

Abstract
Clinical movement screening tests are gaining popularity as a means to determine injury risk and to implement training programs to prevent sport injury. While these screens are being used readily in the clinical field, it is only recently that some of these have started to gain attention from a research perspective. This limits applicability and poses questions to the validity, and in some cases the reliability, of the clinical movement tests as they relate to injury prediction, intervention, and prevention. This editorial will review the following clinical movement screening tests: Functional Movement Screen™, Star Excursion Balance Test, Y Balance Test, Drop Jump Screening Test, Landing Error Scoring System, and the Tuck Jump Analysis in regards to test administration, reliability, validity, factors that affect test performance, intervention programs, and usefulness for injury prediction. It is important to review the aforementioned factors for each of these clinical screening tests as this may help clinicians interpret the current body of literature. While each of these screening tests were developed by clinicians based on what appears to be clinical practice, this paper brings to light that this is a need for collaboration between clinicians and researchers to ensure validity of clinically meaningful tests so that they are used appropriately in future clinical practice. Further, this editorial may help to identify where the research is lacking and, thus, drive future research questions in regards to applicability and appropriateness of clinical movement screening tools.
Keywords: Functional Movement Screen, Y Balance Test, Star excursion balance test, Tuck jump analysis
Core tip: Clinical movement screening tests like the Functional Movement Screen and Y Balance Test have gained a lot of popularity in the clinical setting as a tool to predict injury and guide injury prevention programs/training. However, clinicians should be aware that various factors like sex differences, previous injury history, and sport participation can influence the accuracy of these screening tests; therefore, it is important to evaluate the validity, reliability, and accuracy of these tools before implementing them into clinical practice.
INTRODUCTION
Injury is often unavoidable in sport participation and is reported to be as high as 2.51/1000 Athlete-Exposures[1] and 13.79/1000 Athlete-Exposures[2] in high school and collegiate athletes, respectively. These injuries are further classified as overuse, defined as an injury caused by repeated microtrauma without an identifiable event to attribute the mechanism of injury or acute, defined as a specific, identifiable mechanism of injury[3]. Additionally, acute injuries occur as a result of either contact or non-contact mechanisms. Contact mechanisms as defined by the National Collegiate Athletic Association Injury Surveillance System[4] involve direct contact with another player or the playing surface, apparatus/ball, or other in environment (e.g., wall, fence); while non-contact mechanisms are identified as those that occur with no apparent contact and may involve a rotational force. Although these injury distinctions seem to be well understood, the effect of all potential mechanisms is less clear. Several clinical movement screening tests have been proposed to analyze differing mechanisms for injury prediction. Pre-season movement screening tests are likely less effective in predicting contact injuries due to the external mechanism involved with contact injuries. Thus, when comparing between studies one must be cognizant of the operational definition of injury.
Movement screening tools can be used for non-contact injury risk prediction and to guide injury prevention programs; however, the costly nature of sophisticated research equipment is a barrier to using high speed motion analysis in the practicing clinicians’ pre-participation physical examinations. Therefore, clinician friendly movement screening tools have been developed and are gaining popularity as a means to reduce injury risk. These tools include the Functional Movement Screen™ (FMS), Y Balance/Star Excursion Balance Test (YBT/SEBT), Tuck Jump Assessment (TJA), Drop Jump Screening Test (DJST), and the Landing Error Scoring System (LESS), which are being used fairly regularly in the clinical setting. Thus, it is important to understand the research surrounding the applicability of these tools to non-contact injury prediction. Therefore, the purpose of this editorial is to define the above clinical movement screening tools and to address each test’s normative data, validity, reliability, performance differences across samples, recommendations for use, and injury prediction.
FMS™
The FMS (Figure 1) is a clinical test developed to screen performance with fundamental movements, requiring a balance between stability and mobility while moving through a proximal to distal sequence[5]. The FMS is a proprietary tool purported to measure fundamental movements necessary for athletic performance and comprises 7 individual movement patterns and 3 clearing tests, which are tests associated with some movement patterns to determine the presence of pain (Table 1)[5,6]. Each movement pattern is scored based on degree of compensatory movements required to complete the movement, as well as pain. An ordinal scoring system is used from 3-0, where 3 corresponds to the ability to correctly complete the movement without compensation, 2 corresponds to performing the movement with compensation, 1 corresponds to the inability to perform the movement. A score of 0 is given if there is pain during any portion of the movement or pain with the corresponding clearing test. The sum of the 7 movement patterns is used to assess differences between groups and when testing bilaterally the lower score of the two limbs is used for total score calculation (max = 21). Asymmetry is noted in the 5 movements performed bilaterally: Hurdle step, inline lunge, shoulder mobility, active straight leg raise, and rotational stability. Asymmetry is calculated as the absolute difference between the right and left side with each of these movements.
Figure 1.
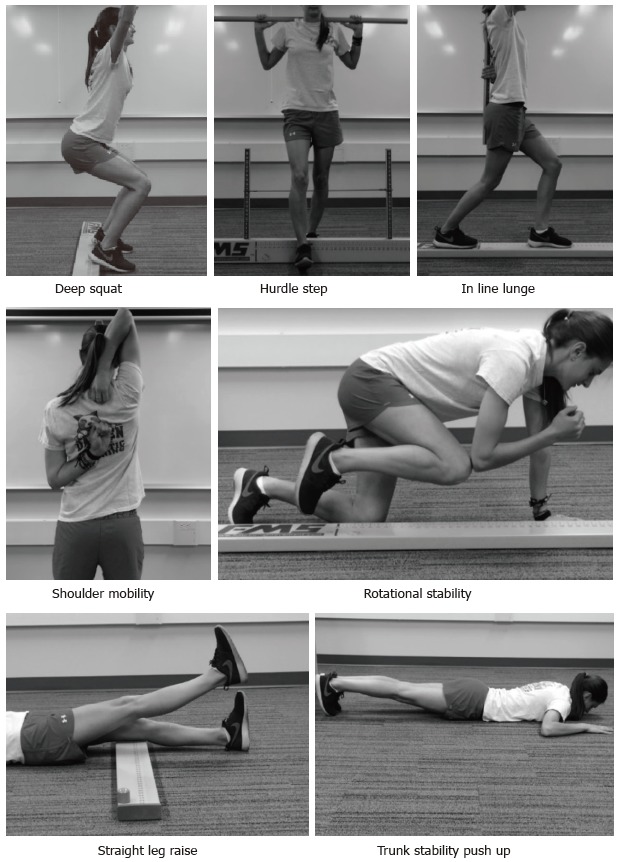
Images of the Functional Movement Screen.
Table 1.
Fundamental movement patterns of the Functional Movement Screen™ and the associated clearing tests
| Fundamental movement pattern | Clearing test |
| Deep squat | |
| Hurdle step1 | |
| Inline lunge1 | |
| Shoulder mobility1 | Shoulder impingement test |
| Active straight leg raise1 | |
| Trunk stability push-up | Spinal extension test |
| Rotatory stability1 | Spinal flexion test |
Performed and scored separately for the right and left side.
The benefits of the FMS are that it is quick, inexpensive, and easy to administer. This screen is clinically relevant in that minimal equipment and training are required to administer and score the FMS, and a standard testing protocol is readily available[5,6]. The FMS testing takes between 12-15 min to administer and score, making this a viable option for many. The FMS test kit (Functional Movement Systems, Inc., Chatham, VA) is approximately $180.00, making it accessible for a wide variety of clinical and performance settings. Reliable and consistent scoring has been shown with just a 2 h training session[7], again enhancing the use with a variety of fitness and healthcare professionals in different settings.
Five studies utilizing varied samples have calculated normative values for the summed total FMS in the last 5 years[8-12]. Two of the studies focused on small samples of participants in specific sports, hurling and Gaelic football (n = 62)[8], and running (n = 43)[9]. The normative value for the total FMS score in both of these studies was very similar (15.6 ± 1.5 for the hurlers and Gaelic football players and 15.4 ± 2.4 in the runners). Teyhen et al[11] reported a higher normative value for 247 male and female active service members at 16.2 ± 2.2. There was a significant age by sex interaction (P = 0.007) with higher scores in females and younger ages. The largest sample (n = 622) of 21 years and older included males and females in the general population and reported age and sex stratified FMS scores[10] in general FMS scores decreased with age and females had higher average FMS scores compared with men. Although a large study overall, care should be taken with application of this population-based study since some of the age/sex categories were very small (for example: n = 34 for females 50-54 years old). Finally, normative data in a large (n = 209) sample of 18-40 years old physical active males and females reported an average FMS score of 15.7 ± 1.9[10]. Taken together, for young to mid-life physically active males and females, normative FMS falls between 15.4 and 16.2 points. Lower FMS overall scores were reported for older ages[12]. No differences in overall score between males and females were reported[9,10,13], but sex differences were seen with specific movement patterns[13].
The validity of the FMS has been assessed in several ways. First, for a screening test to be valid it must first be reliable. The reliability has been examined in several studies, and these studies have recently been summarized[14]. Table 2 on Page 3574 gives an excellent summary of the FMS reliability studies[14]. Additionally, we previously studied inter- and intra-rater reliability of the FMS after a single 2 h training session[7]. Four raters with different experience with FMS, and education scored 20 recreational athletes (10 males and 10 females) and then re-scored a week later. Two raters were experienced with FMS - one was a Physical Therapy (PT) student, and one was a cross country coach (also FMS certified). The 2 inexperienced FMS administrators were a faculty member in Athletic Training and a PT student. Inter-rater reliability was good for session 1 (ICC = 0.89; 95%CI: 0.80-0.95) and for session 2 (ICC = 0.87; 95%CI: 0.76-0.94). Intra-rater reliability was good for each rater, ranging from 0.81 to 0.91.The conclusions of this study are similar to others who assessed real-time, clinically applicable (i.e., not video recorded) FMS reliability[15-17].
Table 2.
