

Abstract
Objectives
The Parkinson Associated Risk Syndrome Study identified a cohort of healthy adults with hyposmia and dopamine transporter binding reduction to characterize individuals at risk for Parkinson's disease (PD). We describe the cognitive profile of this cohort.
Methods
Individuals older than 50 y without PD were recruited. Two hundred twenty-five completed cognitive testing and were included in the final analysis. A neuropsychological test battery was administered and normative scores created for global cognition, memory, executive function/working memory, processing speed/attention, visuospatial abilities, and language domains. Other non-motor symptoms (constipation, depression, anxiety, and rapid eye movement sleep behavior disorder) were assessed through questionnaires.
Results
Individuals with both hyposmia and reduced dopamine transporter binding (n = 38) had lower mean scores for global cognition, executive function/working memory, and memory compared with all other participants (n = 187). In separate multivariate logistic regression models, lower global cognition (odds ratio, 1.97, P = 0.004), and specifically executive function/working memory (odds ratio, 1.84, P = 0.004) scores were associated with membership in the hyposmia with dopamine transporter reduction group. Combining hyposmia with relative impairment on specific cognitive domains increased the odds of dopamine transporter binding reduction compared with hyposmia alone, with the greatest increase in odds for hyposmia plus executive function/working memory relative impairment (68% increase in odds from 4.14 to 6.96).
Conclusion
Changes in global cognitive abilities, and specifically executive function/working memory, are present in individuals at risk for PD. Combining non-motor features, including cognition, improves prediction of dopamine transporter binding reduction.
Keywords: Parkinson's, cognition, prodromal, dopaminergic deficit, hyposmia
Neurodegeneration in Parkinson's disease (PD) begins years before development of motor symptoms.1 Increasingly we have recognized, largely based on multiple failed disease-modification trials,2 that intervention must occur in the earliest stages of the disease to impact neurodegeneration. Characterization of the prodromal PD phase is essential to enable expeditious identification of individuals who may benefit from disease-modifying agents as they emerge. This provides the impetus for several ongoing studies, including the Parkinson Associated Risk Syndrome (PARS) study.3,4 The PARS cohort was established to test a two-stage screening strategy for PD consisting of olfactory testing followed by dopamine transporter (DAT) imaging.
The PARS includes a battery of assessments of non-motor symptoms selected based on evidence suggesting that they may be informative regarding prodromal PD. For example, the incidence of PD is nearly five times greater in individuals with constipation during midlife compared with those without,5 and the odds of developing PD in those with depression are more than three times greater than in those without.6 Increased anxiety is also associated with increased relative risk for PD,7 and more than 50% of individuals with rapid eye movement (REM) sleep behavior disorder (RBD) will go on to develop a neurodegenerative synucleinopathy.8 Although the prevalence of cognitive dysfunction in early PD is as high as 30%,9,10 and abnormalities in executive function, verbal memory, and attention have been shown in idiopathic RBD,11 cognitive function in prodromal PD has not been well characterized. We herein examine the cognitive profile of individuals presumed to be at increased risk of PD based on hyposmia and DAT reduction.
Methods
The PARS protocol was approved by the Western Institutional Review Board, the Human Research Protection Office at the US Army Medical Research Material and Command, and participating center local institutional review boards. Informed consent was obtained from each subject.
Methods for participant recruitment and assessments have been previously described.4,12 Briefly, regional mailings, email invitations, and posts to PD foundation websites were used to target individuals with or without a family history of PD living in specific geographic regions. Recruitment and study assessments occurred at 16 movement disorders specialty clinics in the United States. Inclusion criteria were (1) age older than 50 years (or within 10 years of age of onset of an affected PD relative) and (2) no known reason for abnormal olfaction (eg, nasal trauma, sinus infection/surgery). Exclusion criteria included (1) history of PD or other neurodegenerative disorder, (2) history of dementia or evidence for it on examination (including Mini-Mental State Examination score < 27), and (3) evidence of parkinsonism on examination thought to be consistent with PD (as determined by the investigator).
Self-Administered Non-motor Assessments
The following assessments were mailed to participants for self-administration:
Olfaction: assessed with the 40-item University of Pennsylvania Smell Identification Test.13 Subjects scoring in the 15th percentile or lower based on age and sex (based on study-specific norms, as described4) were classified as hyposmic; all others were considered normosmic.
Bowel movement frequency was assessed with an adapted version of a previously used questionnaire5; constipation was defined as less than 1 bowel movement per day.
Motor symptoms were assessed using the PD Symptom Rating Scale.14 Endorsement of two or more symptoms was considered positive.
RBD was assessed via a questionnaire administered to participants who had input from a bed partner (n = 143). The questionnaire was a three-item modified version of a validated RBD questionnaire.15 Subjects were considered to have RBD if any RBD symptom was reported to occur at least once per month.
Anxiety was assessed with the State-Trait Anxiety Inventory.16 A score greater than 39 on either the state or trait forms is considered significant anxiety.17
Depression was assessed with the Center for Epidemiological Studies Depression Scale. A score of16 or higher indicates significant depression.18
Clinical Evaluation
All hyposmic subjects were invited to participate in the clinical and imaging assessments. Frequency matching was used to select a group of age- (within 5 years) and sex-matched normosmic controls in a 2:1 hyposmic:normosmic ratio. Participants underwent baseline clinical evaluations at the nearest participating movement disorder specialty clinic, including medical history and medication-use interview and administration of the Unified PD Rating Scale (UPDRS) and a PD diagnostic questionnaire, which was completed by clinical investigators blinded to the results of olfactory testing and DAT imaging.
