

Abstract
In haploidentical stem cell transplantations (haplo-SCT), nearly all patients have more than one donor. A key issue in the haplo-SCT setting is the search for the best donor, because donor selection can significantly impact the incidences of acute and chronic graft-versus-host disease, transplant-related mortality, and relapse, in addition to overall survival. In this review, we focused on factors associated with transplant outcomes following unmanipulated haplo-SCT with anti-thymocyte globulin (ATG) or after T-cell-replete haplo-SCT with post-transplantation cyclophosphamide (PT/Cy). We summarized the effects of the primary factors, including donor-specific antibodies against human leukocyte antigens (HLA); donor age and gender; killer immunoglobulin-like receptor-ligand mismatches; and non-inherited maternal antigen mismatches. We also offered some expert recommendations and proposed an algorithm for selecting donors for unmanipulated haplo-SCT with ATG and for T-cell-replete haplo-SCT with PT/Cy.
Keywords: Unmanipulated haploidentical stem cell transplantation, Donor, Donor-specific anti-human leukocyte antigen antibody, Natural killer alloreactivity, Age, Non-inherited maternal antigen mismatch
Background
Allogeneic hematopoietic cell transplantation (SCT) remains the only curative therapy for a majority of malignant hematologic diseases [1–7]. Currently, for patients that require transplantation, but have no related or unrelated donors with matching human leukocyte antigen (HLA), the HLA-haploidentical SCT (haplo-SCT) approach is an attractive option. Haplo-SCT is widely available, and immediate access is possible with donor-derived cellular therapies [1, 5, 6, 8–39]. Many haplo-SCT protocols have been successfully established, with promising clinical outcomes, due to improved understanding of the mechanisms underlying the HLA barriers and how to cross them [1, 8, 16, 24, 26, 40–44]. Approaches for T-cell depletion (TCD) transplantation, including “megadose” CD34-selection and TCRαβ depletion, are designed to preserve γδ T cells, natural killer (NK) cells, and antigen-presenting cells. Alternatively, several approaches are also available for T-cell-replete (TCR) transplantation, including anti-thymocyte globulin (ATG)-based protocols or post-transplantation cyclophosphamide (PT/Cy). Haplo-SCT has become easier to perform than in the past, thanks to the shift from T-depleted grafts to grafts composed of unmanipulated marrow and/or peripheral blood stem cells [5, 6, 10, 19, 21, 30, 31, 34, 45, 46]. In particular, the “GIAC” protocol for haplo-SCT with ATG is a procedure that includes “G”: treating donors with granulocyte colony-stimulating factor (G-CSF), to induce donor immune tolerance [47–51]; “I”: intensified immunologic suppression in the recipient, to promote engraftment and prevent GVHD; “A”: anti-thymocyte globulin administration for prophylaxis of graft-versus-host disease (GVHD) and graft rejection; and “C”: combining G-CSF-primed bone marrow cells (G-BM) and G-CSF-mobilized peripheral blood stem cells (G-PB) harvested from donors to provide a pooled source of stem cells for grafting [1, 52–55]. Results from two additional trials from Lee et al. in Korea [56] and Di Bartolomeo et al. [57] from Italy largely reproduced the data from us; the effectiveness of the “GIAC” protocol was verified by these two external trials. As a result of these trends, the number of treatments that applied unmanipulated haplo-SCT with ATG or PT/Cy [1, 36, 58, 59] has increased significantly every year in China, the USA, and Europe (Table 1) [36–38, 60–66]. Some experienced centers, such as Peking University and Johns Hopkins University, have adopted haplo-SCT as the main source of alternative donors, based on outcomes that compared favorably with HLA-matched sibling or unrelated donor transplantations (MUDT) [17, 22, 62, 67]. With the advancement of haplo-SCT, particularly unmanipulated haplo-SCT, parents, children, siblings, and second-degree relatives, have all become potential donor candidates. Because most patients have more than one potential haplo donor, this raises an important question [68]: Who is the best donor for TCR haplo-SCT? Indeed, haplo donor selection may have a significant impact on the incidence of acute and chronic GVHD, transplant-related mortality (TRM), and relapse, in addition to overall survival (OS) [9–13, 19, 34, 36, 69–72]. In this review, we discuss the effects of HLA mismatching on transplant outcomes in patients treated with unmanipulated haplo-SCT with ATG [1, 52–55] or with PT/Cy [1, 36, 58, 59]. We also summarize donor-related variables that are associated with clinical outcomes, and we provide a rationale for using a personalized algorithm for donor selection in unmanipulated haplo-SCT with ATG [1, 52–55] or PT/Cy [1, 36, 58, 59].
Table 1.
Recent informative trials and results of T-cell-replete haploidentical stem cell transplantation
| Reference, year, ref, and median age | Patients (No.) | Diagnosis | Graft | ANC median (range) | PLT median (range) | GVHD | TRM | Relapse | LFS | OS | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Acute II–IV | Chronic | ||||||||||
| Unmanipulated haplo-SCT with ATG | |||||||||||
| Di Bartolomeo P, et al. [57] (37) | 80 | HM | G-BM | 21 (12–38) | 28 (14–185) | 24 % | 17 % at 2 yr | 36 % at 3 yr | 21 % at 1 yr | 38 % at 3 yr | 45 % at 3 yr |
| Wang Y, et al. [10] (25) | 1210 | HM | G-BM + G-PB | 13 (8–49) | 16 (5–100) | 40 % | 50 % | 17 % at 3 yr | 17 % at 3 yr | 67 % at 3 yr | 70 % at 3 yr |
| Luo Y, et al. [14] (25) | 99 | HM | G-PB | 12 (8–24) | 15 (6–53) | 42.4 % | 41.4 % at 2 yr | 30.5 % at 5 yr | 14.2 % at 5 yr | 58.3 % at 5 yr | 60.8 % at 5 yr |
| Gao L, et al. [66] (25.4) | 26 | SAA | G-PB + G-BM | 13 (11–19) | 13 (10–21) | 8.0 % | 40 % | 15.4 % at 2 yr | NA | NA | 84.6 % at 2 yr |
| Peccatori J, et al. [19] (48) | 121 | HM | G-PB | 17 (11–61) | 19 (7–154) | 35 % | 47 % at 2 yr | 31 % at 3 yr | 48 % at 3 yr | 20 % at 3 yr | 25 % at 3 yr |
| Shin SH, et al. [29] (48) | 60 | MDS | G-PB | 12 (8–23) | 15 (6–132) | 36.7 % | 48.3 % | 23.3 % at 2 yr | 34.8 % at 2 yr | 41.9 % at 2 yr | 46.6 % at 2 yr |
| Yahng SA, et al. [120] (41) | 80 | AML | G-PB | 11 | 10 | 47.5 % | 45 % | 12.2 % at 2 yr | 26.6 % at 2 yr | 61.1 % at 2 yr | 66 % at 2 yr |
| Lin X, et al. [78] (23) | 105 | HM | G-PB | 14 (10–25) | 16 (9–38) | 21.9 % | 24.1 % at 2 yr | 30.5 % at 3 yr | 21.9 % at 3 yr | 41.1 % at 3 yr | 50.6 % at 3 yr |
| TCR haplo-SCT with PT/Cy | |||||||||||
| Raiola AM, et al. [38] (45) | 92 | HM | SS-BM (92) | 18 (11–32) | 32 (5–83) | 14 % | 15 % | 18 % at 1000 days | 35 % | 43 % at 4 yr | 52 % at 4 yr |
| McCurdy SR, et al. [36] (55) | 372 | HM | SS-BM | 90 %a | 88 %b | 32 % at 6 m | 13 % at 2 yr | 11 % at 1 yr | 46 % at 3 yr | 40 % at 3 yr | 50 % at 3 yr |
| Bacigalupo A, et al. [37] (47) | 148 | HM | SS-BM | 17 (13–32) | NA | 18 % | 20 % at 2 yr | 14 % at 4 yr | 27 % at 4 yr | NA | 77 % for CR1 49 % for CR2 38 % for AD |
| Solomon SR, et al. [61] (46) | 30 | HM | G-PB | 16 (NA) | 25 (NA) | 43 % | 56 % | 3 % at 2 yr | 24 % at 2 yr | 73 % at 2 yr | 78 % at 2 yr |
| Cieri N, et al. [64] (55) | 40 | HM | G-PB | 18 (13–45) | 16 (9–100) | 15 % | 20 % at 1 yr | 17 % at 1 yr | 35 % at 1 yr | 48 % at 1 yr | 56 % at 1 yr |
| Esteves I, et al. [65] (17) | 16 | SAA | SS-BM (13) G-PB (3) | 19 (16–29) | 21 (20–29) | 13 % | 20 % | 32.9 % at 1 yr | NA | NA | 67.1 % at 1 yr |
| Ciurea SO, et al. [62] (NA) | 104c | AML | SS-BM (85) G-PB (19) | 90 % | 88 % | 16 % | 30 % at 3 yr | 14 % at 3 yr | 44 % at 3 yr | NA | 45 % at 3 yr |
| 88d | AML | SS-BM (77) G-PB (11) | 93 % | 88 % | 19 % | 34 % at 3 yr | 9 % at 3 yr | 58 % at 3 yr | NA | 46 % at 3 yr | |
| Kasamon YL, et al. [59] (61) | 271 | HM | SS-BM | 88–93 % | 84–89 % | 33 % at 6 m | 12 % at 1 yr | 10 % at 1 yr | 46 % at 3 yr | 37 % at 3 yr | 46 % at 3 yr |
Published between 2013 and 2015
Ref reference, Pts patients, No. number, ANC absolute neutrophil count, PLT platelet, GVHD graft-versus-host disease, TRM transplant-related mortality, LFS leukemia-free survival, OS overall survival, haplo-SCT haploidentical stem cell transplantation, ATG anti-thymocyte globulin, HM hematological malignancies, G-BM granulocyte colony-stimulating factor (G-CSF)-primed bone marrow, yr year, G-PB G-CSF-mobilized peripheral blood stem cell grafts, UCB umbilical cord blood, NA not available, AL acute leukemia, SAA severe aplastic anemia, MDS myelodysplastic syndrome, AML acute myeloid leukemia, PT/Cy posttransplant cyclophosphamide, SS-BM steady-state bone marrow, m months, AD advanced disease
aIndicates the probability of neutrophil recovery by day 30
bIndicates the probability of platelet recovery ≥20,000/μL by day 60
cIndicates that patients received myeloablative conditioning regimens
dIndicates that patients received reduced intensity conditioning regimens
Effects of the locus of HLA-mismatch on haplo-SCT outcomes
Before the year 2000, patients that received haplo-SCT had relatively poor transplant outcomes, due to the use of conditioning and GVHD prophylaxis regimens that were similar to those used for transplantations from HLA-matched donors [73, 74]. Anasetti et al. [73] found that the degree of recipient HLA incompatibility was associated with the incidence of severe acute GVHD. Indeed, survival decreased as the degree of HLA disparity increased. Szydlo et al. [74] showed that, among patients with early leukemia that received transplantations, the relative risks of treatment failure were 2.43 and 3.79, when related donors had one and two mismatched HLA loci, respectively, compared to when donors were HLA-matched siblings (the reference group). Among patients with more advanced leukemia that received transplantations, differences in treatment failure were less striking; the relative risks of treatment failure were 1.22 and 1.81, when related donors had one and two HLA antigen mismatches, respectively, compared to the reference group. These data suggested that clinical outcomes depend on the degree of HLA mismatching in the early stages of haplo-SCT, because of little knowledge on immune tolerance and less approaches to overcome the HLA barriers.