Results of studies using Functional Movement Screen™ score of 14 as a cut point to predict musculoskeletal injuries
| Ref. | Sample | Injury definition | Sensitivity | Specificity | +LR | -LR |
| Kiesel et al[22] | 46 male professional American football players | Athletic performance injury requiring injury reserve and time loss of 3 wk | 54% | 91% | NR | NR |
| Chorba et al[23] | 38 female Division II athletes | Athletic performance injury requiring intervention | 58% | 74% | 2.20 | NR |
| O’Connor et al[24] | 874 male Officer candidates | Any injury: Physical training injury requiring intervention | 45% | 78% | NR | NR |
| Overuse injury: Long term repetitive energy exchange with cumulative microtrauma | 12% | 90% | NR | NR | ||
| Serious injury: Physical training injury requiring removal from training | 12% | 94% | NR | NR | ||
| Butler et al[25] | 108 firefight trainees | Physical training injury with time loss of 3 consecutive days | 84% | 62% | 2.20 | 0.26 |
| Warren et al[26] | 195 male and females Division I athletes | Athletic performance injury requiring intervention | 54% | 46% | NR | NR |
| Garrison et al[27] | 160 male and females Division I athletes | Athletic performance injury requiring intervention, and 24 h missed time or splinting, to continue participation | 67% | 73% | 2.51 | 0.45 |
| Hotta et al[28] | 84 competitive male runners | Physical training injury with time loss of 4 wk | 73% | 54% | NR | NR |
| Knapik et al[29] | 1045 male and female military cadets | Physical training injury | 55% | 49% | NR | NR |
| McGill et al[30] | 53 elite police officer | Back injury not due to specific acute incidents | 28% | 76% | NR | NR |
| All injury | 42% | 47% | NR | NR |
LR: Likelihood ratio.
The FMS has good face validity with movement experts (i.e., physical therapists and athletic trainers) as the developers of the screen[5,6]. The content validity is not known for much of the screen. One of the movement patterns - deep squat - has a published biomechanical analysis[18]; it is currently not known what is occurring biomechanically with the other 6 movement patterns. Recently, the inline lunge was compared with measures of power, speed, and balance and no significant correlations were found[19], pointing to the need for further research into what is occurring with each movement pattern.
The FMS has evolved into a single score as a straight summation the scores of the 7 fundamental movement pattern into a single score, ranging from 0-21. In this scoring algorithm, for those patterns performed bilaterally, the lower score of the right and left sides is used, and all patterns are equally weighted. Three of the movement patterns in the FMS (deep squat, hurdle step, and inline lunge) are considered the “big three” with more complex movement patterns[5,6]. The other 4 are considered the “little four” and it is recommended to intervene with these patterns first before addressing the more complex movements. Despite this, the single summative score weights all 7 patterns equally.
The construct validity of a single value has been assessed recently with two factor analyses of the FMS. Kazman et al[20] administered the FMS to 934 Marine Officer candidates. With exploratory factor analysis, this study failed to show that FMS score was a unitary construct, calling into question the construct validity for a single score. No interpretable factor was found, and Cronbach’s alpha showed low internal consistency; all of the movement patterns had scores below the pre-defined cut-point, suggesting a lack of clustering of the FMS movement patterns. The concept of unidimensionality was further explored in a study of 290 elite Chinese athletes[21]; the results were consistent with Kazman et al[20], demonstrating a lack of unitary construct; this suggests that the summed score does not reflect one latent measure or one single result. The authors cautioned about the use of a single summed score, and instead suggested focusing on each movement pattern independently.
The single summed score (dichotomized as less than or equal to 14 vs greater than 14) has been reported in several prospective cohort studies about the validity of the FMS to predict musculoskeletal injury (Table 2)[22-30]. Most of the studies reported low sensitivity[22-24,26,29] that is the proportion of the sample who sustained an injury with a score less than or equal to 14 (approximately 50%). This means an equal proportion of the sample who sustained an injury scored above 14 or 14 or less. These studies had a variety of injury definitions and studied samples, including professional and collegiate athletes, and military personnel. Two studies[25,28] reported sensitivity above 70%. Hotta et al[28] studied 84 competitive male runners, and with an injury definition of a training related injury resulting in time loss for 4 wk, the sensitivity of the dichotomized FMS score to predict injury was 73%. Butler et al[25] reported a sensitivity of 84% for the dichotomized FMS score and injuries related to training and requiring 3 consecutive days of missed training in 108 firefighter trainees. Therefore, perhaps the FMS is more sensitive for predicting more serious injuries requiring time loss from training, although other studies with this injury definition reported low sensitivity[22,24]. The specificity, or the proportion of the studied samples who did not sustain an injury with a FMS score greater than 14 was far more varied, ranging from 46%[26] to 91%[22], so it is difficult to make any definitive conclusions about the specificity. It is evident that there is not a consensus on the ability of the FMS as a single score to predict injury. Part of this is due to the differing samples studied and injury definitions used, as well as the recent studies pointing to the caution with a single FMS score[20,21]. Additionally, several studies reported an inability to find a point on the receiver operator characteristic (ROC) curve that maximized sensitivity and specificity for the studied sample[24,26], and defaulted to 14 as a cut-point based on previously published literature.
Three of the aforementioned studies prospectively assessed the association of each movement pattern with injury[25,26,28]. Butler et al[25] reported a significant association between 3 d time loss injuries and deep squat (OR = 1.21; 95%CI: 1.01-1.42) and push-up (OR = 1.30; 95%CI: 1.07-1.53) and Hotta et al[28] reported a significant association between 4 wk time loss injury and deep squat and active straight leg raise analyzed together (OR = 9.7; 95%CI: 2.1-44.4). Conversely, Warren et al[26] found no significant association between individual movement patterns and injury. It is obvious that further work is required to determine the validity of the FMS to predict injury, either as a summed single score, or perhaps more appropriately as individual movement patterns.
Finally responsiveness, or the ability of an instrument to accurately detect change when it has occurred[31] is closely related to validity and informs the accuracy of an instrument. The ability of the FMS to improve in response to an intervention has been reported in 4 studies of 3 samples[32-35]. In both American football players (n = 62)[35] and mixed martial arts athletes (n = 25)[32], an intervention of corrective exercise was designed based on baseline FMS scores. After 7 wk, the American football players improved the FMS overall score by approximately 3 points (P < 0.001) and had a significant decrease in the number of participants with asymmetrical movements with the 5 bilateral FMS movement patterns (P = 0.01)[35]. Bodden et al[32] compared an 8 wk intervention program to a control group and reported a significant time by group interaction (P < 0.001). The intervention group improved overall FMS score by approximately 2 points compared with no change in the control group. The change score reported in both of these studies appears to be consistent with a proposed Minimally Clinically Important Difference of 1.25 for the FMS score[13]. Conversely, a study in 60 firefighters comparing 2 different interventions with a control group found no significant changes in FMS score after a 12 wk intervention (P = 0.18)[33,34]. Additionally, no difference in number of participants with asymmetry was found (P = 0.53).
Despite the popularity, the evidence for the FMS is conflicting, limiting the ability to make definitive recommendations for use. It is a reliable instrument and clinicians should feel comfortable with the consistency of the scoring criteria. Caution should be exercised in using a single summed FMS score or a specific cut-point for injury. As an injury prediction screen, the validity was most accurate with firefighters[25], but firefighters’ scores were not responsive to an exercise intervention designed to prevent injury[33,34]. American football players’ scores were very responsive to an intervention[35], and despite low sensitivity an FMS score 14 or less was significantly associated with time loss injuries (OR = 1.87; 95%CI: 1.20-2.96)[36]. Additionally, two studies have failed to show a significant difference in FMS scores between injured and uninjured[25,37]. Although there have been over 60 papers published on the accuracy and use of the FMS in the last 5 years, the only clear conclusions are that the FMS is reliable and appears to have good utility in professional American football players as a single summed score. Although this editorial included studies on adults only, there have been a number of studies recently published on the use of FMS in adolescents. Further work is required here to determine if the similar findings occur in adolescents compared with adults.
STAR EXCURSION BALANCE TEST/Y BALANCE TEST
The Star Excursion Balance Test (SEBT) (Figure 2) was first described in the literature for research purposes more than 15 years ago[38]. Since this time a PubMed search shows that approximately 150 publications have utilized this tool for assessing dynamic balance across numerous populations. The SEBT assesses dynamic single leg balance while reaching in 8 reach directions based on the orientation of the stance limb: Anterior, posterior, medial, lateral, anterior lateral, anterior medial, posterior lateral, and posterior medial. The SEBT was first suggested to be modified based on redundancy, as a result of large amount of shared variance, across the 8 reaching directions; this was identified through a factor analysis of SEBT performance in participants with chronic ankle instability[39]. This led to the suggestion of three reach directions, anterior, posterior medial, and posterior lateral rather than needing to perform all eight from the original SEBT[40].
Figure 2.
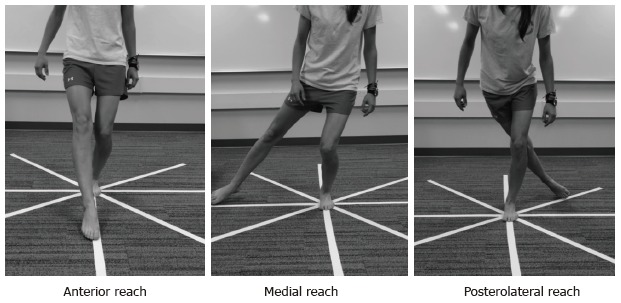
Images of the Star Excursion Balance Test.
The SEBT is performed by placing strips of tape on the floor in a grid format while the participant stands in the middle of the grid and reaches as far as possible in one reach direction touching down lightly so the researcher can mark and subsequently measure the reach distance. Trials are considered successful when there is no movement in the stance limb during performance of the SEBT, controlled motion while maintaining balance, and returning of the reaching limb back to the starting point[39]. The Y Balance Test (YBT) (Figure 3), an instrumented, proprietary version of the modified three reach SEBT, first appeared in the literature in 2009 with the intent of improving test repeatability[41]. This device is made of PVC piping and has a center platform the participant stands on while reaching with the contralateral limb and lightly pushing a reach indicator as far as possible along a PVC piping tube. Scoring for both the modified SEBT and YBT involve determining the farthest reach in each of the three reach directions (anterior, posteromedial, and posterolateral) and creating a normalized composite reach score (CS), a normalized single direction reach, and/or a single reach direction asymmetry measurement. The normalized (by participant’s leg length) reach distance has been recommended for comparison because performance differences may be a result of anthropometric characteristics[42]. The normalized CS, expressed as a percent, is calculated by averaging the maximum reach in each of the three reach directions, dividing this number by 3 times leg length (LL)[43]. The normalized single reach direction is also expressed as a percent, and is calculated by taking the maximum reach in the single reach direction, dividing this number by LL[42]. The single reach direction asymmetry measurement is calculated as the absolute difference in centimeters between the right and left limb for a single reach direction[43].
