

Abstract
Recent publications on both the genetics and environmental factors of restless legs syndrome (RLS) defined as a clinical disorder suggest that overlapping genetic risk factors may play a role in primary (idiopathic) and secondary (symptomatic) RLS. Following a systematic literature search of RLS associated with comorbidities, we identified an increased prevalence of RLS only in iron deficiency and kidney disease. In cardiovascular disease, arterial hypertension, diabetes, migraine, and Parkinson disease, the methodology of studies was poor, but an association might be possible. There is insufficient evidence for conditions such as anemia (without iron deficiency), chronic obstructive pulmonary disease, multiple sclerosis, headache, stroke, narcolepsy, and ataxias. Based on possible gene–microenvironmental interaction, the classifications primary and secondary RLS may suggest an inappropriate causal relation. We recognize that in some conditions, treatment of the underlying disease should be achieved as far as possible to reduce or eliminate RLS symptoms. RLS might be seen as a continuous spectrum with a major genetic contribution at one end and a major environmental or comorbid disease contribution at the other.
The first restless legs syndrome (RLS) diagnostic criteria were established in 1995 and revised in 2003.1 In 2014,2 a fifth criterion was added to improve specificity by excluding mimics. All versions of the criteria have maintained the key features of the clinical picture: sensory symptoms—namely restlessness (urge to move) and unpleasant sensations (paresthesias, pain)—and motor symptoms (periodic limb movements and other motor manifestations). Two major distinctive features emerged to enhance the specificity of the diagnosis of RLS: first, in primary/idiopathic RLS, a high familiarity finally led to the identification of genetic risk factors.3–6 Second, an increasing number of heterogeneous publications investigated the associations of RLS with various diseases, including iron deficiency anemia (IDA),7 multiple sclerosis (MS),8,9 polyneuropathy,10 and Parkinson disease (PD),11,12 as well as common chronic diseases such as arterial hypertension13 or headache14 or conditions such as inflammation15 and pregnancy.16 Over time, a differentiation into “primary, idiopathic” and “secondary, symptomatic” RLS occurred. Although available evidence now encompasses a broad spectrum of pathophysiologic, population-based (cross-sectional or longitudinal) studies, clinical studies, and treatment trials,14,17 the question whether RLS is more a primary disorder or a comorbidity remains unresolved. It is remarkable, however, that in the new DSM-5 criteria, this terminology was changed and the RLS definition criteria no longer differentiate between primary and secondary RLS.18 It is even likely that a cumulative number of diseases within a single patient increases the risk of the additional manifestation of RLS symptoms on the background of the genetic risk load, or vice versa.19
Genetic studies from recent years have shed some light on the molecular mechanism of the disorder. RLS is a genetically complex disorder in which genetic and environmental factors contribute to the phenotype. By means of genome-wide association studies (GWAS), common genetic variants with modest effect (odds ratio [OR] 1.2–1.7) on the phenotype have been identified in a total of 6 genomic regions.5,6 All of these loci combined explain <10% of the total heritability, indicating that an increase in GWAS' sample size will likely uncover a further proportion of the missing heritability. MEIS1 has been the RLS gene with the largest risk factors, harboring both common and rare coding variants with larger effects.20,21 MEIS1 belongs to the TALE family of homeobox transcription factors and is involved in the development and homeostasis of numerous organs and diseases such as leukemia and neuroblastoma, and also plays a role in the development of the CNS.22 Coding variants in MEIS1 are very rare in general. MEIS1 p.R272H has been identified as the most deleterious variant and is located within the first functional amino acid of the homeobox domain, which could raise the possibility of disruption of DNA binding, and isoform-dependent splice variants might contribute to RLS.20,23 The common genetic RLS-associated variant is located in highly conserved genomic regions in intron 8 of MEIS1 and has a regulatory function on the MEIS1 expression in the embryonic ganglionic eminences. This is a transient structure, giving rise to the basal ganglia at later stages. The RLS risk variant is associated with a relatively reduced expression of MEIS1 in these areas, highlighting the fact that RLS has components of a neurodevelopmental disorder. Low MEIS1 expression has also been demonstrated in postmortem tissue in the pons and thalamus.24 This all suggests a loss of function mechanism of MEIS1 in RLS. Finally, the genetic architecture of RLS is heterogeneous with the contribution of rare and common variants as well as coding and noncoding variants with small or large effects on the phenotype acting in concert within an oligogenic mode of inheritance.
In this review, we examine the available studies of RLS and comorbidities, focusing in particular on neurologic and medical disorders and their association with RLS, while keeping in mind the complex genetic architecture of RLS. We did not include any studies based on periodic limb movements in sleep (PLMS) or sleep studies if the clinical diagnosis of RLS was not the primary objective, as PLMS are associated with many comorbidities and reflect a different spectrum of diseases.