Over the last 10 years, haplo-SCT outcomes have substantially improved, due to the development of novel GVHD prophylaxis strategies, improved supportive care strategies, and application of new strategies for relapse prophylaxis and treatment (Table 1) [18, 19, 28, 36, 42, 62, 75–77]. In 2006, a group at the University of Peking reported that the cumulative incidences of acute and chronic GVHD were comparable among patients with one-, two-, or three-locus mismatches, when treated with unmanipulated haploidentical blood and marrow transplantations and an ATG conditioning regimen [52]. They also demonstrated that HLA mismatching had no effect on other transplantation outcomes, including relapse, leukemia-free survival (LFS), and OS [52]. These results were confirmed by researchers from Peking University [9–12] and other transplantation centers in China [14, 35, 78]. Kasamon et al. [59] confirmed the findings by Huang et al., when they showed that greater HLA disparity did not appear to worsen the overall outcome after non-myeloablative haploidentical bone marrow transplantation with a high-dose PT/Cy. In a prospective, multicenter phase I/II study on unmanipulated haplo-SCTs performed in five institutions in Japan, Ikegame et al. [77] reported that HLA disparity was not associated with GVHD, TRM, relapse, or survival. Similar results were observed in recent updated reports on haplo-SCT with TCD or TCR [34, 35, 62, 72].
In an unmanipulated haplo-SCT protocol, Huang et al. [79] found that the HLA-B + DR combination mismatch was an independent risk factor for grades II–III and III–IV acute GVHD in patients with chronic myeloid leukemia (CML). Huo et al. [80] demonstrated that the HLA-B mismatch was also an independent risk factor for acute GVHD and TRM in patients with hematological diseases. However, SCT is not a first-line treatment option for patients with CML; therefore, associations between specific HLA-locus mismatches and haplo-SCT outcomes should be prospectively investigated in other hematological diseases.
In summary, studies on unmanipulated haplo-SCT with ATG [1, 52–55] or with PT/Cy [1, 36, 58, 59] showed that HLA disparity did not impact outcome. However, for donor selection, some specific HLA-loci profiles remain to be explored. Nevertheless, more attention has been focused on how donor-related, non-HLA variables affect clinical outcomes.
Donor selection based on non-HLA variables
Because the impact of HLA disparity on transplantation outcome has diminished, researchers are currently investigating the effects of other variables on survival after unmanipulated haplo-SCT with ATG [1, 52–55] or with PT/Cy [1, 36, 58, 59]. A number of donor-related factors should be considered in donor selection for haplo-SCT, including donor-specific anti-HLA antibodies (DSA) [12, 81, 82], donor age and gender [10, 83], ABO compatibility, natural killer (NK) cell alloreactivity [23, 84–86], and non-inherited maternal antigen (NIMA) mismatches (Table 2) [87–90].
Table 2.
Variables considered for best donor selection in unmanipulated haplo-SCT with ATG or TCR haplo-SCT with PT/Cy
| Variables | Unmanipulated haplo-SCT with ATG | Ref | TCR haplo-SCT with PT/Cy | Ref | |
|---|---|---|---|---|---|
| DSA | DSA was associated with primary graft failure, including GR and PGF. | [12] | DSA was associated with an increased risk of graft failure. | [93] | |
| Donor age | Young donor age (<30) was associated with decreased 2–4 acute GVHD, NRM, and superior survival. | [10] | No effect of donor age on clinical outcomes was found. | [59] | |
| Donor gender | F-M (versus others) correlated with higher incidence of 2–4 acute GVHD. | [10, 14] | Male donors were associated with less NRM and better survival. | [36, 102] | |
| NK alloreactivity | KIR-ligand mismatch was associated with inferior survival. | [23] | A survival benefit associated with donor-recipient mismatches of inhibitory KIR and KIR haplotype B donors. | [59] | |
| NIMA mismatch | NIMA-mismatched was associated with a lower incidence of acute GVHD in unmanipulated haplo-SCT. | [10] | – | ||
| Type of donor | Children | Children donors were associated with less acute GVHD than sibling donors. | [10] | – | |
| Mather | Maternal donors were associated with more acute GVHD, chronic GVHD, and NRM. | – | |||
| Older sister | Older sister donors were inferior to father donors in NRM and survival. | – | |||
| Father | Father donors were associated with less acute GVHD, less NRM, and better survival than mother donors. | – | |||
Haplo-SCT haploidentical stem cell transplantation, ATG anti-thymocyte globulin, TCR T-cell replete, PT/Cy posttransplant cyclophosphamide, Ref reference, DSA donor-specific anti-human leukocyte antibody, GR graft rejection, PGF poor graft function, NK natural killer, KIR inhibitory killer cell immunoglobulin-like receptor, NIMA non-inherited maternal antigen, GVHD graft-versus-host disease, NRM non-relapse mortality, F female, M male
– indicates no data available
DSA
The contribution of DSAs to the pathophysiology of graft failure (GF) has been confirmed in MUDT and in umbilical cord blood transplantation (UCBT) [91, 92]. In TCD haplo-SCT settings, Ciurea et al. [82] reported that three of four patients (75 %) that tested positive for pretransplant DSA (mean fluorescence intensity, MFI > 1500) failed to engraft, compared to 1 out of 20 patients (5 %) that tested DSA negative (P = 0.008), among 24 consecutive patients. In a study of 296 candidates for unmanipulated haplo-SCT with PT/Cy, the overall incidence of DSA was 15 %. Gladstone et al. [93] also found that DSA was associated with an increased risk of graft failure after transplantation. More recently, Chang et al. [12] reported that DSAs (MFI ≥ 10,000) were correlated to primary graft rejection (GR, P < 0.001) and that DSAs (MFI ≥ 2000) were strongly associated with poor graft function (PGF) in patients that received unmanipulated haplo-SCT with ATG. They also showed that primary GF, including GR and PGF, was associated with a significant increase in the incidence of TRM and with reduced DFS and OS [12, 20]. For patients with DSA, it is necessary to select a different donor. However, there is no generally accepted cutoff value for the mean fluorescence intensity of DSA in unmanipulated haplo-SCT with ATG [1, 52–55] or with PT/Cy [1, 36, 58, 59]. Overall, the association between DSA and graft failure was confirmed, both in TCD and in TCR haplo-SCT settings [12, 81, 82]. When a patient is positive for DSA (for example, DSA MFI ≥ 2000 in the Peking University Institute of Hematology), but the donor cannot be changed, a therapy must be given to target the DSA.
Currently in HSCT settings, desensitization methods have been applied, including plasma exchange, intravenous immunoglobulin, rituximab, and bortezomib [94, 95]. However, the efficacy of these strategies remains uncertain, due to the overall small number of patients treated and to the overall poor understanding of the mechanisms underlying DSA-mediated GF and PGF. Further elucidation of these mechanisms is essential to obtain critical insights into how desensitization approaches can be modified and what immuno-modifying therapies can be applied. That information will facilitate improvements in haplo-SCT outcomes.
In summary, DSA must be incorporated into the algorithm for haploidentical donor selection in unmanipulated haplo-SCT, with either the ATG or the PT/Cy modality. Therapies that target DSA might improve clinical outcomes for patients that are DSA positive and have only one haploidentical donor.
Donor age
In haplo-SCT with TCD, no effects of donor age were observed on transplant outcomes. In unmanipulated haplo-SCT, Wang et al. [10] found that transplants from younger donors (age ≤30 years) showed less non-relapse mortality (NRM) and better survival than those from older donors. In previous studies, we found that a high dose of CD34+ cells in haplo-allografts could promote platelet engraftment, and that CD3+CD4−CD8− T cells might contribute to a lower incidence of acute GVHD [96, 97]. More recently, researchers from Peking University also demonstrated that a young donor age (≤30 years) was associated with a higher count of CD34+ cells, CD3+CD4−CD8− T cells, and monocytes in G-BM, G-PB, and mixed allografts of G-BM and G-PB [56]. The impact of donor age was also confirmed by researchers from Korea in unmanipulated haplo-SCT with ATG [98]. They found that donor age (>40 years) was associated with a higher incidence of grades II–IV acute GVHD. More recently, Jaiswal et al. [99] reported that age-related clonal hematopoiesis was commonly associated with increases in hematologic cancer risk and all-cause mortality. Those findings strongly argued for the benefit of selecting younger donors to minimize transfers of clonal hematopoiesis [100].
