

Abstract
This study assessed social skills in post-institutionalized (PI) children with respect to age-at-adoption, age-at-assessment, and gender. Parent ratings of social skills (Social Skills Rating System) and behavior problems (Child Behavior Checklist) were obtained for 214 children and 127 adolescents who were adopted from socially-emotionally depriving Russian institutions. Results showed that children adopted before 18 months of age have better social skills than those adopted after this age; those assessed in childhood demonstrate better social skills than those assessed in adolescence. PI females, especially later-adopted adolescents, have particularly poor social skills. Children with poor social skills tend to have higher rates of behavior problems.
Keywords: Adopted Children, Age at Adoption, Behavior Problems, Psychosocial Development, Social Adjustment
During the first years of life, the caregiver-child relationship theoretically contributes to a number of “building blocks” that seem to form the foundation of later social behavior (Ainsworth, 1973; Bretherton & Munholland, 1999). Children who spend part of their early lives residing in an institution typically receive deficient early social-emotional care that may lead to poor social skills in childhood and adolescence.
When children have a consistent caregiver, they typically experience much social-emotional stimulation from the caregiver, likely the result of a caregiver’s attachment to the child. This frequent stimulation may promote the development of the child’s attachment to a caregiver, as well as a basic understanding of contingencies and social cues (Sroufe & Waters, 1977). Further, a reciprocal caregiver-child relationship may give children experience with how their behavior affects others. It is plausible that these basic skills—reading social cues, understanding contingencies, and developing a sense of agency—are fundamental to socially skilled behavior in childhood and adolescence.
A consistent caregiver is likely key to this process. In fact, for an infant to develop an attachment to a caregiver, the caregiver must behave sensitively and responsively and be a consistent presence in the infant’s life over a period of time (Thompson, 2006). A consistent caregiver provides repetitions of the same behavior patterns over time, making contingencies easier to learn and social cues easier to understand. Noticing these patterns of social behavior may be a crucial first step to developing social skills, and interactions with a sensitive, responsive, stable caregiver contribute to an infant’s development of an internal working model of social relationships.
Children who are reared in an institution lack many of the early experiences that contribute to the development of social understanding. Specifically, institutions tend to be characterized by many and changing caregivers who provide insensitive and unresponsive care (The St. Petersburg-USA Orphanage Research Team, 2005). Children usually live in same-age groups, so it is difficult for a caregiver to devote one-on-one attention to a child while other children are otherwise occupied. Care in institutions is rarely contingently responsive—caregivers’ actions are typically not responsive to a child’s cues.
Further, the institutional environment tends to encourage group conformity; children often eat, sleep, and play at specified times and in a prescribed manner with little room for creativity or flexibility. Even during playtime, caregiver-child interactions, when they occur, are predominantly adult-directed; children are shown the “right” way to play with toys and corrected if they deviate from that method. Thus, the institutional environment does not generally provide a consistent set of stable caregivers that in turn give children consistent experiences with social cues and interactions.
Even adopted children who did not experience institutional care may have a history of abuse or neglect that contributes to a socially-emotionally deficient early rearing environment. Further, while adoption moves a child to a qualitatively better home, it also involves breaking any attachment bonds a child may have had with caregivers before adoption, which can put a child at risk for problems later on (Brodzinsky, Schechter, Braff, & Singer, 1984). As adoptees enter childhood and adolescence, their increasing understanding of their adoption status and awareness of the stigma that can surround adoption can lead to adjustment problems (Brodzinsky, 1993).
Relatively little is known about the lasting consequences of not having an early stable caregiver and developing an early internal working model of social relationships on children’s later social functioning. Adopted children, and particularly those with a history of early institutional rearing, might experience social difficulties later in childhood and adolescence, and a longer duration of residence in a socially-emotionally depriving institution may relate to increased social difficulties.
Social and Behavioral Functioning of Adopted Children
In fact, while most adopted children fall in the normal range of adjustment, they do show higher rates of problems than never-institutionalized parent-reared children in a variety of domains. For instance, PI children tend to have poorer cognitive development and academic achievement, stunted physical development, and higher rates of behavior problems relative to never-institutionalized parent-reared children (Juffer & van IJzendoorn, 2009; MacLean, 2003). In terms of problems that are related to social skills, with some exceptions (e.g., Cederblad, Höök, Irhammar, & Mercke, 1999; Stams, Juffer, Rispens, & Hoksbergen, 2000; Tan & Marfo, 2006), adopted children generally have higher rates of CBCL social problems (Groza & Ryan, 2002; Gunnar, Van Dulmen, & The IAP Team, 2007; Hawk & McCall, 2011; Hoksbergen, Rijk, van Dijkum & ter Laak, 2004; Merz & McCall, 2010; Stams et al., 2000) and lower levels of social competence than non-adopted children (Brodzinsky et al., 1984; Glennen & Bright, 2005; Verhulst, Althaus, & Versluis-Den Bieman, 1990a, 1990b). Adopted children may have difficulty in peer relationships (Fisher, Ames, Chisholm, & Savoie, 1997; Gunnar et al., 2007; Rutter et al., 2010), more problems with their attachment relationships (Rutter, Kreppner, & O’Connor, 2001; Van den Dries, Juffer, van IJzendoorn, & Bakermans-Kranenburg, 2009), and greater difficulty understanding facial expressions of emotions than non-adopted children (Camras, Perlman, Wismer Fries, & Pollak, 2006). Disinhibited social behavior, which may be related to deficits in inhibitory control (Bruce, Tarullo, & Gunnar, 2009), may also be observed in post-institutionalized adopted children (Chisholm, 1998; O’Connor, Rutter, & The ERA Study Team, 2000a; Tizard, 1977). Social difficulties of adopted children may last into adulthood. Adult adoptees are less likely to be married than a non-adopted matched sample (Lindblad, Hjern, & Vinnerljung, 2003; Sigal, Perry, Rossignol, & Ouimet, 2003; Sigal, Rossignol, & Perry, 1999; Tieman, van der Ende, & Verhulst, 2005), and more likely to have marital problems (Rutter & Quinton, 1984) or to be divorced than the general population (McKenzie, 1997).
Children who are adopted often have multiple risk factors, any of which could potentially contribute to later social and behavioral problems; this is particularly true for children who are not adopted at birth. For instance, adoptees may have had poor prenatal or birth circumstances (possibly marked by prematurity or low birth weight) in addition to deficient social-emotional care prior to adoption. In order to attribute outcomes to a child’s care before adoption, it is important to rule out the possibility that birth-related factors explain children’s outcomes. While relatively few studies of adoptees have statistically examined the relation between birth factors and behavioral outcomes (Julian, 2013), the majority of studies have found no significant association (Kreppner et al., 2007; Merz & McCall, 2010, 2011; Sonuga-Barke et al., 2008; but see Bos, Fox, Zeanah, & Nelson, 2009 for an exception).
