

Abstract
Purpose of review:
Neurologic symptoms due to a psychogenic cause are frequently seen in clinical practice. Psychogenic nonepileptic seizures (PNES) and psychogenic movement disorders (PMD) are among the most common psychogenic neurologic disorders. PNES and PMD are usually investigated and managed separately by different neurology subspecialists. We review the main epidemiologic and clinical features of both PNES and PMD, aiming to highlight their similarities and differences and to see whether a common framework for these disorders exists.
Recent findings:
Data from the literature show that there is a profound overlap between PNES and PMD, which would argue for a larger unifying pathophysiology with variable phenotypic manifestations.
Summary:
Collaborative and integrated research among epileptologists, movement disorders experts, psychiatrists, psychologists, and physiotherapists may increase our collective knowledge about the pathophysiologic mechanisms of PNES and PMD and therefore improve outcomes for these patients.
Neurologic symptoms due to a functional or psychogenic cause are common in clinical practice, accounting for up to 16% of patients presenting to neurology outpatient clinics, depending on the clinical definitions and methodology used for case ascertainment.1,2 The yearly costs of patients with medically unexplained symptoms in the United States have been estimated at approximately $256 billion per year.3 Despite their prevalence and associated economic and social burden, appropriate treatments for these disorders are an unmet need. This may reflect the absence of research interest and lack of discourse between neurology and psychiatry regarding these patients. Notably, although approximately 50% of the patients with somatoform disorders are identified by neurologists at the time of first contact, only 1.5% are referred to a psychiatrist or a psychologist.4
Psychogenic nonepileptic seizures (PNES) and psychogenic movement disorders (PMD) are usually investigated and managed separately by different neurology specialists, so studies directly comparing these disorders are scarce. The few studies that directly compared patients with PNES and PMD found that the clinical similarities between these 2 conditions far exceeded their differences.5–7 If PNES and PMD are part of the same clinical spectrum instead of separate entities,8,9 this may provide an ideal disease model for partnership among subspecialties to improve our knowledge and enhance our diagnostic and therapeutic strategies in these disorders. In this review, we compare the clinical and associated features of PNES and PMD, highlighting their similarities and differences, in order to see whether a common framework between these disorders may exist.
Search strategy
We searched MEDLINE with the search terms PNES, psychogenic nonepileptic seizures, pseudoseizures, hysteria, psychogenic movement disorder, functional movement disorder, and nonorganic movement disorder. The list of articles finally included in this review was created according to the aims stated above. The reference lists of relevant articles were also reviewed for important articles not found in the original search.
Definition and terminology
The lack of knowledge about the pathophysiology of these disorders is reflected in the way we describe them (for instance, medically unexplained symptoms), with the implication that diagnosis mainly relies on the exclusion of their organic counterparts rather than on positive signs of a disease process. Accordingly, PNES are defined as paroxysmal episodes clinically resembling an epileptic seizure, but that are not caused by ictal epileptiform activity.10 Similarly, PMD are defined as the occurrence of abnormal movements that do not result from a known general medical or neurologic cause.11 This ambiguity also explains the different terminology that has been used to refer to these disorders (psychogenic nonepileptic seizures, pseudoseizures, hysteria, functional movement disorder, nonorganic movement disorder). Most of such terms imply a presumed causal relation between psychological factors and the generation of either PNES or PMD.12 However, the definition of these disorders with regard to a proposed etiology (i.e., psychological stress/trauma) has been challenged by current evidence.12
As outlined in the following section, the term psychogenic is not widely used by psychiatrists and is in fact not found in the current DSM-5.13 Use of the alternative term functional (at least as far as movement disorders are concerned) has been recently supported11,14; this change in terminology has been included in DSM-5 with regard to conversion disorder (functional neurologic symptom disorder), given that relevant psychological factors may not be demonstrable at the time of diagnosis,13 and also provisionally proposed in the beta draft of the ICD-11.15
An ongoing debate has been similarly raised on the most appropriate name for PNES. It has become clear that some labels that have been used in clinical practice and medical literature, including hysterical seizures and pseudoseizures, offend patients.16 It is also debatable which between the terms attack or seizure is most suitable and better accepted by patients. One linguistic study of 13 PNES patients suggested that they judged both terms as problematic.17 Yet the question regarding the use of the term functional in PNES has not been specifically raised. We would favor the use of the term functional (also with regard to nonepileptic seizures), but we acknowledge that there remain arguments on both sides for the terminology used in research and clinical practice.18,19 However, for the sake of homogeneity and to avoid confusion, in this review we consistently use the terms PNES and PMD, given their wide use in the medical literature.