Figure 3.
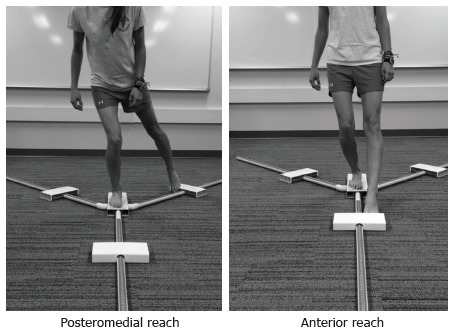
Images of Y Balance Test.
A review of the literature suggests that inter-rater reliability of the YBT is slightly higher than the SEBT for the normalized reach distances [ICC 0.99-1.00 (95%CI: 0.92-1.0)[41] vs 0.89-0.94 (95%CI: 0.80-0.95)][44] and the CS [ICC range 0.97-0.99 (95%CI: 0.92-0.99)[41] vs 0.92 (95%CI: 0.85-0.96)][42]; it should be noted that both the YBT and SEBT have very good inter-rater reliability. Intra-rater reliability appears similar between the YBT normalized reach directions [ICC range = 0.85-0.91 (95%CI: 0.64-0.95)][41] and the SEBT (ICC range = 0.84-0.92; 95%CI: not reported)[45]. For the YBT CS, Plisky et al[41] reported intra-rater reliability to be high (0.91 95%CI: 0.69-0.96); however, Munro et al[45] did not report the ICC for the SEBT CS; therefore, a direct comparison of intra-rater reliability for the CS cannot be made between the YBT and SEBT.
While it appears that using an instrumented device to measure dynamic balance (i.e., YBT), may have a higher overall reliability, there is one main difference in the protocols between the YBT[41] and SEBT[38]. The YBT allows for stance foot movement during performance of dynamic reaching. Although this may seem like a subtle difference in protocol, there have been two studies to date that have found differences in performance and kinematics during a direct comparison of the YBT and SEBT performance[46,47]. Participants reached further in SEBT anterior reach compared to YBT anterior reach[46]; while utilizing less hip flexion[47]. The development of the YBT was based on the SEBT; however, differences in performance may suggest that these two tests are not as similar as previously thought and that there needs to be more research to assess neuromuscular differences between these two dynamic balance tools before assuming that findings from the SEBT translate to the YBT.
The normalized reach distance, composite score, and reach distance asymmetry may seem like reasonable means for comparing the SEBT and YBT performance, little attention has been dedicated to the validity of these measurements. In fact, a factor analysis has yet to be performed. Interestingly, dynamic balance differences have been noted between sexes[13,48], ages[49], countries of origin[50], sport participation[51], and sport level[52]. Further, Lehr et al[53] assessed risk of noncontact injury based on YBT performance in 183 Division III athletes from 10 NCAA sports teams and recommended that injury risk should be based on sport, sex, and age.
Despite the numerous publications involving the use of the SEBT and the YBT, there are only 4 published studies that have used one of these tools to determine sport injury risk. In a study on lower extremity noncontact injury risk in high school athletes, Plisky et al[43] demonstrated that a CS of less than 94% LL resulted in a 6.5 times greater odds (95%CI: 2.4-17.5) of lower extremity injury female high school athletes and an anterior reach asymmetry of more than 4cm resulted in a 2.7 times greater odds (95%CI: 1.4-5.3) of lower extremity injury in all high school athletes (n = 235; 30 boys, 105 girls). Butler et al[54] found that lower extremity noncontact injury risk was 3.5% higher (95%CI: 2.4-5.3) in collegiate Division III football players (n = 59) with a CS of less than 89.6% LL. In this study ROC analysis revealed that a composite score 89.6% LL maximized sensitivity (100%) and specificity (71.7%); however, ROC analysis of reach asymmetry did not find an ideal cut point for identifying injury risk[54]. Conversely, Smith et al[55] also used the YBT to assess risk of injury based on YBT performance in 184 Division I athletes from 13 NCAA sports teams and found that noncontact injury was associated with 4 or more cm of anterior reach asymmetry (OR = 2.33; 95%CI: 1.15-4.76). This study used an ROC curve and determined that 4 cm was the optimal cut point (sensitivity: 59%; specificity: 72%) for predicting injury; interestingly, ROC curve failed to maximize sensitivity and specificity for composite score; there was no relationship between CS and injury[55]. Lastly, Olivier et al[56] found no difference in SEBT composite score between cricket pace bowlers who sustained lower extremity injury and those that did not (n = 32, 17 injured-left leg: 79.65% LL vs 83.26% LL; P = 0.16; right leg: 78.70% LL vs 81.59% LL; P = 0.18); however, those who were injured performed significantly worse on the normalized posteromedial reach direction than those who were not injured (90.07% LL vs 91.26% LL; P = 0.02). In this study of cricket pace bowlers all injuries that resulted in time loss of at least one day or required the bowler to quit activity in which they had already started was included; this implies that all injuries were included rather than just non-contact injuries. Additionally, the authors did not report reach asymmetry differences in this study, which combined with the inclusion of all injuries, makes comparison between this and previous studies difficult. It should be noted that the CS in the cricket bowling study[56] were lower than those reported in the previous studies in which noncontact injury was associated with CS performance of lower than 94%[43] or 89.6%[54].
To date 7 studies have evaluated the effects of dorsiflexion range of motion[57,58], sex and injury history[13], and interventions on SEBT/YBT performance[59-62]. Forty-five individuals (12 males; 33 females with chronic ankle instability and reduced dorsiflexion range of motion had significant, but low positive correlations with performance on the SEBT CS (r = 0.30, r2 = 0.09, P = 0.02) and normalized anterior (r = 0.55, r2 = 0.31, P < 0.001) and posterolateral (r = 0.29, r2 = 0.09, P = 0.03) reach[57]. Further, Hoch et al[58] reported that dorsiflexion range of motion as measured by the weight bearing lunge test (n = 35; 14 males; 21 females) explained 28% of the variance in the normalized anterior reach of the SEBT leading the authors to suggest that the anterior reach of the SEBT may be a good test to determine the effects of dorsiflexion limitations on dynamic balance performance. While it does not appear that males (n =103) and females (n = 87) perform differently on YBT CS (102% ± 8% vs 100% ± 6%; P = 0.05), males have been reported to have a significantly greater anterior reach asymmetry compared to females (4.4 ± 6.7 cm vs 2.7 ± 2.3 cm; P = 0.02)[13]. Additionally, one study indicated that history of injury or surgery did not affect YBT CS or asymmetry; however, those who reported a back or trunk injury had greater variability in asymmetry in the anterior and posterior medial reach directions[13]. This finding is particularly interesting as trunk stability exercises (front plank, quadruped, and back bridges) have been demonstrated to provide immediate improvement in normalized SEBT CS (94.0% ± 4.8% vs 96.8% ± 5.7%; P < 0.001) and posterolateral (102.8% ± 7.3% vs 106.2% ± 8.1%; P = 0.002) and posteromedial (105.3% ± 5.8% vs 109.8% ± 6.4%; P < 0.001) reach directions (n = 11)[59]. Additionally, after 12 wk of trunk stability exercises, 27 soccer players demonstrated improvement in normalized posteromedial (101.5% ± 7.2% vs 110.0% ± 9.3%; P = 0.013) and posterolateral (96.2% ± 12.9% vs 104.7% ± 8.1%; P = 0.02)[60]; while an 8 wk lower extremity neuromuscular training program focused on core stability and lower extremity strength improved SEBT CS (right: Pre-training-96.4% ± 11.7% vs post-training-104.6% ± 6.1%; P = 0.03; left: Pre-training-96.9% ± 10.1%; post-training: 103.4% ± 8.0%; P = 0.04) in 20 uninjured soccer players (13 experimental; 7 control)[61]. Interestingly, Ambegaonkar et al[63] found that hip strength, rather than core endurance (McGill’s Core Endurance Tests), was associated with SEBT performance in 40 collegiate female lacrosse and soccer athletes. Additionally, Garrison et al[62] reported a significant decrease in anterior reach asymmetry tested with the YBT in participants with ACL reconstruction after 12 wk of a traditional rehabilitation plus isolated hip strengthening rehabilitation (n = 22) compared to those in traditional rehabilitation (n = 21) only (2.7 ± 2.9 vs 6.1 ± 4.6; P = 0.008).
These differences between groups and studies may suggest the types of analytic comparisons currently being conducted to determine differences between groups when performing the YBT/SEBT may not fully capture the risk of injury attributable to dynamic balance performance. In taking into consideration all of the studies presented here it appears that anterior reach asymmetry is most affected in terms of sex differences and dorsiflexion range of motion; while core training appears to help mitigate performance differences. Additional research is needed in regards to the CS as there are differences in the maximized cut-point to use for injury prediction; however anterior reach asymmetry of 4 or more cm appears to consistently predict non-contact injury risk. It is also important to consider that there are a number of factors that contribute to dynamic balance performance and thus may need to be accounted for when assessing injury risk based on lower extremity dynamic balance.
DROP JUMP TEST
The Drop Jump Test (Figure 4) has been described in the literature as a tool to evaluate landing patterns from a clinical perspective using either the DJST or the LESS.
Figure 4.

Images of the Drop Jump Screening Test. Participants drop off of the box and upon landing on the ground they are asked to immediately explode up in to a vertical jump. Image is at max height of vertical jump.
DJST
The DJST is a clinical used to assess dynamic knee valgus on landing from a 30.48 cm height and immediately exploding into a vertical jump via a simple frontal plane video analysis of normalized knee joint separation distance (calculated as knee separation distance/hip separation distance); it was first described in the literature approximately 10 years ago[64]. This tool was designed based on the group’s prior work[65], which assessed landing mechanics in youth athletes[64]. This test uses reflective markers placed bilaterally on the greater trochanter, center of the patella, and lateral malleolus to determine differences in hip, knee, and ankle joint separation during three phases of the drop jump: Pre-landing, landing, and take-off. At the completion of three jumps, the researcher chooses the best representative jump and analyzes the jump frame by frame to identify the pre-landing, defined as the frame when the athlete’s toes just touch the ground after the jump from the box, the landing, defined as the frame in which the athlete has the greatest amount of knee flexion, and the take-off, defined as the frame in which there is initial upward movement to initiate the vertical jump[64]. For each of the three identified frames listed previously, the researcher uses a proprietary software (Valgus Digitizer, Sportsmetrics™ Software for Analysis of Jumping Mechanics, Cincinnati, OH) to digitize the marker points; from the digitized points the software computes absolute difference between right and left hips and normalized difference between right and left knees (knee separation distance/hip separation difference) and ankles (ankle separation distance/hip separation difference)[64]. Less than 60% normalized knee joint separation is representative of abnormal frontal plan knee valgus alignment[64].