In summary, younger donors are preferred in unmanipulated haplo-SCT, with ATG or PT/Cy.
Donor gender
For female donors, in general, age is correlated with parity. Older multiparous women may be the least-preferred donors for male recipients, due to the higher incidence of GVHD and the lower OS reported in some studies that focused on unrelated donor transplantations [101, 102]. Donor gender (female versus male) had adverse effects on the incidence of grades II–IV acute GVHD, both in unmanipulated haplo-SCT with PT/Cy and in TCR haplo-SCT with an ATG-based conditioning regimen [14, 36, 103]. Interestingly, in the largest study, the Peking University group showed that transplants from male donors were associated with significantly less NRM and better survival [10].
In summary, a male donor is preferred in unmanipulated haplo-SCT with ATG or with PT/Cy, due to the potential for superior survival.
ABO compatibility
In both HLA-matched and HLA-mismatched settings, allogeneic SCT that involves a major ABO incompatibility requires mononuclear cell separation to prevent a hemolytic reaction. This procedure reduces the transplanted cell dose and may increase the likelihood of graft failure [104, 105]. When possible, transplant donors should not be selected when they have major ABO incompatibilities, to avoid graft manipulations that might reduce the nucleated cell dose, particularly the CD34+ cell dose [97]. Our experience at Peking University showed that a low number of CD34+ cells (less than 2.19 × 106/kg) in the allograft was a critical factor associated with delayed platelet engraftment after unmanipulated haploidentical transplantation, in either adult or pediatric patients [97]. Those results suggested that, when no ABO-compatible donor was available, a donor with a minor ABO mismatch was preferable to a donor with a major mismatch, because the former was less likely to affect the number of hematopoietic stem cells infused. Thus, ensuring an adequate CD34+ cell dose in the allograft is the first step in promoting engraftment and decreasing the incidence of graft failure.
In summary, ABO compatibility should be considered when selecting the best donor in haplo-SCT with TCR; the order of selection should be ABO compatible, a minor ABO mismatch, and a major ABO mismatch.
Killer immunoglobulin-like receptor mismatches and NK cell alloreactivity
Biology of NK cells
NK cells play a central role in viral immunity and tumor immune surveillance. The activity of NK cells is regulated by a balance between activating and inhibiting killer immunoglobulin-like receptors (KIRs) [106]. KIRs are inherited as one of two basic KIR haplotypes, termed group A and group B. Group A haplotypes have a fixed number of genes that encode inhibitory receptors (with the exception of the activating receptor, KIR2DS4). Group B haplotypes have a variable number of genes, including additional activating receptor genes [84, 85].
Because KIR and HLA class I genes segregate to different chromosomes, a tolerance mechanism is required to prohibit the development of autoreactive NK cells. Only NK cells that express inhibitory receptors for self-HLA class I can acquire full functional competence, a process referred to as “education” or “licensing” [23]. In contrast, potentially autoreactive NK cells remain in a hyporesponsive state. Thus, NK cells that are “licensed” or “educated” (highly responsive to non-self cells) express inhibitory KIRs that specifically recognize self-HLA ligands [107, 108]. Examples of inhibitory KIRs include the well-defined KIR2DL2/3, specific for the HLA-Cw group-1 epitope; KIR2DL1, specific for the HLA-Cw group-2 epitope, and KIR3DL1, specific for the HLA-Bw4 epitope [84]. Thus, when educated NK cells confront an allogeneic target, their KIR does not recognize the allogeneic HLA as an inhibitory self-HLA ligand; the lack of the inhibitory ligand mediates NK “alloreactivity” (they attack cells that lack self-recognition molecules) [109–112]. In fact, alloreactive NK cells must only express KIRs that do not engage with any HLA class 1 molecules present on allogeneic target cells. Moreover, for effective alloreactivity, NK cells must also lack expression of CD94/NKG2A, because its inhibitory ligand, HLA-E, is present on all HLA class I-positive cells [87, 113, 114].
Role of NK cell alloreactivity in haplo-SCT
Ruggeri et al. [110] showed that alloreactive NK cells in a mouse model provided the following benefits: (1) elimination of recipient acute myeloid leukemia (AML) cells; (2) destruction of recipient T cells, which permitted a conditioning regimen with reduced toxicity; and (3) ablation of recipient dendritic cells that trigger GVHD, which protected the recipient from GVHD. In this study, the authors also found that increased NK cell alloreactivity in humans, based on the “missing self” model, was associated with a decreased rate of relapse and improved survival in patients with AML but not in patients with ALL. However, Symons et al. [115] failed to demonstrate a positive effect of alloreactive NK cells in patients that received haplo-SCT with PT/Cy. In contrast, Huang et al. [11] showed that a high relapse rate following haplo-SCT was associated with missing self molecules or missing ligands in the hosts.
The discordant results mentioned above may reflect differences in NK functional recovery, determined by the licensing process under different haplo-SCT settings, and/or differences in the presence of T cells in the stem cell graft. More interestingly, the researchers in Huang’s group demonstrated that the host MHC class I could determine NK cell responses, following unmanipulated haplo-SCT with ATG [11, 23]. The functional recovery of donor-derived NK cells was higher in recipients that expressed ligands for donor inhibitory KIRs, and high functional NK recovery correlated with better relapse control. Those results were consistent with previous studies, which suggested that T cells may influence NK cell function via presentation of MHC. Although it remains to be determined by what mechanism(s) the presence of T cells in the allograft influence NK cell licensing, they appear to be clinically relevant. Moreover, NK licensing was observed to have extremely relevant clinical implications, such as relapse and survival.
Symons et al. [115] showed that, in haplo-SCT with PT/Cy, patients with the KIR AA haplotype exhibited significantly higher OS and EFS, when the donor had a KIR Bx haplotype (mismatched) rather than the KIR AA haplotype (matched). In haplo-SCT with negative depletion of CD3/CD19 in allografts, the relapse incidence was significantly reduced in patients with a haplotype B donor, both in adults with hematological malignancies [116] and in children with ALL [117]. However, this phenomenon was not observed in the Perugia or the Peking University protocols, which suggested that the benefit of using donors with KIR B haplotypes was only observed with specific haplo-SCT modalities; however, the mechanisms underlying this phenomenon warrant further study.
In summary, NK cell alloreactivity and KIR haplotype should be considered when choosing the best donor. For patients that receive unmanipulated haplo-SCT with ATG, the best donor will have matching KIR expression. For patients that receive TCR haplo-SCT with PT/Cy, the best donor should have at least one KIR B haplotype.
NIMA mismatching
When a donor and recipient share inheritance of the paternal HLA haplotype, they are said to be mismatched for non-inherited maternal HLA antigens or NIMA (For more details, please see Fig. 1 in [86]). When a donor and recipient share inheritance of the maternal HLA haplotype, they are mismatched for non-inherited paternal HLA antigens or NIPA [88, 90, 118, 119]. Cells from NIMA-mismatched donors are expected to be less immunogenic than cells from NIPA-mismatched donors, because the contact between the immune systems of the mother and child during pregnancy diminishes the immune response of the child against NIMA. Using a mouse model, Aoyama et al. [87] demonstrated that the tolerogenic NIMA effect could be partly dependent on CD4+CD25+ regulatory T cells (Tregs). In TCR haplo-SCT, Wang et al. [10] and other researchers [88, 90, 120] showed that patients that received transplants from a NIMA-mismatched donor had a significantly lower incidence of acute GVHD than those that received transplants from a NIPA-mismatched donor. The Peking University group also found that immune recovery of naive Tregs was more rapid when patients received allografts from NIMA-mismatched donors than when they received allografts from NIPA-mismatched donors (unpublished data). That finding suggested that naive Tregs may play an important role in the tolerogenic NIMA effect. In addition, Kanda et al. [121] showed that a substantial proportion of long-term survivors after NIMA-mismatched haplo-SCT could discontinue the administration of immunosuppressive agents, despite the frequent occurrence of moderate to severe chronic GVHD. However, further studies are warranted to compare late sequelae between haplo-SCTs performed with NIMA- or NIPA-mismatched donors in a large, multicenter, prospective cohort.
Fig. 1.
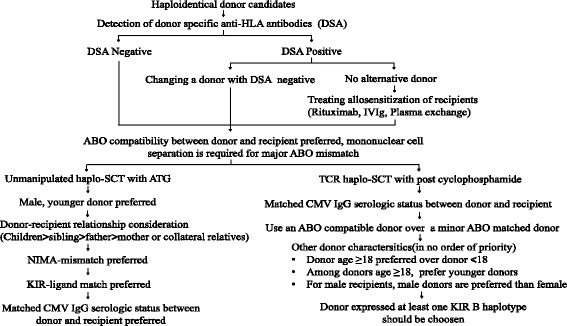
Algorithm for haploidentical donor selection in unmanipulated haplo-SCT with ATG and haplo-SCT with PT/Cy. Abbreviations: haplo-SCT haploidentical stem cell transplantation; ATG anti-thymocyte globulin; PT/Cy posttransplant cyclophosphamide; TCR T-cell replete; IVIg intravenous immunoglobulin; CMV cytomegalovirus; NIMA non-inherited maternal antigen; KIR inhibitory killer cell immunoglobulin-like receptor
Recently, Araki et al. [122] demonstrated that the number of cells that produced interferon-γ (IFN-γ) was significantly lower in a NIMA-exposed tolerance group than in a sensitization group, according to an MLR-ELISPOT assay in a murine model. That study raised the possibility that assays for measuring IFN-γ production in response to NIMA might be used clinically to predict the benefit of using NIMA-mismatched donors.
In summary, NIMA mismatching should be incorporated into the algorithm for selecting donors in unmanipulated haplo-SCT with ATG. The order of donor eligibility is first, NIMA mismatches, and second, NIPA mismatches.
