

Abstract
In the past 15 years, a major research enterprise has emerged that is aimed at understanding associations between geographic and contextual features of the environment (especially the built environment) and elements of human energy balance, including diet, weight, and physical activity. Here we highlight aspects of this research area with a particular focus on research and opportunities in the United States as an example. We address four main areas: 1) The importance of valid and comparable data concerning behavior across geographies, 2) The ongoing need to identify and explore new environmental variables, 3) The challenge of identifying the causally relevant context, and 4) The pressing need for stronger study designs and analytical methods. Additionally, we discuss existing sources of geo-referenced health data which might be exploited by interdisciplinary research teams, personnel challenges and some aspects of funding for geospatial research by the US National Institutes of Health in the past decade, including funding for international collaboration and training opportunities.
Keywords: spatial, contextual, geospatial, energy balance, physical activity, obesity
1. Introduction
Chronic non-infectious diseases are manifest worldwide and are increasingly replacing infectious diseases as the leading causes of death, albeit with considerable variation among regions of the world (Murray et al. 2012). A major focus of public health research is identifying causes of unhealthy behaviors and then developing approaches to change behaviors by addressing the modifiable subset of these causes. Modifiable risk factors involving energy balance, namely diet, weight, and physical activity, which influence incidence, morbidity and mortality associated with many chronic diseases, are a critical target for research and intervention. Individual behaviors, genetics and physiology continue to be a primary focus of energy balance research due to a long history of behavioral research demonstrating that interventions resulting in weight loss or increases in physical activity can be developed and delivered with positive effects on behavior and health. However, when the intervention ends, participants generally regain the lost weight or return to their sedentary habits (Stevens et al. 2001).
An alternative approach to behavior change and to understanding the causes of unhealthy energy balance, focuses on the environment (Hill and Peters 1998). In this view, environmental rather than genetic changes are posited as responsible for the population-wide epidemic of obesity, and gene-environment interactions act to influence individual susceptibility to overweight, obesity, lower activity levels, or sedentary lifestyles (Ogden et al. 2007). Thus, efforts to promote healthy energy balance should focus on both the environment and on individual approaches, but increased focus on changing environments may be warranted. Support for this idea comes from the substantial heterogeneity in obesity and physical activity levels at a range of scales. For example, Latvians are slimmer than Qataris (https://apps.who.int/infobase/), Coloradans are more active than Californians (http://www.cdc.gov/physicalactivity/downloads/pa_state_indicator_report_2014.pdf), and the residents of Portland, Oregon, are more likely to walk or bicycle to work than those of Philadelphia (http://www.census.gov/prod/2014pubs/acs-25.pdf). Many contrasts such as these can be identified, and the presence of such variation, coupled with the frequent failure of individual-level interventions to produce sustained energy balance-related behavior change (Fjeldsoe et al. 2011), indicate that more research attention should be focused on understanding the environmental and contextual causes of obesity, diet, physical activity, and sedentary time. Of course, determining their relative importance compared to genetic and individual factors remains a research challenge; nevertheless environmental changes that make the healthy choice the easy choice have the potential to have a broad population impact (Hill et al. 2003, Sallis et al. 2008).
Geographic and geospatial perspectives and methods are key elements of the effort to understand environmental and contextual causes of health behaviors related to energy balance. This paper highlights aspects of recent geospatial health research we deem important to strengthening the integration of geospatial and health perspectives on environment and energy balance-related health behaviors. We define the environment broadly in the context of a socioecological model of health (Sallis et al. 2008) to include aspects of the built, policy, social, natural, and economic environments. Health researchers are already using a variety of geospatial tools and approaches to understanding prevention and disease, but the level of sophistication of such use varies enormously and has not sufficiently penetrated the full spectrum of health topics or research designs (Thornton et al. 2011).
This paper was conceived of in the context of a recent workshop (Fostering International Geospatial Health Research Collaborations: Challenges and Opportunities. 16-18 June 2014, held at the Chinese University of Hong Kong) designed to explore and foster international collaboration in geospatial health research. We touch on needs for data harmonization and novel data elements, the challenge of identifying causally relevant environments, the push from public health research for stronger study design related to causal inference, personnel and infrastructure challenges, and a short discussion of recent funding by the US National Institutes for Health in this area. Our examples are largely, but not entirely, from the US. Nevertheless, we hope these ideas and links will be useful to geographers and health scientists using geospatial approaches to design studies with environmental variation in a variety of countries to better understand energy balance and how to improve it.
2. Data Challenges and Promising Data Elements: Examples from the US and Beyond
Comparative studies across diverse geographic regions may contribute to causal inference by increasing the observed range(s) of putative causal factor(s). However, comparative studies depend on the collection of comparable measurements. Height, weight and obesity have standardized objective measures that are applied worldwide, but data standardization is more challenging for diet and physical activity and the environmental variables that might influence them. The World Health Organization and other groups have used standardized survey questions to collect harmonized data concerning activity and sedentary behavior. However, comparative studies of physical activity in the United States versus Sweden using objective measurements give different results than do comparisons based on responses to questionnaires (Hagströmer et al. 2010). Questionnaires likely measure something very different about physical activity than do objective measurement devices, and are highly sensitive to cultural context (Troiano et al. 2014). Thus, great care must be taken to collect harmonized and valid data in comparative and geospatial analyses of energy balance, and cultural differences combined with cognitive challenges may make questionnaire-based comparisons of the frequency and duration of complex behaviors difficult. The use of self-reported data for surveillance and epidemiological studies of physical activity e.g., (Troiano et al. 2008, Atienza et al. 2011) and diet e.g., (Vandevijvere et al. 2013) is coming under increasing scrutiny. Continued efforts to clarify the complementary roles of self-report and objective measurement of environments and behaviors are prominent features of the diet and physical activity research communities. These efforts are likely relevant to diverse aspects of how environment and behavior interact to influence health and well-being. In particular, further development of objective techniques to classify behaviors in specific contexts is warranted.
