; 1990. pp. 255–276. [Google Scholar]
- Steinberg L, Monahan KC. Age differences in resistance to peer influence. Developmental Psychology. 2007;43(6):1531–1543. doi: 10.1037/0012-1649.43.6.1531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stice E, Shaw HE. Role of body dissatisfaction in the onset and maintenance of eating pathology: A synthesis of research findings. Journal of Psychosomatic Research. 2002;53(5):985–993. doi: 10.1016/s0022-3999(02)00488-9. [DOI] [PubMed] [Google Scholar]
- Tanofsky-Kraff M, Ranzenhofer LM, Yanovski SZ, Schvey NA, Faith M, Gustafson J, Yanovski JA. Psychometric properties of a new questionnaire to assess eating in the absence of hunger in children and adolescents. Appetite. 2008;51:148–155. doi: 10.1016/j.appet.2008.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tanofsky-Kraff M, Theim KR, Yanovski SZ, Bassett AM, Burns NP, Ranzenhofer LM, Glasofer DR, Yanovski JA. Validation of the Emotional Eating Scale adapted for use in children and adolescents (EES-C) International Journal of Eating Disorders. 2007;40(3):232–240. doi: 10.1002/eat.20362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taylor CB, Sharpe T, Shisslak C, Bryson S, Estes LS, Gray N, McKnight KM, Crago M, Kraemer HC, Killen JD. Factors associated with weight concerns in adolescent girls. International Journal of Eating Disorders. 1998;24:31–42. doi: 10.1002/(sici)1098-108x(199807)24:1<31::aid-eat3>3.0.co;2-1. [DOI] [PubMed] [Google Scholar]
- Tellegen A, Lykken DT, Bouchard TJ, Jr, Wilcox KJ, Segal NL, Rich S. Personality similarity in twins reared apart and together. Journal of Personality and Social Psychology. 1988;54(6):1031–1039. doi: 10.1037//0022-3514.54.6.1031. [DOI] [PubMed] [Google Scholar]
- Vander Wal JS, Thelen MH. Predictors of body image dissatisfaction in elementary-age school girls. Eating Behaviors. 2000;1:105–122. doi: 10.1016/s1471-0153(00)00011-8. [DOI] [PubMed] [Google Scholar]
- Van Huysse JL, Burt SA, O’Connor SM, Thompson JK, Klump KL. Socialization and selection effects in the association between weight conscious peer groups and thin-ideal internalization: A co-twin control study. doi: 10.1016/j.bodyim.2016.01.005. submitted. Submitted. [DOI] [PMC free article] [PubMed] [Google Scholar]
- von Ranson KM, Klump KL, Iacono WG, McGue M. The Minnesota Eating Behavior Survey: A brief measure of disordered eating attitudes and behaviors. Eating Behaviors. 2005;6:373–392. doi: 10.1016/j.eatbeh.2004.12.002. [DOI] [PubMed] [Google Scholar]
- Wertheim EH, Paxton SJ, Schutz HK, Muir SL. Why do adolescent girls watch their weight? An interview study examining sociocultural pressures to be thin. Journal of Psychosomatic Research. 1997;42(4):345–355. doi: 10.1016/s0022-3999(96)00368-6. [DOI] [PubMed] [Google Scholar]
- Zalta AK, Keel PK. Peer influence on bulimic symptoms in college students. Journal of Abnormal Psychology. 2006;115(1):185–189. doi: 10.1037/0021-843X.115.1.185. [DOI] [PubMed] [Google Scholar]