Family relationship or type of donor
Given the fact that parents, children, siblings, and collateral relatives are all potential haploidentical donors [9, 16, 19, 22], the effects of these variables on clinical outcomes were investigated by several groups [1, 10, 70]. In unmanipulated haplo-SCT with ATG, results from Huang et al.’s group in Beijing demonstrated that transplants donated by fathers were associated with less NRM, less acute GVHD, and better survival compared to those donated by mothers [10]. Transplants donated by children were associated with less acute GVHD than those donated by siblings. Transplants donated by older sisters were inferior to those donated by fathers, with regard to NRM and survival. Moreover, transplants donated by mothers were associated with significantly more acute and chronic GVHD and TRM than NIMA-mismatched, but not NIPA-mismatched, transplants donated by siblings [10]. However, Stern et al. [70] observed a survival advantage in patients with ALL or AML that received TCD-allografts from haploidentical maternal donors. The above-mentioned opposite results in the two studies may be related to differences in the conditioning regimens, GVHD prophylaxis, and allografts between the two groups [10, 70]. Zhang et al. [60] found that, when haplo-SCT was performed with collateral-related haploidentical donors (CRDs) or with immediate-related donors (IRDs), the 3-year probability of OS and LFS was similar, but the 2-year incidence of extensive chronic GVHD was significantly higher with CRDs than with IRDs (36.7 % versus 20.2 %, P = 0.03) [60]. The effects of donor-recipient relationships (parents or siblings) on TRM and LFS were also confirmed in patients with AML that received haplo-SCT with TCD [69].
In summary, the family relationship of a donor should be incorporated in the algorithm for selecting the best donor in unmanipulated haplo-SCT with ATG. The order of donor eligibility among relatives should be child, younger brother, older sister, father, mother, and a collateral relative [10].
Donor and recipient serum CMV status
The effects of donor and recipient serum CMV status on clinical outcomes were demonstrated in HLA-matched transplantation settings [123]. Considering the effects of CMV status on outcomes [19, 69, 123], a group from Johns Hopkins [124] suggested that donors should have a CMV IgG serologic status similar to that of recipients. However, Wang et al. [9, 10] found that donor-recipient CMV serostatus matching was not associated with transplant outcomes. This discrepancy may be related to the higher incidence of CMV infections in Chinese compared to Western populations. Therefore, the effects of donor and recipient CMV status on haplo-SCT outcomes should be evaluated in a prospective, multicenter study.
In summary, donor and recipient CMV serostatus should be considered when choosing the best donor in unmanipulated haplo-SCT, particularly when patients receive haplo-SCT with PT/Cy; however, further study is needed to confirm the findings.
Recommendations
Presently, a number of donor-related factors have been identified that affect haplo-SCT outcomes. These factors should be considered when selecting the best donor. Here, we have listed some expert opinions, based on available data from original literature:
HLA matching: The effects of HLA disparity on transplantation outcomes has vanished, due to the improved approaches of unmanipulated haplo-SCT with ATG and haplo-SCT with PT/Cy.
Donor-specific antibodies: DSA must be incorporated in the algorithm for haploidentical donor selection, both in unmanipulated haplo-SCT with ATG and in haplo-SCT with PT/Cy. Procedures to reduce DSA prior to transplantation should be considered for patients that have DSA against potential haploidentical donors.
ABO compatibility: ABO compatibility should be considered in both unmanipulated haplo-SCT with ATG and haplo-SCT with PT/Cy.
Serum CMV status: Among haploidentical donors, donor and recipient CMV serostatus should be considered, in both unmanipulated haplo-SCT with ATG and haplo-SCT with PT/Cy.
Donor age: Among haploidentical donors, young males should be considered optimal, in both unmanipulated haplo-SCT with ATG and haplo-SCT with PT/Cy.
Family relationship: Family relationships should be considered in unmanipulated haplo-SCT with ATG-based conditioning, with the following order of donor preference: child, younger brother, older sister or father, older sibling, mother, and collateral relatives.
NIMA mismatches: NIMA mismatching should be incorporated into the algorithm for donor selection in unmanipulated haplo-SCT with the ATG protocol. The order of donor eligibility should be NIMA mismatches, followed by NIPA mismatches.
NK cell alloreactivity: NK cell alloreactivity should be considered in choosing a donor for both unmanipulated haplo-SCT with ATG and haplo-SCT with PT/Cy.
According to these recommendations, we have proposed an algorithm for haploidentical donor selection (Fig. 1). When choosing the best haploidentical donor, one should keep the following caveats in mind. First, there is not a generally accepted haplo-SCT protocol that can be used in all transplant centers; therefore, a single variable (such as NK alloreactivity) may have different effects on clinical outcomes in patients that receive different haplo-SCT protocols [10, 19, 34, 36, 59, 70, 72, 77, 100, 125]. Second, with improvements in haplo-SCT modalities, the impact of some variables (such as HLA-locus mismatches) on transplant outcomes may vanish. Third, with increasing numbers of haplo-SCT cases, and with updated analyses of donor-related variables associated with transplant outcomes, some new factors may emerge [126, 127].
Conclusions
Presently, TCR haplo-SCT modalities, particularly unmanipulated haplo-SCT with ATG or haplo-SCT with PT/Cy, have been widely accepted as a viable alternative for patients with no HLA-identical donor [1, 5, 6, 9, 10, 34–36, 72, 77, 128, 129]. Despite the challenges in promoting hematopoietic engraftment, in enhancing GVL effects, and in the lack of one universal haplo-SCT modality for most transplant centers, current evidence has indicated that selecting a best donor can improve transplant outcomes [10, 36, 59, 77, 81, 82, 115, 116, 130]. Therefore, employment of the currently available factors, including DSA, donor age, KIR-ligand mismatching, and NIMA mismatching, for guiding treatment is an accepted option in most centers [10, 36, 59, 77, 82, 100, 115, 116, 130]. Many recent excellent studies have advocated that donor selection should be incorporated into clinical trials. Although much work remains to be done, such as who is the best donor in subgroup patients (for example, high-risk AML), we believe that the best donor should be selected according to currently available knowledge, in combination with individualized conditioning regimens [46], optimal allografts [57], and stratification-directed GVHD prophylaxis, relapse prophylaxis, and treatment [131, 132]. This selection strategy will improve transplant outcomes, both in unmanipulated haplo-SCT with ATG and haplo-SCT with PT/Cy.
Acknowledgements
This work was supported (in part) by the National High Technology Research and Development Program of China (Program 863) (Grant No. 2013AA020401), the Milstein Medical Asian American Partnership Foundation, The Key Program of the National Natural Science Foundation of China (Grant No. 81230013), the Scientific Research Foundation for Capital Medicine Development (Grant No. 2011-4022-08), and the National Cancer Institute of the National Institutes of Health (CA 015396), USA. We would also like to thank San Francisco Edit (www.sefedit.net) for assistance in editing this manuscript.
Footnotes
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
X-JH designed the study. Y-JC, X-JH, and LL collected the data. Y-JC, X-JH, LL, and EJF analyzed the data and wrote the manuscript. All authors contributed to data interpretation and manuscript preparation. All authors read and approved the final manuscript.