Diagnostic criteria and categories of diagnostic certainty
The neurologists' perspective
Internationally accepted diagnostic criteria for PNES do not exist. The definitions adopted in the literature vary widely, although they share several aspects. These include the following: (1) an observable abrupt, usually time-limited paroxysmal change in behavior or consciousness resembling an epileptic seizure; (2) absence of electrophysiologic changes that accompany an epileptic seizure (i.e., the absence of ictal or postictal EEG changes); (3) no evidence for other organic causes that might explain the episodes; and (4) evidence or strong suspicion for psychogenic processes as causative factors.20
Based on these features, the International League Against Epilepsy proposed a staged approach for the diagnosis of PNES,21 with the absence of ictal changes on video-EEG recording being the gold standard for diagnosis. Provocative procedures including saline provocation, hypnosis, suggestions, or a combination of them also have been used to induce an attack and demonstrate diagnosis, but ethical concerns have been raised and the use of such provocative procedures therefore has been generally discouraged.21
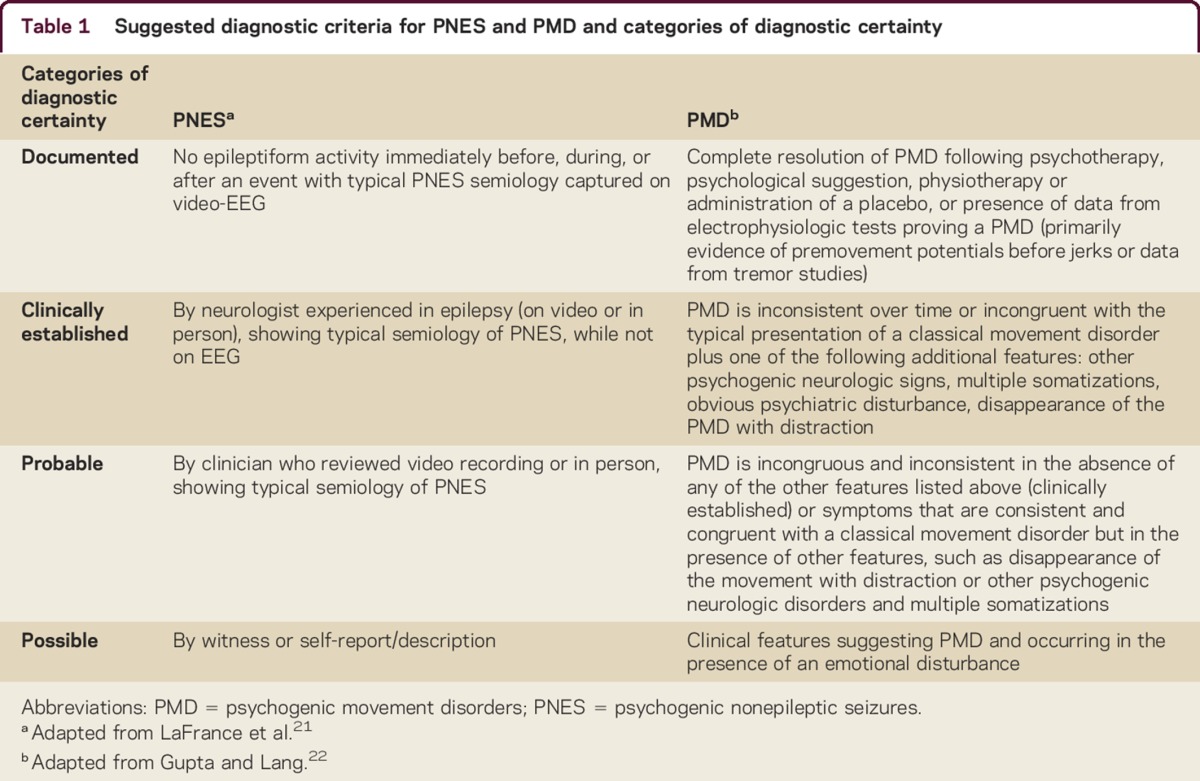
Similarly, diagnostic criteria for documented PMD require the presence of motor symptoms, which are inconsistent over time, incongruent with the typical features of an organic movement disorder, and consistently and persistently relieved by psychotherapy, suggestion, or placebo.22 Coexisting psychological factors or psychiatric disorders are considered supportive (but not necessary) features for the diagnosis. Recently, laboratory-supported criteria for the diagnosis of PMD, at least as far as tremor and myoclonus are concerned, have been proposed, yet not validated.22–24 As such, in most cases the diagnosis of PMD relies on clinical features. Table 1 provides the suggested criteria for the diagnosis of PNES and PMD.
Table 1.
Suggested diagnostic criteria for PNES and PMD and categories of diagnostic certainty
The psychiatrists' perspective
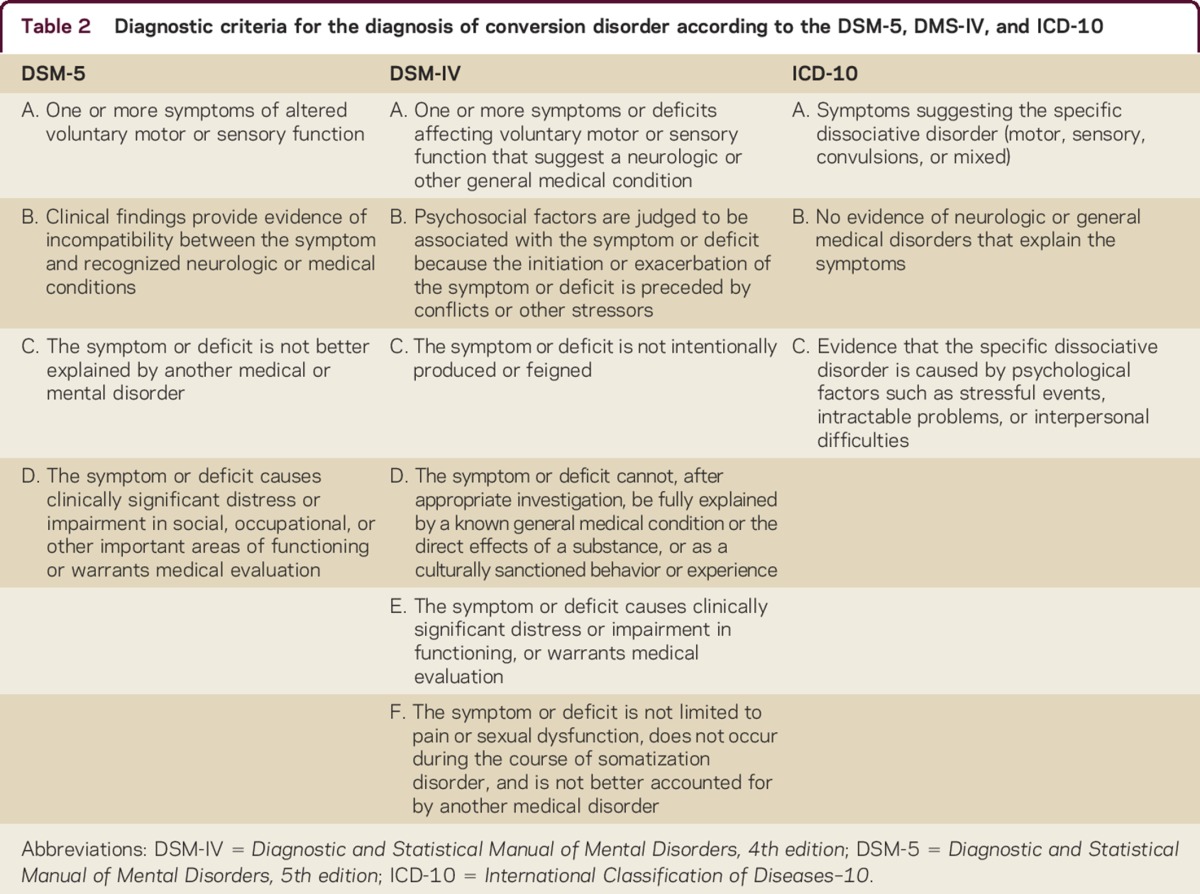
As mentioned before, the term psychogenic has little utility for psychiatrists, who (1) would likely not differentiate between patients with PNES and PMD and (2) for some of these patients would instead diagnose conversion disorder (CD). However, not all these patients fulfill the criteria for CD. As an example, one study found that approximately 11% in their series of patients with fixed dystonia (which—from a neurologic perspective—is thought to be psychogenic in the majority of cases) fulfilled the DSM-IV criteria for CD.25 This finding was due to the fact that in most of the cases there were no evident psychological features that could explain the symptoms.25 Even among psychiatrists, there has been a longstanding debate on what CD represents and how it should be classified. In fact, CD has been classified as a dissociative disorder according to ICD-10 and as a somatoform disorder according to DSM-5. Some authors have argued that dissociative processes seem to underlie PNES, which can be reversed using appropriate hypnotic suggestions.26 Moreover, as in other dissociative