

Abstract
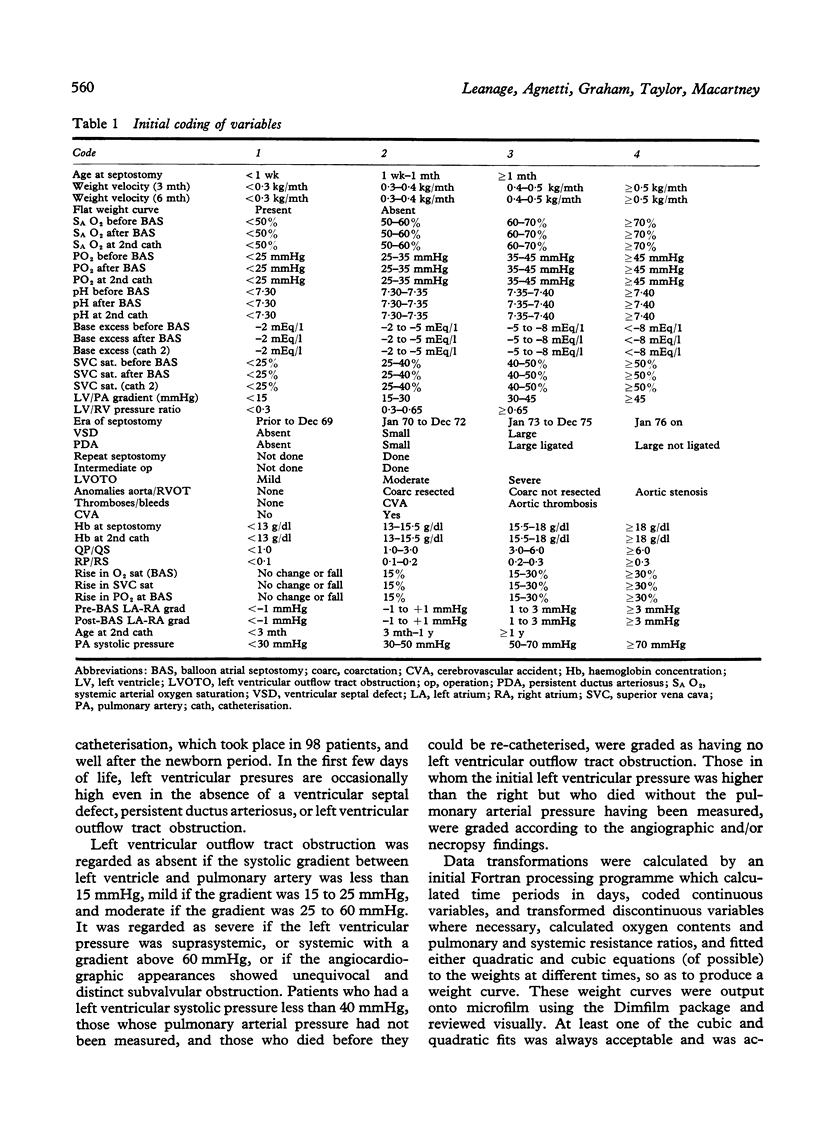
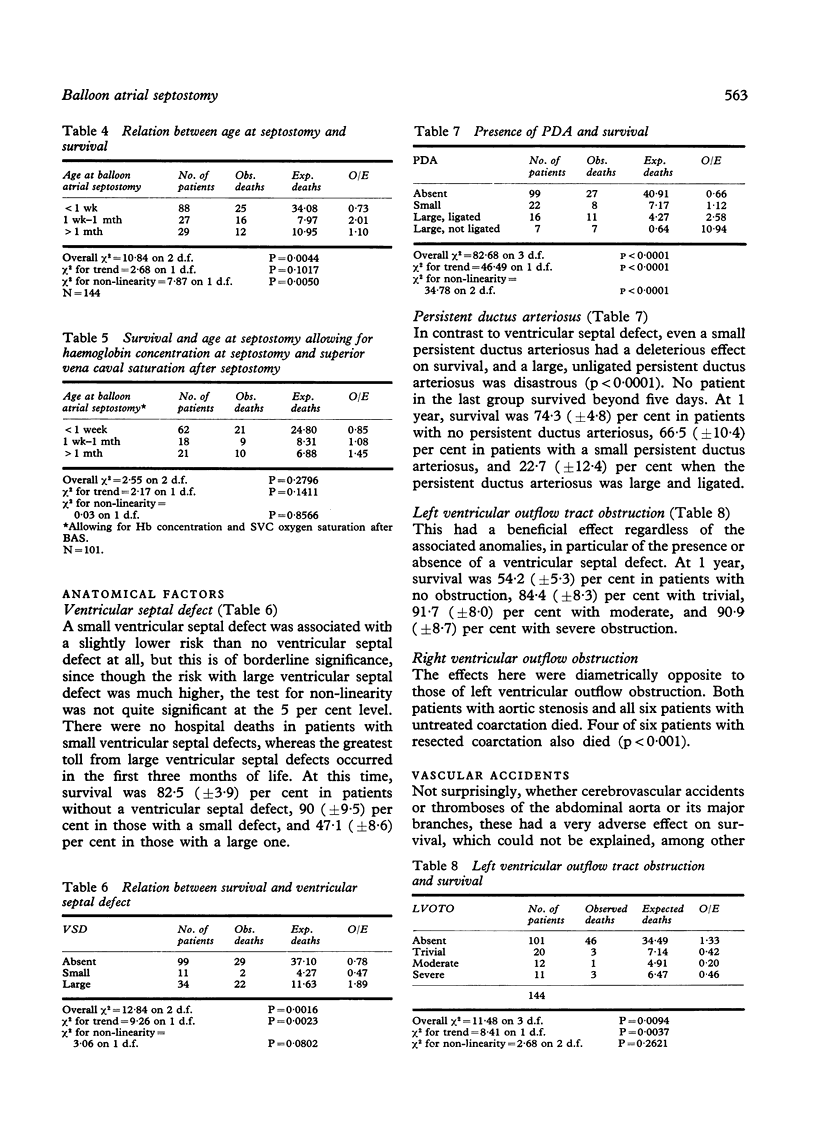
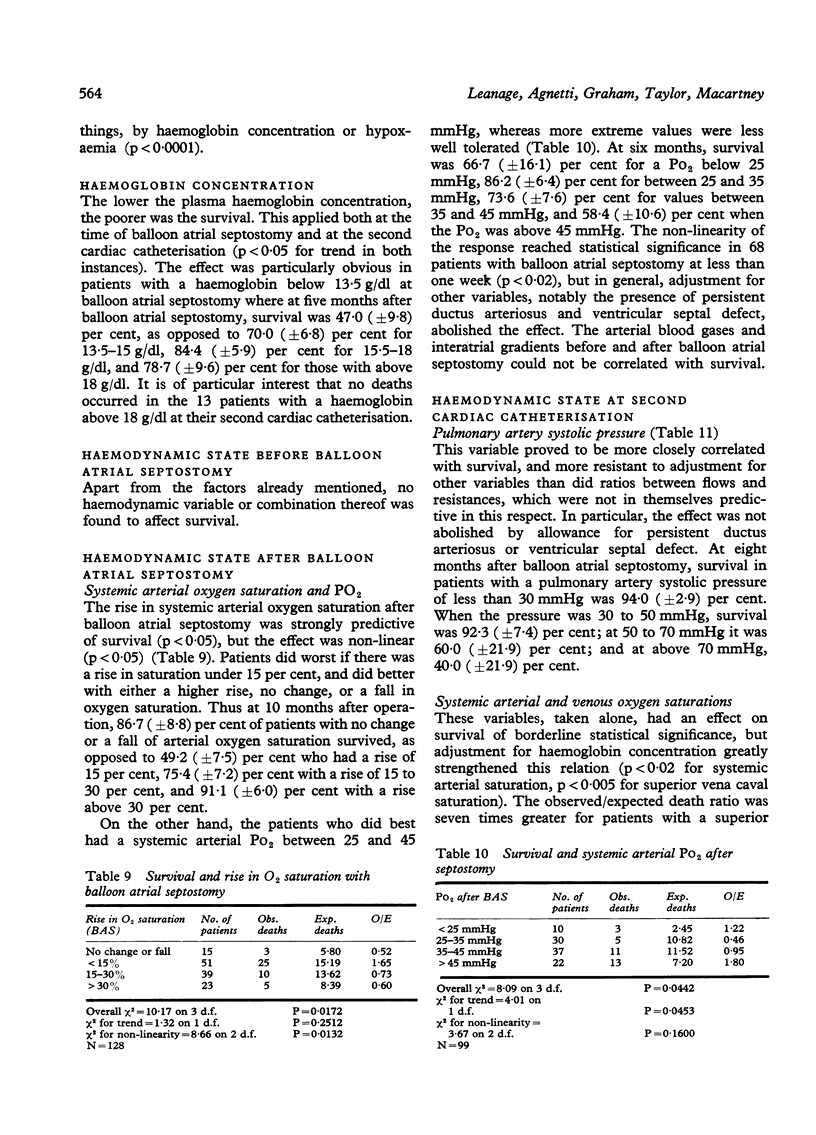
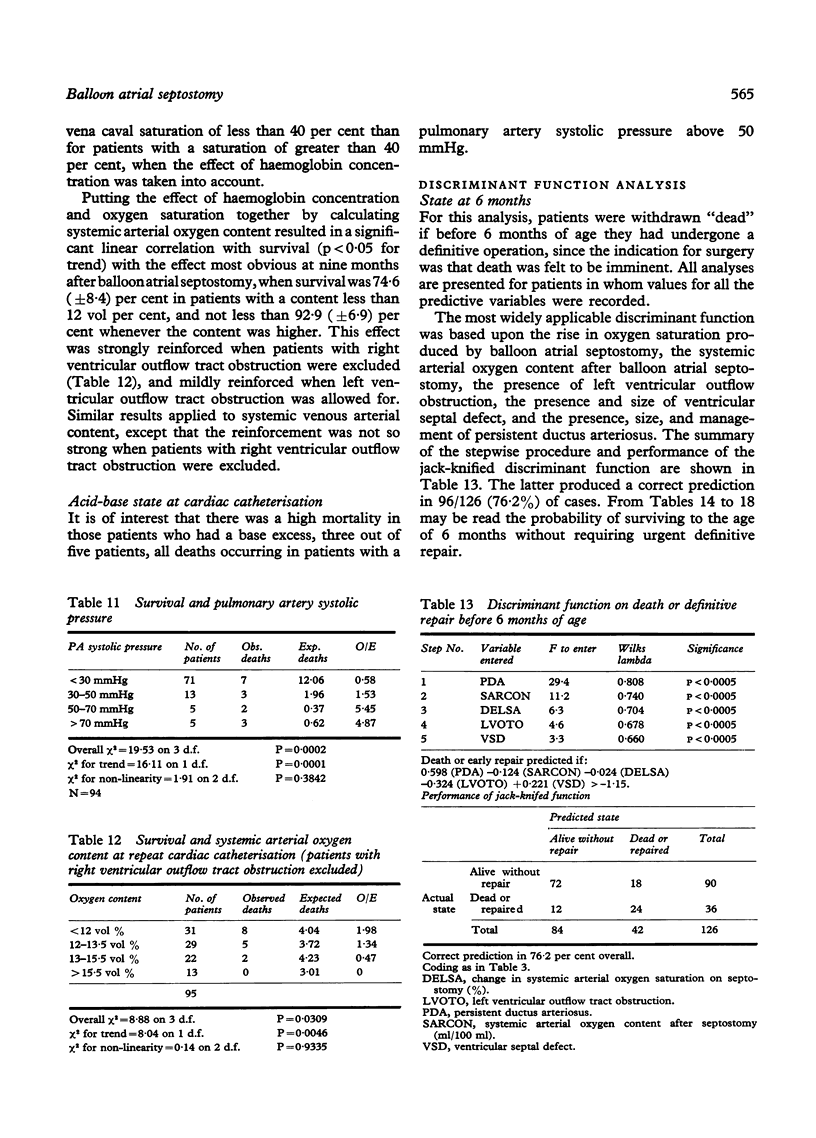
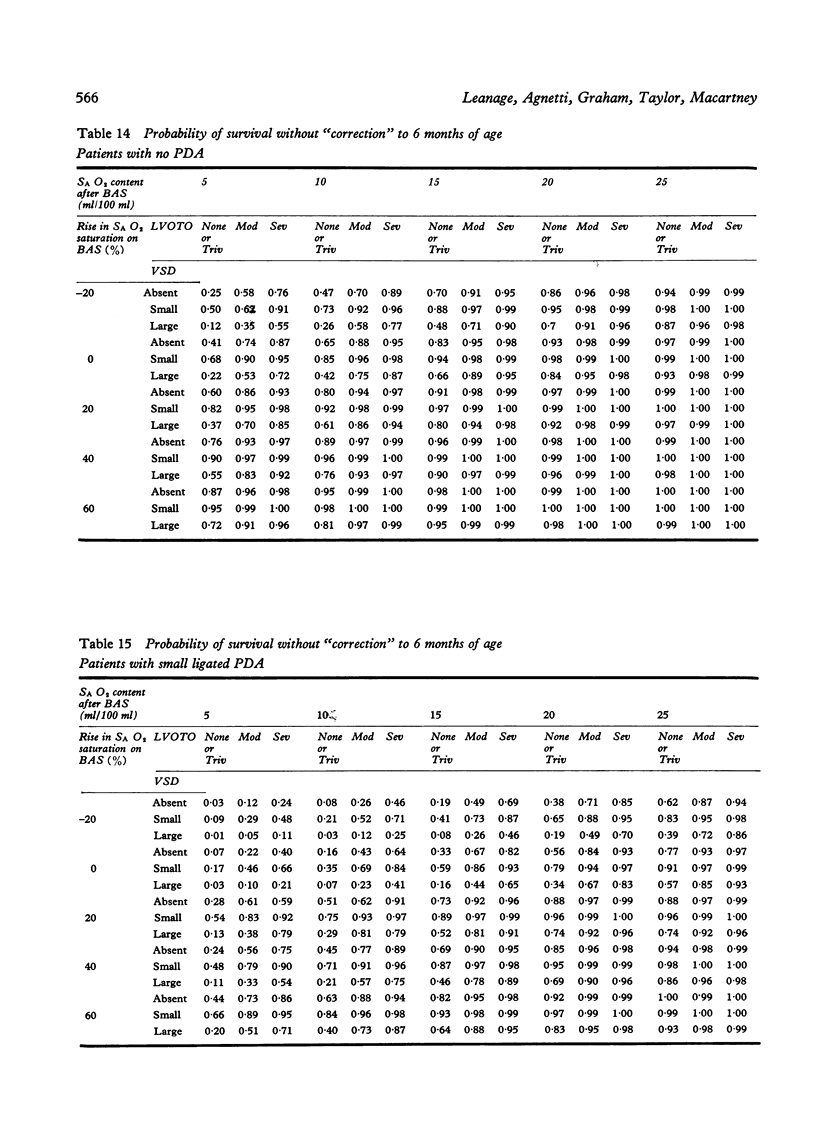
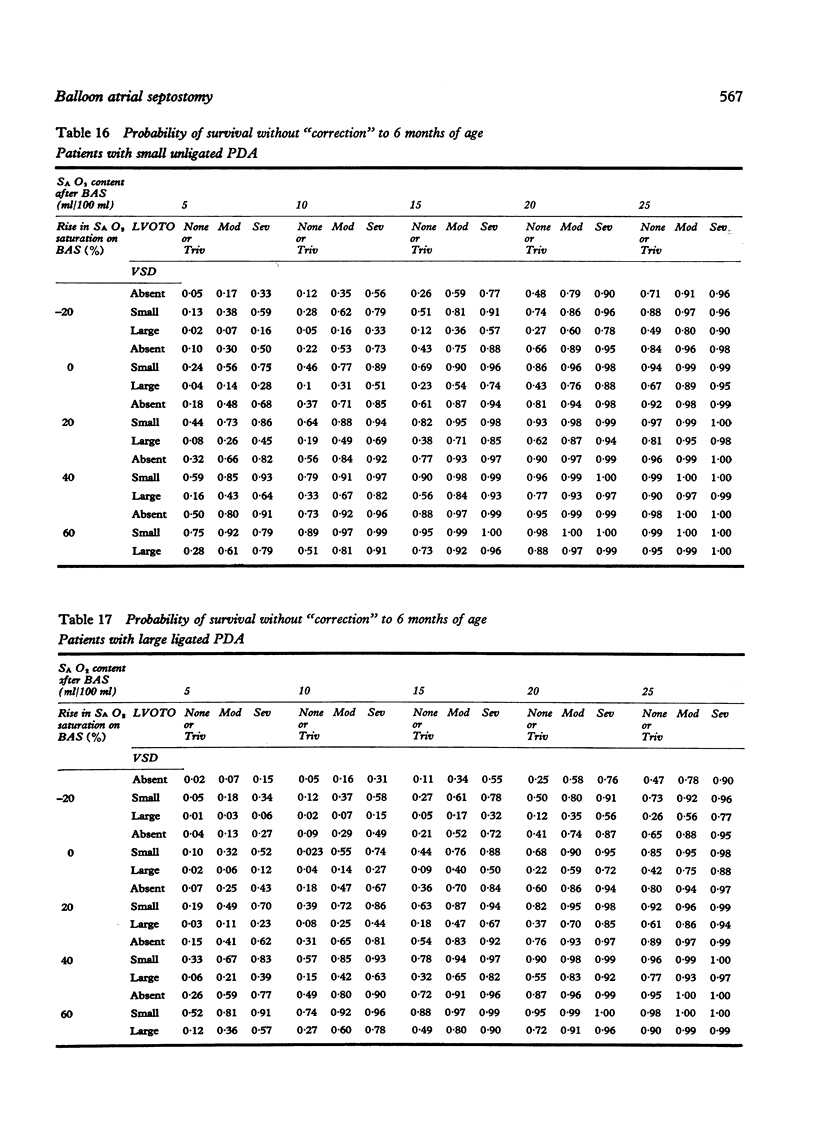
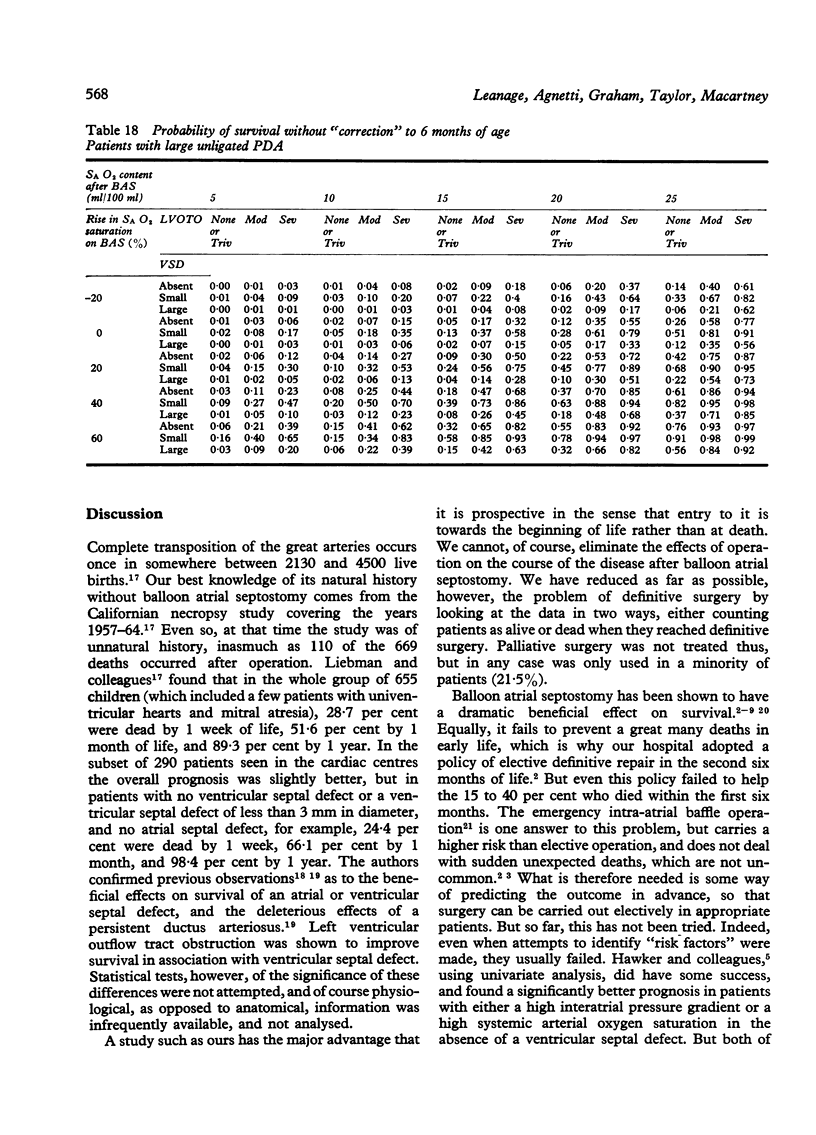
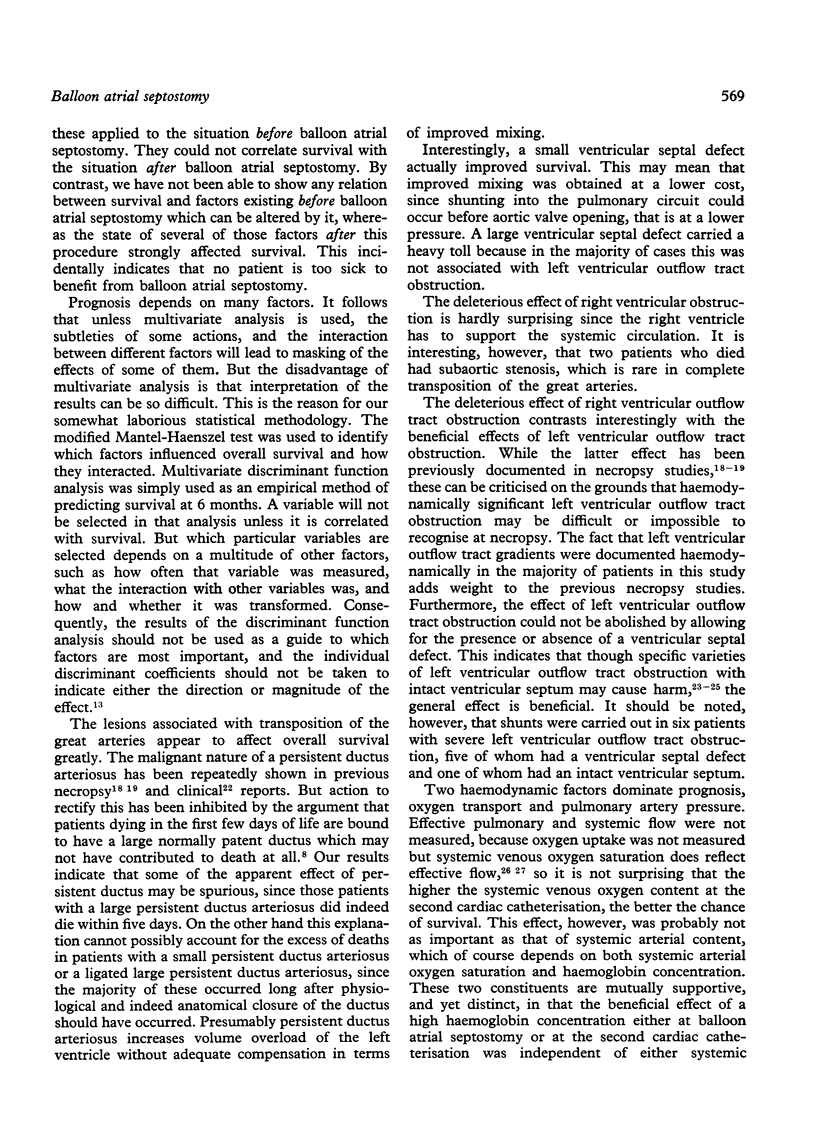
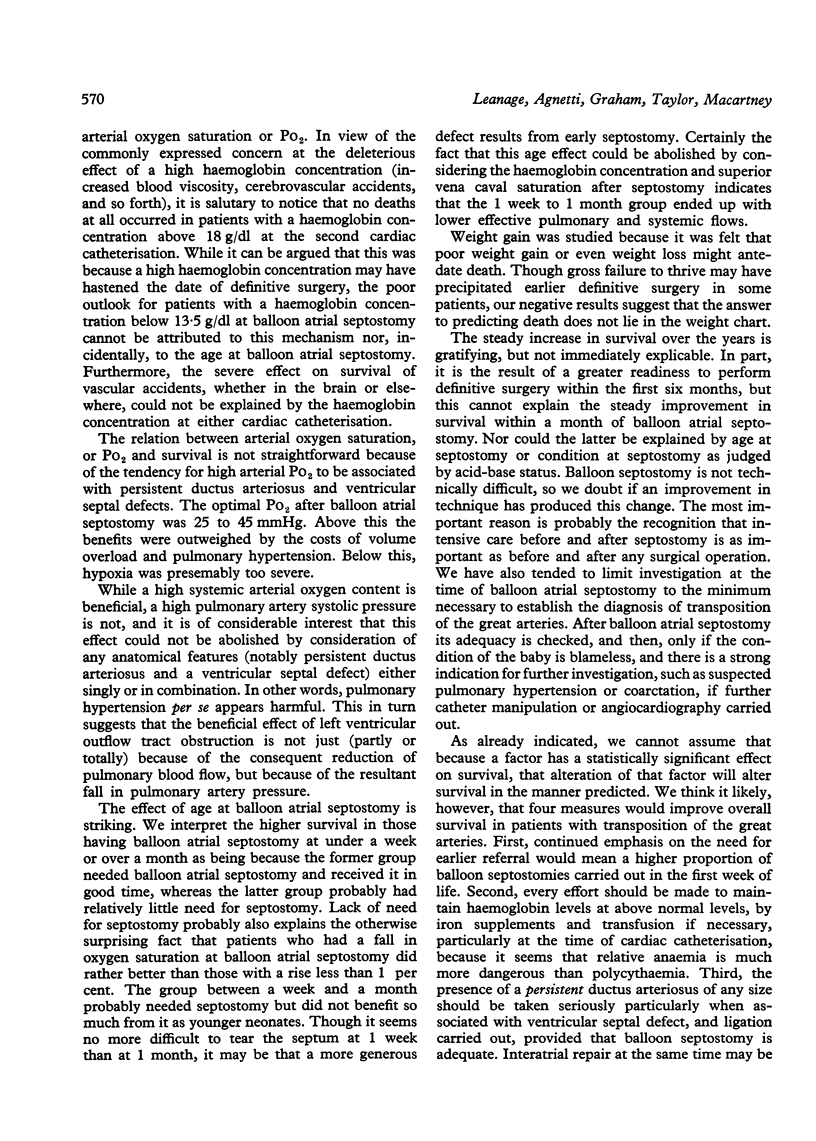
Despite balloon atrial septostomy within the first days of life, some patients with complete transposition of the great arteries die before reaching elective definitive surgery in the second six months of life. To discover why, we analysed the fate of 144 patients who had balloon atrial septostomy after 1966, using a modified