Just as geospatial researchers likely need collaboration with health researchers to insure they are using the best possible data concerning diet, physical activity and weight, health researchers clearly need collaboration with geospatial and other subject-matter experts to ensure that their comparative and spatial analyses are using the best possible spatial data, theoretical constructs, and analytical methods. The types of georeferenced data currently being applied to the research agenda are diverse. Each data set comes with particular strengths and weaknesses that can be leveraged most effectively through robust collaborations across disciplines. Health researchers do not always appreciate the technical challenges and personnel costs associated with obtaining and developing comparable geographic information systems (GIS) data across sites, even within a single country with relatively ubiquitous and inexpensive data, such as the US. The International Physical Activity and Environment Network (IPEN: http://www.ipenproject.org/) is a recent and important example of efforts to integrate sophisticated GIS-based analyses using the best possible harmonized health data across the globe (Adams et al. 2014). More such efforts are needed, and attention should be given to standardizing environmental and health data. Generally, environmental data that are flexible with respect to geographic scale, updated frequently, and available at no or low costs are desirable in studies on the environment and energy balance, particularly to create standardized measures for comparative studies (see Table 1 for comparisons of some common U.S. data sources). Still, it is important to remember that even when data are free, personnel and expertise are required to match, integrate, clean and analyze data and these costs are easy to underestimate (Lohr 2014).
Table 1.
Common Data Sources for Information on Environmental Conditions in the United States.
| Data Characteristics | |||
|---|---|---|---|
| Data Source | Geographic Scale | Temporal Representation/Scale | Cost to Obtain |
| Census Data | Block group | Rolling 5-year averages | Very Low |
| Metropolitan Planning Organizations/Council of Governments | Mixed | Mixed | Low/High* |
| Geo-referenced Built Environment Data | Flexible | Only when collected | High |
| Archived imagery data (e.g., Google StreetView) | Flexible | Only when collected | Medium |
| Appraisal Data | Flexible | Annual | Low |
Data formatting, cleaning and merging cost can be high
As new or underused data sources are leveraged to increase our understanding of the relationship between environment and energy balance, it is important to properly leverage the work of subject-matter experts in diverse disciplines. For example, a number of recent papers have proposed the use of property appraisal values as a measure of neighborhood characteristics (Moudon et al. 2011, Coffee et al. 2013). This is an interesting path because property appraisal values are available in many countries and updated frequently. Furthermore, they may offer a sensitive indicator of some combination of the relative local value of a home, the land it rests on, and an aggregate measure of environmental characteristics and amenities at a highly flexible geographic scale (Table 1). A promising approach is the use of hedonic price regression models of appraisal or rental data to develop reliable new measures of neighborhood conditions (Drewnowski et al. 2014). Appraisal data should also be viewed as part of a sophisticated geographic information system, for which urban economists have developed a robust understanding (Rosen 1974, Brookshire et al. 1982, Can 1992, Smith and Huang 1995, Irwin 2002, Anderson and West 2006). Careful analytical work is required to identify and extract appropriate measures of environments based on appraisal value, home characteristics, and other potential confounding environmental and individual-level variables. Collaboration between health, geospatial, and economic researchers could accelerate this work. Appraisal data may not be useful in places that lack open markets, or where rates of home sales or renegotiation of rental rates are low.
One particularly valuable feature of property appraisal data is that it could be used to describe environments at various, flexible spatial scales, including, but not limited to, census tracts, counties, and other administrative units. This is important because much of the current literature on neighborhood deprivation and health is based on data from administrative units, making it difficult to explore other definitions of the relevant environment and bringing the Modifiable Areal Unit Problem (see below) to the fore (Chaix et al. 2005). Remotely sensed imagery is another underutilized resource for exploring environmental variables potentially related to energy balance without requiring analysis of administrative units. Although traditionally used for physical sciences, satellite remote sensing has been applied to derive quality of life index assessments, home value estimation, vulnerability assessment, and neighborhood delineation (Stow et al. 2010, Patino and Duque 2013) as well as sidewalks and vegetation indices. Patino and Duque provide a very detailed overview of this area and emphasize that growing public availability of high resolution imagery is creating important new possibilities for integrating remote sensing data into diverse analyses of health and the environment.
3. Defining Causally Relevant (Uncertain) Geographic Contexts
Health researchers have long had a keen interest in neighborhood and contextual effects on health behaviors. Some of this interest can be traced to efforts to understand the health consequences of poverty and neighborhood deprivation. Much work in this area has involved the analysis of administrative units, such as census tracts in the US. Currently, many investigators are interested in better defining the “true causally relevant” geographic area (Diez Roux and Mair 2010). Mei-Po Kwan (2012a, b) has called this the “Uncertain Geographic Context Problem or UGCOP (Kwan 2012a, Kwan 2012b). Like the Modifiable Areal Unit Problem, this issue arises when potential causal relationships are explored using data aggregated into specific areas, such as buffers, administrative units, or neighborhoods, however they are delineated. But the UGCOP arises from a lack of understanding of mechanisms linking environment and behavior, rather than as a consequence of dividing up regions into various geographic areas and then estimating rates or other aggregate measures from events occurring in these regions.