disorders, physical or sexual abuse and other traumatizing events are common among individuals with PNES.27 In this view, symptoms and signs are strictly consequential to a (psychological) trauma, there being often a detachment from reality with or without alterations in personal identity or sense of self. However, other researchers have emphasized the overlap between psychogenic neurologic symptoms and anxiety rather than dissociation,28 supporting the hypothesis that they could represent somatizations. In such cases, symptoms are either very distressing or result in significant disruption of functioning, and there are disproportionate thoughts, feelings, and behaviors regarding those symptoms. The diagnosis is therefore not based on medically unexplained symptoms, but on the reporting of bothersome and persistent somatic symptoms accompanied by an excessive psychological response. This shift has been made recently in the current edition of the DSM-5, where the criteria for CD (functional neurologic symptom disorder) emphasize the crucial importance of the neurologic examination and downgrade the presence of (causative) psychological factors to a supportive but not essential criterion (table 2).13 A similar approach also has been proposed recently in the beta draft of ICD-11, where “Functional disorders of the nervous system” is listed among neurologic diseases rather than among psychiatric ones.15
Table 2.
Diagnostic criteria for the diagnosis of conversion disorder according to the DSM-5, DMS-IV, and ICD-10
Such a remarkable shift might render the theoretical debate of whether CD is a dissociative or a somatization disorder somewhat paradoxical, since this would defer to another discipline the responsibility to explain a “neurologic disease.” Attempting to settle such a debate goes beyond the aims of this review, and the interested reader is therefore referred to other works.14
Epidemiology and demographics
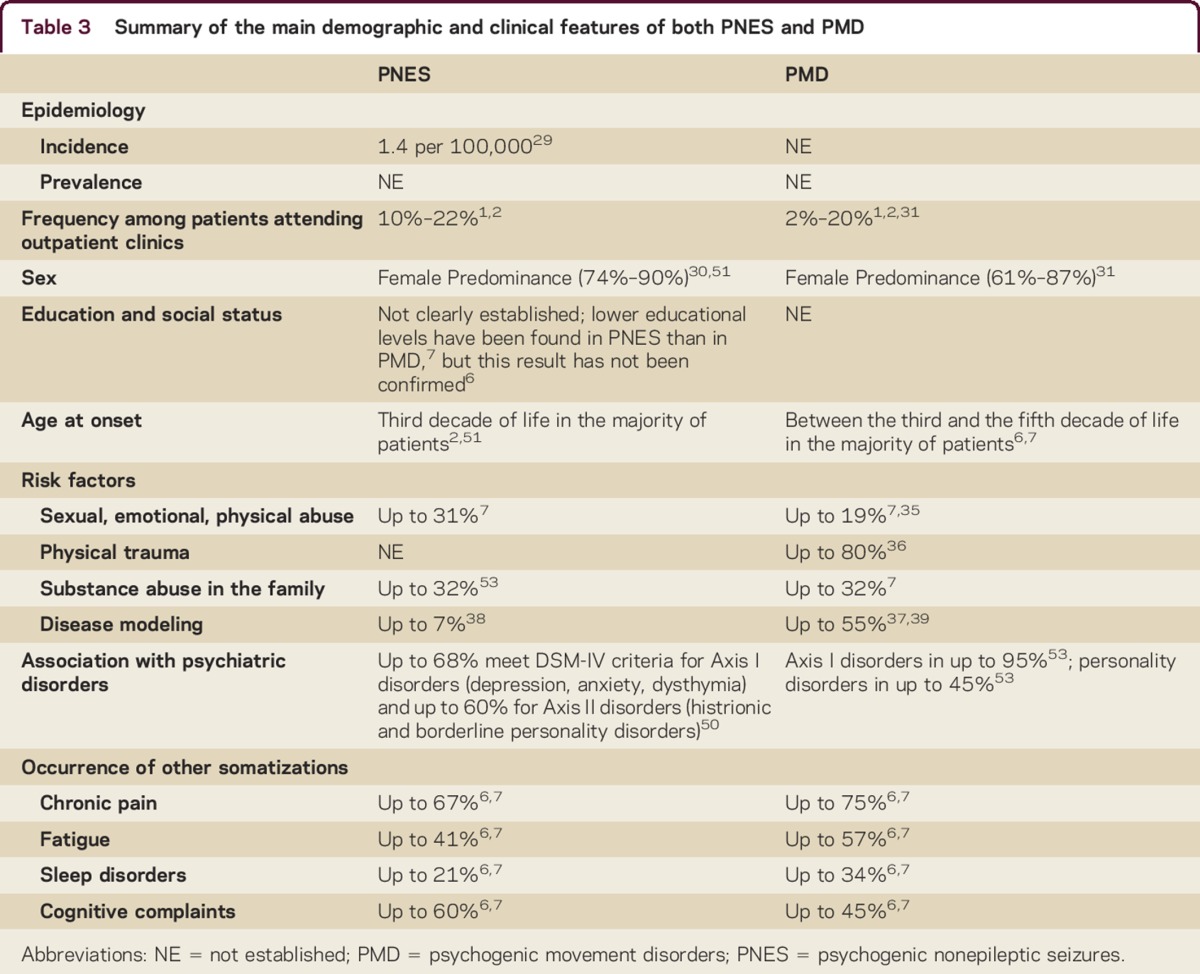
Both PNES and PMD are commonly seen in clinical practice (up to 20% of outpatients1,2), but their precise prevalence and incidence are unknown. The only population-based study available yielded an incidence of PNES of 1.4 per 100,000, with highest age-specific incidence (3.4 per 100,000) in the 15–24 years age group.29 For both disorders, there is a predominance of women (74%–90% among PNES30 and 61%–87% among PMD),31 but in patients with PNES, such sex distinction seems to become evident only after the age of 13 years.32 These disorders can develop at any age,29–32 though a higher occurrence is consistently reported between age 20 and 45 for both PNES and PMD.2,31 Moreover, no demographic and clinical differences with regards to ethnicity have been found between Spanish and North American populations33 and when comparing patients from Latin America with other published series from North America and Turkey,34 supporting the transcultural aspect of these disorders.34 The assessment of other demographic and social features, including education level, employment, and marital status, also did not reveal any difference between patients with PNES and PMD.7
Risk factors
Several risk factors for both PNES and PMD have been identified.