Imaging Evaluation
Dopamine transporter imaging using [123I]-fluoro-propyl-beta-carbomethoxy-3beta-(4-iodophenyl) tropane ([123I]β-CIT) single-photon emission computed tomography (SPECT) was performed at a single imaging center (Institute for Neurodegenerative Disorders, New Haven, CT, USA). Participants received an intravenous administration of 6 mCi [123I]β-CIT. Single-photon emission computed tomography acquisition was performed as previously described.19 The striatal binding ratio (SBR) (mean binding in the bilateral putamen and caudate) was determined from SPECT images, using a standardized region of interest analysis. For the purpose of these analyses, baseline scans were categorized as DAT reduction (≤80% age-expected lowest putamen [123I]β-CIT uptake) or no DAT reduction (>80% age-expected lowest putamen [123I]β-CIT uptake)21. This cutoff was chosen to maximize detection of potentially at-risk individuals. Neuroimaging analyses were performed by experts blinded to all clinical information, neuropsychological test results, and olfactory testing.
Cognitive Assessments
Cognitive testing was introduced after study initiation, therefore a subset of participants did not undergo cognitive testing. Otherwise cognition was assessed (at the time of clinical or imaging evaluation) by using 23 variables from 17 tests that were specific to the following domains:
Memory
Memory was tested with the following tests: (1) Hopkins Verbal Learning Test—Revised (immediate and delayed recall and recognition),22 (2) Repeatable Battery for Assessment of Neuropsychological Status (RBANS Battery A, immediate and delayed recall of the “fire story” and figure recall),23 and (3) Wechsler Memory Scale (WMS-III) logical memory story A, immediate and delayed recall.24
Executive Function/Working Memory
Executive function/working memory was tested with the following tests: (1) Controlled Oral Word Association Test (phonemic fluency: total word generation for letters F, A, and S and semantic fluency: total word generation for male names, animal, fruit, and vegetable categories)25; (2) Trail Making Test Part B (time to complete)26; and (3) Wechsler Adult Intelligence Scale (WAIS)- III digit span backwards.24
Processing Speed/Attention
Processing speed and attention were measured by the following tests: (1) WAIS-III Digit Symbol Coding (raw score), (2) WAIS-III symbol search (raw score), (3) WAIS-III digit span forward,24 and (4) Trail Making Test Part A (time to complete).26
Visuospatial Function
Visuospatial function was tested by the (1) RBANS Battery A figure copying and line orientation,23 (2) Clock Drawing Test, (3) WAIS III Block Design (raw score),24 (4) Test of Visual-Perceptual Skills (TVPS)-UL-R,27 (5) Visual Object and Space Perception Battery (silhouettes animals and silhouettes objects).28
Language
Language was tested with the Boston Naming Test (split half raw score).29
Statistical Analyses
Baseline demographic and hyposmic/normosmic status for PARS subjects who did and did not complete the cognitive testing were compared using t tests and χ2 tests.
Scores for each cognitive test were reversed, if needed, so that higher scores would indicate better performance. As previously described,30 for each raw and unadjusted cognitive variable a z score for each subject was calculated by subtracting the mean and dividing by the standard deviation for the entire study population. A domain z score was then created by summing z scores for all tests pertaining to that domain, then subtracting the mean for that domain and dividing by the standard deviation for the resulting score. A global cognitive score based on the domain z scores was calculated in the same way; although the number of cognitive variables included in each domain varied, each cognitive domain was given equal weight when calculating the global cognitive score. For the purpose of these analyses, z scores were signed so that higher scores indicate better performance, and odds ratios are presented so that an odds ratio greater than 1 implies an increased risk of impairment. Because the sample was drawn from community-dwelling generally healthy and neurologically normal adults, we did not anticipate significant cognitive dysfunction in this group, and reference to impairment within this manuscript is relative. Most of the analyses used cognitive measures as continuous z scores, but, for defining groups with or without relative cognitive impairment, dichotomized variables were calculated based on a score greater than 1 standard deviation (SD) below the group standardized mean, within the range recommended to identify mild cognitive impairment in PD.31
Three groups were defined for comparison: (1) subjects with both hyposmia and a reduction in DAT binding (hyposmia/+DAT reduction group), (2) subjects with hyposmia without a reduction in DAT binding (hyposmia/-DAT reduction group), and (3) subjects with normosmia with no reduction in DAT binding (normosmia/-DAT reduction group). Among all of the groups, the hyposmia/+DAT reduction group is considered at greatest risk for PD, and the normosmia/-DAT reduction group is likely most representative of the general population because of the absence of the two primary risk factors being evaluated in the PARS study.
T tests and Kruskal-Wallis tests were used to compare cognitive function and SBR between groups, and the effect size was estimated using Cohen's d. Logistic regression models, with the domain z scores as predictors, were used to examine associations with group status and also with DAT reduction status. Relative cognitive impairment was evaluated in separate models by comparing subjects with both hyposmia and relatively worse cognitive performance with subjects with neither; non-motor symptoms were similarly evaluated. Models were adjusted for age, education, and sex, all factors that may influence cognitive performance. Influence plots were examined for possible outliers. All P values are two-tailed. Nominal P values are reported, and those P values from logistic regression models that would remain significant after a Bonferroni correction are bolded. All analyses were performed using SAS software version 9.3 (SAS Institute).