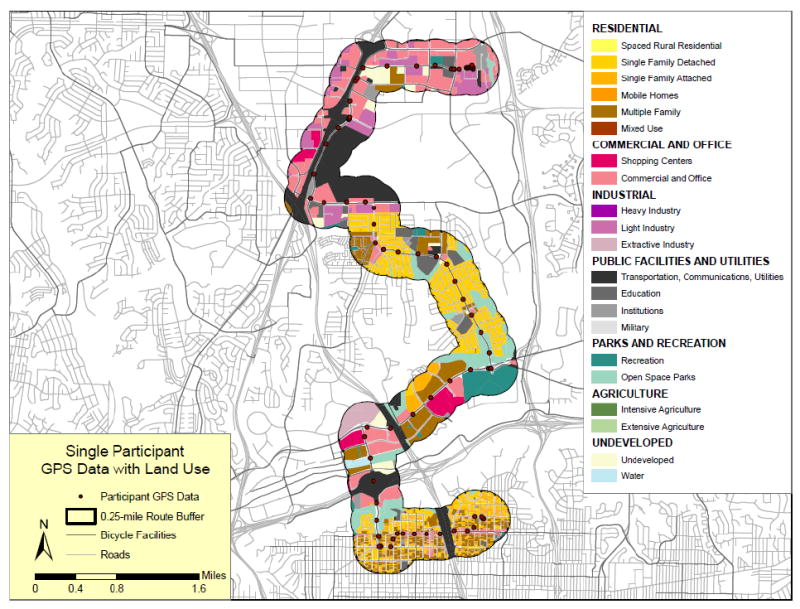
For example, if consumption of fast food is related to exposure to such restaurants, then residence location (a standard focus of studies of the food and physical activity environments) or any specific aggregated area around the residence may be a poor measure of exposure because exposures can occur at other locations in a study subject’s “activity space” (loosely defined as the area in which usual activities occur). Figure 1 of Thornton et al. 2011 nicely illustrates this point (Thornton et al. 2011). Sensitivity analyses examining associations between outcomes and properties of buffers with different shapes and sizes (Figure 1A) are one way to document the UGCOP. Alternatively, examination of actual locations of subjects in time and space using activity space studies (Figure 1B) might provide insight into differential exposures and their consequences (Jankowska et al. 2014). However, model fit, as in Figure 1A, is not a definitive indicator that a better or best “context” has been identified (Spielman and Yoo 2009). Using epidemiological vocabulary, this is because unmeasured covariates or confounders could be responsible for the better fit for a specific buffer size. Stronger experimental or longitudinal study designs are required to address this problem by more clearly identifying causal and policy relevant associations. Additionally, as suggested by Spielman and Yoo (2009), perhaps it is time to forego spatial frames (such as a buffered neighborhood) and move toward “frame-free” analysis. Of course, no study design can ever eliminate the possibility that some unexamined spatial delineation plays a role in determining behavior, but identifying plausible causal relationships can guide policy, even with incomplete understanding of the web of causality.
Fig 1.
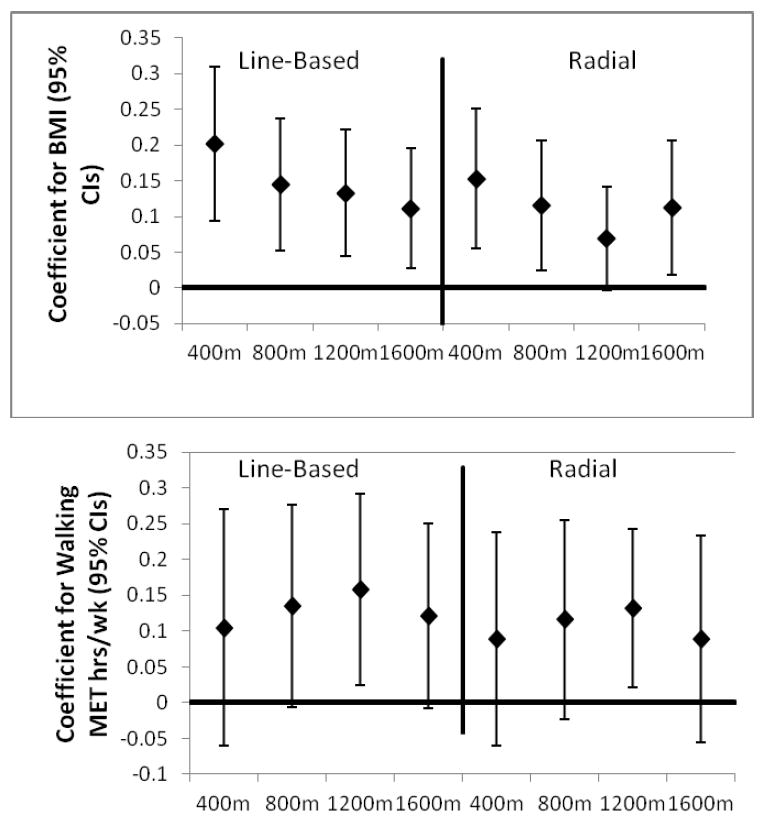
A. Coefficients of the association between Walking/BMI and Intersection Count for line-based and radial buffers of different diameters (James et al. 2014).
B. Portion of the activity space of a person in San Diego and its association with land use mix (Haislip 2011).
Further work concerning geographic contexts is needed, especially to better understand how to define and analyze activity space in large health studies. It is not yet clear whether it is possible to identify buffers or collections of buffers that provide adequate measures of meaningful exposures (Zenk et al. 2011, Chaix et al. 2013). Recently, Boone-Heinonen and Gordon-Larsen (2012) describe lessons learned from diverse analyses of environmental influences on obesity in the Add Health Study, a large prospective cohort of adolescents in the US (Resnick et al. 1997, Boone-Heinonen and Gordon-Larsen 2012). They emphasize both the value of integrating GIS into longitudinal cohort studies and the fact that better delineation of the area that influences diet, PA and obesity is only one of many problems for analyses of energy balance and environment in longitudinal studies. Studies of natural experiments such as changes to the built, transportation or food environment can address some of these problems and indeed are the subject of recent funding opportunities from the US National Institutes of Health (e.g. Program Announcement PA-13-110 Obesity Policy Evaluation Research).
Methodologies developed in space-time analytics to identify causal relationships between environment, diet, weight, and physical activity may also complement epidemiological analyses of cohort data. Health research with a spatial emphasis could benefit from more discussion and focus on the causal mechanisms linking health behaviors and outcomes with the environment and how these mechanisms may be represented or modeled. Careful thinking about the relative contributions of “ambient” exposures, such as policies or neighborhood socioeconomic deprivation, and “concrete” exposures, such as spatially located elements of the built environment to health behaviors and outcomes, could strengthen space- and place-based analyses of health (Spielman and Yoo 2009). Clearly, such “ambient” and “concrete” exposures interact and are collinear, hence the need for thoughtful analyses.