References
- 1.Kanakry CG, Fuchs EJ, Luznik L. Modern approaches to HLA-haploidentical blood or marrow transplantation. Nat Rev Clin Oncol. 2016;13(2):132. doi: 10.1038/nrclinonc.2015.234. [DOI] [PubMed] [Google Scholar]
- 2.Arai Y, Aoki K, Takeda J, et al. Clinical significance of high-dose cytarabine added to cyclophosphamide/total-body irradiation in bone marrow or peripheral blood stem cell transplantation for myeloid malignancy. J Hematol Oncol. 2015;8:102. doi: 10.1186/s13045-015-0201-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Baron F, Labopin M, Ruggeri A, et al. Unrelated cord blood transplantation for adult patients with acute myeloid leukemia: higher incidence of acute graft-versus-host disease and lower survival in male patients transplanted with female unrelated cord blood—a report from Eurocord, the Acute Leukemia Working Party, and the Cord Blood Committee of the Cellular Therapy and Immunobiology Working Party of the European Group for Blood and Marrow Transplantation. J Hematol Oncol. 2015;8(1):107. doi: 10.1186/s13045-015-0207-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Baron F, Zachee P, Maertens J, et al. Non-myeloablative allogeneic hematopoietic cell transplantation following fludarabine plus 2 Gy TBI or ATG plus 8 Gy TLI: a phase II randomized study from the Belgian Hematological Society. J Hematol Oncol. 2015;8:4. doi: 10.1186/s13045-014-0098-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Chang YJ, Huang XJ. Haploidentical bone marrow transplantation without T-cell depletion. Semin Oncol. 2012;39(6):653–663. doi: 10.1053/j.seminoncol.2012.09.003. [DOI] [PubMed] [Google Scholar]
- 6.Chang YJ, Huang XJ. Haploidentical hematopoietic stem cell transplantation with unmanipulated granulocyte colony stimulating factor mobilized marrow and blood grafts. Curr Opin Hematol. 2012;19(6):454–461. doi: 10.1097/MOH.0b013e3283582322. [DOI] [PubMed] [Google Scholar]
- 7.Lai YR, Chen YH, Hu DM, et al. Multicenter phase II study of a combination of cyclosporine a, methotrexate and mycophenolate mofetil for GVHD prophylaxis: results of the Chinese Bone Marrow Transplant Cooperative Group (CBMTCG) J Hematol Oncol. 2014;7:59. doi: 10.1186/s13045-014-0059-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Reisner Y, Hagin D, Martelli MF. Haploidentical hematopoietic transplantation: current status and future perspectives. Blood. 2011;118(23):6006–6017. doi: 10.1182/blood-2011-07-338822. [DOI] [PubMed] [Google Scholar]
- 9.Wang Y, Liu DH, Liu KY, et al. Long-term follow-up of haploidentical hematopoietic stem cell transplantation without in vitro T cell depletion for the treatment of leukemia: nine years of experience at a single center. Cancer. 2013;119(5):978–985. doi: 10.1002/cncr.27761. [DOI] [PubMed] [Google Scholar]
- 10.Wang Y, Chang YJ, Xu LP, et al. Who is the best donor for a related HLA haplotype-mismatched transplant? Blood. 2014;124(6):843–850. doi: 10.1182/blood-2014-03-563130. [DOI] [PubMed] [Google Scholar]
- 11.Huang XJ, Zhao XY, Liu DH, Liu KY, Xu LP. Deleterious effects of KIR ligand incompatibility on clinical outcomes in haploidentical hematopoietic stem cell transplantation without in vitro T-cell depletion. Leukemia. 2007;21(4):848–851. doi: 10.1038/sj.leu.2404566. [DOI] [PubMed] [Google Scholar]
- 12.Chang YJ, Zhao XY, Xu LP, et al. Donor-specific anti-human leukocyte antigen antibodies were associated with primary graft failure after unmanipulated haploidentical blood and marrow transplantation: a prospective study with randomly assigned training and validation sets. J Hematol Oncol. 2015;8:84. doi: 10.1186/s13045-015-0182-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Handgretinger R. Haploidentical transplantation: the search for the best donor. Blood. 2014;124(6):827–828. doi: 10.1182/blood-2014-06-582460. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Luo Y, Xiao H, Lai X, et al. T-cell-replete haploidentical HSCT with low-dose anti-T-lymphocyte globulin compared with matched sibling HSCT and unrelated HSCT. Blood. 2014;124(17):2735–2743. doi: 10.1182/blood-2014-04-571570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Martelli MF, Di Ianni M, Ruggeri L, et al. “Designed” grafts for HLA-haploidentical stem cell transplantation. Blood. 2014;123(7):967–973. doi: 10.1182/blood-2013-10-531764. [DOI] [PubMed] [Google Scholar]
- 16.Ciurea SO, Bayraktar UD. “No donor”? Consider a haploidentical transplant. Blood Rev. 2015;29(2):63–70. doi: 10.1016/j.blre.2014.09.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gorin NC, Labopin M, Piemontese S, et al. T-cell-replete haploidentical transplantation versus autologous stem cell transplantation in adult acute leukemia: a matched pair analysis. Haematologica. 2015;100(4):558–564. doi: 10.3324/haematol.2014.111450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mancusi A, Ruggeri L, Urbani E, et al. Haploidentical hematopoietic transplantation from KIR ligand-mismatched donors with activating KIRs reduces non-relapse mortality. Blood. 2015;125(20):3173–3182. doi: 10.1182/blood-2014-09-599993. [DOI] [PubMed] [Google Scholar]
- 19.Peccatori J, Forcina A, Clerici D, et al. Sirolimus-based graft-versus-host disease prophylaxis promotes the in vivo expansion of regulatory T cells and permits peripheral blood stem cell transplantation from haploidentical donors. Leukemia. 2015;29(2):396–405. doi: 10.1038/leu.2014.180. [DOI] [PubMed] [Google Scholar]
- 20.Sun YQ, He GL, Chang YJ, et al. The incidence, risk factors, and outcomes of primary poor graft function after unmanipulated haploidentical stem cell transplantation. Ann Hematol. 2015;94(10):1699–1705. doi: 10.1007/s00277-015-2440-x. [DOI] [PubMed] [Google Scholar]
- 21.Sun YQ, Wang J, Jiang Q, et al. Haploidentical hematopoietic SCT may be superior to conventional consolidation/maintenance chemotherapy as post-remission therapy for high-risk adult ALL. Bone Marrow Transplant. 2015;50(1):20–25. doi: 10.1038/bmt.2014.195. [DOI] [PubMed] [Google Scholar]
- 22.Wang Y, Liu QF, Xu LP, et al. Haploidentical vs identical-sibling transplant for AML in remission: a multicenter, prospective study. Blood. 2015;125(25):3956–3962. doi: 10.1182/blood-2015-02-627786. [DOI] [PubMed] [Google Scholar]
- 23.Zhao XY, Chang YJ, Zhao XS, et al. Recipient expression of ligands for donor inhibitory KIRs enhances NK-cell function to control leukemic relapse after haploidentical transplantation. Eur J Immunol. 2015;45(8):2396–2408. doi: 10.1002/eji.201445057. [DOI] [PubMed] [Google Scholar]
- 24.Chang YJ, Huang XJ. Haploidentical SCT: the mechanisms underlying the crossing of HLA barriers. Bone Marrow Transplant. 2014;49(7):873–879. doi: 10.1038/bmt.2014.19. [DOI] [PubMed] [Google Scholar]
- 25.Xiao-Jun H, Lan-Ping X, Kai-Yan L, et al. Partially matched related donor transplantation can achieve outcomes comparable with unrelated donor transplantation for patients with hematologic malignancies. Clin Cancer Res. 2009;15(14):4777–4783. doi: 10.1158/1078-0432.CCR-09-0691. [DOI] [PubMed] [Google Scholar]
- 26.Or-Geva N, Reisner Y. The evolution of T-cell depletion in haploidentical stem-cell transplantation. Br J Haematol. 2016;172(5):667–84. doi: 10.1111/bjh.13868. [DOI] [PubMed] [Google Scholar]
- 27.Shabbir-Moosajee M, Lombardi L, Ciurea SO. An overview of conditioning regimens for haploidentical stem cell transplantation with post-transplantation cyclophosphamide. Am J Hematol. 2015;90(6):541–548. doi: 10.1002/ajh.23995. [DOI] [PubMed] [Google Scholar]
- 28.Bertaina A, Merli P, Rutella S, et al. HLA-haploidentical stem cell transplantation after removal of alphabeta + T and B-cells in children with non-malignant disorders. Blood. 2014;124(5):822–826. doi: 10.1182/blood-2014-03-563817. [DOI] [PubMed] [Google Scholar]
- 29.Shin SH, Kim JH, Jeon YW, et al. Feasible outcomes of T cell-replete haploidentical stem cell transplantation with reduced-intensity conditioning in patients with myelodysplastic syndrome. Biol Blood Marrow Transplant. 2015;21(2):342–349. doi: 10.1016/j.bbmt.2014.10.031. [DOI] [PubMed] [Google Scholar]
- 30.Wang Z, Zheng X, Yan H, Li D, Wang H. Good outcome of haploidentical hematopoietic SCT as a salvage therapy in children and adolescents with acquired severe aplastic anemia. Bone Marrow Transplant. 2014;49(12):1481–1485. doi: 10.1038/bmt.2014.187. [DOI] [PubMed] [Google Scholar]
- 31.Yan CH, Jiang Q, Wang J, et al. Superior survival of unmanipulated haploidentical hematopoietic stem cell transplantation compared with chemotherapy alone used as post-remission therapy in adults with standard-risk acute lymphoblastic leukemia in first complete remission. Biol Blood Marrow Transplant. 2014;20(9):1314–1321. doi: 10.1016/j.bbmt.2014.04.011. [DOI] [PubMed] [Google Scholar]
- 32.Zecca M, Strocchio L, Pagliara D, et al. HLA-haploidentical T cell-depleted allogeneic hematopoietic stem cell transplantation in children with Fanconi anemia. Biol Blood Marrow Transplant. 2014;20(4):571–576. doi: 10.1016/j.bbmt.2014.01.015. [DOI] [PubMed] [Google Scholar]
- 33.Esteves I, Bonfim C, Pasquini R, et al. Haploidentical BMT and post-transplant Cy for severe aplastic anemia: a multicenter retrospective study. Bone Marrow Transplant. 2015;50(5):685–689. doi: 10.1038/bmt.2015.20. [DOI] [PubMed] [Google Scholar]