Three studies[64,66,67] have evaluated sex differences in the DJST with one documenting no difference between females and male in normalized knee separation distance at landing (51% ± 19% vs 51% ± 15%; P > 0.05) and take-off (50% ± 18% vs 53% ± 15%; P > 0.05); however, females demonstrated higher normalized knee separation distance than males during the pre-landing phase (63% ± 14% vs 59% ± 11%; P < 0.0001)[64]. Barber-Westin et al[66] also demonstrated no differences in normalized knee separation distance between sexes across various age groups from 9-17 years of age. In another study of a similar population, females had significantly lower knee-hip ratio (0.45 vs 0.63; P = 0.003) (standard deviations were not reported)[67].
In the inaugural study[64] using the DJST to analyze knee joint separation as a means for defining dynamic knee valgus the authors reported the tool is reliable as demonstrated in the following. On a subset of 17 participants who underwent a second DJST 7 wk after the first screening hip joint separation reliability was assessed to provide support for the normalized differences. The authors also presented a subset of another 10 participants in which 2 of the 3 trials were tested for reliability of absolute separation of the hip, knee, and ankle. The ICCs for hip joint separation were reported as very high at pre-landing (0.96), landing (0.94), and take-off (0.94). The ICCs for absolute separation of the hip, knee, and ankle were reported as all being ≥ 0.90.
Several studies have been published evaluating the effects of neuromuscular training program on the DJST; however, all studies have arisen from the same research group. Further, the validity of such a measurement (knee joint separation) to indicate dynamic knee valgus has never been established. In response to the validity of the DJST, Dr. Noyes and Ms. Barber-Westin state in a Letter to the Editor[68] that “our investigations show the dramatic differences (in landing appearance) between knees with ≤ 60% and those with > 60% normalized knee separation distance”. While this does not actually demonstrate that the DJST is a valid measure, there are documented improvements in knee joint separation following neuromuscular training programs in a variety of different athletes[69-71].
Thirty-four female high school volleyball players took part in a 6 wk sport specific neuromuscular training program, which resulted in significant increases in absolute knee separation (21.1 ± 8.2 cm vs 25.9 ± 5.2 cm; P = 0.002) and mean normalized knee separation distance (56.3% ± 19.1% vs 63.3% ± 12.7%; P = 0.04)[69]. Sixty-two female high school soccer player participated in a 6 wk sport specific neuromuscular training program and had post training increased ankle (27.3 ± 6.3 cm vs 34.6 ± 6.0 cm; P < 0.0001) and knee (14.6 ± 3.6 cm vs 23.1 ± 24.7 cm; P < 0.0001) absolute separation distance and normalized knee separation distance (35.9% ± 7.4% vs 54.2% ± 13.7%; P < 0.0001) when completing the DJST[71]. Fifty-seven female high school basketball players demonstrated increased absolute knee separation (18.5 ± 7.4 cm vs 31.8 ± 10.4 cm; P < 0.0001) and mean normalized knee separation distance (44.9% ± 17.2% vs 74.2 %± 18.8%; P < 0.0001) following 6 wk of neuromuscular training[70]. Based on the previous suggestion that less than 60% normalized knee separation distance indicating dynamic knee valgus[64]; these findings suggest that a more neutral knee alignment was achieved at landing following the sport specific neuromuscular training programs in female high school volleyball, soccer, and basketball athletes. Additionally, improvements in landing alignment were maintained at 12 mo after a 6 wk neuromuscular training program in approximately 70% of female volleyball players[72]. It is important to note that although the results of the aforementioned studies suggest that landing alignment may be altered following a specific training program; there remains a lack of literature on the validity of the DJST and to date this screening tool has not be used to predict injury risk.
LESS
The LESS is similar to the DJST in the test procedures with the exception that participant’s jump landing is video recorded from both the frontal and sagittal planes. In addition, when performing the drop jump landing for the LESS, participants jump from a 30-cm height jump to land on the floor at a distance that is 50% of their height away from the box and then immediately perform a maximal vertical jump. In the LESS, which was first described in the literature approximately 6 years ago[73], participants are scored offline via a 17 item clinical tool evaluating “landing error” (Table 3) to identify movement patterns that lead to increased ACL injury risk. Newer studies demonstrate the use of real time scoring of four jumps using a modified version of the LESS (LESS-RT) with the scorer evaluating 10 errors during 4 participant jumps (Table 4)[74] and real time scoring using a single jump and the iLESS scoring (Table 5)[75].
Table 3.
Landing Error Scoring System scoring criteria
| LESS item | Operational definition of error |
| Knee flexion: Initial contact | Knee is flexed less than 30° at initial contact |
| Hip flexion: Initial contact | Thigh is in line with the trunk at initial contact |
| Trunk flexion: Initial contact | Trunk is vertical or extended on the hips at initial contact |
| Ankle plantar flexion: Initial contact | Foot lands heel to toe or with flat foot at initial contact |
| Medial knee position: Initial contact | Center of patella is medial to midfoot at initial contact |
| Lateral trunk flexion: Initial contact | Midline of trunk flexed to left/right side body at initial contact |
| Stance width: Wide | Feet positioned > shoulder width apart at initial contact |
| Stance width: Narrow | Feet positioned < shoulder width apart at initial contact |
| Foot position: External rotation | Foot is internally rotated more than 30° between initial contact and maximum knee flexion |
| Foot position: Internal rotation | Foot is externally rotated more than 30° between initial contact and maximum knee flexion |
| Symmetric initial foot contact | One foot lands before other or one foot lands heel to toe and other lands toe to heel |
| Knee flexion displacement | Knee flexes less than 45° between initial contact and max knee flexion |
| Hip flexion displacement | Thigh does not flex more on trunk between initial contact and maximum knee flexion |
| Trunk flexion displacement | Trunk does not flex more between initial contact and maximum knee flexion |
| Medial knee displacement | At maximum medial knee position, the center of patella is medial to midfoot |
| Joint displacement | Soft: Participant demonstrates large amount of trunk, hip, and knee displacement Average: Participant has some but not large amount of trunk, hip, and knee displacement Stiff: Participant goes through very little, if any, trunk, hip, or knee displacement |
| Overall impression | Excellent: Participant displays soft landing with no frontal or transverse plane motion Poor: Participant displays large frontal or transverse plane motion, or participant displays stiff landing with some frontal or transverse plane motion Average: All other landings |
Flaws 1-15 scored as present: 1 and absent = 0; Flaw 16 scored as soft: 0, average = 1, stiff = 2; Flaw 17 scored as excellent: 0, average = 1, poor = 2. LESS: Landing Error Scoring System.
Table 4.
Landing Error Scoring System scoring criteria real-time
| LESS RT item | Operational definition | View | Jump number |
| Stance width | Participant lands with very wide or very narrow stance (+1) | Front | 1 |
| Maximum foot-rotation position | Participants feet moderately externally or internally rotated at any point during the landing (+1) | Front | 1 |
| Initial foot-contact symmetry | One foot lands before the other or 1 foot lands heel-to-toe and other foot lands toe-to-heel (+1) | Front | 1 |
| Maximum knee-valgus angle | Participant moves into a small amount of knee valgus (+1); Participant moves into a large amount of knee valgus (+2) | Front | 2 |
| Amount of lateral trunk flexion | Participant leans to left or right so trunk is not vertical in the frontal plan (+1) | Front | 2 |
| Initial landing of feet | Participant lands heel to toe or with flat foot (+1) | Side | 3 |
| Amount of knee-flexion displacement | Participant goes through small (+2) or average (+1) amount of knee flexion displacement | Side | 3 |
| Amount of trunk-flexion displacement | Participant goes through small (+2) or average (+1) amount of trunk flexion displacement | Side | 4 |
| Total joint displacement in sagittal plane | Participant goes through large displacement of trunk and knees, score soft (0); Participant goes through average displacement of trunk and knees, score average (+1); Participant goes through minimal displacement of trunk and knees, score stiff (+2) | Side | All |
| Overall impression | Participant displays soft landing and no frontal plane motion at knee, score excellent (0); Participant displays stiff landing and large frontal plane motion at knee, score poor (+2); All other landings score average (+1) |
LESS: Landing Error Scoring System.
Table 5.
i-Landing Error Scoring System criteria
| Good movement pattern | Poor movement pattern |
| Lands with no knee valgus at initial foot contact | Lands with moderate to large knee valgus position at initial foot contact |
| Lands with no knee valgus displacement from initial contact to maximum knee flexion | Lands with moderate to large knee valgus displacement from initial contact to maximum knee flexion |
| Lands with > 30° of knee flexion | Lands with < 30° of knee flexion |
| Undergoes > 30° of knee flexion | Undergoes < 30° of knee flexion from initial contact to full knee flexion |
| Minimal to no sound upon landing | Loud sound upon landing |
The LESS demonstrated good to excellent reliability and was validated against the gold standard of three dimensional kinematic and kinetic analysis in a large study involving approximately 2700 military academy attendees[73]. Intra- (ICC = 0.91) and inter-rater (ICC = 0.84) reliability were established using a random subset of 50 from the initial study; concurrent validity was established by demonstrating that those participants with low LESS scores demonstrated less knee and hip flexion angle, increased knee valgus and hip adduction angle, increased internal knee and hip internal rotation moment, and anterior tibial shear force[73]. The importance of this work is that the authors demonstrated that a clinical movement screen can be used to identify landing errors in multiple planes. Further work has established that the LESS can be used by both novice and expert LESS raters with excellent reliability (overall score: ICC = 0.84; kappa statistics for individual items/landing errors ranged from 80%-100% agreement); however, the validity of the LESS (compared to 3 dimensional motional analysis) is dependent on the item/error being assessed based on Phi-correlation-coefficient analysis leading the authors to suggest that items/errors not valid should be reduced or eliminated from the LESS scoring criteria[76]. To enhance the utility of the LESS, the LESS-RT was developed and the reliability of the composite score (total of 10 errors) was assessed as being good both for interrater reliability (ICC = 0.81)[74]. To create a more efficient clinician screening tool, the iLESS was developed and allows for quicker assessment of large groups in a short amount of time, like a pre participation examination, and demonstrated a high level of agreement between novice and expert raters (iLESS: Kappa = 0.692, Agreement = 90%, P = 0.001; LESS: Kappa = 0.600, Agreement = 80%, P = 0.001) and with the LESS (novice: Kappa = 0.583, Agreement = 85%, P = 0.004; expert: Kappa = 0.500, Agreement = 75%, P = 0.01)[75].