4. Stronger Experimental Designs
Recent commentaries concerning spatial approaches to health issues have emphasized the need for better effect identification, more experiments, and greater effort to obtain both retrospective and prospective place data e.g. (Matthews et al. 2009, Oakes 2013). Some progress has been made on these topics. For example, respondent home addresses from many of the major U.S. health surveys such as Add Health, the California Health Interview Survey (CHIS), the National Health and Nutrition Examination Survey (NHANES), and cohort studies such as the Nurses’ Health Study (NHS), the Multi-Ethnic Study of Atherosclerosis (MESA), the NCI-American Association of Retired Persons (AARP) cohort, the Women’s Health Initiative and the Los Angeles Family and Neighborhood survey (LAFANS) have been geocoded and many geospatial analyses are complete or in progress e.g. (CHIS: Huang et al. 2009, NHANES: Wen and Kowaleski-Jones 2012, NHS: James et al. 2013, MESA: Hirsch et al. 2014, NCI-AARP: Major et al. 2010, WHI: Kerr et al. 2013a). This exciting and important advance reflects the fact that the idea of spatial and contextual approaches has captured the imagination of chronic disease and health behavior researchers. Cohort studies outside the US are also incorporating spatial data layers, especially in Europe and Australia (e.g.(Giles-Corti et al. 2008, Schipperijn et al. 2014)). It could be useful to convene researchers incorporating spatial data in cohort studies to discuss the potential for data pooling to increase power via larger sample sizes and greater environmental variability in the underlying data.
Continued efforts to engage geographers and exploit space-time methods in this work could accelerate progress in clarifying causal relationships between environment and health behaviors as well as strengthen interventions. More detailed measurement of where people spend their time, e.g. via use of global positioning systems GPS, may not achieve the goal of conclusively demonstrating causal associations between environmental variables and health behaviors (Boone-Heinonen and Gordon-Larsen 2012), but greater engagement with geographers could help improve the conceptualization of spatial constructs relevant to health (Thornton et al. 2011, Chaix et al. 2013).
In addition to diverse cross-sectional analyses, more and more longitudinal analyses (Ewing et al. 2006, Powell-Wiley et al. 2014), analyses examining respondents who move (Hirsch et al. 2014, Knuiman et al. 2014), and studies of natural experiments (Fitzhugh et al. 2010) are appearing in the health sector. Such studies can strengthen the case that environmental modifications can lead to changes in health behaviours. Policy change requires more than just evidence that an intervention can result in improved health, among other features, the proposed intervention may receive greater support if it is cost effective. To date, few cost-benefit analyses have been conducted that link changes to the built or policy environment and health (National Institute for Health and Clinical Excellence 2008, McKinnon et al. 2009). More such studies could accelerate progress in addressing the global problem of unhealthy energy balance.
Much more work is also needed to illustrate how geospatial approaches can inform and improve behavioral interventions. For example, building on prior work, (Zenk et al. 2009) Tarlov and Zenk have recently received funding from NIH to examine the extent to which built environment attributes influence response to a weight management program. Specifically, they will examine 200,000 U.S. military veterans who participated in a weight management program and a similar number of matched controls, with the aim of determining the extent to which specific attributes of the residential environment are associated with weight loss at six months and weight loss maintenance at 18 and 60 months. While this study will be able to measure environmental change over time due to actual changes in the environment (e.g., a new supermarket opens near a study participant’s home) as well as moves (e.g., a study participant moves from an environment with a supermarket to one without a supermarket), estimates of the moderating effects of the environment on responses to the intervention might not be fully generalizable in a study of this type, depending on the design, because study participants choose their own neighborhoods.
Nevertheless, if studies of how neighborhoods moderate effects of behavioral interventions are successful in identifying neighborhood features that help or hinder response to weight loss or other interventions, they could lead to improvements in such interventions. For example, investigators could add different elements to help overcome negative environmental effects and target individuals living in communities where the impact of the current intervention was greatest. Recent work suggests that interactions between the environment and response to energy balance may play out in other ways. For example, Kerr et al. (2010) report that individual interventions helped overcome environmental barriers to physical activity (Kerr et al. 2010). Development of a clear taxonomy of how environment and individual interventions might interact for different target behaviors could help guide research in this area. Individual interventions could also include environmental change and employ GPS devices to see if activity locations changed due to improved access or facilities (Kerr et al. 2013a). Other initiatives at the NIH, such as the Mobile Data to Knowledge grants, will include location based prompts where interventions can occur when a participant enters a health risk area, such as a restaurant serving largely unhealthy food or a tobacco outlet.
5. Personnel and Infrastructure Challenges
Research using spatial data to understand health behaviors related to energy balance is growing rapidly; however, the quality of this research is highly variable. Some of this heterogeneity is due to lack of personnel with appropriate training in geospatial thinking across the health research sector. These needs have also been discussed in some detail by geographers and demographers interested in health (Matthews 2012, Matthews and Yang 2013, Shoval et al. 2014). Expertise in geography and geospatial thinking is growing in the health arena, but schools of public health, state and county health departments, cancer research centers, and many NIH Institutes often lack a deep pool of researchers and analysts with geospatial expertise. Thus, more opportunities for collaboration, education, and training are needed to build on existing efforts such as the Communities Putting Prevention to Work program (http://www.cdc.gov/nccdphp/dch/programs/CommunitiesPuttingPreventiontoWork/) and the Active Living Research (ALR) program (Barker and Gutman 2014). The CPPW mission is to “...help large cities, small towns, rural communities, and tribal areas make environmental changes that make healthy living easier.” Similarly, ALR has placed a major emphasis on “communities, active transportation, schools and parks and recreation.” (http://activelivingresearch.org/about).
Achieving the goals of ALR, CPPW and other calls to improve health via contextual and environmental approaches requires incorporation of new data into the analyses of health behaviors and health related interventions. Currently in health research, a great deal of duplication of effort appears to occur in the creation of data layers, confidentiality issues, and analysis of administrative units. Calls to address these problems by creating “…distributed, interoperable spatial data infrastructures…” have been made, but substantial work remains to define this goal and mobilize key health research stakeholders to invest in such infrastructure (Richardson et al. 2013). Useful intermediate goals, such as improving methods for handling confidential health and spatial data and developing protocols for including or linking spatial data and Electronic Health Record (EHR) data may help move the field toward a comprehensive and efficient system for collecting, sorting, and sharing spatial data (Comer et al. 2011, Simpson and Novak 2013).