- 34.Huang W, Li H, Gao C, et al. Unmanipulated HLA-mismatched/haploidentical peripheral blood stem cell transplantation for high-risk hematologic malignancies. Transfusion. 2012;52(6):1354–62. doi: 10.1111/j.1537-2995.2011.03478.x. [DOI] [PubMed] [Google Scholar]
- 35.Wang M, Dong YJ, Qiu ZX, et al. HLA disparity is not crucial for the survival rate and severity of chronic health conditions in adult recipients following family donor hematopoietic stem cell transplantation. Int J Hematol. 2015;101(1):75–82. doi: 10.1007/s12185-014-1691-y. [DOI] [PubMed] [Google Scholar]
- 36.McCurdy SR, Kanakry JA, Showel MM, et al. Risk-stratified outcomes of nonmyeloablative HLA-haploidentical BMT with high-dose posttransplantation cyclophosphamide. Blood. 2015;125(19):3024–3031. doi: 10.1182/blood-2015-01-623991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Bacigalupo A, Dominietto A, Ghiso A, et al. Unmanipulated haploidentical bone marrow transplantation and post-transplant cyclophosphamide for hematologic malignancies following a myeloablative conditioning: an update. Bone Marrow Transplant. 2015;50:S37–S39. doi: 10.1038/bmt.2015.93. [DOI] [PubMed] [Google Scholar]
- 38.Raiola AM, Dominietto A, di Grazia C, et al. Unmanipulated haploidentical transplants compared with other alternative donors and matched sibling grafts. Biol Blood Marrow Transplant. 2014;20(10):1573–1579. doi: 10.1016/j.bbmt.2014.05.029. [DOI] [PubMed] [Google Scholar]
- 39.Gao L, Zhang C, Gao L, et al. Favorable outcome of haploidentical hematopoietic stem cell transplantation in Philadelphia chromosome-positive acute lymphoblastic leukemia: a multicenter study in Southwest China. J Hematol Oncol. 2015;8:90. doi: 10.1186/s13045-015-0186-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Ballen KK, Koreth J, Chen YB, Dey BR, Spitzer TR. Selection of optimal alternative graft source: mismatched unrelated donor, umbilical cord blood, or haploidentical transplant. Blood. 2012;119(9):1972–1980. doi: 10.1182/blood-2011-11-354563. [DOI] [PubMed] [Google Scholar]
- 41.Luznik L, O’Donnell PV, Fuchs EJ. Post-transplantation cyclophosphamide for tolerance induction in HLA-haploidentical bone marrow transplantation. Semin Oncol. 2012;39(6):683–693. doi: 10.1053/j.seminoncol.2012.09.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Martelli MF, Di Ianni M, Ruggeri L, et al. HLA-haploidentical transplantation with regulatory and conventional T-cell adoptive immunotherapy prevents acute leukemia relapse. Blood. 2014;124(4):638–644. doi: 10.1182/blood-2014-03-564401. [DOI] [PubMed] [Google Scholar]
- 43.Ciurea SO, Mulanovich V, Saliba RM, et al. Improved early outcomes using a T cell replete graft compared with T cell depleted haploidentical hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2012;18(12):1835–1844. doi: 10.1016/j.bbmt.2012.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Huang XJ, Zhu HH, Chang YJ, et al. The superiority of haploidentical related stem cell transplantation over chemotherapy alone as postremission treatment for patients with intermediate- or high-risk acute myeloid leukemia in first complete remission. Blood. 2012;119(23):5584–5590. doi: 10.1182/blood-2011-11-389809. [DOI] [PubMed] [Google Scholar]
- 45.Mo XD, Xu LP, Zhang XH, et al. Haploidentical hematopoietic stem cell transplantation in adults with Philadelphia-negative acute lymphoblastic leukemia: no difference in the high- and low-risk groups. Int J Cancer. 2015;136(7):1697–1707. doi: 10.1002/ijc.29146. [DOI] [PubMed] [Google Scholar]
- 46.Sun YQ, Xu LP, Zhang XH, et al. A retrospective comparison of BU-fludarabine and BU-CY regimens in elderly patients or in patients with comorbidities who received unmanipulated haploidentical hematopoietic SCT. Bone Marrow Transplant. 2015;50(4):601–603. doi: 10.1038/bmt.2014.303. [DOI] [PubMed] [Google Scholar]
- 47.Rutella S, Zavala F, Danese S, Kared H, Leone G. Granulocyte colony-stimulating factor: a novel mediator of T cell tolerance. J Immunol. 2005;175(11):7085–7091. doi: 10.4049/jimmunol.175.11.7085. [DOI] [PubMed] [Google Scholar]
- 48.Jun HX, Jun CY, Yu ZX. In vivo induction of T-cell hyporesponsiveness and alteration of immunological cells of bone marrow grafts using granulocyte colony-stimulating factor. Haematologica. 2004;89(12):1517–1524. [PubMed] [Google Scholar]
- 49.Lv M, Zhao XS, Hu Y, et al. Monocytic and promyelocytic myeloid-derived suppressor cells may contribute to G-CSF-induced immune tolerance in haplo-identical allogeneic hematopoietic stem cell transplantation. Am J Hematol. 2015;90(1):E9–E16. doi: 10.1002/ajh.23865. [DOI] [PubMed] [Google Scholar]
- 50.Franzke A, Piao W, Lauber J, et al. G-CSF as immune regulator in T cells expressing the G-CSF receptor: implications for transplantation and autoimmune diseases. Blood. 2003;102(2):734–739. doi: 10.1182/blood-2002-04-1200. [DOI] [PubMed] [Google Scholar]
- 51.D’Aveni M, Rossignol J, Coman T, et al. G-CSF mobilizes CD34+ regulatory monocytes that inhibit graft-versus-host disease. Sci Transl Med. 2015;7(281):281ra242. doi: 10.1126/scitranslmed.3010435. [DOI] [PubMed] [Google Scholar]
- 52.Huang XJ, Liu DH, Liu KY, et al. Haploidentical hematopoietic stem cell transplantation without in vitro T-cell depletion for the treatment of hematological malignancies. Bone Marrow Transplant. 2006;38(4):291–297. doi: 10.1038/sj.bmt.1705445. [DOI] [PubMed] [Google Scholar]
- 53.Huang XJ, Liu DH, Liu KY, et al. Treatment of acute leukemia with unmanipulated HLA-mismatched/haploidentical blood and bone marrow transplantation. Biol Blood Marrow Transplant. 2009;15(2):257–265. doi: 10.1016/j.bbmt.2008.11.025. [DOI] [PubMed] [Google Scholar]
- 54.Lu DP, Dong L, Wu T, et al. Conditioning including antithymocyte globulin followed by unmanipulated HLA-mismatched/haploidentical blood and marrow transplantation can achieve comparable outcomes with HLA-identical sibling transplantation. Blood. 2006;107(8):3065–3073. doi: 10.1182/blood-2005-05-2146. [DOI] [PubMed] [Google Scholar]
- 55.Huang XJ, Chang YJ. Unmanipulated HLA-mismatched/haploidentical blood and marrow hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2011;17(2):197–204. doi: 10.1016/j.bbmt.2010.03.006. [DOI] [PubMed] [Google Scholar]
- 56.Lee KH, Lee JH, Kim DY, et al. Reduced-intensity conditioning therapy with busulfan, fludarabine, and antithymocyte globulin for HLA-haploidentical hematopoietic cell transplantation in acute leukemia and myelodysplastic syndrome. Blood. 2011;118(9):2609–2617. doi: 10.1182/blood-2011-02-339838. [DOI] [PubMed] [Google Scholar]
- 57.Di Bartolomeo P, Santarone S, De Angelis G, et al. Haploidentical, unmanipulated, G-CSF-primed bone marrow transplantation for patients with high-risk hematologic malignancies. Blood. 2013;121(5):849–857. doi: 10.1182/blood-2012-08-453399. [DOI] [PubMed] [Google Scholar]
- 58.Luznik L, O’Donnell PV, Symons HJ, et al. HLA-haploidentical bone marrow transplantation for hematologic malignancies using nonmyeloablative conditioning and high-dose, posttransplantation cyclophosphamide. Biol Blood Marrow Transplant. 2008;14(6):641–650. doi: 10.1016/j.bbmt.2008.03.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Kasamon YL, Luznik L, Leffell MS, et al. Nonmyeloablative HLA-haploidentical bone marrow transplantation with high-dose posttransplantation cyclophosphamide: effect of HLA disparity on outcome. Biol Blood Marrow Transplant. 2010;16(4):482–489. doi: 10.1016/j.bbmt.2009.11.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Zhang YY, Liu DH, Liu KY, et al. HLA-haploidentical hematopoietic SCT from collateral related donors without in vitro T-cell depletion for hematological malignancies. Bone Marrow Transplant. 2014;49(4):496–501. doi: 10.1038/bmt.2013.223. [DOI] [PubMed] [Google Scholar]
- 61.Solomon SR, Sizemore CA, Sanacore M, et al. TBI-based myeloablative haploidentical stem cell transplantation is a safe and effective alternative to unrelated donor transplantation in patients without matched sibling donors. Biol Blood Marrow Transplant. 2015;21(7):1299–1307. doi: 10.1016/j.bbmt.2015.03.003. [DOI] [PubMed] [Google Scholar]
- 62.Ciurea SO, Zhang MJ, Bacigalupo AA, et al. Haploidentical transplant with post-transplant cyclophosphamide versus matched unrelated donor transplant for acute myeloid leukemia. Blood. 2015;126(8):1033–1040. doi: 10.1182/blood-2015-04-639831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Kasamon YL, Bolanos-Meade J, Prince GT, et al. Outcomes of nonmyeloablative HLA-haploidentical blood or marrow transplantation with high-dose post-transplantation cyclophosphamide in older adults. J Clin Oncol. 2015;33(28):3152–3161. doi: 10.1200/JCO.2014.60.4777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Cieri N, Greco R, Crucitti L, et al. Post-transplantation cyclophosphamide and sirolimus after haploidentical hematopoietic stem cell transplantation using a treosulfan-based myeloablative conditioning and peripheral blood stem cells. Biol Blood Marrow Transplant. 2015;21(8):1506–1514. doi: 10.1016/j.bbmt.2015.04.025. [DOI] [PubMed] [Google Scholar]
- 65.Ciceri F, Lupo-Stanghellini MT, Korthof ET, et al. Haploidentical transplantation in patients with acquired aplastic anemia. Bone Marrow Transplant. 2013;48(2):183–5. doi: 10.1038/bmt.2012.231. [DOI] [PubMed] [Google Scholar]
- 66.Gao L, Li Y, Zhang Y, et al. Long-term outcome of HLA-haploidentical hematopoietic SCT without in vitro T-cell depletion for adult severe aplastic anemia after modified conditioning and supportive therapy. Bone Marrow Transplant. 2014;49(4):519–524. doi: 10.1038/bmt.2013.224. [DOI] [PubMed] [Google Scholar]