logrank survival test with multivariate capability. Patients were withdrawn "alive" on reaching definitive surgery. The following largely independent factors were associated with a statistically significant excess mortality: pulmonary hypertension, the presence and size of a ventricular septal defect of persistent ductus arteriosus, relative anaemia, absence of left ventricular outflow tract obstruction, low arterial oxygen saturation, aortic stenosis and coarctation, and balloon atrial septostomy between 1 week and 1 month of life. Those of the above factors which can be determined at balloon atrial septostomy or at routine cardiac catheterisation at 3 months of age were then introduced into discriminant function analysis on survival to 6 months. Hence the probability of any individual patient dying in the first six months was calculated, allowing for these factors. This prediction was correct in 76 per cent of the patients studied. By offering earlier definitive correction to patients thus identified as being at high risk of premature death, it should prove possible to reduce overall mortality in transposition of the great arteries.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bierman F. Z., Williams R. G. Subxiphoid two-dimensional imaging of the interatrial septum in infants and neonates with congenital heart disease. Circulation. 1979 Jul;60(1):80–90. doi: 10.1161/01.cir.60.1.80. [DOI] [PubMed] [Google Scholar]
- Clarkson P. M., Barratt-Boyes B. G., Neutze J. M., Lowe J. B. Results over a ten-year period of palliation followed by corrective surgery for complete transposition of the great arteries. Circulation. 1972 Jun;45(6):1251–1258. doi: 10.1161/01.cir.45.6.1251. [DOI] [PubMed] [Google Scholar]
- Gutgesell H. P., Garson A., McNamara D. G. Prognosis for the newborn with transposition of the great arteries. Am J Cardiol. 1979 Jul;44(1):96–100. doi: 10.1016/0002-9149(79)90256-x. [DOI] [PubMed] [Google Scholar]
- Gutgesell H. P., McNamara D. G. Transposition of the great arteries. Results of treatment with early palliation and late intracardiac repair. Circulation. 1975 Jan;51(1):32–38. doi: 10.1161/01.cir.51.1.32. [DOI] [PubMed] [Google Scholar]