There is considerable interest throughout the health sector in the potential for better environmental and spatial data to contribute to health. A recent abstract illustrates this interest and the need for more trained personnel to fulfill the promise of geospatial data in health. In the abstract, Pruitt (2014) states that “Duke Medicine has incorporated geospatial information within its EHRs, which add thousands of new ‘big-geo-data’ elements to a patients clinical record.” (Pruitt 2014). It is important to acknowledge the considerable effort that will be required to define, harmonize, and carry out useful research with such a large number of data elements. These data elements are likely obtained from census and other administrative sources and, as discussed above, they may not be the most useful, meaningful, or causally relevant contextual variables. Additionally, adequate infrastructure to help address confidentiality, for example via data enclaves or data centers, is not yet widely available.
Nevertheless, there are some fields where the public health research community has significant expertise in geospatial tools and concepts. Examples include research communities related to cancer mapping, infectious disease and pollution modeling, as well as research related to built environment, transportation, and physical activity. These communities are scattered haphazardly across institutes and institutions and are not yet sufficiently expansive to support the integration of geospatial perspectives in all areas where they could contribute. Similarly, research areas such as regional science have not historically focused on health but have the potential to make significant conceptual contributions to understanding how national or global processes influence health (http://www.regionalscience.org/). Thus, further challenges include how to coordinate existing expertise, establish best practices, and increase communication across disciplines. The Robert Wood Johnson Foundation’s Active Living Research program provides an example of the level of effort required to create a community of researchers focused on environmental influences on physical activity that has resulted in growing public health sector expertise in geospatial analyses (Barker and Gutman 2014).
6. US National Institutes of Health Funding, Including International Projects and Training
In the past decade, the NIH has funded considerable research on geospatial approaches to energy balance. Examples of these grants are listed in Table 2. Some of these grants were submitted in response to calls for proposals related to spatial uncertainty, obesity policy research, and geographic and contextual influences on energy balance-related health behaviors; others were investigator-initiated submissions. Additional grants have been funded through unsolicited submission, conference grant mechanisms, and special initiatives such as the NCI Provocative Questions initiative (http://provocativequestions.nci.nih.gov/). A general introduction to NIH grants is available (http://grants.nih.gov/grants).
Table 2.
Examples of recent grants concerning geospatial and contextual analyses of energy balance from the United States National Institutes of Health.
| Grant Title | Investigator | Years/Total Funding Requested* | Institute |
|---|---|---|---|
| Environmental Attributes and Weight Control: Study of Over 1.3 Million Veterans | Zenk, S; Tarlov, E. | 4/$2,400,000 | NCI |
| Community Influences on NHANES Diet and Physical Activity | Scribner, R | 3/$750,000 | NCI |
| Effects of the Built Environment, Crime & Food Prices on BMI, Activity & Eating | Colabianchi, N | 3/$1,080,000 | NCI |
| Neighborhood Built and Social Environment and Physical Activity and Weight Status | Wen, M | 5/$1,250,000 | NCI |
| Obesogenic Environment: Impact on Breast, Colorectal and Prostate Cancer Risk | Cheng, I | 4/$1,370,000 | NCI |
| New Statistical Methods To Handle Spatial Uncertainty In Cancer Risk Estimation | Guan, Y | 4/$1,340,000 | NCI |
| Uncertainty In Spatial Health Analysis Due To Missingness And Aggregation Effects | Lawson, AB. | 3/$890,000 | NCI |
| IPEN: International Study Of Built Environment, Physical Activity, And Obesity | Sallis, J | 4/$2,140,000 | NCI |
| Structural & Programmatic Effects Of Bus Rapid Transit On Physical Activity | Saelens BE | 5/$2,200,000 | NCI |
| GPS Exposure To Environments & Relations With Biomarkers Of Cancer Risk | Kerr, J | 4/$2,980,000 | NCI |
| Economic Contextual Influences on Population Diet and Obesity | Powell, LM | 3/$1,180,000 | NHLBI |
| Longitudinal Associations of Neighborhood Environment with Obesity and Health | Babey, S | 5/$3,000,000 | NHLBI |
| Validating GIS-Based Methods To Address Spatial Uncertainty In Clinical Trials | Clougherty, J. | 5/$1,860,000 | NHLBI |
| Impacts of School Policies on Student Diet & Activity Behaviors & Obesity | Nanney, MS | 5/$2,190,000 | NHLBI |
| Physical Activity and Nutrition Intervention in Afterschool Programs | Beets, MW | 5/$2,770,00 | NHLBI |
| Environments Impact On Children’s Diet, Activity & Obesity: A Natural Experiment | Datar, A | 5/$3,950,000 | NICHD |
| Bayesian Integration Of Biomarkers And Spatial Exposure Data | Bartell, SM | 2/$387,000 | NIEHS |
| Statistical Methods For Exposure Uncertainty In Air Pollution And Health Studies | Chang, H | 2/$442,000 | NIEHS |
| Walkability’s Impact on Senior Health | Glicksman, A | 2/$315,000 | NINR |
| Geospatial Frontiers In Health And Social Environments | Richardson, D | 2/98,000 | OBBSR |
Abstracts of these and other grants can be searched for and accessed via the NIH Reporter (http://projectreporter.nih.gov/reporter.cfm).
Actual funding levels somewhat lower
A number of features of the NIH funding system are worth noting in the context of fostering further research on spatial and contextual aspects of health, especially in an international context. First, because geospatial activities cut across multiple institutes at the NIH, it can be difficult to track funding activities and opportunities in this area. Personal contact with an NIH Program Officer is very helpful for prospective grantees. Specific grants, grant abstracts, funding Institutes and other details, including the name of the Program Officer, can be accessed through the NIH RePORTER (http://projectreporter.nih.gov/reporter.cfm). This system facilitates identifying Program Officers who have handled grants on similar topics.
Second, a potentially salient model for US funding of international research concerning spatial and environmental influences on energy balance is IPEN, which has received funding from NIH’s National Cancer Institute and National Heart, Lung, and Blood Institute. The IPEN team has effectively argued that causal inference concerning associations between built environment and physical activity could be strengthened by a research program emphasizing the use of common measures across more diverse built and cultural environments than are available in any one country (Kerr et al. 2013b, Van Dyck et al. 2014). Third, NIH funding spans a continuum (Table 2), ranging from studies of exposures related to regional or national policies (e.g., Nanney, Datar) to diverse studies addressing potential effects of exposures associated with specific geographic units or locations (e.g., Wen) as well as specific spatially located features of the environment (e.g., Saelens). This continuum is related to the idea of place versus space in geographic thinking, to the distinction between “ambient” and “concrete” exposures in analyses of context and energy balance, and to study designs focusing on people in multiple spaces versus those tracking individuals across spaces. Health research could benefit from further discussion addressing exposure in the context of these ideas (Chaix et al. 2013).