- 67.El-Cheikh J, Crocchiolo R, Furst S, et al. Unrelated cord blood compared with haploidentical grafts in patients with hematological malignancies. Cancer. 2015;121(11):1809–1816. doi: 10.1002/cncr.29271. [DOI] [PubMed] [Google Scholar]
- 68.Kekre N, Antin JH. Hematopoietic stem cell transplantation donor sources in the 21st century: choosing the ideal donor when a perfect match doesn’t exist. Blood. 2014;124(3):334–343. doi: 10.1182/blood-2014-02-514760. [DOI] [PubMed] [Google Scholar]
- 69.Ciceri F, Labopin M, Aversa F, et al. A survey of fully haploidentical hematopoietic stem cell transplantation in adults with high-risk acute leukemia: a risk factor analysis of outcomes for patients in remission at transplantation. Blood. 2008;112(9):3574–3581. doi: 10.1182/blood-2008-02-140095. [DOI] [PubMed] [Google Scholar]
- 70.Stern M, Ruggeri L, Mancusi A, et al. Survival after T cell-depleted haploidentical stem cell transplantation is improved using the mother as donor. Blood. 2008;112(7):2990–2995. doi: 10.1182/blood-2008-01-135285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Moscardo F, Romero S, Sanz J, et al. T cell-depleted related HLA-mismatched peripheral blood stem cell transplantation as salvage therapy for graft failure after single unit unrelated donor umbilical cord blood transplantation. Biol Blood Marrow Transplant. 2014;20(7):1060–1063. doi: 10.1016/j.bbmt.2014.03.024. [DOI] [PubMed] [Google Scholar]
- 72.Wang Y, Fu HX, Liu DH, et al. Influence of two different doses of antithymocyte globulin in patients with. standard-risk disease following haploidentical transplantation: a randomized trial. Bone Marrow Transplant. 2014;49(3):426–33. doi: 10.1038/bmt.2013.191. [DOI] [PubMed] [Google Scholar]
- 73.Anasetti C, Beatty PG, Storb R, et al. Effect of HLA incompatibility on graft-versus-host disease, relapse, and survival after marrow transplantation for patients with leukemia or lymphoma. Hum Immunol. 1990;29(2):79–91. doi: 10.1016/0198-8859(90)90071-V. [DOI] [PubMed] [Google Scholar]
- 74.Szydlo R, Goldman JM, Klein JP, et al. Results of allogeneic bone marrow transplants for leukemia using donors other than HLA-identical siblings. J Clin Oncol. 1997;15(5):1767–1777. doi: 10.1200/JCO.1997.15.5.1767. [DOI] [PubMed] [Google Scholar]
- 75.Chang YJ, Zhao XY, Huang XJ. Immune reconstitution after haploidentical hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2014;20(4):440–449. doi: 10.1016/j.bbmt.2013.11.028. [DOI] [PubMed] [Google Scholar]
- 76.Mo XD, Zhao XY, Liu DH, et al. Umbilical cord blood transplantation and unmanipulated haploidentical hematopoietic SCT for pediatric hematologic malignances. Bone Marrow Transplant. 2014;49(8):1070–1075. doi: 10.1038/bmt.2014.109. [DOI] [PubMed] [Google Scholar]
- 77.Ikegame K, Yoshida T, Yoshihara S, et al. Unmanipulated haploidentical reduced-intensity stem cell transplantation using fludarabine, busulfan, low-dose antithymocyte globulin, and steroids for patients in non-complete remission or at high risk of relapse: a prospective multicenter phase I/II study in Japan. Biol Blood Marrow Transplant. 2015;21(8):1495–1505. doi: 10.1016/j.bbmt.2015.04.012. [DOI] [PubMed] [Google Scholar]
- 78.Lin X, Lu ZG, Song CY, et al. Long-term outcome of HLA-haploidentical hematopoietic stem cell transplantation without in vitro T-cell depletion based on an FBCA conditioning regimen for hematologic malignancies. Bone Marrow Transplant. 2015;50(8):1092–1097. doi: 10.1038/bmt.2015.108. [DOI] [PubMed] [Google Scholar]
- 79.Xiao-Jun H, Lan-Ping X, Kai-Yan L, et al. HLA-mismatched/haploidentical hematopoietic stem cell transplantation without in vitro T cell depletion for chronic myeloid leukemia: improved outcomes in patients in accelerated phase and blast crisis phase. Ann Med. 2008;40(6):444–455. doi: 10.1080/07853890801908903. [DOI] [PubMed] [Google Scholar]
- 80.Huo MR, Xu LP, Li D, et al. The effect of HLA disparity on clinical outcome after HLA-haploidentical blood and marrow transplantation. Clin Transplant. 2012;26(2):284–291. doi: 10.1111/j.1399-0012.2011.01499.x. [DOI] [PubMed] [Google Scholar]
- 81.Yoshihara S, Maruya E, Taniguchi K, et al. Risk and prevention of graft failure in patients with preexisting donor-specific HLA antibodies undergoing unmanipulated haploidentical SCT. Bone Marrow Transplant. 2012;47(4):508–515. doi: 10.1038/bmt.2011.131. [DOI] [PubMed] [Google Scholar]
- 82.Ciurea SO, de Lima M, Cano P, et al. High risk of graft failure in patients with anti-HLA antibodies undergoing haploidentical stem-cell transplantation. Transplantation. 2009;88(8):1019–1024. doi: 10.1097/TP.0b013e3181b9d710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Wang Y-T, Zhao X-Y, Zhao X-S, et al. The impact of donor characteristics on the immune cell composition of mixture allografts of granulocyte-colony-stimulating factor-mobilized marrow harvests and peripheral blood harvests. Transfusion. 2015;55(12):2874–2881. doi: 10.1111/trf.13251. [DOI] [PubMed] [Google Scholar]
- 84.Uhrberg M, Valiante NM, Shum BP, et al. Human diversity in killer cell inhibitory receptor genes. Immunity. 1997;7(6):753–763. doi: 10.1016/S1074-7613(00)80394-5. [DOI] [PubMed] [Google Scholar]
- 85.Parham P. MHC class I molecules and KIRs in human history, health and survival. Nat Rev Immunol. 2005;5(3):201–214. doi: 10.1038/nri1570. [DOI] [PubMed] [Google Scholar]
- 86.Moretta L, Locatelli F, Pende D, Marcenaro E, Mingari MC, Moretta A. Killer Ig-like receptor-mediated control of natural killer cell alloreactivity in haploidentical hematopoietic stem cell transplantation. Blood. 2011;117(3):764–771. doi: 10.1182/blood-2010-08-264085. [DOI] [PubMed] [Google Scholar]
- 87.Aoyama K, Koyama M, Matsuoka K, et al. Improved outcome of allogeneic bone marrow transplantation due to breastfeeding-induced tolerance to maternal antigens. Blood. 2009;113(8):1829–1833. doi: 10.1182/blood-2008-05-155283. [DOI] [PubMed] [Google Scholar]
- 88.Ichinohe T, Uchiyama T, Shimazaki C, et al. Feasibility of HLA-haploidentical hematopoietic stem cell transplantation between noninherited maternal antigen (NIMA)-mismatched family members linked with long-term fetomaternal microchimerism. Blood. 2004;104(12):3821–3828. doi: 10.1182/blood-2004-03-1212. [DOI] [PubMed] [Google Scholar]
- 89.Matsuoka K, Ichinohe T, Hashimoto D, Asakura S, Tanimoto M, Teshima T. Fetal tolerance to maternal antigens improves the outcome of allogeneic bone marrow transplantation by a CD4+ CD25+ T-cell-dependent mechanism. Blood. 2006;107(1):404–409. doi: 10.1182/blood-2005-07-3045. [DOI] [PubMed] [Google Scholar]
- 90.van Rood JJ, Loberiza FR, Jr, Zhang MJ, et al. Effect of tolerance to noninherited maternal antigens on the occurrence of graft-versus-host disease after bone marrow transplantation from a parent or an HLA-haploidentical sibling. Blood. 2002;99(5):1572–1577. doi: 10.1182/blood.V99.5.1572. [DOI] [PubMed] [Google Scholar]
- 91.Spellman S, Bray R, Rosen-Bronson S, et al. The detection of donor-directed, HLA-specific alloantibodies in recipients of unrelated hematopoietic cell transplantation is predictive of graft failure. Blood. 2010;115(13):2704–2708. doi: 10.1182/blood-2009-09-244525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Cutler C, Kim HT, Sun L, et al. Donor-specific anti-HLA antibodies predict outcome in double umbilical cord blood transplantation. Blood. 2011;118(25):6691–6697. doi: 10.1182/blood-2011-05-355263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Gladstone DE, Zachary AA, Fuchs EJ, et al. Partially mismatched transplantation and human leukocyte antigen donor-specific antibodies. Biol Blood Marrow Transplant. 2013;19(4):647–652. doi: 10.1016/j.bbmt.2013.01.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Yoshihara S, Taniguchi K, Ogawa H, Saji H. The role of HLA antibodies in allogeneic SCT: is the ‘type-and-screen’ strategy necessary not only for blood type but also for HLA? Bone Marrow Transplant. 2012;47(12):1499–1506. doi: 10.1038/bmt.2011.249. [DOI] [PubMed] [Google Scholar]
- 95.Jordan SC, Vo AA. Donor-specific antibodies in allograft recipients: etiology, impact and therapeutic approaches. Curr Opin Organ Transplant. 2014;19(6):591–597. doi: 10.1097/MOT.0000000000000128. [DOI] [PubMed] [Google Scholar]
- 96.Chang YJ, Xu LP, Liu DH, et al. Platelet engraftment in patients with hematologic malignancies following unmanipulated haploidentical blood and marrow transplantation: effects of CD34+ cell dose and disease status. Biol Blood Marrow Transplant. 2009;15(5):632–638. doi: 10.1016/j.bbmt.2009.02.001. [DOI] [PubMed] [Google Scholar]
- 97.Chang YJ, Xu LP, Liu DH, et al. The impact of CD34+ cell dose on platelet engraftment in pediatric patients following unmanipulated haploidentical blood and marrow transplantation. Pediatr Blood Cancer. 2009;53(6):1100–1106. doi: 10.1002/pbc.22159. [DOI] [PubMed] [Google Scholar]
- 98.Chen L, Chang YJ, Xu LP, et al. The impact of donor characteristics on the immune cell composition of second allografts in Chinese people. Vox Sang. 2016 Feb 25. doi: 10.1111/vox.12394. [Epub ahead of print]. [DOI] [PubMed]