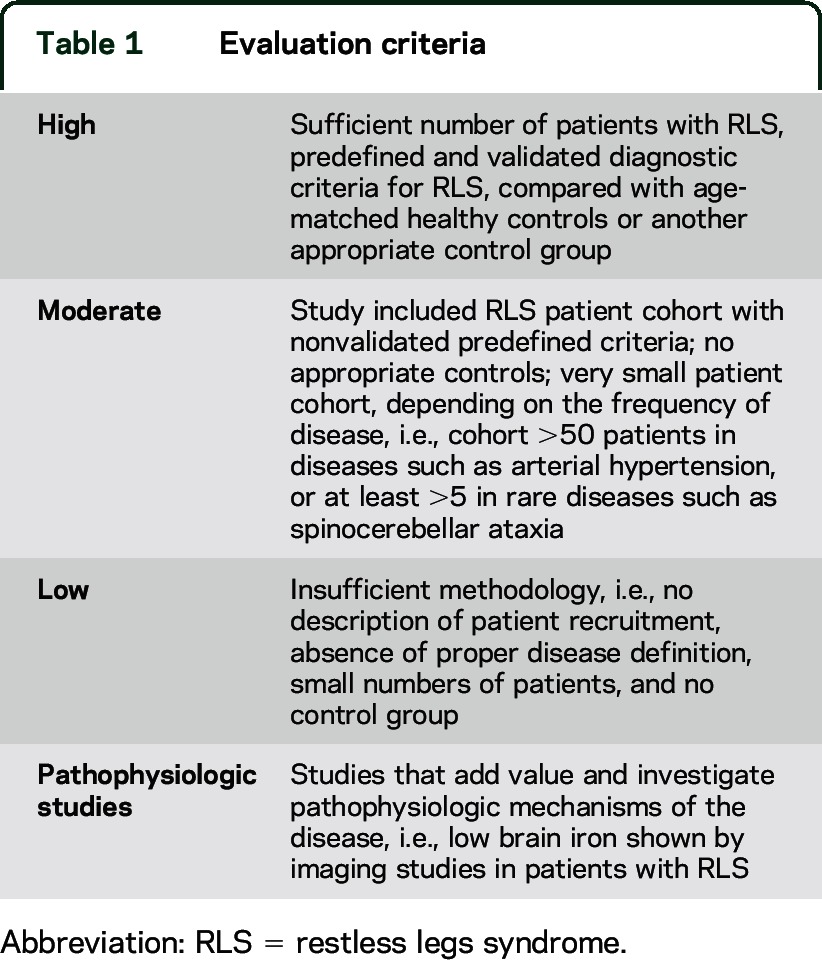
We evaluated the studies retrieved using the priority ratings described in table 1 (for details on methodology, see appendix e-1 on the Neurology® Web site at Neurology.org).
Table 1.
Evaluation criteria
MEDICAL DISORDERS
A review of additional medical disorders—varicose veins, gastrointestinal and inflammatory diseases, thyroid function, diabetes, obstructive sleep apnea, and chronic obstructive pulmonary disease—can be found in appendix e-1.
Iron deficiency.
The RLS literature on iron deficiency can be divided into 3 types of studies: pathophysiology, iron treatment, and epidemiology. Eleven pathophysiology studies all reported decreased brain/CSF measures of iron for RLS compared to controls (see table e-1 and e-References for a more complete reference list).25,e1,e2 The treatment studies reported improvement in RLS for 2 oral iron trials (with iron-deficient patients) and 3 of 4 IV iron studies—only one exclusively iron deficiency,26 2 with iron deficiency complicated by other disorders (end-stage renal disease [ESRD] and blood donor populations). One IV iron trial failed to find improvement, but this, unlike the other IV iron studies, used an iron formulation producing a rapid release of iron. Aside from this one study, the IV iron studies have the striking outcome of complete and long-lasting resolution of RLS in about 20% of those treated. The only epidemiologic studies that included adequate numbers with defined iron deficiency were those selected from an iron deficiency or RLS population. All of these show increased prevalence of RLS with iron deficiency. Several studies generally failed to find any relation between RLS occurrence and iron in medical conditions: blood donors (2 of 3 studies), kidney disease (1 study), dialysis (2 studies), and celiac disease (1 study).
Overall, studies universally demonstrated an iron-management problem for RLS.7 Iron treatment may produce partial or complete resolution of RLS in some but not all patients; cross-sectional studies report mixed evidence for increased RLS with iron deficiency. RLS in patients with clearly defined IDA has a very high prevalence (25%–35%) and iron treatments reduce or resolve RLS symptoms, but in the disease states that affect iron there is generally no consistent relation between RLS and serum iron or ferritin status.
Anemia.
RLS prevalence for IDA is 25%–35% (13 studies: 3 with blood donors, 2 ESRD, one with celiac disease, and 7 with undefined cause) without a clear relation to anemia severity. One study classified as high reported RLS prevalence in India of 34% with IDA vs 6% in healthy controls.27 Three of the 7 studies with undefined cause did not differentiate between IDA and anemia without iron deficiency.
Two of the 3 studies in blood donor populations (classified as low/very low) with presumed IDA failed to find indications of increased prevalence among blood donors with lower hemoglobin levels. One blood donor study (classified as moderate) reported a 16% prevalence of RLS in IDA individuals vs 11% for those with normal iron levels.28 It reported that oral iron treatment of IDA improved RLS.28 Two general population studies (both classified as low) produced conflicting results. RLS prevalence with anemia was 27% in China,29 but in a European population study anemia did not relate to the risk of RLS.19 However, in these studies anemia was only self-reported. The 4 studies from special medical populations (one each for celiac and heart disease, and 2 for ESRD) all had small samples, and were classified as low and failed to find any relation between hemoglobin and occurrence of RLS.