A history of sexual, emotional, and physical abuse, or combinations of them, has been reported in up to 50% of patients with PNES and in up to 19% of patients with PMD.7,35 It has been found more frequently in PNES than in PMD in one comparative study (31% vs 16% respectively, p = 0.0335), although the authors acknowledged that this could reflect an ascertainment bias, as abuse history was unknown/not recorded in some of the PMD patients. Other trauma, including previous surgery or physical trauma, dysfunctional family relationships, and major emotionally stressful life events, such as divorce or death of a family member, also has been more frequently reported in both PNES and PMD patients.30 However, this could also reflect a selection bias, since it has been recently found that up to 80% of patients can have a physical event shortly preceding the onset of the PMD.36
In both groups, a family history of substance abuse has been reported as high as 32%, particularly with regard to alcohol abuse (about 25%).7 Finally, there have been some suggestions that a positive family history of neurologic disease or frequent exposure to individuals with neurologic disease (for example, in health care workers) can act as modeling of organic disease and play an important role in the development of psychogenic symptoms. This is the case in up to 55% of patients with PMD37 and in up to 7% of patients with PNES.38 Recently, a study suggested a significant association between PMD and exposure to phenotypically congruent movement disorder models among family members or friendship.39 Moreover, PMD have been also reported to occur in several members of the same family,40 again reinforcing the concept that familial illness exposure might play a role in the pathogenesis of the symptoms.
Clinical features
A general overview of the clinical features of PNES and PMD is provided in table 3.
Table 3.
Summary of the main demographic and clinical features of both PNES and PMD
Phenomenology of PNES and PMD
The description of the phenomenologic features of PNES has been usually made in comparison with those of epileptic seizures. Several studies have identified different subgroups based on the phenomenology of the attacks, aiming to provide a clinical classification of PNES.41 Among the different classifications, a number of PNES subgroups have been consistently identified, suggesting that there exists a consistent semiology among patients with PNES across countries and cultures.42 Accordingly, PNES may manifest with one of the following 5 main phenomenologic patterns43 (although, in clinical practice, patients often present with a mixture of these): (1) attacks of excessive, violent movements of limbs (less frequently with the involvement of the trunk), often associated with hyperventilation (hypermotor or hyperkinetic attacks); (2) more bizarre attacks of motor activity manifesting with trunk extension or, less frequently, flexion (complex motor or axial dystonic attacks); (3) attacks associated with a rhythmic motor pattern, resembling tremor, usually associated with preserved responsiveness (rhythmic motor or paukinetic attacks); (4) attacks with unresponsiveness as the only clinical feature, which can be further associated with hyperventilation (pseudosyncope, dialeptic or psychogenic atonic attacks); and (5) subjective feeling of dizziness, anxiety, abdominal pain, or swelling in the throat during the attack without any external manifestations (nonepileptic aura). It is obvious that, although potentially useful, such classification is characterized by an excessive simplification, which does not take into account a number of other clinical features such as stuttering course, forced eye closure, ictal avoidance, fighting, or crying/weeping, and intelligible speech, which may accompany the attacks.44 Moreover, it focuses on the phenomenology of the attacks, discarding important features such as the experience of a buildup before the attack and a sense of relief after the attack, which has been reported in a number of patients with PNES.45
Similarly, PMD have been classified based on the description of the main (but often not the unique) clinical features. When evaluated this way, the predominant types of PMD are tremor (30%–50%), dystonia and myoclonus (about 20%–25% each), gait disorder (roughly 10%), and less frequently parkinsonism (about 5%).46 Described in general, however, PMD can present with a great variety of movements and can also affect speech.47 Moreover, in a number of patients there can be other features such as give-way weakness or psychogenic patterns of sensory loss and convergence spasm might be present on eye movement examination.47 Altered responsiveness can be present in up to one-third of PMD as well as “convulsive” features,6 suggesting a certain overlap with PNES. Moreover, PMD usually have an episodic course (up to 60%, according to one study6). Only one study, however, has focused on a relatively large cohort of paroxysmal PMD.48 Detailed analysis of these patients found that at least one-third of them had additional clinical characteristics including occasions of unresponsiveness during attacks, episodes of “collapse,” speech disturbances, drowsiness, blurred vision, and changes in the respiratory rhythm, all features that have been commonly reported in PNES.19 Interestingly, also in this group of patients there could be a premonitory feeling or a sense of relief once the “attack” has terminated.49
Association with psychiatric disorders
Both PNES and PMD can be frequently encountered in the context of a coexisting psychiatric disorder. One study conducted in 30 PNES patients found that 67.7% met criteria for 2 or more simultaneous Axis I DSM-4 diagnoses (mostly major depression, 13.3%; dysthymia, 16.7%; and anxiety disorders, 16.6%) and 60% for an Axis II personality disorder (histrionic personality disorder in 26.7% and borderline personality disorder in 13.3%).50 Comparative studies between patients with PNES and with epilepsy yielded contrasting results in this regard. Some studies found no differences,51 whereas other found increased Axis I disorders in PNES patients.52 In one study conducted on 42 patients with documented PMD, a structured interview disclosed a coexisting psychiatric disorder in almost all of them: 19.1% had major depression, 38.2% anxiety disorders, 11.9% comorbid major depression and anxiety disorders, and 45% personality disorders.53 Major depression and anxiety disorders were associated with poorer outcome with respect to the abnormal movements.53 However, in other series co-occurrence of psychiatric disorders has been reported to occur in only one-third of patients.54 Moreover, other authors did not find a causal relationship between psychological distress and psychogenic symptoms, suggesting that the psychological complaints were a general result of having an illness.55
One study directly comparing PNES and PMD patients found anxiety to be more frequent among the latter (16% vs 48%, p < 0.001).7 However, another comparative study between PNES and PMD found similar psychological profiles with regards to depression, anxiety, or other somatizations.6