Performance of the LESS is influenced by sex[77,78], fatigue[79], and previous ACL reconstruction[79-81]. In a large study of over 200 collegiate athletes, Lam et al[77] found that while males and females demonstrate similar overall LESS scores statistically, males performed worse on items 1, 4, 14 and females performed worse on items 5 and 15 and had more overall frontal plane movement and total errors. This study suggested that males demonstrate more sagittal plane landing errors while females display more frontal plane landing errors. Beutler et al[78] reported that females cadets had lower overall LESS scores compared to male counterparts (5.34 ± 1.51 vs 4.65 ± 1.69; P < 0.001); this study of 2753 participants also completed a factor analysis and determined that there are five groups of related errors: Factor 1: Knee (item 1), decreased hip (item 2), and trunk flexion (item 3) at initial contact; Factor 2: Knee valgus (item 5 and 15) and wide stance at initial contact (item 7); Factor 3: Toe out (item 10) and knee flexion at initial contact (item 1); Factor 4: Heel-to-toe landing (item 4) and asymmetric foot landing pattern (item 11); Factor 5: Reduced sagittal plane flexion during the landing phase (items 12, 13, and 14)[78]. T-tests between male and females suggested that females are significantly more likely to present with Factors 1, 2, and 5 (P < 0.001), while males had greater likelihood of Factors 3 and 4 (P < 0.001)[78]. Although not directly tested, the authors suggested that perhaps fatigue worsens movement patterns, which was validated by Gokeler et al[79] who demonstrated that after a fatigue protocol in participants with anterior cruciate ligament reconstruction (ACLR) and controls (no ACLR) performed worse on LESS total score compared to pre fatigue scores [median 7.0 (IQR: 4.3; 7.8) vs 5.0 (IQR: 2.0; 7.0); P = 0.001]. This study also assessed frequency of errors and found that post fatigue ACLR had a greater percentage of errors than control in knee flexion at initial contact, extension on the hips, lateral trunk flexion, and asymmetrical foot contact although the article did not state if these were significant differences[79]. Similarly, Kuenze et al[80] and Bell et al[81] demonstrated that ACLR have significantly lower total LES scores than healthy controls (6.0 ± 3.6 vs 2.8 ± 2.2; P = 0.002 and 6.7 ± 2.1 vs 5.6 ± 1.5; P = 0.04, respectively).
Recent evidence suggests that the LESS can be modified through training[82-84] and it can also be used to identify those at risk for injury[85,86]. Following completion of a military course designed to improve performance in military tasks, cadets had significant improvement in LESS scores (5.01 ± 1.83 vs 4.48 ± 1.97; P < 0.001)[81]. Similarly, completion of an 8 wk program including progressive resistance exercise and core stability, power, and agility exercises participants performed better on the LESS compared to those who participated in an program that consisted of progressive resistive upper and lower extremity exercises only (pretest: 3.90 ± 1.02, posttest: 3.03 ± 1.02; P = 0.02)[83]. However, length of training appears to impact retention of improved performance on the LESS as participants taking part in 9 mo of training maintained movement pattern changes after 3 mo of no training while those that participated in 3 mo of training did not[84].
A very recent report suggests that LESS scores can be used to predict ACL injury risk[85]; however, this is in contradiction to a slightly older study in which LESS scores were unable to predict ACL injury[86]. Smith et al[86] was unable to determine a relationship between ACL injury risk and LESS score in a large study of over 5000 collegiate and high school athletes (OR = 1.04 per unit increase in LESS score; 95%CI: 0.80-1.35). Padua et al[85], however, was able to identify through ROC analysis that the optimal cut-point for LESS scoring as a predictor of ACL injury was 5.17 (sensitivity: 86%, specificity: 71%) using a sample of 829 youth elite soccer players. Athletes who sustained ACL injury had higher LESS scores than those that did not (6.24 ± 1.75 vs 4.43 ± 1.71; P < 0.005) and those athletes who had a LESS score of 5 or more had a 10.7 greater risk ratio than those who scored less than 5[85].
The LESS is a reliable tool that appears to have validity although caution should be taken as there may be some items/errors that are not completely validated. Clinicians should account for sex, fatigue, and previous ACLR as these all have demonstrated effects on LESS performance. Further, various types of training programs may improve LESS performance, which may influence ACL injury rate although more studies are warranted at this point.
TJA
The TJA (Figure 5) is a clinical test developed to identify lower extremity landing technique flaws during a plyometric activity[87,88]. The TJA is a quick (10 s) assessment of repetitive tuck jump performance, requiring a high level of effort, which may result in fatigue. The TJA is video recorded in the sagittal and frontal plane and is scored from the recording allowing assessment in slow motion and repeated viewings. There are 10 technique flaws (Table 6) scored as either present or absent during the TJA[87,88].
Figure 5.
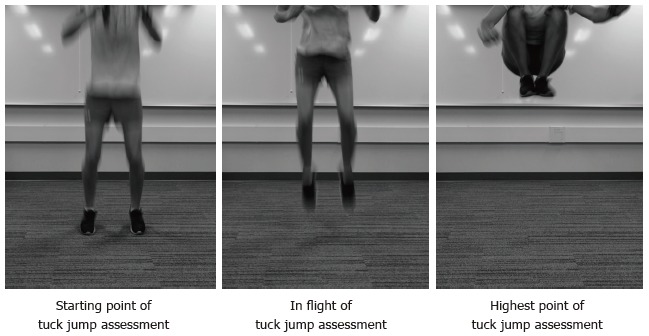
Images of the Tuck Jump Assessment.
Table 6.
Technique flaws of the Tuck Jump Assessment
| Lower extremity valgus at landing |
| Thighs do not reach parallel (peak of jump) |
| Thighs not equal side-to-side (during flight) |
| Foot placement not shoulder width apart |
| Foot placement not parallel (front to back) |
| Foot contact timing not equal |
| Excessive landing contact noise |
| Pause between jumps |
| Technique declines prior to 10 s |
| Does not land in same footprint (excessive in-flight motion) |
The benefits of the TJA are that it is a quick, inexpensive, and easy to administer. Two off-the-shelf video camera, tripods, and marking tape are all that is required to complete this test. The cameras must allow full visualization of the trunk and lower extremities with jumping and landing, so this test can be completed with minimal space requirements (8’ x 8’). The TJA takes no more than 2 min to administer, and no more than 10 min to score, making this a viable option for many.
There is limited literature published on the TJA (the 10 s test). A PubMed search using the search terms (“tuck jump assessment” OR “tuck jump”) yielded only 7 results that included the TJA. Despite the lack of evidence, this assessment is widely used clinically based on anecdotal information from PTs, ATs, and performance specialists.
There are 3 studies assessing the reliability of the TJA. The first assessed a different version of the scoring of the TJA[89]. A continuous 10 cm scale was used for 8 technique flaws and reported an intra-rater reliability correlation of 0.84 (range 0.72 -0.97). The TJA scoring was modified to dichotomize the technique flaws (10 rather than the initial 8) to enhance reliability[87], and is the test used in the 2 more recent TJA reliability articles[90,91]. Two raters (including 1 of the developers of the TJA) initially examined inter- and intra-rater reliability in 10 participants 1 mo apart[90]. Excellent inter-rater reliability was reported with high percentage exact agreement (PEA) between the 2 raters (93%, range 80%-100%) and Kappa of 0.88 indicating good/excellent agreement. Intra-rater reliability was also excellent with PEA 96% and 100% for the 2 raters for male participants and average of 87.2% for female participants. Both of these raters are experts and highly educated in movement science, and one of the raters developed the test. Therefore, these excellent results may not generalize to the variety of clinicians who employ the TJA. We examined inter- and intra-rater reliability in 40 participants using 5 raters of different educational backgrounds and clinical experience (PT and PT students, AT, and strength and conditioning coach)[91]. All raters were given instructions, Myer et al[88] that describes the TJA and scoring in detail, as well as a scored, example TJA previously scored and consensus achieved by the researchers. Inter-reliability between the 5 raters was poor (ICC = 0.47; 95%CI: 0.33-0.62). Incidentally, the 3 raters who completed the intra-rater reliability improved the inter-rater reliability on the second scoring 1 wk later (ICC = 0.52; 95%CI: 0.35-0.68 for scoring 1 vs ICC = 0.69; 95%CI: 0.55-0.81). This improvement in consistency amongst raters may be due to a learned effect with the scoring criteria. Intra-rater ICC (95%CI) was varied for the 3 raters, ranging from 0.44 (0.22-0.68) to 0.72 (0.55-0.84). Surprisingly, the most consistent rater was a 1st year PT student with very little experience in movement analysis. The difference in reliability between these 2 studies highlights the need for more research on TJA for consistent use clinically.
The validity of the TJA has not been formally assessed. Again, the face validity is unquestioned as the developers are movement specialists and have an extensive body of literature on lower extremity biomechanics published from the lab[88,92-94]. Furthermore, Myer et al[88] presented a categorization of the 10 TJA technique flaws into five different modifiable risk factors: Ligament dominance, quadriceps dominance, leg dominance or residual injury deficits, trunk dominance (“core” dysfunction), and technique perfection (Table 7). Biomechanical research provided some support for these risk factor categorizations[94], but this has not been assessed clinically or statistically. The responsiveness was also recommended that anyone with 6 or more flaws should be targeted for preventive intervention[88], but no data were presented to justify that recommendation.
Table 7.