Kidney disease.
Fourteen studies investigated the prevalence of RLS in individuals with ESRD, on hemodialysis, or with chronic renal insufficiency (CRI). Nearly all studies employed an observational, cross-sectional design, evaluating hemodialysis (or CRI) populations for the presence of RLS symptoms. All except one study had a control group of hemodialysis or CRI individuals without RLS, leading to a classification of low in all but one case. Recorded prevalence ranged from 15% (Hungary)30 to 68% (European American).31 Factors associated with an increased risk for RLS included intake of Ca++ antagonists,e3 lower intact parathyroid hormone at baseline,e4 duration of dialysis (discordant results in multiple studies),30,e4–e6 lower serum transferrin saturation (discordant results in multiple studies),e4,e5 DMII (3 studies),e7–e9 number of additional comorbidities,30 Caucasian ethnicity,31 lower education levels,31 and conventional hemodialysis (vs short daily home dialysis),e10 but were, in most cases, only reported in singular studies (see table e-1 and e-References for a more complete reference list).
Hypertension.
Eighteen studies investigated either the prevalence of hypertension in individuals with RLS or vice versa. Most studies were large-scale observational, cross-sectional general population studies assessing thousands to tens of thousands of individuals. These studies were classified as high. Overall, results show large discrepancies between studies and comparison is often difficult because logistic regression analyses were adjusted for a different set of cofactors in each study and several studies only assessed men or women but not both sexes. In 4 of 6 studies, there was an increased risk for RLS in those reporting hypertension (OR 1.15–1.96).19,32–35 Individuals with RLS had an increased risk for hypertension in 6 of 10 studies (OR 1.2–2.4).33,34,e11–e20 Generally, the larger the study and the more stringent the adjustment for cofactors, the less likely an association in either direction (see table e-1 and e-References for a more complete reference list). A recent population-based retrospective cohort study used medical records for RLS diagnosis and divided the RLS population into primary and comorbid cases, finally concluding that the patients with primary RLS were younger with no increased risk for hypertension, but comorbid cases did have a higher risk for CVD and hypertension (hazard ratio [HR] 1.28; 95% confidence interval [CI] 1.18–1.40).
Pathophysiologically, single PLMS were shown to coincide with transient blood pressure elevations during polysomnography36—possibly explaining why some studies saw a correlation between increased RLS severity and blood pressure—and the presence of RLS was significantly associated with a nondipper status on 24-hour blood pressure monitoring.33 These examples show the entire spectrum of problems classifying RLS into primary, comorbid, and with and without PLMS. Hypertension can therefore be mentioned only as a weak risk factor, when regarded as a single disease, but becomes more relevant in the context of CVD, in so-called secondary RLS.37
Cardiovascular diseases.
Nineteen studies investigated the prevalence of RLS in cardiovascular disease (CVD), which comprises both coronary artery diseases and various heart diseases such as myocardial infarction and heart insufficiency. Two cross-sectional studies detected higher numbers of patients with RLS among individuals with lower coronary flow (38% and 27%) vs 17% prevalence of RLS in those with normal coronary artery flow; endothelial dysfunction is postulated as a possible mechanism of action.33,38 Large epidemiologic cohorts assessing RLS using 3 well-known questions39 in postal questionnaires could not detect any increased risk for CVD in patients with RLS,40,e20 either for women (US Health Professionals) nor when combined with men (Physician Health Study); the same results were obtained in Iceland and Sweden in population-based studies.e21 Physician-diagnosed RLS changed the results for nonfatal myocardial infarction and fatal CVD in women with an OR of 1.80 and 1.49, respectively, when the duration of RLS was >3 years.41 An association between RLS and CVD was found in the Wisconsin Sleep cohort, using interviews for diagnosis.42 Similarly, in Taiwanese patients assessed by validated phone interviews, a significant increase in the incidence of cardiovascular cases in patients with RLS was reported (22.7%).43 An increased prevalence of RLS in patients with CVD in general was not confirmed except for women who had had RLS for ≥3 years.41 Even in a recent large cohort study, this correlation was weak and applied only to comorbid RLS (HR 1.33; 95% CI 1.21–1.46) (see Hypertension).
NEUROLOGIC DISEASES
Headache.
Twenty-six studies evaluated the prevalence of RLS in patients with migraine or headaches. In migraine patients, RLS as a comorbid disorder seems to be increased, ranging from 8.7% to 39.0%.44 No difference was found between sexes for migraine with or without aura. The prevalence of RLS ranged from 1.8% without migraine to 13.7% with migraine in Asian populations.45 Weak evidence suggests that morning headache in patients with RLS may benefit from pramipexole treatment, while dopamine receptor antagonists used to treat headaches may induce akathisia. An independent review on migraine and RLS supports the concept of RLS as an important comorbidity, although the degree of association appears to be strongly determined by study design.14
The dopamine hypothesis as a common link to migraine is weaker that the link between migraine and other neuromodulators such as serotonin or norepinephrine; it is, however, corroborated by the lack of any correlation with RLS for other headache types and by a diversity of arguments favoring this link.46 In fact, no other comorbidity has such a dopaminergic link. Cluster headaches and RLS seem to have an even lower than expected prevalence.14
Stroke.