Occurrence of other psychogenic symptoms
Besides the neurologic manifestations, both PNES and PMD patients often have a number of additional psychogenic symptoms. Chronic pain has been reported to occur in PNES with a frequency between 47%56 and 70%.7 Patients with PNES are prescribed pain medications (including opioid) more frequently than patients with idiopathic generalized epilepsy.57 Interestingly, a personal history of chronic pain or fibromyalgia was found to have a predictive value of 75% for the diagnosis of PNES in a retrospective series of patients with drug-resistant epilepsy.57 Compared with epilepsy patients, those with PNES were found to be more likely to have functional somatic syndromes (chronic pain disorders, tension headache, irritable bowel syndrome) and chronic medical illness characterized by intermittent attacks (migraine, asthma, gastroesophageal reflux disease).58 It has been suggested that the presence of at least one of these additional disorders greatly increases the clinical suspicion of PNES (positive predictive value of 75.7%). However, the retrospective nature of this study carries the risk of incomplete or inconsistent data collection.58
The occurrence of psychogenic non-neurologic symptoms in PMD has not been systematically evaluated. However, it is common clinical knowledge that patients with PMD often have other complaints. One example is the controversial coexistence of psychogenic dystonia with the complex regional pain syndrome (CRPS). A psychogenic cause has been suggested in a vast proportion of these patients and one study found that all of their 58 patients with CRPS with abnormal movements were likely to be “nonorganic” in origin.59 In another series of patients with psychogenic myoclonus, approximately 50% of them reported other unexplained medical symptoms (mainly gastrointestinal, fatigue, and pain).54 One study directly comparing patients with PNES and PMD found no difference between the 2 groups with regards to chronic pain syndrome (67% vs 75%, p = 0.30), subjective fatigue (41% vs 57%, p = 0.052), and sleep disorders (21% vs 34%, p = 0.06).7
Similarities and differences between PNES and PMD
The reappraisal of the existing literature in the field, with a focus on the few studies aimed to directly compare PNES and PMD patients, suggests that the similarities between these 2 groups appear to far exceed their differences (table 3). Despite some clinical features seeming to differentiate the 2 conditions, with loss of consciousness being the most striking difference between PNES and PMD, the clinical similarities between PNES and PMD seem to be impressive, and include the following: (1) age and sex distribution; (2) the relatively frequent co-occurrence of psychiatric disorders or similar psychological profiles between the 2 groups; and (3) the high rates of chronic pain and other somatization disorders. On this basis, we would advocate that these 2 groups of patients represent 2 ends of a continuum, where different clinical presentations explain referral to either the epilepsy or movement disorder specialists. In other words, the questionable clinical differences between these disorders seem to simply rely upon our a priori classification based on the main phenomenology. This criterion does not seem to underpin a robust rationale, also because in a number of these patients there are clear overlapping clinical features, with patients with paroxysmal PMD clearly reflecting the phenomenologic bridge between PNES and PMD. A possible criticism would come from the observation that some patients with paroxysmal PMD also fulfill the criteria for PNES, and vice versa.5–7,48,49 This misclassification bias could potentially overestimate the similarities between PNES and PMD. On the other hand, considering PNES and PMD as 2 different disorders might give rise to artificial differences. We would rather support the proposal that PNES and PMD should be considered as 2 syndromes, possibly sharing common pathophysiologic mechanisms. Hence, the crucial question would be whether we should lump or split.
From the clinical standpoint, such an ultraclassification of psychogenic (functional) neurologic symptoms (i.e., PNES vs PMD) can still have value, at least as far as diagnostic strategies are concerned. In fact, diagnosis of both PNES and PMD can be challenging and may rely in some patients on the personal experience of the involved physicians. There is hence no doubt that diagnostic certainty is higher in ultraspecialized tertiary centers, where additional investigations (i.e., video-EEG or neurophysiology) can also be carried out. On the other hand, however, such subclassification can hamper the development of successful treatments for these disorders. In fact, current therapeutic approaches vary between PNES and PMD, but there is poor systematic evidence to guide decisions and justify this. Psychotherapy (particularly cognitive behavioral therapy [CBT]) is the recommended and best-validated approach to treat PNES,60 whereas there are no large trials on CBT in PMD,61 despite individual small studies reporting success.62 Conversely, there has been considerable interest in the use of specific physiotherapy approaches to treat PMD, whereas this treatment seems less likely, intuitively, to be of benefit for people with intermittent attacks of abnormal movement, especially if associated with significant loss of awareness. However, there may still be overlap in treatment approaches here as commonly used CBT treatments for PNES often teach patients to distract themselves when they feel an attack coming on, and this distraction commonly involves movement. Other proposed treatments may have more overlap between PNES and PMD, for example pharmacologic approaches, psychodynamic psychotherapy, complementary medical treatments (acupuncture, hypnosis), and proposed experimental treatments (e.g., transcranial magnetic stimulation). While the interested reader is referred elsewhere for an overview of the possible treatments in PNES60 and PMD,63 there is clearly an unmet need both for well-designed clinical trials of established treatments and development of novel treatment approaches, especially for severely affected patients who are refractory to currently available treatments.
The proposal here of a similar pathophysiologic process underlying PNES and PMD suggests a potential opportunity for common therapeutic strategies, while still acknowledging that specific treatments may be most suitable for a particular phenotype. Although collaborative care seems obvious for patients with other neurologic conditions (one would think as an example of the complex care of advanced Parkinson disease, where treatment planning, including access to specialist treatments such as deep brain stimulation and infusion therapies, is planned within a multidisciplinary team), such a complex and multistepped approach has only recently suggested for psychogenic neurologic disorders.60,63 We would support the latter suggestions, highlighting the need of an integrated functional neurology service to implement more complex multidisciplinary care for both PNES and PMD.