Categorization of 10 technique flaws from the Tuck Jump Assessment into modifiable risk factors
| Modifiable risk factor | Description | Technique flaws |
| Ligament dominance | “Imbalance between the neuromuscular and ligamentous control of the dynamic knee stability” | Lower extremity valgus at landing |
| Foot placement not shoulder width apart | ||
| Quadriceps dominance | “Imbalance between knee extensor and flexor strength, recruitment, and coordination” | Excessive landing contact noise |
| Leg dominance or residual injury deficits | “Imbalance between the 2 lower extremities in strength, coordination, and control“ | Thighs not equal side-to-side (during flight) |
| Foot placement not parallel (front to back) | ||
| Foot contact timing not equal | ||
| Trunk dominance/core dysfunction | “Imbalance between the inertial demands of the trunk and core control and coordination to resist it” | Thighs do not reach parallel (peak of jump) |
| Pause between jumps | ||
| Does not land in same footprint (excessive in-flight motion) | ||
| Technique perfection | Not defined | Technique declines prior to 10 s |
The TJA has not been compared with other clinical jumping assessments, but there may be some advantages of the TJA compared with the DJST, which requires a participant to jump off a 30.48 cm box, land, and immediately perform a maximal vertical jump[95]. Because this screening tool involves the use of markers it has a slightly more involved set up. The TJA is also advantageous over the LESS as the scoring for the LESS is more involved as a result of evaluating 17 landing technique errors (present or not) on “a range of readily observable items of human movement”[73]. The TJA is a 10 s test vs the 1-2 jumps for other tests and may potentially allow measurement of performance endurance, and fatigue[87]. Similar validation with the TJA is required to ensure the validity of the assessment. The TJA, unlike the other two tests, starts and stops from ground level instead of jumping from a box; this better represents techniques encountered in normal jumping activities.
None of these jumping assessments have been investigated as an injury prediction tool. All of these assessments were designed to better understand ACL injury, and it is well known that ACL injury are multifactorial, and the mechanism of non-contact ACL injury is multiplanar[73,95], the inclusion of these clinically jumping assessments as a sole predictor for ACL injury is not recommended. Despite the minimal published literature on the TJA, one recommendation can be offered. For the most consistent results, a single clinician should score the TJA if using this to assess progress with an intervention. Further research on the validity is needed to advocate the further use of the TJA clinically.
CONCLUSION
This editorial focused on clinical movement screening tests as they have gained a lot of popularity in the clinical setting as a tool to predict injury and guide injury prevention programs/training. However, clinicians should be aware that various factors like sex differences, previous injury history, and sport participation can influence the accuracy of these screening tests. The validity of the FMS has been questioned and conflicting findings on injury prediction make recommendations for use difficult at this time. The SEBT/YBT appear to have some potential for injury prediction when assessing anterior reach asymmetry, but the CS is a little less clear as there are varying cut-points being identified for injury risk prediction. Additionally, the validity of the SEBT/YBT has yet to be established. It is of the authors opinion that, while both the SEBT and YBT are reliable tools, the YBT is easier to use from a clinician standpoint. The DJST, while proven to detect normalized knee separation differences following neuromuscular training, has yet to be validated or established as a tool to predict injury risk. The LESS appears to have recent potential as an injury predictor; however, results between the only two studies published conflict on this. Additionally, one study has suggested that the LESS may need to have irrelevant items/errors removed to improve validity. Finally, the TJA appeared to be reliable from early studies; however, a newer study suggests that it may not be very reliable and scoring by a single clinician leads to more consistency. Additionally, this tool has yet to be validated or proven as an injury risk predictor.
Footnotes
Conflict-of-interest statement: Chimera NJ and Warren M have no conflicts of interest related to this publication.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Peer-review started: August 11, 2015
First decision: October 16, 2015
Article in press: January 4, 2016
P- Reviewer: Anand A, Chen C, Finestone AS, Franklyn M, Luo XH S- Editor: Qiu S L- Editor: A E- Editor: Wu HL
References
- 1.Rechel JA, Yard EE, Comstock RD. An epidemiologic comparison of high school sports injuries sustained in practice and competition. J Athl Train. 2008;43:197–204. doi: 10.4085/1062-6050-43.2.197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hootman JM, Dick R, Agel J. Epidemiology of collegiate injuries for 15 sports: summary and recommendations for injury prevention initiatives. J Athl Train. 2007;42:311–319. [PMC free article] [PubMed] [Google Scholar]
- 3.Fuller CW, Ekstrand J, Junge A, Andersen TE, Bahr R, Dvorak J, Hägglund M, McCrory P, Meeuwisse WH. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Br J Sports Med. 2006;40:193–201. doi: 10.1136/bjsm.2005.025270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Dick R, Agel J, Marshall SW. National Collegiate Athletic Association Injury Surveillance System commentaries: introduction and methods. J Athl Train. 2007;42:173–182. [PMC free article] [PubMed] [Google Scholar]
- 5.Cook G, Burton L, Hoogenboom B. Pre-participation screening: the use of fundamental movements as an assessment of function - part 1. N Am J Sports Phys Ther. 2006;1:62–72. [PMC free article] [PubMed] [Google Scholar]
- 6.Cook G, Burton L, Hoogenboom B. Pre-participation screening: the use of fundamental movements as an assessment of function - part 2. N Am J Sports Phys Ther. 2006;1:132–139. [PMC free article] [PubMed] [Google Scholar]
- 7.Smith CA, Chimera NJ, Wright NJ, Warren M. Interrater and intrarater reliability of the functional movement screen. J Strength Cond Res. 2013;27:982–987. doi: 10.1519/JSC.0b013e3182606df2. [DOI] [PubMed] [Google Scholar]
- 8.Fox D, O’Malley E, Blake C. Normative data for the Functional Movement Screen in male Gaelic field sports. Phys Ther Sport. 2014;15:194–199. doi: 10.1016/j.ptsp.2013.11.004. [DOI] [PubMed] [Google Scholar]
- 9.Loudon JK, Parkerson-Mitchell AJ, Hildebrand LD, Teague C. Functional movement screen scores in a group of running athletes. J Strength Cond Res. 2014;28:909–913. doi: 10.1097/JSC.0000000000000233. [DOI] [PubMed] [Google Scholar]
- 10.Schneiders AG, Davidsson A, Hörman E, Sullivan SJ. Functional movement screen normative values in a young, active population. Int J Sports Phys Ther. 2011;6:75–82. [PMC free article] [PubMed] [Google Scholar]
- 11.Teyhen DS, Riebel MA, McArthur DR, Savini M, Jones MJ, Goffar SL, Kiesel KB, Plisky PJ. Normative data and the influence of age and gender on power, balance, flexibility, and functional movement in healthy service members. Mil Med. 2014;179:413–420. doi: 10.7205/MILMED-D-13-00362. [DOI] [PubMed] [Google Scholar]
- 12.Perry FT, Koehle MS. Normative data for the functional movement screen in middle-aged adults. J Strength Cond Res. 2013;27:458–462. doi: 10.1519/JSC.0b013e3182576fa6. [DOI] [PubMed] [Google Scholar]
- 13.Chimera NJ, Smith CA, Warren M. Injury history, sex, and performance on the functional movement screen and Y balance test. J Athl Train. 2015;50:475–485. doi: 10.4085/1062-6050-49.6.02. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kraus K, Schütz E, Taylor WR, Doyscher R. Efficacy of the functional movement screen: a review. J Strength Cond Res. 2014;28:3571–3584. doi: 10.1519/JSC.0000000000000556. [DOI] [PubMed] [Google Scholar]
- 15.Frohm A, Heijne A, Kowalski J, Svensson P, Myklebust G. A nine-test screening battery for athletes: a reliability study. Scand J Med Sci Sports. 2012;22:306–315. doi: 10.1111/j.1600-0838.2010.01267.x. [DOI] [PubMed] [Google Scholar]
- 16.Onate JA, Dewey T, Kollock RO, Thomas KS, Van Lunen BL, DeMaio M, Ringleb SI. Real-time intersession and interrater reliability of the functional movement screen. J Strength Cond Res. 2012;26:408–415. doi: 10.1519/JSC.0b013e318220e6fa. [DOI] [PubMed] [Google Scholar]
- 17.Shultz R, Anderson SC, Matheson GO, Marcello B, Besier T. Test-retest and interrater reliability of the functional movement screen. J Athl Train. 2013;48:331–336. doi: 10.4085/1062-6050-48.2.11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Butler RJ, Plisky PJ, Southers C, Scoma C, Kiesel KB. Biomechanical analysis of the different classifications of the Functional Movement Screen deep squat test. Sports Biomech. 2010;9:270–279. doi: 10.1080/14763141.2010.539623. [DOI] [PubMed] [Google Scholar]
- 19.Hartigan EH, Lawrence M, Bisson BM, Torgerson E, Knight RC. Relationship of the functional movement screen in-line lunge to power, speed, and balance measures. Sports Health. 2014;6:197–202. doi: 10.1177/1941738114522412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kazman JB, Galecki JM, Lisman P, Deuster PA, O’Connor FG. Factor structure of the functional movement screen in marine officer candidates. J Strength Cond Res. 2014;28:672–678. doi: 10.1519/JSC.0b013e3182a6dd83. [DOI] [PubMed] [Google Scholar]