Results
Sample
Of a total of 303 individuals (203 with hyposmia, and 100 with normosmia) who completed the baseline clinical and imaging evaluations for the PARS study, 225 also completed the detailed baseline cognitive testing and were included in the final analysis. Compared with those who completed the battery, those not tested (n = 78) were significantly younger (mean base-line age, 58.6 years [SD = 8.5] vs 66.0 [SD = 8.4], P < 0.001), and more likely to be female (58/78 [74%] vs 95/225 [42%], P < 0.0001), hyposmic (61/78 [78%] vs 142/225 [63%], P = 0.01), and to have a family member with PD (60/78 [77%] vs 86/225 [38%], P < 0.001).
Among the 225 participants, 38 were in the hyposmia/+DAT reduction group, 104 participants were in the hyposmia/-DAT reduction group, and 76 were in the normosmia/-DAT reduction group (Fig. 1). Mean DAT SBR was 4.16 (SD = 0.82) in the hyposmia/+DAT reduction group compared with 5.96 (SD = 1.00) in the normosmia/-DAT reduction group (P < 0.001) (Fig. 2). No significant differences were found between the hyposmia/+DAT reduction group (n = 38) and all others (n = 187) in history of cardiovascular, neurological, or psychiatric disorders, or in use of antidepressant and antipsychotic medications, or medications for cognitive dysfunction or dementia.
Fig. 1.

Frequency of hyposmia and dopamine transporter reduction in sample with cognitive testing.
Fig. 2.
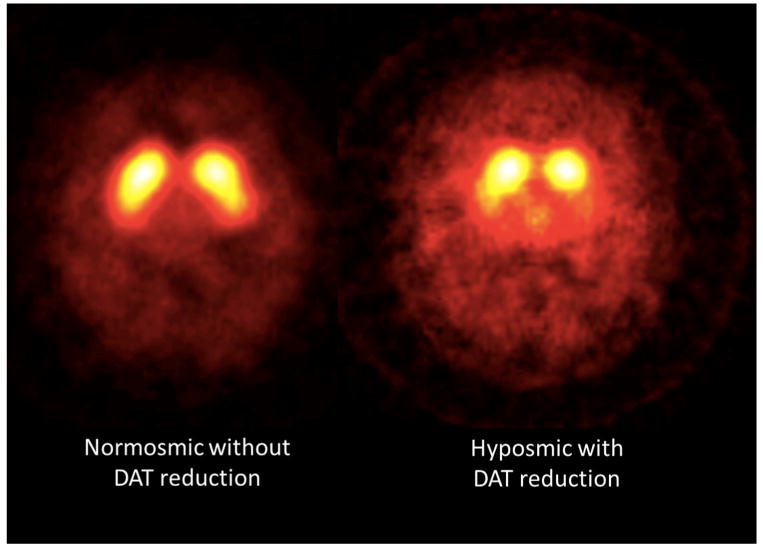
Representative dopamine transporter single-photon emission computed tomography images. [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
Cognitive Performance in the Hyposmia/+DAT Reduction Group Versus All Other Subjects
Compared with the rest of the sample (n+187), the hyposmia/+DAT reduction group was more likely to be male and had lower DAT SBR and higher UPDRS scores, although UPDRS scores were low in both groups (Table 1) (despite the higher UPDRS motor scores, none of the participants included in this analysis, in any group, met criteria for a diagnosis of PD based on the investigator's opinion). The 38 individuals in this hyposmia/+DAT reduction group had significantly lower mean z scores of global cognition, executive function/working memory, and memory compared with all other participants combined on bivariate analyses, with small to medium effect sizes (Supplemental Data Table e-1).
Table 1. Demographics and clinical features of hyposmia/+DAT reduction group versus all others.
| Variable | Hyposmia/+DAT Reduction Groupa (n = 38) | All Othersb (n = 187) | P Value for Differencesc |
|---|---|---|---|
| Mean age at cognitive testing (SD; range) | 65.7 (6.9; 49.4-79.1) | 67.1 (8.4; 50.4-92.9) | 0.50 |
| Male sex (N, %) | 28 (74%) | 102 (55%) | 0.03 |
| Mean education in years (SD; range) | 15.6 (2.7; 12.0-20.0) | 16.0 (2.3; 9.0-20.0) | 0.37 |
| ≥ Family member with PD (n, %) | 12 (32%) | 74 (40%) | 0.36 |
| Smoking history, current or past (n, %) | 20 (53%) | 97 (52%) | 0.99 |
| Mean total UPDRS (SD; range) | 4.6 (3.5; 0.0-11.0) | 2.6 (3.5; 0.0-25.0) | <0.001 |
| Mean striatal binding ratio (SD; range) | 4.2 (0.8; 2.0-5.5) | 5.8 (1.0; 2.5-9.3) | <0.001 |
DAT binding ≤80%.
Normosmia/-DAT reduction, hyposmia/-DAT reduction, or normosmics with DAT reduction.
Kruskal-Wallis test or χ2 test.
DAT, dopamine transporter; SD, standard deviation; PD, Parkinson's disease; UPDRS, Unified Parkinson's Disease Rating Scale.