Despite there being clinical overlap in a large number of patients with PNES and PMD, which suggests a shared underlying pathophysiology, it remains to be clarified why an individual patient develops a particular phenotype. A partial answer comes from evidence suggesting a significant association between PMD and exposure to phenotypically congruent movement disorder models among family members or friends.39 Yet disease modeling (which can occur both intraindividually and interindividually) does not seem to fully answer such a question. In fact, a recent study assessing the presence of physical events preceding the onset of PMD in 50 consecutive patients found that the phenomenology of the symptoms was plausibly related to the physical trigger in some of the cases,36 confirming previous suggestions that the nature of the physical precipitating and the affected body parts during the physical illness may influence the subsequent psychogenic symptom.64 This fits also with the common co-occurrence of epilepsy and PNES, where the epileptic seizure can be considered as a physical trigger (as well as perhaps a disease model) for PNES to develop.
Our findings demonstrate that there is a profound overlap between PNES and PMD, which would argue for a larger unifying psychopathology with variable phenotypic manifestations.8,9 Interestingly, an increasing number of functional neuroimaging studies recently have been performed in these populations, showing shared abnormalities in specific brain areas such as temporo-parietal, frontal, sensorimotor, and limbic regions,65 thus proving preliminary evidence for an abnormal integration of attention, emotion, and movement control, as the neurobiological basis for the generation of both PNES and PMD.
AUTHOR CONTRIBUTIONS
R. Erro: study concept and design, acquisition of data, analysis and interpretation. F. Brigo: study concept and design, acquisition of data, analysis and interpretation. E. Trinka: analysis and interpretation, critical revision of the manuscript for important intellectual content, study supervision. G. Turri: analysis and interpretation. M.J. Edwards: critical revision of the manuscript for important intellectual content, study supervision. M. Tinazzi: study concept and design, analysis and interpretation, study supervision.
STUDY FUNDING
No targeted funding reported.
DISCLOSURES
R. Erro serves on the editorial board of Movement Disorders. F. Brigo has received funding for travel or speaker honoraria from UCB Pharma and Eisai. E. Trinka served on scientific advisory boards for UCB, Eisai, Biogen, Takeda, Ever Neuropharma, Newbridge Pharma, Bial, and Sunovion; has received funding to attend conferences from UCB, Eisai, Böhringer, Biogen, Bayer, and Bial; serves on editorial advisory boards for Zweitschrift für Epileptologie, Mitteilungen der Österreichischen Sektion der ILAE, Klinische Neurophysiologie, Epileptologia, and Journal for Clinical Neurophysiology; and has received research support from UCB, FWF (Fonds zur Förderung der wissenschaftlichen Forschung), Austrian Research Foundation, European Union, and Austrian Science Fund. G. Turri reports no disclosures. M.J. Edwards serves on a scientific advisory board for Cure Parkinson's Trust; has received funding for travel and accommodation from the Movement Disorder Society; receives publishing royalties for Oxford Specialist Handbook of Parkinson's Disease and Movement Disorders (Oxford University Press, 2008); and receives research support from Medical Research Council NIHR (UK), UCL/UCLH Biomedical Research Centre, and Parkinson's UK Dystonia Society. M. Tinazzi reports no disclosures. Full disclosure form information provided by the authors is available with the full text of this article at Neurology.org/cp.
REFERENCES
- 1.Stone J, Carson A, Duncan R, et al. Who is referred to neurology clinics? The diagnoses made in 3781 new patients. Clin Neurol Neurosurg 2010;112:747–751. [DOI] [PubMed] [Google Scholar]
- 2.Lempert T, Dieterich M, Huppert D, Brandt T. Psychogenic disorders in neurology: frequency and clinical spectrum. Acta Neurol Scand 1990;82:335–340. [DOI] [PubMed] [Google Scholar]
- 3.Evens A, Vendetta L, Krebs K, Herath P. Medically unexplained neurologic symptoms: a primer for physicians who make the initial encounter. Am J Med 2015;128:1059–1064. [DOI] [PubMed] [Google Scholar]
- 4.Fink P, Steen Hansen M, Søndergaard L. Somatoform disorders among first-time referrals to a neurology service. Psychosomatics 2005;46:540–548. [DOI] [PubMed] [Google Scholar]
- 5.Grimaldi I, Dubuc M, Kahane P, Bougerol T, Vercueil L. Anxiety and depression in psychogenic movement disorder and non-epileptic seizures: a prospective comparative study. Rev Neurol 2010;166:515–522. [DOI] [PubMed] [Google Scholar]
- 6.Hopp JL, Anderson KE, Krumholz A, Gruber-Baldini AL, Shulman LM. Psychogenic seizures and psychogenic movement disorders: are they the same patients? Epilepsy Behav 2012;25:666–669. [DOI] [PubMed] [Google Scholar]
- 7.Driver-Dunckley E, Stonnington CM, Locke DE, Noe K. Comparison of psychogenic movement disorders and psychogenic nonepileptic seizures: is phenotype clinically important? Psychosomatics 2011;52:337–345. [DOI] [PubMed] [Google Scholar]
- 8.Erro R, Tinazzi M. Functional (psychogenic) paroxysms: the diagnosis is in the eye of the beholder. Parkinsonism Relat Disord 2014;20:343–344. [DOI] [PubMed] [Google Scholar]