- 21.Li Y, Wang X, Chen X, Dai B. Exploratory factor analysis of the functional movement screen in elite athletes. J Sports Sci. 2015;33:1166–1172. doi: 10.1080/02640414.2014.986505. [DOI] [PubMed] [Google Scholar]
- 22.Kiesel K, Plisky PJ, Voight ML. Can Serious Injury in Professional Football be Predicted by a Preseason Functional Movement Screen. N Am J Sports Phys Ther. 2007;2:147–158. [PMC free article] [PubMed] [Google Scholar]
- 23.Chorba RS, Chorba DJ, Bouillon LE, Overmyer CA, Landis JA. Use of a functional movement screening tool to determine injury risk in female collegiate athletes. N Am J Sports Phys Ther. 2010;5:47–54. [PMC free article] [PubMed] [Google Scholar]
- 24.O’Connor FG, Deuster PA, Davis J, Pappas CG, Knapik JJ. Functional movement screening: predicting injuries in officer candidates. Med Sci Sports Exerc. 2011;43:2224–2230. doi: 10.1249/MSS.0b013e318223522d. [DOI] [PubMed] [Google Scholar]
- 25.Butler RJ, Contreras M, Burton LC, Plisky PJ, Goode A, Kiesel K. Modifiable risk factors predict injuries in firefighters during training academies. Work. 2013;46:11–17. doi: 10.3233/WOR-121545. [DOI] [PubMed] [Google Scholar]
- 26.Warren M, Smith CA, Chimera NJ. Association of the Functional Movement Screen with injuries in division I athletes. J Sport Rehabil. 2015;24:163–170. doi: 10.1123/jsr.2013-0141. [DOI] [PubMed] [Google Scholar]
- 27.Garrison M, Westrick R, Johnson MR, Benenson J. Association between the functional movement screen and injury development in college athletes. Int J Sports Phys Ther. 2015;10:21–28. [PMC free article] [PubMed] [Google Scholar]
- 28.Hotta T, Nishiguchi S, Fukutani N, Tashiro Y, Adachi D, Morino S, Shirooka H, Nozaki Y, Hirata H, Yamaguchi M, et al. Functional Movement Screen for Predicting Running Injuries in 18- to 24-Year-Old Competitive Male Runners. J Strength Cond Res. 2015;29:2808–2815. doi: 10.1519/JSC.0000000000000962. [DOI] [PubMed] [Google Scholar]
- 29.Knapik JJ, Cosio-Lima LM, Reynolds KL, Shumway RS. Efficacy of functional movement screening for predicting injuries in coast guard cadets. J Strength Cond Res. 2015;29:1157–1162. doi: 10.1519/JSC.0000000000000704. [DOI] [PubMed] [Google Scholar]
- 30.McGill S, Frost D, Lam T, Finlay T, Darby K, Cannon J. Can fitness and movement quality prevent back injury in elite task force police officers A 5-year longitudinal study. Ergonomics. 2015;58:1682–1689. doi: 10.1080/00140139.2015.1035760. [DOI] [PubMed] [Google Scholar]
- 31.Beaton DE, Bombardier C, Katz JN, Wright JG. A taxonomy for responsiveness. J Clin Epidemiol. 2001;54:1204–1217. doi: 10.1016/s0895-4356(01)00407-3. [DOI] [PubMed] [Google Scholar]
- 32.Bodden JG, Needham RA, Chockalingam N. The effect of an intervention program on functional movement screen test scores in mixed martial arts athletes. J Strength Cond Res. 2015;29:219–225. doi: 10.1519/JSC.0b013e3182a480bf. [DOI] [PubMed] [Google Scholar]
- 33.Frost DM, Beach TA, Callaghan JP, McGill SM. Using the Functional Movement Screen™ to evaluate the effectiveness of training. J Strength Cond Res. 2012;26:1620–1630. doi: 10.1519/JSC.0b013e318234ec59. [DOI] [PubMed] [Google Scholar]
- 34.Beach TA, Frost DM, McGill SM, Callaghan JP. Physical fitness improvements and occupational low-back loading - an exercise intervention study with firefighters. Ergonomics. 2014;57:744–763. doi: 10.1080/00140139.2014.897374. [DOI] [PubMed] [Google Scholar]
- 35.Kiesel K, Plisky P, Butler R. Functional movement test scores improve following a standardized off-season intervention program in professional football players. Scand J Med Sci Sports. 2011;21:287–292. doi: 10.1111/j.1600-0838.2009.01038.x. [DOI] [PubMed] [Google Scholar]
- 36.Kiesel KB, Butler RJ, Plisky PJ. Prediction of injury by limited and asymmetrical fundamental movement patterns in american football players. J Sport Rehabil. 2014;23:88–94. doi: 10.1123/jsr.2012-0130. [DOI] [PubMed] [Google Scholar]
- 37.Kodesh E, Shargal E, Kislev-Cohen R, Funk S, Dorfman L, Samuelly G, Hoffman JR, Sharvit N. Examination of the Effectiveness of Predictors for Musculoskeletal Injuries in Female Soldiers. J Sports Sci Med. 2015;14:515–521. [PMC free article] [PubMed] [Google Scholar]
- 38.Kinzey SJ, Armstrong CW. The reliability of the star-excursion test in assessing dynamic balance. J Orthop Sports Phys Ther. 1998;27:356–360. doi: 10.2519/jospt.1998.27.5.356. [DOI] [PubMed] [Google Scholar]
- 39.Hertel J, Braham RA, Hale SA, Olmsted-Kramer LC. Simplifying the star excursion balance test: analyses of subjects with and without chronic ankle instability. J Orthop Sports Phys Ther. 2006;36:131–137. doi: 10.2519/jospt.2006.36.3.131. [DOI] [PubMed] [Google Scholar]
- 40.Hertel J. Sensorimotor deficits with ankle sprains and chronic ankle instability. Clin Sports Med. 2008;27:353–370, vii. doi: 10.1016/j.csm.2008.03.006. [DOI] [PubMed] [Google Scholar]
- 41.Plisky PJ, Gorman PP, Butler RJ, Kiesel KB, Underwood FB, Elkins B. The reliability of an instrumented device for measuring components of the star excursion balance test. N Am J Sports Phys Ther. 2009;4:92–99. [PMC free article] [PubMed] [Google Scholar]
- 42.Gribble PA, Hertel J. Considerations for Normalizing Measures of the Star Excursion Balance Test. Meas Phys Educ Exerc Sci. 2003;7:89–100. [Google Scholar]
- 43.Plisky PJ, Rauh MJ, Kaminski TW, Underwood FB. Star Excursion Balance Test as a predictor of lower extremity injury in high school basketball players. J Orthop Sports Phys Ther. 2006;36:911–919. doi: 10.2519/jospt.2006.2244. [DOI] [PubMed] [Google Scholar]
- 44.Gribble PA, Kelly SE, Refshauge KM, Hiller CE. Interrater reliability of the star excursion balance test. J Athl Train. 2013;48:621–626. doi: 10.4085/1062-6050-48.3.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Munro AG, Herrington LC. Between-session reliability of the star excursion balance test. Phys Ther Sport. 2010;11:128–132. doi: 10.1016/j.ptsp.2010.07.002. [DOI] [PubMed] [Google Scholar]
- 46.Coughlan GF, Fullam K, Delahunt E, Gissane C, Caulfield BM. A comparison between performance on selected directions of the star excursion balance test and the Y balance test. J Athl Train. 2012;47:366–371. doi: 10.4085/1062-6050-47.4.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Fullam K, Caulfield B, Coughlan GF, Delahunt E. Kinematic analysis of selected reach directions of the Star Excursion Balance Test compared with the Y-Balance Test. J Sport Rehabil. 2014;23:27–35. doi: 10.1123/jsr.2012-0114. [DOI] [PubMed] [Google Scholar]
- 48.Gribble PA, Robinson RH, Hertel J, Denegar CR. The effects of gender and fatigue on dynamic postural control. J Sport Rehabil. 2009;18:240–257. doi: 10.1123/jsr.18.2.240. [DOI] [PubMed] [Google Scholar]
- 49.Bouillon LE, Baker JL. Dynamic Balance Differences as Measured by the Star Excursion Balance Test Between Adult-aged and Middle-aged Women. Sports Health. 2011;3:466–469. doi: 10.1177/1941738111414127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Butler RJ, Queen RM, Beckman B, Kiesel KB, Plisky PJ. Comparison of dynamic balance in adolescent male soccer players from rwanda and the United States. Int J Sports Phys Ther. 2013;8:749–755. [PMC free article] [PubMed] [Google Scholar]
- 51.Bressel E, Yonker JC, Kras J, Heath EM. Comparison of static and dynamic balance in female collegiate soccer, basketball, and gymnastics athletes. J Athl Train. 2007;42:42–46. [PMC free article] [PubMed] [Google Scholar]
- 52.Butler RJ, Southers C, Gorman PP, Kiesel KB, Plisky PJ. Differences in soccer players’ dynamic balance across levels of competition. J Athl Train. 2012;47:616–620. doi: 10.4085/1062-6050-47.5.14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Lehr ME, Plisky PJ, Butler RJ, Fink ML, Kiesel KB, Underwood FB. Field-expedient screening and injury risk algorithm categories as predictors of noncontact lower extremity injury. Scand J Med Sci Sports. 2013;23:e225–e232. doi: 10.1111/sms.12062. [DOI] [PubMed] [Google Scholar]
- 54.Butler RJ, Lehr ME, Fink ML, Kiesel KB, Plisky PJ. Dynamic balance performance and noncontact lower extremity injury in college football players: an initial study. Sports Health. 2013;5:417–422. doi: 10.1177/1941738113498703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Smith CA, Chimera NJ, Warren M. Association of y balance test reach asymmetry and injury in division I athletes. Med Sci Sports Exerc. 2015;47:136–141. doi: 10.1249/MSS.0000000000000380. [DOI] [PubMed] [Google Scholar]
- 56.Olivier B, Stewart AV, Olorunju SA, McKinon W. Static and dynamic balance ability, lumbo-pelvic movement control and injury incidence in cricket pace bowlers. J Sci Med Sport. 2015;18:19–25. doi: 10.1016/j.jsams.2013.10.245. [DOI] [PubMed] [Google Scholar]
- 57.Basnett CR, Hanish MJ, Wheeler TJ, Miriovsky DJ, Danielson EL, Barr JB, Grindstaff TL. Ankle dorsiflexion range of motion influences dynamic balance in individuals with chronic ankle instability. Int J Sports Phys Ther. 2013;8:121–128. [PMC free article] [PubMed] [Google Scholar]
- 58.Hoch MC, Staton GS, McKeon PO. Dorsiflexion range of motion significantly influences dynamic balance. J Sci Med Sport. 2011;14:90–92. doi: 10.1016/j.jsams.2010.08.001. [DOI] [PubMed] [Google Scholar]
- 59.Imai A, Kaneoka K, Okubo Y, Shiraki H. Comparison of the immediate effect of different types of trunk exercise on the star excursion balance test in male adolescent soccer players. Int J Sports Phys Ther. 2014;9:428–435. [PMC free article] [PubMed] [Google Scholar]