For children adopted from institutional care, the case for institutional care as a potential causal factor for later behavioral outcomes is strengthened by associations between duration of exposure to institutional care and behavioral outcomes. In fact, the problems that post-institutionalized (PI) children experience often do vary as a function of the length of time a child spends in an institution (Gunnar, 2001; MacLean, 2003). Age at adoption is often used as a surrogate for time in an institution because the latter is likely more accurately reported by parents and the variables are typically highly correlated. Generally, a later age at adoption is associated with a variety of behavioral and physical growth problems including more difficulty with attachment and parent-child relationships, higher rates of disinhibited social behavior, social problems and poorer peer relationships, and higher rates of quasi-autism (Gunnar et al., 2007; Merz & McCall, 2010; Morison & Ellwood, 2000; Rutter et al., 2010; van den Dries et al., 2009; van IJzendoorn & Juffer, 2006).
Some studies (e.g., Kreppner et al., 2007; Merz & McCall, 2010) find that children adopted before a certain age have rates of problems similar to never-institutionalized parent-reared children, and children adopted after that age have a step-like increase in their rates of problems, with no apparent increase in risk with adoption at even later ages (Julian, 2013). This step function may occur at approximately 18 months of age in PI children adopted from one set of social-emotionally depriving institutions in St. Petersburg, Russian Federation (Hawk & McCall, 2011; Merz & McCall, 2010), but after as little as 6 months in children from globally depriving Romanian institutions (Colvert et al., 2008; Kreppner et al., 2007; Stevens et al., 2008).
Several independent samples have found that PI adoptees are more likely to have behavior problems in adolescence than in childhood (Groza & Ryan, 2002; Merz & McCall, 2010; Verhulst & Versluis-Den Bieman, 1995). This apparent sleeper effect suggests that the effects of institutionalization may not be apparent until children reach adolescence. While gender differences are rarely assessed in this population, some studies, including a meta-analysis, detect no significant differences between male and female international adoptees for behavior problems (Hoksbergen et al., 2004; Juffer & van IJzendoorn, 2005); when gender differences are detected, adopted boys tend to have more problems than adopted girls (Gunnar et al., 2007; Stams et al., 2000; Verhulst et al., 1990a).
The Current Study
The current study seeks to investigate the social skills of adopted PI children, particularly with respect to age at adoption, age at assessment, and gender, and compare the social skills of PI children to those of never-institutionalized parent-reared children. Social skills will first be examined with respect to birth circumstances to determine whether these factors explain variability in social skills among PI children. Next, social skills will be examined within the PI sample to determine whether social skills are related to age at adoption, and specifically whether social skills follow a step function with regard to age at adoption. In line with previous research with this sample (e.g., Hawk & McCall, 2011; Merz & McCall, 2010), it is hypothesized that children adopted before 18 months will have better social skills than children adopted after this age. Because previous studies have detected a higher likelihood of poor outcomes when adoptees are assessed in adolescence, it is hypothesized that PI children assessed in childhood will have better social skills than those assessed in adolescence. When PI children are compared to a non-PI standardization sample, it is hypothesized that few differences will be detected in childhood, but PI children, particularly those adopted at relatively older ages, will have poorer social skills in adolescence. Gender differences will be assessed, but it is hypothesized that no systematic gender differences will be detected.
Methods
Sample Description
Adoptive parents were recruited through a local adoption agency that specializes in the placement of Russian children with US families. Parents were first made aware of the larger study of the development of PI children through a newsletter or a letter from the director of the adoption agency. Packets containing numerous assessments including the Social Skills Rating System (SSRS; Gresham & Elliott, 1990) and the Child Behavior Checklist (CBCL; Achenbach & Rescorla, 2001) were sent to parents on the adoption agency’s mailing list on four waves of data collection in 2001, 2003, 2008, and 2010. The sample differed somewhat in each survey wave due to the addition of newly adopted children, and some children aging out of the age range for some measures in later waves. The response rate (e.g., number of surveys returned out of total number of surveys mailed, excluding undeliverable surveys, for each wave of data collection) was 40% (226 of 565) in Wave 1, 37% (254 of 687) in Wave 2, 51% (545 of 1069) in Wave 3, and 38% (448 of 1179) in Wave 4. While this response rate is lower than one of the largest international adoption follow-ups where the response rate was based on a sample who had already shown a non-specific interest in participating (65.6%; Gunnar et al., 2007), it is higher than the largest follow-up of Romanian adoptees (23.7–30%; Groza & Ryan, 2002). Parents were offered a modest payment for completion of the packet. Reminder post-cards were sent or phone calls (Wave 3 and 4 only) were made to parents several weeks after the packets were initially mailed.
Children were included in the current sample if they had complete SSRS data, had been in their adoptive homes at least one year, and had not been adopted following the implementation of a social-emotional intervention at their institution. Children whose parents reported a marked functional deficit (e.g., autism or severe cognitive impairment) were excluded (N = 25). If children had complete assessments available from multiple waves of data assessment, only the most recent (oldest age at assessment) record was included so as to increase the size of the smaller Secondary age sample. The number of children with longitudinal data was too small for analysis. The final sample included 341 PI children; characteristics of the sample (including family characteristics) are given in Table 1. The vast majority of children in this sample come from two-parent families with Caucasian parents who have at least a 4-year college degree and a median income of $125,000–150,000 per year. Approximately 85% of surveys were completed by the child’s adoptive mother. The standardization sample of the SSRS, comprised of never-institutionalized parent-reared children, was described in the SSRS manual (Gresham & Elliott, 1990). This sample was used to calculate Z scores for the SSRS, and to provide a basis against which PI children were directly compared in some analyses.
Table 1.
Sample Characteristics
| Elementary | Secondary | |
|---|---|---|
| N | 214 | 127 |
| Male | 94 | 56 |
| Female | 120 | 71 |
| Age at assessment (years) | 5.01–12.88 (Mdn=8.08) |
12.64–18.78 (Mdn=15.63) |
| Age at adoption (months) | 4.66–57.85 (Mdn=11.48) |
3.29–189.09 (Mdn=13.50) |
| Time in adoptive home (years) | 1.10–12.04 (Mdn=6.84) |
1.89–17.41 (Mdn=13.74) |
| Birth Country | ||
| Russia | 177 | 116 |
| Belarus | 34 | — |
| Uzbekistan | — | 9 |
| Other Eastern Europe | 3 | 2 |
| Mother-report | 84.6% | 85% |
| Two-parent household | 87.9% | 91.2% |
| Parent(s) with 4-year college degree or higher education | 91.0% | 90.2% |
| Median income | $125,000–$150,000 | $125,000–$150,000 |
| Respondent’s ethnicity | 99.5% white | 98.4% white |
Baby Home Characteristics
The vast majority of PI children in this study were adopted from “Baby Homes” or institutions for children up to four years of age in the Russian Federation, mostly in St. Petersburg. The remainder of the children were adopted from similar institutions in other countries in Eastern Europe.