Five studies investigated the prevalence of RLS in stroke patients, providing 3 findings: first, there is not a higher incidence of stroke in patients with RLS; a non–statistically significant increase was reported in a small group of 26 patients with RLS,47 and a more recent study confirmed that RLS does not increase the incidence of stroke.35 Second, poststroke patients may develop an increased prevalence of RLS in general, possibly related to cardiovascular risk factors.40 Third, and most specifically, certain types of stroke may be located at a strategic location for inducing RLS.e22 Most frequent lesions have been found in the basal ganglia (30%) and in the pons (22%).e23
Neurodegenerative disease.
Parkinson disease.
Twenty-four investigations looked into PD populations of 2 types: de novo or treated PD, with some investigating mixed cohorts. The frequency of RLS varied substantially across countries and studies. In patients with de novo, untreated PD, the prevalence of RLS was not significantly different from controls in population-based studies from Norway (15.3% vs 9.6%)11 and Italy (lifetime prevalence of RLS in PD 5.5%, controls 4.3%12), with prevalence of 16% RLS in untreated Korean patients with PD.48
For patients with treated PD, RLS prevalence is generally higher than expected. The prevalence of RLS in Thailand was reported to range between 0.98% and 1.2% for consecutive patients with PD (untreated and treated) and 3% in Singapore vs 0.5% in ethnically matched controls. In contrast, in India, a study found 7.9% RLS in consecutive patients with PD vs 0.8% in controls,49 and 12% in patients with treated PD vs 3% in controls in Japan.e24 In a cross-sectional study from Canada, patients with treated PD showed a significantly higher prevalence for RLS (21%) compared to controls with pain 4.1%.e25 Similar increases (up to 16%) found in Korean patients with treated PD correlated with the duration but not the dosage of dopaminergic treatment.e23 This is of note as another study found an inverse correlation between the dopaminergic dosages for PD with RLS.e26 In European and US studies, the percentage of RLS in treated PD varied between 11%e27 and 24%.e26 When applying the 3 epidemiologic questions reflecting roughly the 4 essential criteria of RLS, one large studye28 found a 4-fold increased risk for PD in patients with RLS in a US male population, but only for the first 4 years after assessment.
Polyneuropathy.
Several smaller studies on RLS argue in favor of spinal or supraspinal central sensitization using quantitative sensory testing.50,51 Idiopathic RLS shows hyperalgesia to blunt pressure, pinprick, and vibratory hyperesthesia but not dynamic mechanical allodynia, which differentiates it from neuropathic pain. RLS associated with (small fiber) neuropathy has, in addition, significantly increased thermal detection thresholds, indicating the loss of small fibers.e29 On this basis, it is understandable that the majority of studies report an increased prevalence of RLS in patients with polyneuropathy (up to 40%).10 This, however, was questioned when the exclusion of mimics (e.g., cramps or nondiurnal paresthesias) decreased the prevalence of RLS to 12.2% in neuropathy patients vs 8.2% in controls.10
Multiple sclerosis.
Of the 15 studies reviewed, several reported a higher frequency of RLS in MS, thereby pointing to a possible association. However, the reported frequencies vary greatly, between 13.3%8 and 65.1%,9 perhaps indicating that the diagnosis of RLS in patients with MS on clinical grounds is extremely difficult, and mimics of RLS are possible.e30 One hypothesis concerning the possible pathophysiology of RLS in MS could be that spinal lesions increase PLMS as well as subjective sensory disturbance of the legs; however, current studies cannot prove this.
A review of further neurologic disorders—narcolepsy, hereditary ataxias, and multiple system atrophy (MSA)—can be found in appendix e-1.
DISCUSSION
This systematic review confirmed a higher prevalence of RLS in kidney disease and iron deficiency, with some likelihood of association in some cardiovascular diseases in women, diabetes (and neuropathy), migraine, and dopaminergic treatment in PD. Questionable or insufficient evidence exists for diseases such as anemia without iron deficiency, hypertension, MS, headache other than migraine, stroke, and ataxias. Furthermore, this review revealed a broad spectrum of studies that were overall heterogeneous in size, study design, methodology, and outcome measures. A common problem encountered was a lack of any appropriate control group. This is of importance because RLS is a common diseasee31 that also occurs frequently in other disorders, which makes it difficult to evaluate the prevalence unless there is an appropriate control group. From evaluation of the published studies, we draw several specific conclusions and identified a number of limitations.
Methodologic problems.
A number of large cross-sectional studies used mailed questionnaires; however, it is well-known that this methodology limits diagnostic accuracy and increases the likelihood of including RLS mimics. Some of these studies, however, investigated incident cases and excluded many diseases despite their relevance to RLS.52 Interview-based diagnosis resulted in a more accurate RLS diagnosis in comparison to the large cross-sectional studies.
Single diseases with comorbid RLS: The expected and the unexpected.