In separate multivariate logistic regression models adjusted for age, sex, and years of education, worse global cognition (odds ratio [OR] = 1.97; 95% confidence interval [CI], 1.24-3.12), executive function/working memory (OR = 1.84; 95%CI, 1.21-2.81), memory (OR = 1.64; 95%CI, 1.09-2.48), and processing speed/attention (OR = 1.53; 95%CI, 1.00-2.34) were associated with the combination of hyposmia and DAT reduction (Table 2). Results were similar when three outliers were removed. When these results were adjusted for multiple comparisons using a Bonferroni correction for the six statistical test results shown in Table 2, the global cognition and executive function findings remained significant.
Table 2. Association of cognitive domains with membership in the hyposmia/+DAT reduction group (n = 38) versus all others (n = 187)a.
| Variable | Regression Coefficient | Standard Error | Wald X2 | Odds Ratio | 95% CI | P value |
|---|---|---|---|---|---|---|
| Global cognition | 0.68 | 0.24 | 8.30 | 1.97 | 1.24-3.12 | 0.004b |
| Executive function/working memory | 0.61 | 0.21 | 8.18 | 1.84 | 1.21-2.81 | 0.004b |
| Language | 0.25 | 0.20 | 1.66 | 1.29 | 0.88-1.90 | 0.20 |
| Memory | 0.50 | 0.21 | 5.52 | 1.64 | 1.09-2.48 | 0.02 |
| Processing speed/attention | 0.43 | 0.22 | 3.92 | 1.53 | 1.00-2.34 | 0.048 |
| Visuospatial | 0.17 | 0.21 | 0.65 | 1.18 | 0.79-1.78 | 0.42 |
Separate logistic regression models adjusted for age at testing, sex, and education.
Global cognition and executive function remained significant after adjusting for multiple comparisons using a Bonferroni corrected threshold for statistical significance of P < 0.008.
DAT, dopamine transporter.
Cognitive Performance in the Hyposmia/+DAT Reduction Group Versus Normosmia/-DAT Reduction Group
When the hyposmia/+DAT reduction group (n538) was compared with the normosmia/-DAT reduction group (n = 76) in separate multivariate logistic regression models, significant between-group differences were noted in global cognition (OR = 2.54; 95%CI, 1.42-4.54), executive function/working memory (OR = 2.03; 95%CI, 1.27-3.27), memory (OR = 1.71; 95%CI, 1.03-2.82), and processing speed/attention (OR = 1.91; 95%CI, 1.14-3.21) (Supplemental Data Table e-2). When these results were adjusted for multiple comparisons using a Bonferroni correction for the six statistical test results shown in Supplemental Data Table e-2, the global cognition and executive function findings remained significant.
Cognitive Performance in the Hyposmia/-DAT Reduction Group Versus Normosmia/-DAT Reduction Group
Comparisons of the hyposmia/-DAT reduction group (n = 104) with the normosmia/-DAT reduction group (n = 76) did not show significant differences in cognition between the two groups (Supplemental Data Table e-3).
Association of Cognitive Performance and DAT Reduction
As previously reported,12 presence of hyposmia was strongly associated with DAT reduction in the PARS cohort. In the current analysis, hyposmic subjects with relative cognitive impairment (defined as >1 SD below the group mean score for the global or specific domain scores) were compared with normosmic subjects who were without cognitive impairment, for evidence of DAT reduction (using the cutoff of ≤80% of age-expected [123I]β-CIT uptake to define DAT reduction). The odds ratio of hyposmia alone as a predictor of DAT reduction was 4.14 (95%CI, 1.68-10.16) in a logistic regression model adjusting for age, sex, and education. The odds ratios for DAT reduction increased over that for hyposmia alone when either relative global cognitive impairment or individual cognitive domain impairments were separately added to the model (Table 3). For example, presence of DAT reduction in subjects with hyposmia plus relative executive function/working memory impairment (n = 31; 35% with DAT binding ≤80%) was compared with nonimpaired normosmics (n = 74, 8% with DAT binding ≤80%), yielding an odds ratio of 6.96; 95% CI, 1.97-24.64, a 68% increase over that of hyposmia alone (4.14). When these results were adjusted for multiple comparisons using a Bonferroni correction for the six statistical test results shown in Table 3, the hyposmia + global cognitive impairment and hyposmia + executive function impairment findings remained significant.
Table 3. Association of hyposmia plus specific cognitive domain impairmentsa with DAT reduction.
| Cognitive Domain | With Both Risk Factors | Without Either Risk Factor | Odds Ratio (95% CI)b | P Value |
|---|---|---|---|---|
| Hyposmia alone | 142 | 83 | 4.14 (1.68-10.16) | 0.002 |
| Hyposmia + global cognitive impairment | 36 | 76 | 6.86 (1.67-28.25) | 0.008c |
| Hyposmia + executive function/working memory impairment | 31 | 74 | 6.96 (1.97-24.64) | 0.003c |
| Hyposmia + language impairment | 23 | 70 | 3.57 (0.64-19.88) | 0.15 |
| Hyposmia + memory impairment | 31 | 73 | 5.83 (1.48-23.04) | 0.01 |
| Hyposmia + processing speed/attention impairment | 26 | 78 | 5.38 (1.14-25.30) | 0.03 |
| Hyposmia + visuospatial impairment | 30 | 76 | 3.84 (0.98-15.11) | 0.05 |
>1 SD below standardized mean score.