The nature of the St. Petersburg Baby Homes is well described (see The St. Petersburg-USA Orphanage Research Team, 2005, 2008). They are typically adequate in terms of medical care, nutrition, safety, sanitation, toys, and equipment, but caregiver-child relationships are lacking. Caregivers often work 24-hour shifts on non-consecutive days, and children often “graduate” to new sets of caregivers and peers as they reach new developmental milestones. As a result, children don’t see the same caregivers today as they saw yesterday or will see tomorrow, and they can have 60–100 different caregivers by the time they reach 19 months of age. Caregivers tend to provide insensitive, unresponsive, adult-directed care, and are rarely emotionally engaged with the children. Delays in physical growth and development are common in this set of institutionalized children (The St. Petersburg-USA Orphanage Research Team, 2005).
Measures
Social Skills Rating System
The SSRS (Gresham & Elliott, 1990) is a widely used measure of social competence and adaptive functioning. This study utilized the parent-rated forms assessing children’s social skills. The SSRS survey versions are defined by grade, not age, so parents were directed to complete the Elementary version for children in kindergarten through 6th grade, and the Secondary version for children in 7th through 12th grade. Because grade level was not reliably available in the current sample, the Elementary sample was restricted to children aged 5 to 13 years, and the Secondary sample was restricted to children aged 12 to 19 years to limit the chance of children erroneously being included in the wrong sample (e.g., the parent of a 3rd grader might mistakenly complete the Secondary version). Each child is only included in one group. Of the 40 items on the Secondary version of the SSRS and 38 items on the Elementary version, 30 are substantively identical and the remainder are thematically similar. Examples of items include “Helps you with household tasks without prompting,” “Makes friends easily,” “Answers the phone appropriately,” and “Ends disagreements with you calmly.” Parents responded to items by reporting how often a behavior occurs: Never (0), Sometimes (1), or Very Often (2). For all items, a higher score reflects better (or at least more frequent displays of positive) social skills based on parent-reared norms. While both the Elementary and Secondary versions of the SSRS contain four subscales (Cooperation, Assertion, Responsibility, Self Control), these subscales are highly correlated with each other (Elementary: .543 to .699; Secondary: .539 to .842) and with the Total Social Skills score (Elementary: .807 to .859; Secondary: .824 to .913). Because of this, the current study utilized only the Total Social Skills score. Both the Elementary and Secondary versions of the SSRS demonstrate adequate internal consistency in the current sample with Cronbach’s alpha coefficients of .927 and .954, respectively.
Child Behavior Checklist for Ages 6–18
The CBCL (Achenbach & Rescorla, 2001) is a parent-report measure of children’s behavioral and emotional problems. The measure consists of 118 items describing specific behavioral and emotional problems, and parents rate how true this problem is for their child within the past 6 months: Not True (0), Somewhat or Sometimes True (1), Very True or Often True (2). Examples of items include “Cries a lot,” “Destroys things belonging to his/her family or others,” “Feels dizzy or lightheaded,” and “Easily jealous.” This study utilized the Total Score and the broadband Internalizing Problems and Externalizing Problems scales; these scales demonstrated adequate internal consistency in the current sample with Cronbach’s alpha coefficients of .961, .873, and .937, respectively.
Parent-reported information
Parents reported demographic information, their child’s birth weight, and whether they were born prematurely. Parents also provided their child’s date of birth, date of adoption, and date the survey was completed, and this was used to calculate the child’s age at adoption, age at assessment, and number of years of residence in their adoptive home.
Results
Data Preparation and Preliminary Analyses
If items were missing on a given SSRS subscale for a participant, the score value (0, 1, 2) closest to the mean of the remaining items on that subscale was imputed for the missing data (Osborne, 2013); no participant in either the Elementary or Secondary sample had more than three items missing on a 10-item subscale. Fewer than 10% of participants had missing data imputed, and less than .5% of the total items were imputed. A similar strategy was used to fill in missing data on the CBCL.
Z-scores were calculated for both the Elementary and Secondary samples using the means and standard deviations of the SSRS standardization sample of never-institutionalized parent-reared USA children available in the SSRS manual (Gresham & Elliott, 1990). Some analyses compared Elementary and Secondary scores, with the understanding that these comparisons reflect relative standing on the same conceptual set of skills if not the same specific behaviors. Z-scores were used when Elementary and Secondary PI scores were compared across SSRS forms, and raw scores were utilized when PI and Non-PI children’s scores were compared. For analyses that compared SSRS and CBCL scores, SSRS Z-scores and CBCL T-scores were utilized.
In order to rule out the possibility that Survey Wave (e.g., survey completed in 2001, 2003, 2008, or 2010) accounted for any effects, Survey Wave was added as a factor to the main analyses in the “Within the PI Sample” section below. These analyses revealed no interactions between Survey Wave and Sample or Age at Adoption. Furthermore, while average Social Skills were slightly different in each wave, scores were not systematically changing (Wave 2 was highest, Wave 4 was lowest, and Waves 1 and 3 were intermediate). There is no reason to believe that survey wave is a meaningful factor contributing to social skills scores, so all four waves of data will be analyzed, and Survey Wave is not included as a factor in further analyses.
Birth Circumstances
Parent-reported prematurity status was available for approximately 60% of PI children, and birth weight was available for approximately 76% of PI children. Low birth weight was defined as below 5 lbs, 8 oz (approximately 2500 grams) at birth. Of children with data available, approximately 35.4% (92 of 260) were born prematurely, and approximately 38.6% (80 of 207) had low birth weight. Consistent with prior research with this sample on behavior problems and executive function (Merz & McCall, 2010, 2011), there was no apparent association between PI children’s Total Social Skills (z-scores) and their prematurity status, F(1, 206) = .065, p = .800, or low birth weight, F(1, 259) = 2.649, p = .105.
Within the PI Sample
To test the possibility of a step function of age at adoption, an Age at Adoption (0–11 months, 12–17 months, 18–23 months, 24+ months) × Sample (Elementary, Secondary) ANOVA was conducted. The Age at Adoption × Sample interaction was non-significant, indicating that there was no evidence that any age at adoption effect was different for the two samples. While the main effect of age at adoption was marginal in this two-factor analysis, F(3, 335) = 2.429, p = .065, the age at adoption effect reached significance when the non-significant Sample factor was omitted, F(3, 339) = 3.429, p < .05 (see Figure 1).
Figure 1.