- 60.Imai A, Kaneoka K, Okubo Y, Shiraki H. Effects of two types of trunk exercises on balance and athletic performance in youth soccer players. Int J Sports Phys Ther. 2014;9:47–57. [PMC free article] [PubMed] [Google Scholar]
- 61.Filipa A, Byrnes R, Paterno MV, Myer GD, Hewett TE. Neuromuscular training improves performance on the star excursion balance test in young female athletes. J Orthop Sports Phys Ther. 2010;40:551–558. doi: 10.2519/jospt.2010.3325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Garrison JC, Bothwell J, Cohen K, Conway J. Effects of hip strengthening on early outcomes following anterior cruciate ligament reconstruction. Int J Sports Phys Ther. 2014;9:157–167. [PMC free article] [PubMed] [Google Scholar]
- 63.Ambegaonkar JP, Mettinger LM, Caswell SV, Burtt A, Cortes N. Relationships between core endurance, hip strength, and balance in collegiate female athletes. Int J Sports Phys Ther. 2014;9:604–616. [PMC free article] [PubMed] [Google Scholar]
- 64.Noyes FR, Barber-Westin SD, Fleckenstein C, Walsh C, West J. The drop-jump screening test: difference in lower limb control by gender and effect of neuromuscular training in female athletes. Am J Sports Med. 2005;33:197–207. doi: 10.1177/0363546504266484. [DOI] [PubMed] [Google Scholar]
- 65.Hewett TE, Stroupe AL, Nance TA, Noyes FR. Plyometric training in female athletes. Decreased impact forces and increased hamstring torques. Am J Sports Med. 1996;24:765–773. doi: 10.1177/036354659602400611. [DOI] [PubMed] [Google Scholar]
- 66.Barber-Westin SD, Noyes FR, Galloway M. Jump-land characteristics and muscle strength development in young athletes: a gender comparison of 1140 athletes 9 to 17 years of age. Am J Sports Med. 2006;34:375–384. doi: 10.1177/0363546505281242. [DOI] [PubMed] [Google Scholar]
- 67.Ugalde V, Brockman C, Bailowitz Z, Pollard CD. Single leg squat test and its relationship to dynamic knee valgus and injury risk screening. PM R. 2015;7:229–235; quiz 235. doi: 10.1016/j.pmrj.2014.08.361. [DOI] [PubMed] [Google Scholar]
- 68.Hewett T, Snyder-Mackler L, Spindler KP. The drop-jump screening test: difference in lower limb control by gender and effect of neuromuscular training in female athletes. Am J Sports Med. 2007;35:145; author reply 146–147. doi: 10.1177/0363546506296609. [DOI] [PubMed] [Google Scholar]
- 69.Noyes FR, Barber-Westin SD, Smith ST, Campbell T. A training program to improve neuromuscular indices in female high school volleyball players. J Strength Cond Res. 2011;25:2151–2160. doi: 10.1519/JSC.0b013e3181f906ef. [DOI] [PubMed] [Google Scholar]
- 70.Noyes FR, Barber-Westin SD, Smith ST, Campbell T, Garrison TT. A training program to improve neuromuscular and performance indices in female high school basketball players. J Strength Cond Res. 2012;26:709–719. doi: 10.1519/JSC.0b013e318228194c. [DOI] [PubMed] [Google Scholar]
- 71.Noyes FR, Barber-Westin SD, Tutalo Smith ST, Campbell T. A training program to improve neuromuscular and performance indices in female high school soccer players. J Strength Cond Res. 2013;27:340–351. doi: 10.1519/JSC.0b013e31825423d9. [DOI] [PubMed] [Google Scholar]
- 72.Barber-Westin SD, Smith ST, Campbell T, Noyes FR. The drop-jump video screening test: retention of improvement in neuromuscular control in female volleyball players. J Strength Cond Res. 2010;24:3055–3062. doi: 10.1519/JSC.0b013e3181d83516. [DOI] [PubMed] [Google Scholar]
- 73.Padua DA, Marshall SW, Boling MC, Thigpen CA, Garrett WE, Beutler AI. The Landing Error Scoring System (LESS) Is a valid and reliable clinical assessment tool of jump-landing biomechanics: The JUMP-ACL study. Am J Sports Med. 2009;37:1996–2002. doi: 10.1177/0363546509343200. [DOI] [PubMed] [Google Scholar]
- 74.Padua DA, Boling MC, Distefano LJ, Onate JA, Beutler AI, Marshall SW. Reliability of the landing error scoring system-real time, a clinical assessment tool of jump-landing biomechanics. J Sport Rehabil. 2011;20:145–156. doi: 10.1123/jsr.20.2.145. [DOI] [PubMed] [Google Scholar]
- 75.Cortes N, Onate J. Clinical Assessment of Drop-Jump Landing for Determination of Risk for Knee Injury. Int J Athl Ther Amp Train. 2013;18:10–13. [Google Scholar]
- 76.Onate J, Cortes N, Welch C, Van Lunen BL. Expert versus novice interrater reliability and criterion validity of the landing error scoring system. J Sport Rehabil. 2010;19:41–56. doi: 10.1123/jsr.19.1.41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Lam KC, Valovich McLeod TC. The impact of sex and knee injury history on jump-landing patterns in collegiate athletes: a clinical evaluation. Clin J Sport Med. 2014;24:373–379. doi: 10.1097/JSM.0000000000000053. [DOI] [PubMed] [Google Scholar]
- 78.Beutler A, de la Motte S, Marshall S, Padua D, Boden B. Muscle strength and qualitative jump-landing differences in male and female military cadets: the jump-acl study. J Sports Sci Med. 2009;8:663–671. [PMC free article] [PubMed] [Google Scholar]
- 79.Gokeler A, Eppinga P, Dijkstra PU, Welling W, Padua DA, Otten E, Benjaminse A. Effect of fatigue on landing performance assessed with the landing error scoring system (less) in patients after ACL reconstruction. A pilot study. Int J Sports Phys Ther. 2014;9:302–311. [PMC free article] [PubMed] [Google Scholar]
- 80.Kuenze CM, Foot N, Saliba SA, Hart JM. Drop-Landing Performance and Knee-Extension Strength After Anterior Cruciate Ligament Reconstruction. J Athl Train. 2015;50:596–602. doi: 10.4085/1062-6050-50.2.11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Bell DR, Smith MD, Pennuto AP, Stiffler MR, Olson ME. Jump-landing mechanics after anterior cruciate ligament reconstruction: a landing error scoring system study. J Athl Train. 2014;49:435–441. doi: 10.4085/1062-6050-49.3.21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Owens BD, Cameron KL, Duffey ML, Vargas D, Duffey MJ, Mountcastle SB, Padua D, Nelson BJ. Military movement training program improves jump-landing mechanics associated with anterior cruciate ligament injury risk. J Surg Orthop Adv. 2013;22:66–70. doi: 10.3113/jsoa.2013.0066. [DOI] [PubMed] [Google Scholar]
- 83.Distefano LJ, Distefano MJ, Frank BS, Clark MA, Padua DA. Comparison of integrated and isolated training on performance measures and neuromuscular control. J Strength Cond Res. 2013;27:1083–1090. doi: 10.1519/JSC.0b013e318280d40b. [DOI] [PubMed] [Google Scholar]
- 84.Padua DA, DiStefano LJ, Marshall SW, Beutler AI, de la Motte SJ, DiStefano MJ. Retention of movement pattern changes after a lower extremity injury prevention program is affected by program duration. Am J Sports Med. 2012;40:300–306. doi: 10.1177/0363546511425474. [DOI] [PubMed] [Google Scholar]
- 85.Padua DA, DiStefano LJ, Beutler AI, de la Motte SJ, DiStefano MJ, Marshall SW. The Landing Error Scoring System as a Screening Tool for an Anterior Cruciate Ligament Injury-Prevention Program in Elite-Youth Soccer Athletes. J Athl Train. 2015;50:589–595. doi: 10.4085/1062-6050-50.1.10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Smith HC, Johnson RJ, Shultz SJ, Tourville T, Holterman LA, Slauterbeck J, Vacek PM, Beynnon BD. A prospective evaluation of the Landing Error Scoring System (LESS) as a screening tool for anterior cruciate ligament injury risk. Am J Sports Med. 2012;40:521–526. doi: 10.1177/0363546511429776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Myer GD, Ford KR, Hewett TE. Tuck Jump Assessment for Reducing Anterior Cruciate Ligament Injury Risk. Athl Ther Today. 2008;13:39–44. doi: 10.1123/att.13.5.39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Myer GD, Brent JL, Ford KR, Hewett TE. Real-time assessment and neuromuscular training feedback techniques to prevent ACL injury in female athletes. Strength Cond J. 2011;33:21–35. doi: 10.1519/SSC.0b013e318213afa8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Myer GD, Paterno MV, Ford KR, Quatman CE, Hewett TE. Rehabilitation after anterior cruciate ligament reconstruction: criteria-based progression through the return-to-sport phase. J Orthop Sports Phys Ther. 2006;36:385–402. doi: 10.2519/jospt.2006.2222. [DOI] [PubMed] [Google Scholar]
- 90.Herrington L, Myer GD, Munro A. Intra and inter-tester reliability of the tuck jump assessment. Phys Ther Sport. 2013;14:152–155. doi: 10.1016/j.ptsp.2012.05.005. [DOI] [PubMed] [Google Scholar]
- 91.Dudley LA, Smith CA, Olson BK, Chimera NJ, Schmitz B, Warren M. Dudley LA, Smith CA, Olson BK, Chimera NJ, Schmitz B, Warren M. Interrater and intrarater reliability of the Tuck Jump Assessment by health professionals of varied educational backgrounds. J Sports Med. 2013;2013:1–5. doi: 10.1155/2013/483503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Hewett TE, Myer GD, Ford KR, Heidt RS, Colosimo AJ, McLean SG, van den Bogert AJ, Paterno MV, Succop P. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005;33:492–501. doi: 10.1177/0363546504269591. [DOI] [PubMed] [Google Scholar]
- 93.Paterno MV, Ford KR, Myer GD, Heyl R, Hewett TE. Limb asymmetries in landing and jumping 2 years following anterior cruciate ligament reconstruction. Clin J Sport Med. 2007;17:258–262. doi: 10.1097/JSM.0b013e31804c77ea. [DOI] [PubMed] [Google Scholar]
- 94.Boden BP, Sheehan FT, Torg JS, Hewett TE. Noncontact anterior cruciate ligament injuries: mechanisms and risk factors. J Am Acad Orthop Surg. 2010;18:520–527. doi: 10.5435/00124635-201009000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Noyes FR, Barber SD, Mangine RE. Abnormal lower limb symmetry determined by function hop tests after anterior cruciate ligament rupture. Am J Sports Med. 1991;19:513–518. doi: 10.1177/036354659101900518. [DOI] [PubMed] [Google Scholar]