Separate logistic regression models adjusted for age at testing, sex, and education.
Hyposmia + global cognitive impairment and hyposmia + executive function impairment remained significant after adjusting for multiple comparisons using a Bonferroni corrected threshold for statistical significance of P < 0.008.
Similarly, examining the combination of hyposmia in the presence of other non-motor symptoms in separate logistic regression models, adjusting for age at testing, sex, and education, the combination of hyposmia plus depression, compared with subjects with neither, increased the odds of having DAT reduction by 189%, from 4.14 (95% CI, 1.68-10.16) for hyposmia alone to 11.98 (95%CI, 2.93-48.95). (Additional adjustment for depression did not substantially change the results presented in the previous tables.) The combination of hyposmia and constipation (OR = 9.27; 95%CI, 2.46-35.02) also increased the odds of DAT reduction, whereas adding presence of either RBD symptoms or anxiety did not meaningfully alter the odds compared with those for hyposmia alone (data not shown).
Associations with DAT reduction were also examined among the entire group of 142 patients with hyposmia (n = 38 with DAT reduction and n = 104 without) in a single logistic regression model including age, sex, education, global cognitive z score, and presence or absence of anxiety, depression, and constipation. Presence of depression (OR = 4.70; 95%CI, 0.77-28.78; P = 0.09) and worse global cognitive performance (OR = 1.58; 95%CI, 0.94-2.64; P = 50.08) were associated with DAT reduction.
Discussion
We found that cognitive performance was worse in a group of individuals enriched for risk of developing PD because of the presence of both hyposmia and DAT reduction. Cognitive differences in this cohort of individuals at risk for PD were most pronounced on the global cognitive measure, and more specifically for executive abilities (with some suggestion for memory and attention as well). This suggests that cognitive abnormalities may be part of the prodromal PD syndrome. This study extends the findings in early, untreated (incident) PD.9
Although a variety of non-motor symptoms may be part of prodromal PD, many, including hyposmia, constipation, and depression or anxiety, are relatively nonspecific, particularly in older adults. Findings from the PARS cohort presented here and elsewhere12 suggest that combining various non-motor signs and symptoms along with hyposmia increases the association with DAT reduction. The results presented herein suggest the incorporation of cognitive performance into such models as well. Of course, predictive models will require optimization to minimize the tradeoff in negative predictive value that will occur for models with strong positive predictive value.
Very few studies have evaluated the cognitive profile of individuals at risk for PD. In the Honolulu-Asia Aging Study31 of 3,387 men without PD, 17% of those scoring in the lowest tertile on simple reaction time testing exhibited incidental Lewy bodies postmortem, compared with 6% in the other tertiles. In addition, those scoring in the lowest quartile on executive function scales had an incidence of PD of 26.1/10,000 person years, compared with 10.9 for those scoring in the highest quartile.
It is likely most individuals in the PARS cohort who have hyposmia without DAT deficit will not go on to develop PD. The cause of their hyposmia was not part of our analyses. Data suggest that the presence of hyposmia, irrespective of the underlying cause, is associated with cognitive dysfunction. Subjective cognitive complaints are common among individuals with isolated hyposmia,32 and among older adults without cognitive impairment, olfactory loss has been associated with increased risk of mild cognitive impairment and predicts conversion to Alzheimer's disease.33 In our cohort, as well another hyposmic cohort examined for cognitive deficits,34 subjects identified just on the basis of hyposmia (with no DAT reduction) did not show significant differences in cognition compared with those subjects without hyposmia. Ongoing longitudinal analyses of our cohort will investigate whether presence of hyposmia itself, irrespective of the underlying cause, is associated with greater rates of decline in cognition over time.
Although our data do not allow any conclusions to be drawn regarding the cause of cognitive dysfunction in individuals potentially at risk of PD, several possibilities warrant consideration and future study. In the general population, an association between DAT binding and cognitive function was demonstrated in 12 individuals without PD,35 and in a cohort of 491 PD patients, de novo at baseline, lower baseline striatal DAT binding was associated with global cognitive decline over a 22-month period.36 Conversely, cognitive reductions in prodromal PD may be partially mediated by early extrastriatal disease pathology or nondopaminergic systems. This is supported by animal data; in a mouse model of PD, cognitive dysfunction (abnormalities in spatial learning and novel object recognition) was noted preceding motor abnormalities and before loss of dopaminergic neurons was expected.37 In humans, abnormalities in noradrenergic38 and cholinergic pathways39 have been implicated in cognitive dysfunction in PD and are present even in early disease stages.40 Involvement of these neurotransmitter systems occurs early in Braak's proposed pathologic staging,41 at a time when brainstem nuclei and the olfactory bulb are hypothesized to be involved by the pathologic process but before involvement of nigral or cortical neurons (ie, in the premotor PD phase), making them prime candidates for mediating cognitive dysfunction in prodromal PD. A stronger association of hyposmia with cholinergic, as compared with dopaminergic, denervation supports this hypothesis.42 Functional imaging of these other neurotransmitter systems in prodromal cohorts would offer a means for further investigation. Another consideration is that progression of neuropathology in PD does not conform to Braak's staging system in all cases.43 Instead, possibly in at least a subset of patients with prodromal PD, cortical involvement with Lewy body pathology precedes nigral involvement, particularly in those more likely to ultimately be diagnosed with dementia with Lewy bodies.