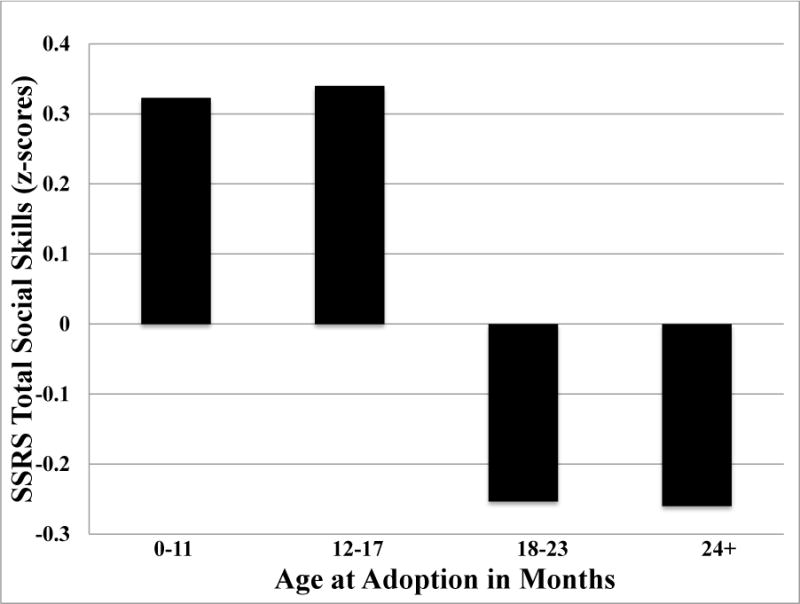
Mean Total Social Skills scores by Age at Adoption for Combined Elementary and Secondary Sample
In either case, however, an ANOVA with a four-level factor (or orthogonal polynomial trend analysis) is relatively insensitive to detecting a step function hypothesized to occur between the second and third levels because the two levels before and the two levels after the step are hypothesized to not be different (Kirk, 1982). Therefore, pairwise comparisons matching the step hypothesis were conducted. In the one-way ANOVA of Age at Adoption on Social Skills, specific contrast tests demonstrated that the significant Age at Adoption effect was due to the difference between children adopted before versus after 18 months, as hypothesized. In particular, there was no significant difference between children adopted between 0–11 months of age and 12–17 months of age, Contrast Estimate1 = .006, p = .977, nor was there a significant difference between children adopted at 18–23 months of age and 24+ months of age, Contrast Estimate = −.015, p = .965. In contrast, children adopted before 18 months had significantly higher/better scores than children adopted after 18 months, Contrast Estimate = 1.178, p < .01. Parallel specific contrast tests in the Age at Adoption × Sample ANOVA also revealed that the marginal Age at Adoption effect was due to the contrast between children adopted before versus after 18 months of age. Because a step function at 18 months of age at adoption was confirmed, age at adoption was dichotomized at 18 months for the remaining analyses.
Next, an Age at Adoption (<18 months, >18 months) × Sample (Elementary, Secondary) × Gender ANOVA on SSRS Total Social Skills (Z-scores) revealed that scores were significantly higher/better for earlier-adopted than later-adopted children, F(1, 335) = 4.443, p < .05, Elementary than Secondary PI children, F(1, 335) = 12.835, p < .01, and males than females, F(1, 335) = 9.099, p < .01. There were no significant interactions.
PI Sample versus Non-PI Standardization Sample
To determine how PI children compare to the Non-PI standardization sample, SSRS Total Social Skills (raw) scores for the Elementary and Secondary PI samples were compared to Non-PI children in a PI-Status (PI, Non-PI) × Sample (Elementary, Secondary) × Gender ANOVA. All main effects were nonsignificant, but there were significant interactions for PI Status × Sample, F(1, 1161) = 21.32, p < .01, PI Status × Gender, F(1, 1161) = 14.46, p < .01, and Sample × Gender, F(1, 1161) = 5.27, p < .05 (see Figure 2). The three-way interaction was not significant. Specifically, the PI sample had higher/better social skills than the Non-PI sample in the Elementary sample, whereas the reverse was true in the Secondary sample. Furthermore, PI Females in the Secondary sample have particularly low/poor social skills scores, contributing to both the PI × Gender and Sample × Gender interactions.
Figure 2. Elementary and Secondary SSRS Social Skills Scores for PI and Non-PI Children.
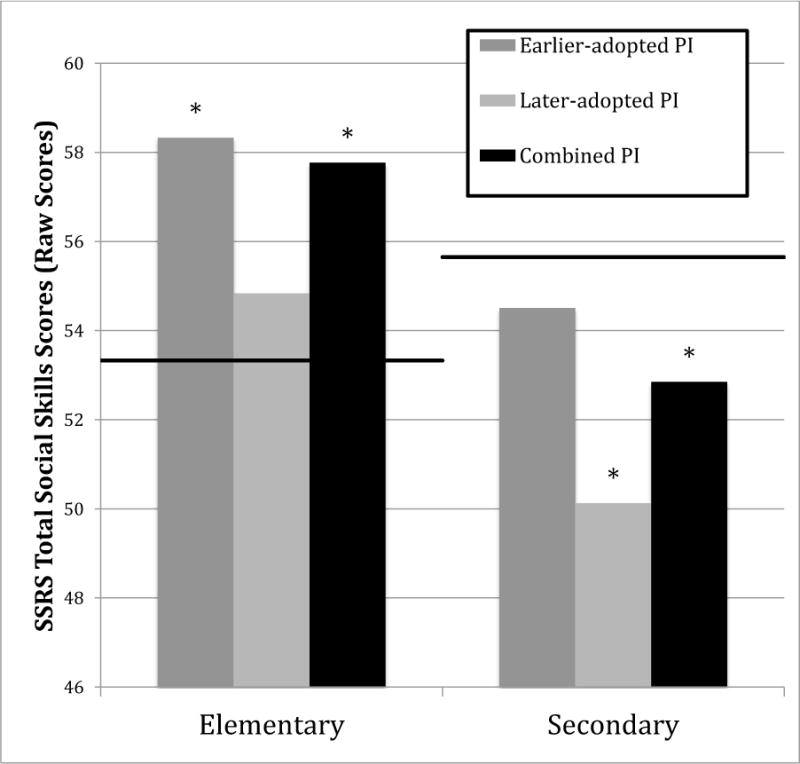
Note. Line indicates Non-PI average score. * p < .05 difference between Non-PI and PI subsample.