As expected, iron deficiency was one condition with a clearly increased prevalence of RLS in clinical studies but conflicting results in cross-sectional studies where iron or ferritin values are often limited or lacking. Pathophysiologic studies added information about possible disease mechanisms of iron deficiency and RLS (see Earley et al.7 for review).53,e2 A putative iron deficiency related to the CNS is supported by successful treatment trials with oral or IV iron in iron deficiency patients,26 but it may also account for a percentage of patients with RLS regardless of iron status.54 Unexpectedly, there was an overall lack of association between anemia or hemoglobin and RLS in investigations of blood donors.55 Kidney disease/ESRD and uremia (with/without dialysis) was another expected disease with RLS comorbidity, with an increased prevalence of RLS ranging from 15% to 68% in various populations worldwide.52,56 Besides these major conditions, there were inconsistent results for arterial hypertension and cardiovascular diseases. Pathophysiologic studies found that PLMS in patients with RLS induce blood pressure elevations17,36 via activation of the sympathetic system, but the clinical relevance of these findings needs to be evaluated. For cardiovascular diseases, even studies on incident cases did not provide conclusive results.41,57 For diabetes, both cross-sectional studies and clinical studies point to increased prevalence of RLS, but it could not be decided if diabetes itself19,35 or the occurrence of neuropathye32 in diabetes is the major factor.
In neurologic diseases, only migraine, but not headache in general, shows an increased prevalence of RLS.14 Of particular interest for both migraine and RLS is a possible link via the dopamine metabolism/neurotransmission: it has been postulated that migraine attacks are accompanied by an ictal dopamine release on the background of dopamine receptor hypersensitivity caused by chronic dopaminergic deficit.58
In PD cohorts, we detected a major factor affecting RLS prevalence: in the de novo untreated populations, the prevalence was similar to controls across populations.11,12 In contrast, the number of RLS-positive patients with RLS significantly increased with both disease and treatment duration,e23 but not dosages.e27 For neuropathy there was, as expected, an overall increased prevalence of RLS among patients with neuropathies. RLS associated with (small-fiber) neuropathy has, in addition, significantly increased thermal detection thresholds, indicating the loss of small fibers.e29 Hypoxia as a factor related to changes of the sympathetic nervous system may further play a role in small-fiber pathology of RLS.e33
In many areas PLMS may confound (or interfere with) the clinical diagnosis of RLS, and pathophysiologic studies showed increased PLMS, not RLS, in diseases such as arterial hypertension36 and narcolepsy.e34
Genetic and environmental interaction.
Familial RLS has an earlier age at onset in comparison to nonfamilial RLS and RLS in combination with further diseases that classically manifest later in life.59 In line with this finding, the environmental factors may trigger the manifestation of RLS symptoms and several environmental factors, e.g., multiple diseases in a single individual, may further increase the risk (figure).
Figure. Model of the hypothesis that the more genetic factors contribute to the manifestation of restless legs syndrome (RLS), the less environmental trigger is needed.

CVD = cardiovascular disease; PD = Parkinson disease.
Furthermore, RLS might be considered transient in patients with pregnancy or uremia. RLS occurs during pregnancy16 and mostly disappears after delivery,16 but manifests again in these women later in life.60 Another example is the disappearance of RLS within days after kidney transplantation, and re-occurrence with transplant failure.e33,e35 These observations, together with a benefit of iron supplementation in iron deficient and uremic patients with RLS, strongly supports the existence of a change of microenvironment that manifests through altered metabolic factors triggering RLS manifestations in genetically susceptible patients.e36 Other environmental factors, such as nutrition, may play an important role in the manifestation of symptoms, however, no RLS studies—except for one with RLS in PDe37—exist.
We suggest that a dichotomous classification of primary and secondary RLS is misleading, suggesting causality rather than the more complex RLS genetic and environmental interaction. This may especially apply for cardiovascular disease and arterial hypertension.33,38 Some of these studies even presume that hypertension may increase the risk for developing RLS, assuming a pathophysiologic mechanism via PLMS.
We recognize that treatment/resolution of some comorbid conditions may reduce RLS symptoms, and identification of these is needed for clinical trials.
Treatable conditions—IDA, diabetes, or hypertension—should be optimized first. With an increase in medical knowledge, some nontreatable conditions such as MSA, neuropathy, and others may become treatable conditions and therefore this terminology is variable, and best illustrated by the examples of dialysis and renal transplant.
Supplementary Material
ACKNOWLEDGMENT
The authors thank Arthur Walters for his comments on the manuscript, Anne-Marie Williams for editing and coordinating the tables and manuscript, and Sabine Panier for providing support in the literature search and organizing the table structure.
GLOSSARY
- CI
confidence interval
- CRI
chronic renal insufficiency
- CVD
cardiovascular disease
- DSM-5
Diagnostic and Statistical Manual of Mental Disorders, 5th edition
- ESRD
end-stage renal disease
- GWAS
genome-wide association studies
- HR
hazard ratio
- IDA
iron deficiency anemia
- MS
multiple sclerosis
- MSA
multiple system atrophy
- OR
odds ratio
- PD
Parkinson disease
- PLMS
periodic limb movements in sleep
- RLS
restless legs syndrome
Footnotes
Supplemental data at Neurology.org
AUTHOR CONTRIBUTIONS
Conception and design: C.T., J.W., R.P.A., W.P. Table organization: C.T. Evaluation and extraction of studies, topic summaries: C.T., J.W., R.P.A., B.H., W.P. Drafting the manuscript: C.T., J.W. Critical input and comments on manuscript: all authors.