A limitation of this study is that, because cognitive testing was implemented after study initiation, only 74% of the PARS sample completed it, so our sample may not be fully representative of the entire PARS cohort. Those who did not complete cognitive testing were younger than those who did, and our findings therefore also may not be generalized to younger PD at-risk groups. In addition, the PARS cohort was recruited from both family members of PD patients and the community, so this may not be entirely representative of a typical prodromal PD group. Although we administered a relatively large battery of neuropsychological tests, we acknowledge that some of the tests can be assigned to more than one cognitive domain. Furthermore, the approach we took of creating both domain scores and a global cognitive measure accounting for all the domains, although previously used30, has not been explicitly validated. Future analyses could use principal components or factor analysis to assign the cognitive variables to domains in an unbiased fashion, and to validate the derivation of the global cognitive score from domain subscores. We emphasize that, because these analyses were exploratory, our results will need to be confirmed in a subsequent study. The RBD assessments were limited to only the subset of participants with a bed partner, and the questions administered may have lacked diagnostic accuracy. This may account for the lack of improvement in prediction of DAT reduction when adding RBD into the model along with hyposmia. Finally, because no cutoffs have been defined for what is considered normal versus abnormal DAT binding in prodromal PD, we selected a liberal cutoff of 80% or less of age-expected putamen [123I]β-CIT uptake to minimize risk of misclassification of at-risk individuals in the normal group. Future work examining cognition in larger cohorts with more conservative cutoffs is needed.
Our study demonstrates cognitive abnormalities in a PD at-risk cohort. Our data support the need to extensively characterize non-motor features of prodromal PD and suggest that combining a range of demographic and non-motor features may maximize the accuracy of predicting risk.31 The significance of these data, and their utility in clinical practice, will ultimately be determined through longitudinal follow-up currently underway to evaluate the rate of phenoconversion to PD among these at-risk subjects. This will allow us to validate our techniques for identifying prodromal individuals and our predictive models for determining their future risk of PD. Ongoing work to characterize prodromal PD will be essential in quantifying disease risk and ultimately identifying which individuals are candidates for disease-modifying interventions during the prodromal period.
Supplementary Material
Acknowledgments
Funding agencies: Support for this study is provided by the Department of Defense award number W81XWH-06-067
Appendix. PARS Study Group Investigators and Coordinators
David Russell, MD, Abby Fiocco, The Institute for Neurodegenerative Disorders, New Haven, CT; Kapil-Sethi, MD, Paula Jackson, Medical College of Georgia, Augusta, GA; Samuel Frank, MD, Cathi A. Thomas MS, RN, Raymond C. James, Boston University Medical Center, Boston, MA; Tanya Simuni, MD, Emily Borushko, MPH, Northwestern University, Chicago, Ill; Matt Stern, MD, Jacqueline Rick, PhD, University of Pennsylvania PDMDC, Philadelphia, PA; Robert Hauser, MD, LeylaKhavarian, University of South Florida, Tampa, FL; Irene Richard, MD, Cheryl Deeley, University of Rochester, Rochester, NY; Grace S. Liang, MD, Liza Infeld, The Parkinson's Institute, Sunnyvale, CA; Charles H. Adler, MD, PhD, Amy K. Duffy, Mayo Clinic Arizona, Scottsdale, AZ; Rachel Saunders-Pullman, MD, MPH, Beth Israel Medical Center, New York, NY; Marian L. Evatt, MD, Becky McMurray, RN, Emory University, Atlanta, GA; Eugene Lai, MD, Shawna Johnson RN BSN, Michael E. DeBakey Department of Veteran's Affairs Medical Center, Houston, TX; Indu Subramanian, MD, Angelina Gratiano, UCLA Medical Center, Los Angeles, CA; Kathryn Chung, MD, Brenna Lobb, Susan O'Conner, Portland VA Medical Center, Portland, OR.
Footnotes
Relevant conflicts of interest: Lama Chahine reports no disclosure relevant to the manuscript. Daniel Weintraub is a consultant for Teva and Biotie. Keith Hawkins reports no disclosure relevant to the manuscript. Andrew Siderowf is an employee of Avid Radiopharmaceuticals. Shirley Eberly reports no disclosure relevant to the manuscript. David Oakes reports no disclosure relevant to the manuscript. John Seibyl is a paid consultant for GE Healthcare. He holds an equity interest in Molecular NeuroImaging, LLC. Matthew Stern is a consultant for Adamas, Civitas, Merz, and Teva. Kenneth Marek is a consultant for GE Healthcare and has ownership interest in Molecular NeuroImaging, LLC. Danna Jennings is an employee of Molecular NeuroImaging, LLC.
Financial disclosures: Full financial disclosures and author roles may be found in the online version of this article.
Supporting Data: Additional Supporting Information may be found in the online version of this article at the publisher's web-site.