Total Social Skills scores for each Sample (Elementary, Secondary) × Age at Adoption (<18 months, >18 months) × Gender cell were compared to the Non-PI standardization sample’s means for each Sample and Gender (see Figure 2). Overall in the Elementary sample, PI children scored higher/better than Non-PI children, t(213) = 4.893, p < .01, and this was true for both males and females. Earlier-adopted Elementary children scored higher/better than Non-PI children, t(170) = 5.344, p < .01, and this was true for both males and females, but later-adopted Elementary children did not differ from Non-PI children. Secondary PI children scored significantly lower/poorer than Non-PI children, t(126) = −2.239, p < .05, and this effect was due to females, but not males, scoring significantly lower/poorer than Non-PI children. Both earlier-adopted females, t(41) = −2.092, p < .05, and later-adopted females, t(27) = −2.427, p < .05, scored significantly lower/poorer than Non-PI children in the Secondary sample, but this was not true for males.
Social Skills and Behavior Problems
SSRS Social Skills were significantly negatively correlated with CBCL Total, Internalizing, and Externalizing behavior problems in the Combined sample, Elementary sample, and Secondary sample, and for males and females separately within each sample (Table 2). Furthermore, children who scored in the extreme low/poor range of the SSRS (lowest 15% of the standardization sample) also tended to score in the highest/poorest 15% of the CBCL for Total, X2 (1, N = 321) = 109.719, p < .001, Internalizing, X2 (1, N = 320) = 61.406, p < .001, and Externalizing, X2 (1, N = 320) = 117.254, p < .001, behavior problems. Again, this was also true when the Elementary and Secondary samples were tested independently.
Table 2.
Correlations between SSRS Total Social Skills and CBCL Internalizing, Externalizing, and Total Behavior Problems.
| Internalizing | Externalizing | Total Behavior Problems | ||
|---|---|---|---|---|
| Elementary Sample | Male | r(86) = −.541* | r(86) = −.632* | r(88) = −.545* |
| Female | r(105) = −.484* | r(105) = −.736* | r(109) = −.655* | |
| Total | r(193) = −.487* | r(193) = −.690* | r(199) = −.609* | |
|
| ||||
| Secondary Sample | Male | r(51) = −.697* | r(50) = −.643* | r(54) = −.795* |
| Female | r(68) = −.759* | r(69) = −.815* | r(69) = −.845* | |
| Total | r(121) = −.747* | r(121) = −.771* | r(125) = −.821* | |
|
| ||||
| Combined Sample | Male | r(139) = −.577* | r(138) = −.606* | r(144) = −.634* |
| Female | r(177) = −.634* | r(178) = −.784* | r(182) = −.741* | |
| Total | r(318) = −.605* | r (318) = −.721* | r(328) = −.696* | |
p < .001
Discussion
This study sought to better understand the how social skills may relate to PI adopted children’s age at adoption, age at assessment, and gender, and to examine how PI children’s social skills compare to Non-PI children. Preliminary analyses suggest that PI children’s social skills are not significantly accounted for by a child’s prematurity status or whether they were low birth weight, so birth circumstances can be ruled out as a primary contributor to social skills outcomes in this set of PI children. Previous studies on this set of PI children have detected a clear step function at 18 months at adoption for behavior problems and executive function (Hawk & McCall, 2011; Merz & McCall, 2010, 2011), and the current study suggests a similar pattern for social skills. In the Elementary years, PI children, especially those who were adopted before 18 months, have better social skills than Non-PI children, but in the Secondary years, PI children, especially those who were adopted after 18 months, have poorer social skills than Non-PI children. Furthermore, PI females are rated as particularly poor in their social skills, especially in the Secondary sample.
The high correlations and associations between extreme scores on the SSRS and CBCL suggest that those PI children who display social skills difficulties are the same subset of PI children who display higher rates of behavior problems. Thus, it is possible that a similar etiology underlies both types of problems. For instance, PI children who lacked a supportive early caregiver-child relationship within the institution may have had excessively high levels of stress (Kertes et al., 2008), which is associated with later executive function and emotion regulation problems (National Scientific Council on the Developing Child, 2010, 2011); poor executive function and emotion regulation could potentially contribute to both behavior problems and social skill deficits (Eisenberg, Fabes, Bernzweig, Karbon, Poulin, & Hanish, 1993; Hughes, 2011).
Age at Adoption Step Function
Prior studies have detected a clear step function for age at adoption such that children adopted before a certain age have rates of problems comparable to never-institutionalized parent-reared children, and there is a clear rise in risk of behavior and executive function problems for children adopted after that age, with no additional increase in risk for increasingly older ages at adoption (Colvert et al., 2008; Hawk, & McCall, 2011; Merz & McCall, 2010; Kreppner et al., 2007; Stevens et al., 2008). For studies of the current sample of children adopted from socially-emotionally depriving Russian institutions, this step tends to occur at about 18 months for behavior problems and executive function (Hawk & McCall, 2011; Merz & McCall, 2010, 2011). In the current study, this same pattern was detected in the combined Elementary and Secondary sample for social skills.
The step function for age at adoption suggests that some sort of sensitive period may play a role. But, the boundaries of such a sensitive period seem to be different depending on the severity of the institutional deprivation; a step function may occur much earlier (e.g., 6 months at adoption; Colvert et al., 2008; Kreppner et al., 2007; Stevens et al., 2008) for children from globally depriving Romanian institutions and somewhat later for children from institutions in which the primary deprivation is social-emotional in nature (e.g., 18 months at adoption for Russian institutions; Hawk & McCall, 2011; Merz & McCall, 2010, 2011). Thus, it may be that cumulative exposure within a broader sensitive period accounts for the apparent step function. While the cause of these changes is unclear, it may be that epigenetic changes and biological stress responses are at least partially responsible (Julian, 2013; Shonkoff, Boyce, & McEwen, 2009). Given that changes occur even when medical care and nutrition are adequate, it is likely that social-emotional deprivation is the relevant domain of early experience.
Practitioners and policy makers should be aware of the increased risk for social and behavioral problems among children adopted at relatively later ages. Efforts should be made to streamline judicial and administrative procedures that often delay a child’s eligibility for adoption, while being careful not to unnecessarily hurry biological parents into making a decision about their child’s status before they are ready.
Age at Assessment
The finding that problems are more evident when assessed in adolescence than in childhood is consistent with prior research on PI samples (e.g., Rutter et al., 2010; Merz & McCall, 2010; Verhulst et al., 1990a; Wolkind, 1974). The effects of institutionalization on social skills are unlikely to be simply the persistence of behaviors previously learned in the institution—if this were the case, problems would be most evident in younger samples who are temporally closer to the experience of institutional life. Instead, it may be that problems in the adolescent years reflect underlying deficits in certain basic skills that only become evident in behaviors that emerge later in development (Zeanah, Gunnar, McCall, Kreppner, & Fox, 2011). Adolescence is a time when social and behavioral demands and expectations heighten, adolescents become more independent, and adults tend to pull back their support, so it could be that this population is somewhat less able to adapt when they are immersed in a more complex social environment.