- Hawker R. E., Krovetz L. J., Rowe R. D. An analysis of prognostic factors in the outcome of balloon atrial septostomy for transposition of the great arteries. Johns Hopkins Med J. 1974 Feb;134(2):95–106. [PubMed] [Google Scholar]
- Liebman J., Cullum L., Belloc N. B. Natural history of transpositon of the great arteries. Anatomy and birth and death characteristics. Circulation. 1969 Aug;40(2):237–262. doi: 10.1161/01.cir.40.2.237. [DOI] [PubMed] [Google Scholar]
- MANTEL N., HAENSZEL W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst. 1959 Apr;22(4):719–748. [PubMed] [Google Scholar]
- Mair D. D., Ritter D. G. The physiology of cyanotic congenital heart disease. Int Rev Physiol. 1976;9:275–303. [PubMed] [Google Scholar]
- Parsons C. G., Astley R., Burrows F. G., Singh S. P. Transposition of great arteries. A study of 65 infants followed for 1 to 4 years after balloon septostomy. Br Heart J. 1971 Sep;33(5):725–731. doi: 10.1136/hrt.33.5.725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peto R., Pike M. C., Armitage P., Breslow N. E., Cox D. R., Howard S. V., Mantel N., McPherson K., Peto J., Smith P. G. Design and analysis of randomized clinical trials requiring prolonged observation of each patient. II. analysis and examples. Br J Cancer. 1977 Jan;35(1):1–39. doi: 10.1038/bjc.1977.