References
- 1.Fearnley JM, Lees AJ. Ageing and Parkinson's disease: substantia nigra regional selectivity. Brain. 1991;114:2283–2301. doi: 10.1093/brain/114.5.2283. [DOI] [PubMed] [Google Scholar]
- 2.Athauda D, Foltynie T. The ongoing pursuit of neuroprotective therapies in Parkinson disease. Nat Rev Neurol. 2015;11:25–40. doi: 10.1038/nrneurol.2014.226. [DOI] [PubMed] [Google Scholar]
- 3.Siderowf A, Stern MB. Premotor Parkinson's disease: clinical features, detection, and prospects for treatment. Ann Neurol. 2008;64(Suppl 2):S139–S147. doi: 10.1002/ana.21462. [DOI] [PubMed] [Google Scholar]
- 4.Siderowf A, Jennings D, Eberly S, et al. Impaired olfaction and other prodromal features in the Parkinson at-risk syndrome study. Mov Disord. 2012;27:406–412. doi: 10.1002/mds.24892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Abbott RD, Petrovitch H, White LR, et al. Frequency of bowel movements and the future risk of Parkinson's disease. Neurology. 2001;57:456–462. doi: 10.1212/wnl.57.3.456. [DOI] [PubMed] [Google Scholar]
- 6.Shen CC, Tsai SJ, Perng CL, Kuo BI, Yang AC. Risk of Parkinson disease after depression: a nationwide population-based study. Neurology. 2013;81:1538–1544. doi: 10.1212/WNL.0b013e3182a956ad. [DOI] [PubMed] [Google Scholar]
- 7.Ishihara L, Brayne C. A systematic review of depression and mental illness preceding Parkinson's disease. Acta Neurol Scand. 2006;113:211–220. doi: 10.1111/j.1600-0404.2006.00579.x. [DOI] [PubMed] [Google Scholar]
- 8.Iranzo A, Fernandez-Arcos A, Tolosa E, et al. Neurodegenerative disorder risk in idiopathic REM sleep behavior disorder: study in 174 patients. PLoS One. 2014;9:e89741. doi: 10.1371/journal.pone.0089741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Weintraub D, Simuni T, Caspell-Garcia C, et al. Cognitive performance and neuropsychiatric symptoms in early, untreated Parkinson's disease. Mov Disord. 2015;30:919–927. doi: 10.1002/mds.26170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Aarsland D, Bronnick K, Larsen JP, Tysnes OB, Alves G Norwegian ParkWest Study Group. Cognitive impairment in incident, untreated Parkinson disease: The Norwegian ParkWest study. Neurology. 2009;72:1121–1126. doi: 10.1212/01.wnl.0000338632.00552.cb. [DOI] [PubMed] [Google Scholar]
- 11.Massicotte-Marquez J, Decary A, Gagnon J, et al. Executive dysfunction and memory impairment in idiopathic REM sleep behavior disorder. Neurology. 2008;70:1250–1257. doi: 10.1212/01.wnl.0000286943.79593.a6. [DOI] [PubMed] [Google Scholar]
- 12.Jennings D, Siderowf A, Stern M, et al. Imaging prodromal Parkinson disease: the Parkinson associated risk syndrome study. Neurology. 2014;83:1739–1746. doi: 10.1212/WNL.0000000000000960. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Doty RL, Shaman P, Dann M. Development of the University of Pennsylvania smell identification test: a standardized microencapsulated test of olfactory function. Physiol Behav. 1984;32:489–502. doi: 10.1016/0031-9384(84)90269-5. [DOI] [PubMed] [Google Scholar]
- 14.Tanner CM, Ellenberg JH, Mayeux R, Ottoman R, Langston JW. A sensitive and specific screening method for Parkinsons disease. Neurology. 1990;44(4 Suppl. 2):A136. [Google Scholar]
- 15.Comella CL, Nardine TM, Diederich NJ, Stebbins GT. Sleep-related violence, injury, and REM sleep behavior disorder in Parkinson's disease. Neurology. 1998;51:526–529. doi: 10.1212/wnl.51.2.526. [DOI] [PubMed] [Google Scholar]
- 16.Spielberger CD, Gorsuch RL, Lushene PR, Vagg PR, Jacobs AG. Manual for the state-trait anxiety inventory (form Y) Palo Alto, CA: Consulting Psychologists Press, Inc.; 1983. [Google Scholar]
- 17.Knight RG, Waal-Manning HJ, Spears GF. Some norms and reliability data for the state-trait anxiety inventory and the Zung self-rating depression scale. Br J Clin Psychol. 1983;22:245–249. doi: 10.1111/j.2044-8260.1983.tb00610.x. [DOI] [PubMed] [Google Scholar]
- 18.Zich JM, Attkisson CC, Greenfield TK. Screening for depression in primary care clinics: the CES-D and the BDI. Int J Psychiatry Med. 1990;20:259–277. doi: 10.2190/LYKR-7VHP-YJEM-MKM2. [DOI] [PubMed] [Google Scholar]
- 19.Seibyl JP, Marek KL, Quinlan D, et al. Decreased single-photon emission computed tomographic [123I]beta-CIT striatal uptake correlates with symptom severity in Parkinson's disease. Ann Neurol. 1995;38:589–598. doi: 10.1002/ana.410380407. [DOI] [PubMed] [Google Scholar]
- 20.Seibyl JP, Marek K, Sheff K, et al. Iodine-123-beta-CIT and iodine-123-FPCIT SPECT measurement of dopamine transporters in healthy subjects and Parkinson's patients. J Nucl Med. 1998;39:1500–1508. [PubMed] [Google Scholar]