- 9.Mula M. Are psychogenic non-epileptic seizures and psychogenic movement disorders two different entities? When even neurologists stop talking to each other. Epilepsy Behav 2013;26:100–101. [DOI] [PubMed] [Google Scholar]
- 10.LaFrance WC, Jr, Devinsky O. The treatment of nonepileptic seizures: historical perspectives and future directions. Epilepsia 2004;45(suppl 2):15–21. [DOI] [PubMed] [Google Scholar]
- 11.Edwards MJ, Stone J, Lang AE. From psychogenic movement disorder to functional movement disorder: it's time to change the name. Mov Disord 2014;29:849–852. [DOI] [PubMed] [Google Scholar]
- 12.Edwards MJ, Bhatia KP. Functional (psychogenic) movement disorders: merging mind and brain. Lancet Neurol 2012;11:250–260. [DOI] [PubMed] [Google Scholar]
- 13.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Health Disorders: DSM-5, 5th ed Washington, DC: American Psychiatric Publishing; 2013. [Google Scholar]
- 14.Stone J, LaFrance WC, Jr, Levenson JL, Sharpe M. Issues for DSM-5: conversion disorder. Am J Psychiatry 2010;167:626–627. [DOI] [PubMed] [Google Scholar]
- 15.ICD-11 Beta Draft [online]. Available at: http://apps.who.int/classifications/icd11/browse/f/en#!/http%3A%2F%2Fid.who.int%2Ficd%2Fentity%2F1614846095. Accessed August 2015. [Google Scholar]
- 16.Stone J, Campbell K, Sharma N, Carson A, Warlow CP, Sharpe M. What should we call pseudoseizures? The patient's perspective. Seizure 2003;12:568–572. [DOI] [PubMed] [Google Scholar]
- 17.Plug L, Sharrack B, Reuber M. Seizure, fit or attack? The use of diagnostic labels by patients with epileptic or non-epileptic seizures. Appl Linguist 2009;31:91–114. [Google Scholar]
- 18.Fahn S, Olanow C. Reply to: psychogenic movement disorders: what's in a name? Mov Disord 2014;29:1699–1701. [DOI] [PubMed] [Google Scholar]
- 19.Ganos C, Erro R, Bhatia KP, Tinazzi M. Comment on psychogenic versus functional movement disorders. Mov Disord 2014;29:1696. [DOI] [PubMed] [Google Scholar]
- 20.Bodde NM, Brooks JL, Baker GA, et al. , Psychogenic non-epileptic seizures: definition, etiology, treatment and prognostic issues: a critical review. Seizure 2009;18:543–553. [DOI] [PubMed] [Google Scholar]
- 21.LaFrance WC, Jr, Baker GA, Duncan R, Goldstein LH, Reuber M. Minimum requirements for the diagnosis of psychogenic nonepileptic seizures: a staged approach: a report from the International League Against Epilepsy Nonepileptic Seizures Task Force. Epilepsia 2013;54:2005–2018. [DOI] [PubMed] [Google Scholar]
- 22.Gupta A, Lang AE. Psychogenic movement disorders. Curr Opin Neurol 2009;22:430–436. [DOI] [PubMed] [Google Scholar]
- 23.Schwingenschuh P, Katschnig P, Seiler S, et al. Moving toward “laboratory-supported” criteria for psychogenic tremor. Mov Disord 2011;26:2509–2515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Erro R, Bhatia KP, Edwards MJ, Farmer SF, Cordivari C. Clinical diagnosis of propriospinal myoclonus is unreliable: an electrophysiologic study. Mov Disord 2013;28:1868–1873. [DOI] [PubMed] [Google Scholar]
- 25.Schrag A, Trimble M, Quinn N, Bhatia K. The syndrome of fixed dystonia: an evaluation of 103 patients. Brain 2004;127:2360–2372. [DOI] [PubMed] [Google Scholar]
- 26.Oakley DA. Hypnosis and conversion hysteria: a unifying model. Cogn Neuropsychiatry 1999;4:243–265. [DOI] [PubMed] [Google Scholar]
- 27.Reilly J, Baker GA, Rhodes J, Salmon P. The association of sexual and physical abuse with somatization: characteristics of patients presenting with irritable bowel syndrome and non-epileptic attack disorder. Psychol Med 1999;29:399–406. [DOI] [PubMed] [Google Scholar]
- 28.Brown RJ. Different types of “dissociation” have different psychological mechanisms. J Trauma Dissociation 2006;7:7–28. [DOI] [PubMed] [Google Scholar]
- 29.Sigurdardottir KR, Olafsson E. Incidence of psychogenic seizures in adults: a population-based study in Iceland. Epilepsia 1998;39:749–752. [DOI] [PubMed] [Google Scholar]
- 30.Lancman ME, Brotherton TA, Asconapé JJ, Penry JK. Psychogenic seizures in adults: a longitudinal analysis. Seizure 1993;2:281–286. [DOI] [PubMed] [Google Scholar]
- 31.Factor SA, Podskalny GD, Molho ES. Psychogenic movement disorders: frequency, clinical profile, and characteristics. J Neurol Neurosurg Psychiatry 1995;59:406–412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Patel H, Scott E, Dunn D, Garg B. Nonepileptic seizures in children. Epilepsia 2007;48:2086–2092. [DOI] [PubMed] [Google Scholar]
- 33.Cubo E, Hinson VK, Goetz CG, et al. Transcultural comparison of psychogenic movement disorders. Mov Disord 2005;20:1343–1345. [DOI] [PubMed] [Google Scholar]
- 34.Munhoz RP, Zavala JA, Becker N, Teive HA. Cross-cultural influences on psychogenic movement disorders: a comparative review with a Brazilian series of 83 cases. Clin Neurol Neurosurg 2011;113:115–118. [DOI] [PubMed] [Google Scholar]
- 35.Kranick S, Ekanayake V, Martinez V, Ameli R, Hallett M, Voon V. Psychopathology and psychogenic movement disorders. Mov Disord 2011;26:1844–1850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Pareés I, Kojovic M, Pires C, et al. Physical precipitating factors in functional movement disorders. J Neurol Sci 2014;338:174–177. [DOI] [PubMed] [Google Scholar]
- 37.Shill H, Gerber P. Evaluation of clinical diagnostic criteria for psychogenic movement disorders. Mov Disord 2006;21:1163–1168. [DOI] [PubMed] [Google Scholar]
- 38.Asadi-Pooya AA, Emami M. Demographic and clinical manifestations of psychogenic non-epileptic seizures: the impact of co-existing epilepsy in patients or their family members. Epilepsy Behav 2013;27:1–3. [DOI] [PubMed] [Google Scholar]