Opportunities exist for international researchers through collaboration with US-based investigators, investigator-initiated grants from overseas and diverse training programs. Many of these activities are organized by NIH’s Fogarty International Center (http://www.fic.nih.gov/). The recently established National Cancer Institute’s Center for Global Health (http://www.cancer.gov/aboutnci/organization/global-health) also offers a variety of research and training opportunities emphasizing cancer control and training for investigators from low- to middle-income countries. This short introduction to US NIH funding highlights the need for a more overarching international exchange concerning research questions, funding opportunities and paths to international collaboration in this research area.
7. Conclusion
At its heart, public health research is an applied science, with social justice through health and healthy environments as one of its key goals (McKinnon et al. 2012, Lee et al. 2012). Currently, Fogarty International Center describes its vision as “a world in which the frontiers of health research extend across the globe and advances in science are implemented to reduce the burden of disease, promote health, and extend longevity for all people.” (http://www.fic.nih.gov/). Strengthening international geospatial health research is a logical element of such a vision, and given the negative trends in diet, weight, and physical activity across the globe, a focus on energy balance appears timely. Comparative studies can strengthen causal inference (Kerr et al. 2013b) and transdisciplinary teams can improve scientific productivity (Hall et al. 2012). Of course, it is hoped that fostering international collaboration will accelerate scientific discovery, but it remains to be seen whether this will occur. This paper has emphasized the need for conceptual clarity, valid and harmonized data, and better study designs in order to better understand causal pathways and to improve evaluation of interventions. These factors are always desirable in health research, but geospatial research on energy balance is ripe for progress on all of these fronts. Continued international collaboration between health and geospatial researchers should help accelerate this progress.
Acknowledgments
We thank the organizers of the Forum where this work was originally presented, Anne Rodgers for editorial assistance, and Penny Randall-Levy for formatting the bibliography. Funding for Dr. Powell-Wiley is provided by the Division of Intramural Research of the National Institutes of Health. This work was also supported by the NCI Centers for Transdisciplinary Research on Energetics and Cancer (TREC) (U54 CA155626, U54 CA155435, U54 CA155850, U54 CA155796, U54 CA116850).
Reference List
- 1.Adams MA, et al. International variation in neighborhood walkability, transit, and recreation environments using geographic information systems: the IPEN adult study. International Journal of Health Geographics. 2014;13(1):43. doi: 10.1186/1476-072X-13-43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Anderson ST, West SE. Open space, residential property values, and spatial context. Regional Science and Urban Economics. 2006;36(6):773–789. [Google Scholar]
- 3.Atienza AA, et al. Self-reported and objectively measured activity related to biomarkers using NHANES. Medicine and Science in Sports and Exercise. 2011;43(5):815–821. doi: 10.1249/MSS.0b013e3181fdfc32. [DOI] [PubMed] [Google Scholar]
- 4.Barker DC, Gutman MA. Evaluation of active living research: ten years of progress in building a new field. American Journal of Preventive Medicine. 2014;46(2):208–215. doi: 10.1016/j.amepre.2013.10.003. [DOI] [PubMed] [Google Scholar]
- 5.Boone-Heinonen J, Gordon-Larsen P. Obesogenic environments in youth: concepts and methods from a longitudinal national sample. American Journal of Preventive Medicine. 2012;42(5):e37–e46. doi: 10.1016/j.amepre.2012.02.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Brookshire DS, et al. Valuing public goods: a comparison of survey and hedonic approaches. American Economic Review. 1982;72(1):165–177. [Google Scholar]
- 7.Can A. Specification and estimation of hedonic housing price models. Regional Science and Urban Economics. 1992;22(3):453–474. [Google Scholar]
- 8.Chaix B, et al. GPS tracking in neighborhood and health studies: a step forward for environmental exposure assessment, a step backward for causal inference? Health & Place. 2013;21:46–51. doi: 10.1016/j.healthplace.2013.01.003. [DOI] [PubMed] [Google Scholar]
- 9.Chaix B, Merlo J, Chauvin P. Comparison of a spatial approach with the multilevel approach for investigating place effects on health: the example of healthcare utilisation in France. Journal of Epidemiology and Community Health. 2005;59(6):517–526. doi: 10.1136/jech.2004.025478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Coffee NT, et al. Relative residential property value as a socio-economic status indicator for health research. International Journal of Health Geographics. 2013;12:22. doi: 10.1186/1476-072X-12-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Comer KF, et al. Incorporating geospatial capacity within clinical data systems to address social determinants of health. Public Health Reports. 2011;126(Suppl 3):54–61. doi: 10.1177/00333549111260S310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Diez Roux AV, Mair C. Neighborhoods and health. Annals of the New York Academy of Sciences. 2010;1186:125–145. doi: 10.1111/j.1749-6632.2009.05333.x. [DOI] [PubMed] [Google Scholar]
- 13.Drewnowski A, et al. Environments perceived as obesogenic have lower residential property values. American Journal of Preventive Medicine. 2014;47(3):260–274. doi: 10.1016/j.amepre.2014.05.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ewing R, Brownson RC, Berrigan D. Relationship between urban sprawl and weight of United States youth. American Journal of Preventive Medicine. 2006;31(6):464–474. doi: 10.1016/j.amepre.2006.08.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Fitzhugh EC, Bassett DR, Jr, Evans MF. Urban trails and physical activity: a natural experiment. American Journal of Preventive Medicine. 2010;39(3):259–262. doi: 10.1016/j.amepre.2010.05.010. [DOI] [PubMed] [Google Scholar]
- 16.Fjeldsoe B, et al. Systematic review of maintenance of behavior change following physical activity and dietary interventions. Health Psychology. 2011;30(1):99–109. doi: 10.1037/a0021974. [DOI] [PubMed] [Google Scholar]
- 17.Giles-Corti B, et al. Evaluation of the implementation of a state government community design policy aimed at increasing local walking: design issues and baseline results from RESIDE, Perth Western Australia. Preventive Medicine. 2008;46(1):46–54. doi: 10.1016/j.ypmed.2007.08.002. [DOI] [PubMed] [Google Scholar]