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rashkind W. J., Miller W. W. Creation of an atrial septal defect without thoracotomy. A palliative approach to complete transposition of the great arteries. JAMA. 1966 Jun 13;196(11):991–992. [PubMed] [Google Scholar]
- Sansa M., Tonkin I. L., Bargeron L. M., Jr, Elliott L. P. Left ventricular outflow tract obstruction in transposition of the great arteries: an angiographic study of 74 cases. Am J Cardiol. 1979 Jul;44(1):88–95. doi: 10.1016/0002-9149(79)90255-8. [DOI] [PubMed] [Google Scholar]
- Stark F., de Leval M., Waterston D. J., Carter R. E. Proceedings: Current surgical management of transpositon of great arteries in infancy. Br Heart J. 1975 May;37(5):553–553. [PubMed] [Google Scholar]
- Tynan M. J., Becker A. E., Macartney F. J., Jiménez M. Q., Shinebourne E. A., Anderson R. H. Nomenclature and classification of congenital heart disease. Br Heart J. 1979 May;41(5):544–553. doi: 10.1136/hrt.41.5.544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tynan M. Haemodynamic effects of balloon atrial septostomy in infants with transposition of the great arteries. Br Heart J. 1972 Aug;34(8):791–794. doi: 10.1136/hrt.34.8.791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tynan M. Survical of infants with transposition of great arteries after balloon atrial septostomy. Lancet. 1971 Mar 27;1(7700):621–623. doi: 10.1016/s0140-6736(71)91553-4. [DOI] [PubMed] [Google Scholar]