- 99.Jaiswal S, Fontanillas P, Flannick J, et al. Age-related clonal hematopoiesis associated with adverse outcomes. N Engl J Med. 2014;371(26):2488–2498. doi: 10.1056/NEJMoa1408617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Ciurea SO, Champlin RE. Donor selection in T cell-replete haploidentical hematopoietic stem cell transplantation: knowns, unknowns, and controversies. Biol Blood Marrow Transplant. 2013;19(2):180–184. doi: 10.1016/j.bbmt.2012.08.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Kongtim P, Di Stasi A, Rondon G, et al. Can a female donor for a male recipient decrease the relapse rate for patients with acute myeloid leukemia treated with allogeneic hematopoietic stem cell transplantation? Biol Blood Marrow Transplant. 2015;21(4):713–719. doi: 10.1016/j.bbmt.2014.12.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Stern M, Brand R, de Witte T, et al. Female-versus-male alloreactivity as a model for minor histocompatibility antigens in hematopoietic stem cell transplantation. Am J Transplant. 2008;8(10):2149–2157. doi: 10.1111/j.1600-6143.2008.02374.x. [DOI] [PubMed] [Google Scholar]
- 103.Piemontese S, Ciceri F, Labopin M, et al. A survey on unmanipulated haploidentical hematopoietic stem cell transplantation in adults with acute leukemia. Leukemia. 2015;29(5):1069–1075. doi: 10.1038/leu.2014.336. [DOI] [PubMed] [Google Scholar]
- 104.Guttridge MG, Sidders C, Booth-Davey E, Pamphilon D, Watt SM. Factors affecting volume reduction and red blood cell depletion of bone marrow on the COBE Spectra cell separator before haematopoietic stem cell transplantation. Bone Marrow Transplant. 2006;38(3):175–181. doi: 10.1038/sj.bmt.1705420. [DOI] [PubMed] [Google Scholar]
- 105.Gajewski JL, Johnson VV, Sandler SG, Sayegh A, Klumpp TR. A review of transfusion practice before, during, and after hematopoietic progenitor cell transplantation. Blood. 2008;112(8):3036–3047. doi: 10.1182/blood-2007-10-118372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Vivier E, Raulet DH, Moretta A, et al. Innate or adaptive immunity? The example of natural killer cells. Science. 2011;331(6013):44–49. doi: 10.1126/science.1198687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Orr MT, Lanier LL. Natural killer cell education and tolerance. Cell. 2010;142(6):847–856. doi: 10.1016/j.cell.2010.08.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Joncker NT, Raulet DH. Regulation of NK cell responsiveness to achieve self-tolerance and maximal responses to diseased target cells. Immunol Rev. 2008;224:85–97. doi: 10.1111/j.1600-065X.2008.00658.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Ruggeri L, Mancusi A, Capanni M, et al. Donor natural killer cell allorecognition of missing self in haploidentical hematopoietic transplantation for acute myeloid leukemia: challenging its predictive value. Blood. 2007;110(1):433–440. doi: 10.1182/blood-2006-07-038687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Ruggeri L, Capanni M, Urbani E, et al. Effectiveness of donor natural killer cell alloreactivity in mismatched hematopoietic transplants. Science. 2002;295(5562):2097–2100. doi: 10.1126/science.1068440. [DOI] [PubMed] [Google Scholar]
- 111.Moretta A, Vitale M, Bottino C, et al. P58 molecules as putative receptors for major histocompatibility complex (MHC) class I molecules in human natural killer (NK) cells. Anti-p58 antibodies reconstitute lysis of MHC class I-protected cells in NK clones displaying different specificities. J Exp Med. 1993;178(2):597–604. doi: 10.1084/jem.178.2.597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Karre K. Natural killer cell recognition of missing self. Nat Immunol. 2008;9(5):477–480. doi: 10.1038/ni0508-477. [DOI] [PubMed] [Google Scholar]
- 113.Costello RT, Sivori S, Marcenaro E, et al. Defective expression and function of natural killer cell-triggering receptors in patients with acute myeloid leukemia. Blood. 2002;99(10):3661–3667. doi: 10.1182/blood.V99.10.3661. [DOI] [PubMed] [Google Scholar]
- 114.Bottino C, Castriconi R, Moretta L, Moretta A. Cellular ligands of activating NK receptors. Trends Immunol. 2005;26(4):221–226. doi: 10.1016/j.it.2005.02.007. [DOI] [PubMed] [Google Scholar]
- 115.Symons HJ, Leffell MS, Rossiter ND, Zahurak M, Jones RJ, Fuchs EJ. Improved survival with inhibitory killer immunoglobulin receptor (KIR) gene mismatches and KIR haplotype B donors after nonmyeloablative, HLA-haploidentical bone marrow transplantation. Biol Blood Marrow Transplant. 2010;16(4):533–542. doi: 10.1016/j.bbmt.2009.11.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Michaelis SU, Mezger M, Bornhauser M, et al. KIR haplotype B donors but not KIR-ligand mismatch result in a reduced incidence of relapse after haploidentical transplantation using reduced intensity conditioning and CD3/CD19-depleted grafts. Ann Hematol. 2014;93(9):1579–1586. doi: 10.1007/s00277-014-2084-2. [DOI] [PubMed] [Google Scholar]
- 117.Oevermann L, Michaelis SU, Mezger M, et al. KIR B haplotype donors confer a reduced risk for relapse after haploidentical transplantation in children with ALL. Blood. 2014;124(17):2744–2747. doi: 10.1182/blood-2014-03-565069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Obama K, Utsunomiya A, Takatsuka Y, Takemoto Y. Reduced-intensity non-T-cell depleted HLA-haploidentical stem cell transplantation for older patients based on the concept of feto-maternal tolerance. Bone Marrow Transplant. 2004;34(10):897–899. doi: 10.1038/sj.bmt.1704692. [DOI] [PubMed] [Google Scholar]
- 119.Ochiai N, Shimazaki C, Fuchida S, et al. Successful non-T cell-depleted HLA haplo-identical three-loci mismatched hematopoietic stem cell transplantation from mother to son based on the feto-maternal microchimerism in chronic myelogenous leukemia. Bone Marrow Transplant. 2002;30(11):793–796. doi: 10.1038/sj.bmt.1703736. [DOI] [PubMed] [Google Scholar]
- 120.Yahng SA, Kim JH, Jeon YW, et al. A well-tolerated regimen of 800 cGy TBI-fludarabine-busulfan-ATG for reliable engraftment after unmanipulated haploidentical peripheral blood stem cell transplantation in adult patients with acute myeloid leukemia. Biol Blood Marrow Transplant. 2015;21(1):119–129. doi: 10.1016/j.bbmt.2014.09.029. [DOI] [PubMed] [Google Scholar]
- 121.Kanda J, Ichinohe T, Shimazaki C, et al. Long-term survival after HLA-haploidentical SCT from noninherited maternal antigen-mismatched family donors: impact of chronic GVHD. Bone Marrow Transplant. 2009;44(5):327–329. doi: 10.1038/bmt.2009.18. [DOI] [PubMed] [Google Scholar]
- 122.Araki M, Hirayama M, Azuma E, et al. Prediction of reactivity to noninherited maternal antigen in MHC-mismatched, minor histocompatibility antigen-matched stem cell transplantation in a mouse model. J Immunol. 2010;185(12):7739–7745. doi: 10.4049/jimmunol.1001226. [DOI] [PubMed] [Google Scholar]
- 123.Boeckh M, Nichols WG, Papanicolaou G, Rubin R, Wingard JR, Zaia J. Cytomegalovirus in hematopoietic stem cell transplant recipients: current status, known challenges, and future strategies. Biol Blood Marrow Transplant. 2003;9(9):543–558. doi: 10.1016/S1083-8791(03)00287-8. [DOI] [PubMed] [Google Scholar]
- 124.Fuchs EJ, Luznik L. HLA-haploidentical hematopoietic cell transplantation. www.uptodate.com.
- 125.Federmann B, Bornhauser M, Meisner C, et al. Haploidentical allogeneic hematopoietic cell transplantation in adults using CD3/CD19 depletion and reduced intensity conditioning: a phase II study. Haematologica. 2012;97(10):1523–1531. doi: 10.3324/haematol.2011.059378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Shook DR, Triplett BM, Eldridge PW, Kang G, Srinivasan A, Leung W. Haploidentical stem cell transplantation augmented by CD45RA negative lymphocytes provides rapid engraftment and excellent tolerability. Pediatr Blood Cancer. 2015;62(4):666–673. doi: 10.1002/pbc.25352. [DOI] [PubMed] [Google Scholar]
- 127.Bleakley M, Heimfeld S, Loeb KR, et al. Outcomes of acute leukemia patients transplanted with naive T cell-depleted stem cell grafts. J Clin Invest. 2015;125(7):2677–2689. doi: 10.1172/JCI81229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Aversa F, Terenzi A, Tabilio A, et al. Full haplotype-mismatched hematopoietic stem-cell transplantation: a phase II study in patients with acute leukemia at high risk of relapse. J Clin Oncol. 2005;23(15):3447–3454. doi: 10.1200/JCO.2005.09.117. [DOI] [PubMed] [Google Scholar]
- 129.Bolanos-Meade J, Fuchs EJ, Luznik L, et al. HLA-haploidentical bone marrow transplantation with posttransplant cyclophosphamide expands the donor pool for patients with sickle cell disease. Blood. 2012;120(22):4285–4291. doi: 10.1182/blood-2012-07-438408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Pende D, Marcenaro S, Falco M, et al. Anti-leukemia activity of alloreactive NK cells in KIR ligand-mismatched haploidentical HSCT for pediatric patients: evaluation of the functional role of activating KIR and redefinition of inhibitory KIR specificity. Blood. 2009;113(13):3119–3129. doi: 10.1182/blood-2008-06-164103. [DOI] [PubMed] [Google Scholar]
- 131.Yan CH, Liu DH, Liu KY, et al. Risk stratification-directed donor lymphocyte infusion could reduce relapse of standard-risk acute leukemia patients after allogeneic hematopoietic stem cell transplantation. Blood. 2012;119(14):3256–3262. doi: 10.1182/blood-2011-09-380386. [DOI] [PubMed] [Google Scholar]
- 132.Zhu HH, Zhang XH, Qin YZ, et al. MRD-directed risk stratification treatment may improve outcomes of t(8;21) AML in the first complete remission: results from the AML05 multicenter trial. Blood. 2013;121(20):4056–4062. doi: 10.1182/blood-2012-11-468348. [DOI] [PubMed] [Google Scholar]