- 18.Hagströmer M, et al. Levels and patterns of objectively assessed physical activity--a comparison between Sweden and the United States. American Journal of Epidemiology. 2010;171(10):1055–1064. doi: 10.1093/aje/kwq069. [DOI] [PubMed] [Google Scholar]
- 19.Haislip LD. Thesis. San Diego State University School of Public Affairs; 2011. [September 2, 2014]. An examination of utilitarian bicycle trip route choice preference in San Diego. Available from http://libpac.sdsu.edu/search/X?laura+haislip. [Google Scholar]
- 20.Hall KL, et al. Assessing the value of team science: a study comparing center- and investigator-initiated grants. American Journal of Preventive Medicine. 2012;42(2):157–163. doi: 10.1016/j.amepre.2011.10.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hill JO, Peters JC. Environmental contributions to the obesity epidemic. Science. 1998;280(5368):1371–1374. doi: 10.1126/science.280.5368.1371. [DOI] [PubMed] [Google Scholar]
- 22.Hill JO, et al. Obesity and the environment: where do we go from here? Science. 2003;299(5608):853–855. doi: 10.1126/science.1079857. [DOI] [PubMed] [Google Scholar]
- 23.Hirsch JA, et al. Change in walking and body mass index following residential relocation: the multi-ethnic study of atherosclerosis. American Journal of Public Health. 2014;104(3):e49–e56. doi: 10.2105/AJPH.2013.301773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Huang L, et al. Identifying clusters of active transportation using spatial scan statistics. American Journal of Preventive Medicine. 2009;37(2):157–166. doi: 10.1016/j.amepre.2009.04.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Irwin EG. The effects of open space on residential property values. Land Economics. 2002;78(4):465–480. [Google Scholar]
- 26.James P, et al. Effects of buffer size and shape on associations between the built environment and energy balance. Health & Place. 2014;27:162–170. doi: 10.1016/j.healthplace.2014.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.James P, et al. Urban sprawl, physical activity, and body mass index: Nurses’ Health Study and Nurses’ Health Study II. American Journal of Public Health. 2013;103(2):369–375. doi: 10.2105/AJPH.2011.300449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Jankowska MM, Schipperijn J, Kerr J. A framework for using GPS data in physical activity and sedentary behavior studies. Exercise and Sport Sciences Review. 2014 doi: 10.1249/JES.0000000000000035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kerr J, et al. Neighborhood environment and physical activity among older women: findings from the San Diego Cohort of the Women’s Health Initiative. Journal of Physical Activity & Health. 2013a;11(6):1070–1077. doi: 10.1123/jpah.2012-0159. [DOI] [PubMed] [Google Scholar]
- 30.Kerr J, et al. Do neighborhood environments moderate the effect of physical activity lifestyle interventions in adults? Health & Place. 2010;16(5):903–908. doi: 10.1016/j.healthplace.2010.05.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kerr J, et al. Advancing science and policy through a coordinated international study of physical activity and built environments: IPEN adult methods. Journal of Physical Activity & Health. 2013b;10(4):581–601. doi: 10.1123/jpah.10.4.581. [DOI] [PubMed] [Google Scholar]
- 32.Knuiman MW, et al. A longitudinal analysis of the influence of the neighborhood built environment on walking for transportation: the RESIDE Study. American Journal of Epidemiology. 2014;180(5):453–461. doi: 10.1093/aje/kwu171. [DOI] [PubMed] [Google Scholar]
- 33.Kwan MP. How GIS can help address the uncertain geographic context problem in social science research. Annals of GIS. 2012a;18(4):245–255. [Google Scholar]
- 34.Kwan MP. The uncertain geographic context problem. Annals of the Association of American Geographers. 2012b;102(5):958–968. [Google Scholar]
- 35.Lee IM, et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012;380(9838):219–229. doi: 10.1016/S0140-6736(12)61031-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Lohr S. For big-data scientists, ‘janitor work’ is key hurdle to insights. [December 15, 2014];The New York Times. 2014 Available from http://www.nytimes.com/2014/08/18/technology/for-big-data-scientists-hurdle-to-insights-is-janitor-work.html?_r=0.
- 37.Major JM, et al. Neighborhood socioeconomic deprivation and mortality: NIH-AARP diet and health study. PLoS One. 2010;5(11):e15538. doi: 10.1371/journal.pone.0015538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Matthews SA. Thinking about place, spatial behavior, and spatial processes in childhood obesity. American Journal of Preventive Medicine. 2012;42(5):516–520. doi: 10.1016/j.amepre.2012.02.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Matthews SA, Moudon AV, Daniel M. Work group II: Using Geographic Information Systems for enhancing research relevant to policy on diet, physical activity, and weight. American Journal of Preventive Medicine. 2009;36(4 Suppl):S171–S176. doi: 10.1016/j.amepre.2009.01.011. [DOI] [PubMed] [Google Scholar]
- 40.Matthews SA, Yang TC. Spatial polygamy and contextual exposures (SPACEs): promoting activity space approaches in research on place and health. American Behavioral Scientist. 2013;57(8):1057–1081. doi: 10.1177/0002764213487345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.McKinnon RA, et al. Considerations for an obesity policy research agenda. American Journal of Preventive Medicine. 2009;36(4):351–357. doi: 10.1016/j.amepre.2008.11.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.McKinnon RA, et al. The National Collaborative on Childhood Obesity Research catalogue of surveillance systems and measures registry: new tools to spur innovation and increase productivity in childhood obesity research. American Journal of Preventive Medicine. 2012;42(4):433–435. doi: 10.1016/j.amepre.2012.01.004. [DOI] [PubMed] [Google Scholar]
- 43.Moudon AV, et al. A neighborhood wealth metric for use in health studies. American Journal of Preventive Medicine. 2011;41(1):88–97. doi: 10.1016/j.amepre.2011.03.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Murray CJ, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2197–2223. doi: 10.1016/S0140-6736(12)61689-4. [DOI] [PubMed] [Google Scholar]
- 45.National Institute for Health and Clinical Excellence. Physical activity and the environment. Costing report: implementing NICE guidance. [September 4, 2014];2008 National Institute for Health and Clinical Excellence. Available from www.nice.org.uk/guidance/ph8/resources/physical-activity-and-the-environment-cost-report2.