Further, in childhood (but not in adolescence), PI children were found to be rated better than non-PI children in their social skills. It is possible that this effect partially represents carry-over from the culture of conformity and obedience that characterizes institutions, or the typically high quality home environments of adoptive families. While the current data were cross-sectional, not longitudinal, adoptive families should be aware that social and behavioral problems might emerge in adolescence, even for adoptees who appeared to be functioning quite well in childhood. Families and providers might offer additional support to adoptees as they enter adolescence in order to anticipate and remediate the problems that are more likely to emerge at these ages.
Gender Differences
While gender is not often assessed in this field, most studies find either no gender effects (e.g., Juffer & van IJzendoorn, 2005), or adopted boys have more problems than adopted girls (e.g., Gunnar et al., 2007). The current study found that in the older Secondary sample, males did not differ from Non-PI adolescents, but females had significantly poorer social skills than Non-PI children. While this finding of PI females having more problems than PI males is inconsistent with prior literature, it may be that PI males are more likely to exhibit different kinds of problems (e.g., behavior problems) than PI females. Alternatively, it is possible that adults have greater social expectations of adolescent females than males, so social deficits may become particularly apparent to parents of PI females as they enter adolescence. But, this study’s findings need to be replicated in an independent sample to be sure that it is not a chance finding.
Conclusions and Implications
Findings from this study suggest that children adopted from socially-emotionally depriving institutions may exhibit poor social skills in adolescence, particularly if they were adopted after 18 months and are female. Interestingly, childhood-aged PI adoptees are rated by their parents, on average, as having better social skills than a non-PI standardization sample. Perhaps in part due to adoptees’ typically high quality home environment, and in part due to carryover from the environment of conformity and obedience of institutional life, PI children are judged by their parents as functioning quite well in social contexts. While previous research (e.g., Rutter et al., 2010; Verhulst et al., 1990a) suggests that problems tend not to be as evident in PI samples during the childhood period, this study builds on those findings to suggest that children may, in fact, behave exceptionally well at these ages. As PI children enter adolescence, however, deficient social skills become more likely, particularly for females adopted after 18 months of age. Parents, teachers, and providers should be aware that social skills deficits may emerge during adolescence, even for PI youth who had relatively problem-free childhoods; despite the temporal distance between adolescence and pre-adoption experience, these problems are likely a legacy of their early care environment. PI adolescents, particularly girls, might benefit from extra support and scaffolding from adults in their lives as they learn to navigate the complex social environment of adolescence.
Limitations and Future Directions
One limitation of this study is that it only includes parent-report of PI children’s social behavior. While parent-report has the advantage that parents experience their children in a variety of domains, parents also depend on their own perceptions and standards, which vary between parents and may change with their child’s age. As children enter adolescence, and peers become more central to their social life than their families, it may be especially important to obtain peer reports of PI children’s social functioning. Further, while the SSRS standardization sample provided an opportunity to assess how PI children’s social skills relate to a typical Non-PI sample, the standardization sample differs from the PI sample in ways other than the experience of institutionalization (e.g., SES, assessment date, ethnicity).
Future studies would benefit from utilizing additional measures of social skills and social problems, and examining more discrete categories of social skills. Child-, teacher-, and peer-report measures in addition to parent report would also provide a complementary perspective on PI children’s social skills. Lastly, obtaining assessments of the social skills of PI children’s siblings or peers would be ideal, because siblings and peers represent the individuals to whom PI children are most often compared in their everyday lives.
Acknowledgments
The authors are grateful to Celia Brownell and Susan B. Campbell for their helpful comments on earlier drafts of this manuscript, to Emily Merz, Johana Rosas, and Brandi Hawk for their assistance with the database, and to the participating families who made this study possible.
Funding: This research was supported by NICHD grants ND39017 and HD050212 to Robert B. McCall and Christina J. Groark. The content is solely the responsibility of the authors and does not necessarily represent the official views of NICHD or NIH.
Footnotes
The Contrast Estimate is the difference between the marginal means of the two age-at-adoption groups being compared, and the error term for this estimate is the error estimate from the full ANOVA (Kirk, 1982).
Contributor Information
Megan M. Julian, Email: Mmj17@pitt.edu, meganjulian@gmail.com, Doctoral Candidate, Clinical and Developmental Psychology, University of Pittsburgh, Psychology Department, 210 South Bouquet St., 3rd Floor, Pittsburgh, PA 15260.
Robert B. McCall, Email: mccall2@pitt.edu, Professor, Department of Psychology, Co-Director, University of Pittsburgh Office of Child Development, 400 N. Lexington St., Pittsburgh, PA 15208.
References
- Achenbach TM, Rescorla LA. Manual for the ASEBA school-age forms and profiles. Burlington: University of Vermont, Research Center for Children, Youth, and Families; 2001. [Google Scholar]
- Ainsworth MDS. The development of infant-mother attachment. In: Caldwell B, Ricciuti H, editors. Review of child development research. Vol. 3. Chicago: University of Chicago Press; 1973. pp. 1–94. [Google Scholar]
- Bos KJ, Fox N, Zeanah CH, Nelson CA. Effects of early psychosocial deprivation on the development of memory and executive function. Frontiers in Behavioral Neuroscience. 2009;3:1–16. doi: 10.3389/neuro.08.016.2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bretherton I, Munholland K. Internal working models in attachment relationships: A construct revisited. In: Cassidy J, Shaver P, editors. Handbook of attachment. New York: Guilford Press; 1999. pp. 89–111. [Google Scholar]
- Brodzinsky DM. Long-term outcomes in adoption. The Future of Children. 1993;3(1):153–166. [Google Scholar]