- 39.Pellicciari R, Superbo M, Gigante AF, Livrea P, Defazio G. Disease modeling in functional movement disorders. Parkinsonism Relat Disord 2014;20:1287–1289. [DOI] [PubMed] [Google Scholar]
- 40.Stamelou M, Cossu G, Edwards MJ, et al. Familial psychogenic movement disorders. Mov Disord 2013;28:1295–1298. [DOI] [PubMed] [Google Scholar]
- 41.Meierkord H, Will B, Fish D, Shorvon S. The clinical features and prognosis of pseudoseizures diagnosed using video-EEG telemetry. Neurology 1991;41:1643–1646. [DOI] [PubMed] [Google Scholar]
- 42.Dhiman V, Sinha S, Rawat VS, Harish T, Chaturvedi SK, Satishchandra P. Semiological characteristics of adults with psychogenic nonepileptic seizures (PNESs): an attempt towards a new classification. Epilepsy Behav 2013;27:427–432. [DOI] [PubMed] [Google Scholar]
- 43.Hubsch C, Baumann C, Hingray C, et al. Clinical classification of psychogenic non-epileptic seizures based on video-EEG analysis and automatic clustering. J Neurol Neurosurg Psychiatry 2011;82:955–960. [DOI] [PubMed] [Google Scholar]
- 44.Syed TU, LaFrance WC, Jr, Kahriman ES, et al. Can semiology predict psychogenic nonepileptic seizures? A prospective study. Ann Neurol 2011;69:997–1004. [DOI] [PubMed] [Google Scholar]
- 45.Roberts NA, Reuber M. Alterations of consciousness in psychogenic nonepileptic seizures: emotion, emotion regulation and dissociation. Epilepsy Behav 2014;30:43–49. [DOI] [PubMed] [Google Scholar]
- 46.Miyasaki JM, Sa DS, Galvez-Jimenez N, Lang AE. Psychogenic movement disorders. Can J Neurol Sci 2003;30(suppl 1):94–100. [DOI] [PubMed] [Google Scholar]
- 47.Hallett M, Weiner WJ, Kompoliti K. Psychogenic movement disorders. Parkinsonism Relat Disord 2012;18(suppl 1):155–157. [DOI] [PubMed] [Google Scholar]
- 48.Ganos C, Aguirregomozcorta M, Batla A, et al. Psychogenic paroxysmal movement disorders: clinical features and diagnostic clues. Parkinsonism Relat Disord 2014;20:41–46. [DOI] [PubMed] [Google Scholar]
- 49.Vidailhet M, Bourdain F, Nuss P, Trocello J. Paroxysmal psychogenic movement disorders. In: Fahn S, Hallet M, eds. Psychogenic Movement Disorders. Philadelphia: Lippincott Williams & Wilkins; 2006: 76–81. [Google Scholar]
- 50.Baillés E, Pintor L, Fernandez-Egea E, et al. Psychiatric disorders, trauma, and MMPI profile in a Spanish sample of nonepileptic seizure patients. Gen Hosp Psychiatry 2004;26:310–315. [DOI] [PubMed] [Google Scholar]
- 51.Abubakr A, Kablinger A, Caldito G. Psychogenic seizures: clinical features and psychological analysis. Epilepsy Behav 2003;4:241–245. [DOI] [PubMed] [Google Scholar]
- 52.Scévola L, Teitelbaum J, Oddo S, et al. Psychiatric disorders in patients with psychogenic nonepileptic seizures and drug-resistant epilepsy: a study of an Argentine population. Epilepsy Behav 2013;29:155–160. [DOI] [PubMed] [Google Scholar]
- 53.Feinstein A, Stergiopoulos V, Fine J, Lang AE. Psychiatric outcome in patients with a psychogenic movement disorder: a prospective study. Neuropsychiatry Neuropsychol Behav Neurol 2001;14:169–176. [PubMed] [Google Scholar]
- 54.Erro R, Edwards MJ, Bhatia KP, Esposito M, Farmer SF, Cordivari C. Psychogenic axial myoclonus: clinical features and long-term outcome. Parkinsonism Relat Disord 2014;20:596–599. [DOI] [PubMed] [Google Scholar]
- 55.Van Beilen M, Griffioen BT, Gross A, Leenders KL. Psychological assessment of malingering in psychogenic neurological disorders and non-psychogenic neurological disorders: relationship to psychopathology levels. Eur J Neurol 2009;16:1118–1123. [DOI] [PubMed] [Google Scholar]
- 56.Gazzola DM, Carlson C, Rugino A, Hirsch S, Starner K, Devinsky O. Psychogenic nonepileptic seizures and chronic pain: a retrospective case-controlled study. Epilepsy Behav 2012;25:662–665. [DOI] [PubMed] [Google Scholar]
- 57.Benbadis SR. A spell in the epilepsy clinic and a history of “chronic pain” or “fibromyalgia” independently predict a diagnosis of psychogenic seizures. Epilepsy Behav 2005;6:264–265. [DOI] [PubMed] [Google Scholar]
- 58.Dixit R, Popescu A, Bagić A, Ghearing G, Hendrickson R. Medical comorbidities in patients with psychogenic nonepileptic spells (PNES) referred for video-EEG monitoring. Epilepsy Behav 2013;28:137–140. [DOI] [PubMed] [Google Scholar]
- 59.Verdugo RJ, Ochoa JL. Abnormal movements in complex regional pain syndrome: assessment of their nature. Muscle Nerve 2000;23:198–205. [DOI] [PubMed] [Google Scholar]
- 60.LaFrance WC, Jr, Reuber M, Goldstein LH. Management of psychogenic nonepileptic seizures. Epilepsia 2013;54(suppl 1):53–67. [DOI] [PubMed] [Google Scholar]
- 61.Ruddy R, House A. Psychosocial interventions for conversion disorder. Cochrane Database Syst Rev 2005;4:CD005331. [DOI] [PubMed] [Google Scholar]
- 62.Hopp JL, LaFrance WC., Jr Cognitive behavioral therapy for psychogenic neurological disorders. Neurologist 2012;18:364–372. [DOI] [PubMed] [Google Scholar]
- 63.Ricciardi L, Edwards MJ. Treatment of functional (psychogenic) movement disorders. Neurotherapeutics 2014;11:201–207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Moss-Morris R, Spence M. To “lump” or to “split” the functional somatic syndromes: can infectious and emotional risk factors differentiate between the onset of chronic fatigue syndrome and irritable bowel syndrome? Psychosom Med 2006;68:463–469. [DOI] [PubMed] [Google Scholar]
- 65.Van der Kruijs SJ, Bodde NM, Vaessen MJ, et al. Functional connectivity of dissociation in patients with psychogenic non-epileptic seizures. J Neurol Neurosurg Psychiatry 2012;83:239–247. [DOI] [PubMed] [Google Scholar]