STUDY FUNDING
No targeted funding reported.
DISCLOSURE
C. Trenkwalder has received honoraria for speaking, advisory boards, and/or grants from UCB Pharma, Mundipharma (Research Grant), Britannia, Teva (Research Grant), Novartis, Astra Zeneca, Desitin, and Schattauer (book). R. Allen has received honoraria, consulting fees, and/or grant support from UCB Pharma, Pharmacosmos, AMG Pharmaceuticals, Xenoport, Pfizer, and Mundipharma. B. Högl has received honoraria for speaking and/or advisory board or consulting from Otsuka, Mundipharma, UCB, Pfizer, BI, GSK, and Sanofi. W. Paulus has received honoraria from EBS Technologies, Desitin, Schaaf Verlagsgesellschaft GmbH, Aesculap, Mundipharma, and Pfizer. J. Winkelmann has received an honorarium for speaking from Xenoport and a research grant from UCB Pharma. Go to Neurology.org for full disclosures.
REFERENCES
- 1.Allen RP, Picchietti D, Hening WA, Trenkwalder C, Walters AS, Montplaisir J. Restless legs syndrome: diagnostic criteria, special considerations, and epidemiology: a report from the Restless Legs Syndrome Diagnosis and Epidemiology Workshop at the National Institutes of Health. Sleep Med 2003;4:101–119. [DOI] [PubMed] [Google Scholar]
- 2.Allen RP, Picchietti DL, Garcia-Borreguero D, et al. Restless legs syndrome/Willis-Ekbom disease diagnostic criteria: updated International Restless Legs Syndrome Study Group (IRLSSG) consensus criteria: history, rationale, description, and significance. Sleep Med 2014;15:860–873. [DOI] [PubMed] [Google Scholar]
- 3.Winkelmann J, Polo O, Provini F, et al. Genetics of restless legs syndrome (RLS): state-of-the-art and future directions. Mov Disord 2007;22(suppl 18):S449–S458. [DOI] [PubMed] [Google Scholar]
- 4.Winkelmann J, Schormair B, Lichtner P, et al. Genome-wide association study of restless legs syndrome identifies common variants in three genomic regions. Nat Genet 2007;39:1000–1006. [DOI] [PubMed] [Google Scholar]
- 5.Stefansson H, Rye DB, Hicks A, et al. A genetic risk factor for periodic limb movements in sleep. N Engl J Med 2007;357:639–647. [DOI] [PubMed] [Google Scholar]
- 6.Winkelmann J, Czamara D, Schormair B, et al. Genome-wide association study identifies novel restless legs syndrome susceptibility Loci on 2p14 and 16q12.1. PLoS Genet 2011;7:e1002171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Earley CJ, Connor J, Garcia-Borreguero D, et al. Altered brain iron homeostasis and dopaminergic function in restless legs syndrome (Willis-Ekbom disease). Sleep Med 2014;15:1288–1301. [DOI] [PubMed] [Google Scholar]
- 8.Gomez-Choco MJ, Iranzo A, Blanco Y, Graus F, Santamaria J, Saiz A. Prevalence of restless legs syndrome and REM sleep behavior disorder in multiple sclerosis. Mult Scler 2007;13:805–808. [DOI] [PubMed] [Google Scholar]
- 9.Shaygannejad V, Ardestani PE, Ghasemi M, Meamar R. Restless legs syndrome in Iranian multiple sclerosis patients: a case-control study. Int J Prev Med 2013;4:S189–S193. [PMC free article] [PubMed] [Google Scholar]
- 10.Hattan E, Chalk C, Postuma RB. Is there a higher risk of restless legs syndrome in peripheral neuropathy? Neurology 2009;72:955–960. [DOI] [PubMed] [Google Scholar]
- 11.Gjerstad MD, Tysnes OB, Larsen JP. Increased risk of leg motor restlessness but not RLS in early Parkinson disease. Neurology 2011;77:1941–1946. [DOI] [PubMed] [Google Scholar]
- 12.Angelini M, Negrotti A, Marchesi E, Bonavina G, Calzetti S. A study of the prevalence of restless legs syndrome in previously untreated Parkinson's disease patients: absence of co-morbid association. J Neurol Sci 2011;310:286–288. [DOI] [PubMed] [Google Scholar]
- 13.Ferini-Strambi L, Walters AS, Sica D. The relationship among restless legs syndrome (Willis-Ekbom disease), hypertension, cardiovascular disease, and cerebrovascular disease. J Neurol 2014;261:1051–1068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Schurks M, Winter A, Berger K, Kurth T. Migraine and restless legs syndrome: a systematic review. Cephalalgia 2014;34:777–794. [DOI] [PubMed] [Google Scholar]
- 15.Weinstock LB, Walters AS, Paueksakon P. Restless legs syndrome: theoretical roles of inflammatory and immune mechanisms. Sleep Med Rev 2012;16:341–354. [DOI] [PubMed] [Google Scholar]
- 16.Picchietti DL, Hensley JG, Bainbridge JL, et al. Consensus clinical practice guidelines for the diagnosis and treatment of restless legs syndrome/Willis-Ekbom disease during pregnancy and lactation. Sleep Med Rev 2015;22:64–77. [DOI] [PubMed] [Google Scholar]