- Brodzinsky DM, Schechter DE, Braff AM, Singer LM. Psychological and Academic Adjustment in Adopted Children. Journal of Consulting and Clinical Psychology. 1984;52:582–590. doi: 10.1037//0022-006x.52.4.582. [DOI] [PubMed] [Google Scholar]
- Bruce J, Tarullo AR, Gunnar MR. Disinhibited social behavior among internationally adopted children. Development and Psychopathology. 2009;21(1):157–171. doi: 10.1017/S0954579409000108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Camras LA, Perlman SB, Wismer Fries AB, Pollak SD. Post-institutionalized Chinese and Eastern European children: Heterogeneity in the development of emotion understanding. International Journal of Behavioral Development. 2006;30(3):193–199. doi: 10.1177/0165025406063608. [DOI] [Google Scholar]
- Cederblad M, Höök B, Irhammar M, Mercke A. Mental health in international adoptees as teenagers and young adults. An epidemiological study. Journal of Child Psychology and Psychiatry. 1999;40(8):1239–1248. [PubMed] [Google Scholar]
- Chisholm K. A three year follow-up of attachment and indiscriminate friendliness in children adopted from Romanian orphanages. Child Development. 1998;69(4):1092–1106. [PubMed] [Google Scholar]
- Colvert E, Rutter M, Kreppner J, Beckett C, Castle J, Groothues C, Sonuga-Barke EJS. Do theory of mind and executive function deficits underlie the adverse outcomes associated with profound early deprivation?: Findings from the English and Romanian Adoptees study. Journal of Abnormal Child Psychology. 2008;36(7):1057–1068. doi: 10.1007/s10802-008-9232-x. [DOI] [PubMed] [Google Scholar]
- Eisenberg N, Fabes RA, Bernzweig J, Karbon M, Poulin R, Hanish L. The relations of emotionality and regulation to preschoolers’ social skills and sociometric status. Child Development. 1993;64(5):1418–1438. [PubMed] [Google Scholar]
- Fisher L, Ames EW, Chisholm K, Savoie L. Problems reported by parents of Romanian orphans adopted to British Colombia. International Journal of Behavioral Development. 1997;20(1):67–82. doi: 10.1080/016502597385441. [DOI] [Google Scholar]
- Glennen S, Bright B. Five years later: Language in school-age internationally adopted children. Seminars in Speech and Language. 2005;26(1):86–101. doi: 10.1055/s-2005-864219. [DOI] [PubMed] [Google Scholar]
- Gresham FM, Elliott SN. Social Skills Rating System. Circle Pines, MN: American Guidance Service; 1990. [Google Scholar]
- Groza V, Ryan S. Domestic Special Needs Adoption, International Adoption, and Child Behavior. Psychoneurendocrinology. 2002;27(1–2):181–197. doi: 10.1016/s0306-4530(01)00044-0. [DOI] [PubMed] [Google Scholar]
- Gunnar MR. Effects of early deprivation: Findings from orphanage-reared infants and children. In: Nelson CA, Luciana M, editors. Handbook of Developmental Cognitive Neuroscience. Cambridge, MA: MIT Press; 2001. pp. 617–629. [Google Scholar]
- Gunnar MR, Van Dulmen MHM, The International Adoption Project Team Behavior problems in postinstitutionalized internationally adopted children. Development and Psychopathology. 2007;19(1):129–148. doi: 10.1017/S0954579407070071. [DOI] [PubMed] [Google Scholar]
- Hawk BN, McCall RB. Specific extreme behaviors of postinstitutionalized Russian adoptees. Developmental Psychology. 2011;47(3):732–738. doi: 10.1037/a0021108. [DOI] [PubMed] [Google Scholar]
- Hoksbergen R, Rijk K, van Dijkum C, ter Laak J. Adoption of Romanian children in the Netherlands: Behavior problems and parenting burden of upbringing for adoptive parents. Developmental and Behavioral Pediatrics. 2004;25(3):175–180. doi: 10.1097/00004703-200406000-00006. [DOI] [PubMed] [Google Scholar]
- Hughes C. Changes and challenges in 20 years of research into the development of executive functions. Infant and Child Development. 2011;20:251–271. doi: 10.1002/icd.736. [DOI] [Google Scholar]
- Juffer F, van IJzendoorn MH. Behavior problems and mental health referrals of international adoptees: A meta-analysis. Journal of the American Medical Association. 2005;293(20):2501–2515. doi: 10.1001/jama.293.20.2501. [DOI] [PubMed] [Google Scholar]
- Juffer F, van IJzendoorn MH. International adoption comes of age: Development of international adoptees from a longitudinal and meta-analytical perspective. In: Wrobel GM, Neil E, editors. International advances in adoption research for practice. West Sussex, UK: John Wiley & Sons; 2009. pp. 169–192. [Google Scholar]
- Julian MM. Age at adoption from institutional care as a window into the lasting effects of early experiences. Clinical Child and Family Psychology Psychology Review. 2013;16(2):101–145. doi: 10.1007/s10567-013-0130-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kertes DA, Gunnar MR, Madsen NJ, Long JD. Early deprivation and home basal cortisol levels: A study of internationally adopted children. Development and Psychopathology. 2008;20(2):473–491. doi: 10.1017/S0954579408000230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kirk RE. Experimental Design. 2nd. Belmont CA: Brooks Cole; 1982. [Google Scholar]
- Kreppner JM, Rutter M, Beckett C, Castle J, Colvert E, Groothues C, Sonuga-Barke EJS. Normality and impairment following profound early institutional deprivation: A longitudinal follow-up into early adolescence. Developmental Psychology. 2007;43(4):931–946. doi: 10.1037/0012-1649.43.4.931. [DOI] [PubMed] [Google Scholar]
- Lindblad F, Hjern A, Vinnerljung B. Intercountry adopted children as young adults—A Swedish cohort study. American Journal of Orthopsychiatry. 2003;73(2):190–202. doi: 10.1037/0002-9432.73.2.190. [DOI] [PubMed] [Google Scholar]
- MacLean K. The impact of institutionalization on child development. Development and Psychopathology. 2003;15(4):853–884. doi: 10.1017/s0954579403000415. [DOI] [PubMed] [Google Scholar]
- McKenzie RB. Orphanage alumni: How they have done and how they evaluate their experience. Child and Youth Care. 1997;26:87–111. [Google Scholar]
- Merz EC, McCall RB. Behavior problems in children adopted from psychosocially depriving institutions. Journal of Abnormal Child Psychology. 2010;38(4):459–470. doi: 10.1007/s10802-009-9383-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Merz EC, McCall RB. Parent ratings of executive functioning in children adopted from psychosocially depriving institutions. Journal of Child Psychology and Psychiatry. 2011;52(5):537–546. doi: 10.1111/j.1469-7610.2010.02335.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morison SJ, Ellwood AL. Resiliency in the aftermath of deprivation: A second look at the development of Romanian orphanage children. Merrill-Palmer Quarterly. 2000;46:717–737. [Google Scholar]
- National Scientific Council on the Developing Child. Persistent fear and anxiety can affect young children’s learning and development: Working paper #9. 2010 http://www.developingchild.net.
- National Scientific Council on the Developing Child. Building the brain’s “air traffic control” system: How early experiences shape the development of executive function: Working paper #11. 2011 http://www.developingchild.net.