- 46.Oakes JM. Invited commentary: Paths and pathologies of social epidemiology. American Journal of Epidemiology. 2013;178(6):850–851. doi: 10.1093/aje/kwt144. [DOI] [PubMed] [Google Scholar]
- 47.Ogden CL, et al. The epidemiology of obesity. Gastroenterology. 2007;132(6):2087–2102. doi: 10.1053/j.gastro.2007.03.052. [DOI] [PubMed] [Google Scholar]
- 48.Patino JE, Duque JC. A review of regional science applications of satellite remote sensing in urban settings. Computers, Environment and Urban Systems. 2013;37:1–17. [Google Scholar]
- 49.Powell-Wiley TM, et al. Neighborhood-level socioeconomic deprivation predicts weight gain in a multi-ethnic population: Longitudinal data from the Dallas Heart Study. Preventive Medicine. 2014;66:22–27. doi: 10.1016/j.ypmed.2014.05.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Pruitt S. Big-GEO-data EHR infrastructure development for on-demand analytics. Healthcare Analytics Symposium; July 14-16, 2014; Chicago, IL. HealthData Management; 2014. [September 2, 2014]. Available from http://www.healthdatamanagement.com/conferences/1_5/big-geo-data-ehr-infrastructure-development-for-on-demand-analytics-47627-1.html. [Google Scholar]
- 51.Resnick MD, et al. Protecting adolescents from harm. Findings from the National Longitudinal Study on Adolescent Health. Journal of the American Medical Association. 1997;278(10):823–832. doi: 10.1001/jama.278.10.823. [DOI] [PubMed] [Google Scholar]
- 52.Richardson DB, et al. Medicine. Spatial turn in health research. Science. 2013;339(6126):1390–1392. doi: 10.1126/science.1232257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Rosen S. Hedonic prices and implicit markets: product differentiation in pure competition. Journal of Political Economy. 1974;82(1):34–55. [Google Scholar]
- 54.Sallis JF, Owen N, Fisher EB. Ecological models of health behavior. In: Glanz K, Rimer BK, Viswanath K, editors. Health behavior and health education: theory, research, and practice. 4. San Francisco: Jossey-Bass; 2008. pp. 465–486. [Google Scholar]
- 55.Schipperijn J, et al. A longitudinal study of objectively measured built environment as determinant of physical activity in young adults - the European Youth Heart Study. Journal of Physical Activity & Health. 2014 doi: 10.1123/jpah.2014-0039. [DOI] [PubMed] [Google Scholar]
- 56.Shoval N, et al. The shoemaker’s son always goes barefoot: implementations of GPS and other tracking technologies for geographic research. Geoforum. 2014;51:1–5. [Google Scholar]
- 57.Simpson CL, Novak LL. Place matters: the problems and possibilities of spatial data in electronic health records. AMIA Annual Symposium Proceedings; 2013. pp. 1303–1311. [PMC free article] [PubMed] [Google Scholar]
- 58.Smith VK, Huang JC. Can markets value air quality? A meta-analysis of hedonic property value models. Journal of Political Economy. 1995;103(1):209–227. [Google Scholar]
- 59.Spielman SE, Yoo EH. The spatial dimensions of neighborhood effects. Social Science & Medicine. 2009;68(6):1098–1105. doi: 10.1016/j.socscimed.2008.12.048. [DOI] [PubMed] [Google Scholar]
- 60.Stevens VJ, et al. Long-term weight loss and changes in blood pressure: results of the Trials of Hypertension Prevention, phase II. Annals of Internal Medicine. 2001;134(1):1–11. doi: 10.7326/0003-4819-134-1-200101020-00007. [DOI] [PubMed] [Google Scholar]
- 61.Stow DA, Lippitt CD, Weeks JR. Geographic object-based delineation of neighborhoods of Accra, Ghana using QuickBird satellite imagery. Photogrammetric Engineering & Remote Sensing. 2010;76(8):907–914. doi: 10.14358/pers.76.8.907. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Thornton LE, Pearce JR, Kavanagh AM. Using Geographic Information Systems (GIS) to assess the role of the built environment in influencing obesity: a glossary. International Journal of Behavioral Nutrition and Physical Activity. 2011;8:71. doi: 10.1186/1479-5868-8-71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Troiano RP, et al. Physical activity in the United States measured by accelerometer. Medicine and Science in Sports and Exercise. 2008;40(1):181–188. doi: 10.1249/mss.0b013e31815a51b3. [DOI] [PubMed] [Google Scholar]
- 64.Troiano RP, et al. Evolution of accelerometer methods for physical activity research. British Journal of Sports Medicine. 2014;48(13):1019–1023. doi: 10.1136/bjsports-2014-093546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Van Dyck D, et al. International study of objectively measured physical activity and sedentary time with body mass index and obesity: IPEN adult study. International Journal of Obesity (London) 2014 doi: 10.1038/ijo.2014.115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Vandevijvere S, et al. Monitoring and benchmarking population diet quality globally: a stepwise approach. Obesity Reviews. 2013;14(Suppl 1):135–149. doi: 10.1111/obr.12082. [DOI] [PubMed] [Google Scholar]
- 67.Wen M, Kowaleski-Jones L. The built environment and risk of obesity in the United States: racial-ethnic disparities. Health & Place. 2012;18(6):1314–1322. doi: 10.1016/j.healthplace.2012.09.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Zenk SN, et al. Activity space environment and dietary and physical activity behaviors: a pilot study. Health & Place. 2011;17(5):1150–1161. doi: 10.1016/j.healthplace.2011.05.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Zenk SN, et al. Neighborhood environment and adherence to a walking intervention in African American women. Health Education & Behavior. 2009;36(1):167–181. doi: 10.1177/1090198108321249. [DOI] [PMC free article] [PubMed] [Google Scholar]