- 17.Walters AS, Rye DB. Review of the relationship of restless legs syndrome and periodic limb movements in sleep to hypertension, heart disease, and stroke. Sleep 2009;32:589–597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed Washington, DC: American Psychiatric Association; 2013. [Google Scholar]
- 19.Szentkiralyi A, Volzke H, Hoffmann W, Trenkwalder C, Berger K. Multimorbidity and the risk of restless legs syndrome in 2 prospective cohort studies. Neurology 2014;82:2026–2033. [DOI] [PubMed] [Google Scholar]
- 20.Schulte EC, Kousi M, Tan PL, et al. Targeted resequencing and systematic in vivo functional testing identifies rare variants in MEIS1 as significant contributors to restless legs syndrome. Am J Hum Genet 2014;95:85–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Schulte EC, Knauf F, Kemlink D, et al. Variant screening of the coding regions of MEIS1 in patients with restless legs syndrome. Neurology 2011;76:1106–1108. [DOI] [PubMed] [Google Scholar]
- 22.Azcoitia V, Aracil M, Martinez AC, Torres M. The homeodomain protein Meis1 is essential for definitive hematopoiesis and vascular patterning in the mouse embryo. Dev Biol 2005;280:307–320. [DOI] [PubMed] [Google Scholar]
- 23.Vilarino-Guell C, Chai H, Keeling BH, et al. MEIS1 p.R272H in familial restless legs syndrome. Neurology 2009;73:243–245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Xiong L, Catoire H, Dion P, et al. MEIS1 intronic risk haplotype associated with restless legs syndrome affects its mRNA and protein expression levels. Hum Mol Genet 2009;18:1065–1074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Connor JR, Ponnuru P, Wang XS, Patton SM, Allen RP, Earley CJ. Profile of altered brain iron acquisition in restless legs syndrome. Brain 2011;134:959–968. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Mehmood T, Auerbach M, Earley CJ, Allen RP. Response to intravenous iron in patients with iron deficiency anemia (IDA) and restless leg syndrome (Willis‚ Ekbom disease). Sleep Med 2014;15:1473–1476. [DOI] [PubMed] [Google Scholar]
- 27.Rangarajan S, D'Souza GA. Restless legs syndrome in Indian patients having iron deficiency anemia in a tertiary care hospital. Sleep Med 2007;8:247–251. [DOI] [PubMed] [Google Scholar]
- 28.Bryant BJ, Yau YY, Arceo SM, Hopkins JA, Leitman SF. Ascertainment of iron deficiency and depletion in blood donors through screening questions for pica and restless legs syndrome. Transfusion 2013;53:1637–1644. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Li LH, Chen HB, Zhang LP, Wang ZW, Wang CP. A community-based investigation on restless legs syndrome in a town in China. Sleep Med 2012;13:342–345. [DOI] [PubMed] [Google Scholar]
- 30.Mucsi I, Molnar MZ, Rethelyi J, et al. Sleep disorders and illness intrusiveness in patients on chronic dialysis. Nephrol Dial Transpl 2004;19:1815–1822. [DOI] [PubMed] [Google Scholar]
- 31.Kutner NG, Bliwise DL. Restless legs complaint in African-American and Caucasian hemodialysis patients. Sleep Med 2002;3:497–500. [DOI] [PubMed] [Google Scholar]
- 32.De Vito K, Li Y, Batool-Anwar S, Ning Y, Han J, Gao X. Prospective study of obesity, hypertension, high cholesterol, and risk of restless legs syndrome. Mov Disord 2014;29:1044–1052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Erden EC, Erden I, Turker Y, Sivri N, Dikici S, Ozsahin M. Incremental effects of restless legs syndrome on nocturnal blood pressure in hypertensive patients and normotensive individuals. Blood Press Monit 2012;17:231–234. [DOI] [PubMed] [Google Scholar]
- 34.Ferreira KF, Eckeli A, Dach F, Schwalbach MT, Schwalbach J, Speciali JG. Prevalence of restless legs syndrome in patients with chronic pain in Maputo, Mozambique. Sleep Med 2013;14:1417–1418. [DOI] [PubMed] [Google Scholar]
- 35.Szentkiralyi A, Volzke H, Hoffmann W, Happe S, Berger K. A time sequence analysis of the relationship between cardiovascular risk factors, vascular diseases and restless legs syndrome in the general population. J Sleep Res 2013;22:434–442. [DOI] [PubMed] [Google Scholar]
- 36.Pennestri MH, Montplaisir J, Fradette L, Lavigne G, Colombo R, Lanfranchi PA. Blood pressure changes associated with periodic leg movements during sleep in healthy subjects. Sleep Med 2013;14:555–561. [DOI] [PubMed] [Google Scholar]
- 37.Van Den Eeden SK, Albers KB, Davidson JE, et al. Risk of cardiovascular disease associated with a restless legs syndrome diagnosis in a retrospective cohort study from Kaiser Permanente Northern California. Sleep 2015;38:1009–1015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Erden I, Cakcak Erden E, Durmus H, et al. Association between restless leg syndrome and slow coronary flow. Anadolu Kardiyol Derg 2014;14:612–616. [DOI] [PubMed] [Google Scholar]