- O’Connor TG, Rutter M, The ERA Study Team Attachment disorder behavior following early severe deprivation: Extension and longitudinal follow-up. Journal of the American Academy of Child and Adolescent Psychiatry. 2000a;39:703–712. doi: 10.1097/00004583-200006000-00008. [DOI] [PubMed] [Google Scholar]
- Osborne JW. Best Practices in Data Cleaning: A Complete Guide to Everything you Need to Do Before and After Collecting Your Data. SAGE Publications; 2013. Dealing with missing or incomplete data: debunking the myth of emptiness; pp. 105–138. [Google Scholar]
- Rutter M, Kreppner JM, O’Connor TG. Specificity and heterogeneity in children’s responses to profound institutional privation. British Journal of Psychiatry. 2001;179:97–103. doi: 10.1192/bjp.179.2.97. [DOI] [PubMed] [Google Scholar]
- Rutter M, Quinton D. Long-term follow-up of women institutionalized in childhood: Factors promoting good functioning in adult life. British Journal of Developmental Psychology. 1984;2:191–204. [Google Scholar]
- Rutter M, Sonuga-Barke EJ, Beckett C, Castle J, Kreppner J, Kumsta R, Bell CA. Deprivation-specific psychological patterns: Effects of institutional deprivation. Monographs of the Society for Research in Child Development. 2010;75(1):1–250. doi: 10.1111/j.1540-5834.2010.00550.x. [DOI] [PubMed] [Google Scholar]
- Shonkoff JP, Boyce WT, McEwen BS. Neuroscience, molecular biology, and the childhood roots of health disparities: Building a new framework for health promotion and disease prevention. Journal of the American Medical Association. 2009;301(21):2252–2259. doi: 10.1001/jama.2009.754. [DOI] [PubMed] [Google Scholar]
- Sigal JJ, Perry JC, Rossignol M, Ouimet MC. Unwanted infants: Psychological and physical consequences of inadequate orphanage care 50 years later. American Journal of Orthopsychiatry. 2003;73(1):3–12. doi: 10.1037/0002-9432.73.1.3. [DOI] [PubMed] [Google Scholar]
- Sigal JJ, Rossignol M, Perry JC. Some psychological and physical consequences in middle-aged adults of underfunded institutional care in childhood. The Journal of Nervous and Mental Disease. 1999;187(1):57–59. doi: 10.1097/00005053-199901000-00011. [DOI] [PubMed] [Google Scholar]
- Sonuga-Barke EJ, Beckett C, Kreppner J, Castle J, Colvert E, Stevens S, et al. Is sub-nutrition necessary for a poor outcome following early institutional deprivation? Developmental Medicine and Child Neurology. 2008;50(9):664–671. doi: 10.1111/j.1469-8749.2008.03065.x.. [DOI] [PubMed] [Google Scholar]
- Sroufe LA, Waters E. Attachment as an organizational construct. Child Development. 1977;48:1184–1199. [Google Scholar]
- Stams GJM, Juffer F, Rispens J, Hoksbergen RAC. The development and adjustment of 7-year-old children adopted in infancy. Journal of Psychological Psychiatry. 2000;41(8):1025–1037. [PubMed] [Google Scholar]
- Stevens S, Sonuga-Barke EJS, Kreppner J, Beckett C, Castle J, Colvert E, Rutter M. Inattention/overactivity following early severe institutional deprivation: Presentation and associations in early adolescence. Journal of Abnormal Child Psychology. 2008;36(3):385–398. doi: 10.1007/s10802-007-9185-5. [DOI] [PubMed] [Google Scholar]
- Tan TX, Marfo K. Parental ratings of behavioral adjustment in two samples of adopted Chinese girls: Age-related versus socio-emotional correlates and predictors. Journal of Applied Developmental Psychology. 2006;27(1):14–30. doi: 10.1016/j.appdev.2005.12.004. [DOI] [Google Scholar]
- The St. Petersburg-USA Orphanage Research Team. Characteristics of children, caregivers, and orphanages for young children in St. Petersburg, Russian Federation. Journal of Applied Developmental Psychology: Child Abandonment, Special Issue. 2005;26(5):477–506. [Google Scholar]
- The St. Petersburg-USA Orphanage Research Team. The effects of early social-emotional and relationship experience on the development of young orphanage children. Monographs of the Society for Research in Child Development. 2008;73(3) doi: 10.1111/j.1540-5834.2008.00483.x. 291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thompson RA. The development of the person: Social understanding, relationships, conscience, self. In: Damon W, Lerner RM, editors. Handbook of child psychology (6th Ed), Vol. 3. Social, emotional, and personality development. New York: Wiley; 2006. pp. 24–98. N. Eisenberg, Vol. Ed. [Google Scholar]
- Tieman W, van der Ende J, Verhulst FC. Psychiatric disorders in young adult intercountry adoptees: An epidemiological study. American Journal of Psychiatry. 2005;162(3):592–598. doi: 10.1176/appi.ajp.162.3.592. [DOI] [PubMed] [Google Scholar]
- Tizard B. Adoption: A second chance. London: Open Books; 1977. [Google Scholar]
- van den Dries L, Juffer F, van IJzendoorn MH, Bakermans-Kranenburg MJ. Fostering security? A meta-analysis of attachment in adopted children. Children and Youth Services Review. 2009;31(3):410–421. doi: 10.1016/j.childyouth.2008.09.008. [DOI] [Google Scholar]
- Van IJzendoorn MH, Juffer F. The Emanuel Miller memorial lecture 2006: Adoption as intervention. Meta-analytic evidence for massive catch-up and plasticity in physical, socio-emotional, and cognitive development. Journal of Child Psychology and Psychiatry. 2006;47(12):1228–1245. doi: 10.1111/j.1469-7610.2006.01675.x. [DOI] [PubMed] [Google Scholar]
- Verhulst F, Althaus M, Versluis-Den Bieman HJ. Problem behavior in international adoptees: I. An epidemiological study. Journal of the American Academy of Child and Adolescent Psychology. 1990a;29:94–103. doi: 10.1097/00004583-199001000-00015. [DOI] [PubMed] [Google Scholar]
- Verhulst F, Althaus M, Versluis-Den Bieman HJ. Problem behavior in international adoptees: II. Age at placement. Journal of the American Academy of Child and Adolescent Psychology. 1990b;29:104–111. doi: 10.1097/00004583-199001000-00016. [DOI] [PubMed] [Google Scholar]
- Verhulst FC, Versluis-Den Bieman HJM. Developmental course of problem behaviors in adolescent adoptees. Journal of American Academy of Child and Adolescent Psychiatry. 1995;24:151–159. doi: 10.1097/00004583-199502000-00010. [DOI] [PubMed] [Google Scholar]
- Wolkind SN. The components of “affectionless psychopathy” in institutionalized children. Journal of Child Psychology and Psychiatry. 1974;15:215–220. doi: 10.1111/j.1469-7610.1974.tb01246.x. [DOI] [PubMed] [Google Scholar]
- Zeanah CH, Gunnar MR, McCall RB, Kreppner J, Fox NA. VI. Sensitive periods. In: McCall RB, van IJzendoorn MH, Juffer F, Groark CJ, Groza VK, editors. Children without permanent parents: Research, practice, and policy. 4. Vol. 76. 2011. pp. 147–162. (Monographs of the Society for Research in Child Development, Serial No. 301). [DOI] [PMC free article] [PubMed] [Google Scholar]