- 21.van Dyck CH, Seibyl JP, Malison RT, et al. Age-related decline in dopamine transporters: analysis of striatal subregions, nonlinear effects, and hemispheric asymmetries. Am J Geriatr Psychiatry. 2002;10:36–43. [PubMed] [Google Scholar]
- 22.Brandt J, Benedict RHB. The Hopkins verbal learning test— revised. Odessa, FL: Psychological Assessment Reources: 2001. [Google Scholar]
- 23.Randolph C. Repeatable battery for the assessment of neuropsychological status. San Antonio: Psychological Corporation; 1998. [Google Scholar]
- 24.Wechsler D. Wechsler memory scale. 3rd. San Antonio, TX: Psychological Corporation; 1997. [Google Scholar]
- 25.Spreen O, Strauss E. A Compendium of Neuropsychological Tests: Administration, Norms and Commentary. 2nd. New York: Oxford University Press; 1998. [Google Scholar]
- 26.Manual of directions and scoring. Washington, DC: War Department, Adjutant General's Office; 1944. Army Individual Test Battery. [Google Scholar]
- 27.Gardner MF, Falkmer T, Vogel K, Gregersen NP. TVPS(UL)-R: Test of Visual-Perceptual Skills (Non motor) (Upper Level) Revised. Hydesville, CA: Psychological and Educational Publications; 1997. [Google Scholar]
- 28.Warrington EK, James M. Visual object and space perception battery (VOSP) Bury St Edmunds, England: Thames Valley Test Co.; 1991. [Google Scholar]
- 29.Kaplan E, Goodglass H, Weintraub S. Boston Naming Test. Philadelphia: Lea & Febiger; 1983. [Google Scholar]
- 30.Hawkins KA, Keefe RS, Christensen BK, et al. Neuropsychological course in the prodrome and first episode of psychosis: Findings from the PRIME North America double blind treatment study. Schizophr Res. 2008;105:1–9. doi: 10.1016/j.schres.2008.07.008. [DOI] [PubMed] [Google Scholar]
- 31.Ross GW, Abbott RD, Petrovitch H, Tanner CM, White LR. Premotor features of Parkinson's disease: the Honolulu-Asia aging study experience. Parkinsonism Relat Disord. 2012;18(Suppl 1):S199–S202. doi: 10.1016/S1353-8020(11)70062-1. [DOI] [PubMed] [Google Scholar]
- 32.Gaenslen A, Wurster I, Brockmann K, et al. Prodromal features for Parkinson's disease: baseline data from the TREND study. Eur J Neurol. 2014;21:766–772. doi: 10.1111/ene.12382. [DOI] [PubMed] [Google Scholar]
- 33.Devanand DP, Michaels-Marston KS, Liu X, et al. Olfactory deficits in patients with mild cognitive impairment predict alzheimer's disease at follow-up. Am J Psychiatry. 2000;157:1399–1405. doi: 10.1176/appi.ajp.157.9.1399. [DOI] [PubMed] [Google Scholar]
- 34.Ponsen MM, Stoffers D, Twisk JW, Wolters EC, Berendse HW. Hyposmia and executive dysfunction as predictors of future Parkinson's disease: a prospective study. Mov Disord. 2009;24:1060–1065. doi: 10.1002/mds.22534. [DOI] [PubMed] [Google Scholar]
- 35.Erixon-Lindroth N, Farde L, Wahlin TB, Sovago J, Halldin C, Backman L. The role of the striatal dopamine transporter in cognitive aging. Psychiatry Res. 2005;138:1–12. doi: 10.1016/j.pscychresns.2004.09.005. [DOI] [PubMed] [Google Scholar]
- 36.Ravina B, Marek K, Eberly S, et al. Dopamine transporter imaging is associated with long-term outcomes in Parkinson's disease. Mov Disord. 2012;27:1392–1397. doi: 10.1002/mds.25157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Li X, Redus L, Chen C, et al. Cognitive dysfunction precedes the onset of motor symptoms in the MitoPark mouse model of Parkinson's disease. PLoS One. 2013;8:e71341. doi: 10.1371/journal.pone.0071341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Trillo L, Das D, Hsieh W, et al. Ascending monoaminergic systems alterations in Alzheimer's disease: translating basic science into clinical care. Neurosci Biobehav Rev. 2013;37:1363–1379. doi: 10.1016/j.neubiorev.2013.05.008. [DOI] [PubMed] [Google Scholar]
- 39.Hilker R, Thomas AV, Klein JC, et al. Dementia in Parkinson disease: functional imaging of cholinergic and dopaminergic pathways. Neurology. 2005;65:1716–1722. doi: 10.1212/01.wnl.0000191154.78131.f6. [DOI] [PubMed] [Google Scholar]
- 40.Bohnen NI, Albin RL. Cholinergic denervation occurs early in Parkinson disease. Neurology. 2009;73:256–257. doi: 10.1212/WNL.0b013e3181b0bd3d. [DOI] [PubMed] [Google Scholar]
- 41.Braak H, Del Tredici K, Rub U, de Vos RA, Jansen Steur EN, Braak E. Staging of brain pathology related to sporadic Parkinson's disease. Neurobiol Aging. 2003;24:197–211. doi: 10.1016/s0197-4580(02)00065-9. [DOI] [PubMed] [Google Scholar]
- 42.Bohnen NI, Muller ML. In vivo neurochemical imaging of olfactory dysfunction in Parkinson's disease. J Neural Transm. 2013;120:571–576. doi: 10.1007/s00702-012-0956-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Burke RE, Dauer WT, Vonsattel JP. A critical evaluation of the Braak staging scheme for Parkinson's disease. Ann Neurol. 2008;64:485–491. doi: 10.1002/ana.21541. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.