- 39.Rothdach AJ, Trenkwalder C, Haberstock J, Keil U, Berger K. Prevalence and risk factors of RLS in an elderly population: the MEMO study: Memory and Morbidity in Augsburg Elderly. Neurology 2000;54:1064–1068. [DOI] [PubMed] [Google Scholar]
- 40.Winter AC, Schurks M, Glynn RJ, et al. Vascular risk factors, cardiovascular disease, and restless legs syndrome in women. Am J Med 2013;126:220–227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Li Y, Walters AS, Chiuve SE, Rimm EB, Winkelman JW, Gao X. Prospective study of restless legs syndrome and coronary heart disease among women. Circulation 2012;126:1689–1694. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Winkelman JW, Shahar E, Sharief I, Gottlieb DJ. Association of restless legs syndrome and cardiovascular disease in the Sleep Heart Health Study. Neurology 2008;70:35–42. [DOI] [PubMed] [Google Scholar]
- 43.Chen NH, Chuang LP, Yang CT, et al. The prevalence of restless legs syndrome in Taiwanese adults. Psychiatry Clin Neurosci 2010;64:170–178. [DOI] [PubMed] [Google Scholar]
- 44.Schurks M, Winter AC, Berger K, Buring JE, Kurth T. Migraine and restless legs syndrome in women. Cephalalgia 2012;32:382–389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Suzuki S, Suzuki K, Miyamoto M, et al. Evaluation of contributing factors to restless legs syndrome in migraine patients. J Neurol 2011;258:2026–2035. [DOI] [PubMed] [Google Scholar]
- 46.Akerman S, Goadsby PJ. Dopamine and migraine: biology and clinical implications. Cephalalgia 2007;27:1308–1314. [DOI] [PubMed] [Google Scholar]
- 47.Walters AS, Moussouttas M, Siddiqui F, et al. Prevalence of stroke in restless legs syndrome: initial results point to the need for more sophisticated studies. Open Neurol J 2010;4:73–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Lee JE, Shin HW, Kim KS, Sohn YH. Factors contributing to the development of restless legs syndrome in patients with Parkinson disease. Mov Disord 2009;24:579–582. [DOI] [PubMed] [Google Scholar]
- 49.Krishnan PR, Bhatia M, Behari M. Restless legs syndrome in Parkinson's disease: a case-controlled study. Mov Disord 2003;18:181–185. [DOI] [PubMed] [Google Scholar]
- 50.Gemignani F, Brindani F, Vitetta F, Marbini A. Restless legs syndrome and painful neuropathy-retrospective study: a role for nociceptive deafferentation? Pain Med 2009;10:1481–1486. [DOI] [PubMed] [Google Scholar]
- 51.Lim YM, Chang SE, Chung S, Kang BH, Kim KK. Small fiber function in drug naive patients with idiopathic restless legs syndrome. J Clin Neurosci 2012;19:702–705. [DOI] [PubMed] [Google Scholar]
- 52.Berger K, Kurth T. RLS epidemiology: frequencies, risk factors and methods in population studies. Mov Disord 2007;22(suppl 18):S420–S423. [DOI] [PubMed] [Google Scholar]
- 53.Earley CJ, B Barker P, Horska A, Allen RP. MRI-determined regional brain iron concentrations in early- and late-onset restless legs syndrome. Sleep Med 2006;7:458–461. [DOI] [PubMed] [Google Scholar]
- 54.Allen RP, Adler CH, Du W, Butcher A, Bregman DB, Earley CJ. Clinical efficacy and safety of IV ferric carboxymaltose (FCM) treatment of RLS: a multi-centred, placebo-controlled preliminary clinical trial. Sleep Med 2011;12:906–913. [DOI] [PubMed] [Google Scholar]
- 55.Spencer BR, Kleinman S, Wright DJ, et al. Restless legs syndrome, pica, and iron status in blood donors. Transfusion 2013;53:1645–1652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Garcia-Borreguero D, Egatz R, Winkelmann J, Berger K. Epidemiology of restless legs syndrome: the current status. Sleep Med Rev 2006;10:153–167. [DOI] [PubMed] [Google Scholar]
- 57.Winter AC, Schurks M, Glynn RJ, et al. Restless legs syndrome and risk of incident cardiovascular disease in women and men: prospective cohort study. BMJ Open 2012;2:e000866. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Barbanti P, Fofi L, Aurilia C, Egeo G. Dopaminergic symptoms in migraine. Neurol Sci 2013;34(suppl 1):S67–S70. [DOI] [PubMed] [Google Scholar]
- 59.Winkelmann J, Muller-Myhsok B, Wittchen HU, et al. Complex segregation analysis of restless legs syndrome provides evidence for an autosomal dominant mode of inheritance in early age at onset families. Ann Neurol 2002;52:297–302. [DOI] [PubMed] [Google Scholar]
- 60.Winkelmann J, Wetter TC, Collado-Seidel V, et al. Clinical characteristics and frequency of the hereditary restless legs syndrome in a population of 300 patients. Sleep 2000;23:597–602. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.