

Abstract
Femoral pseudoaneurysm is a common complication of repeated femoral puncture during cardiac catheterisation. We describe here the development of femoral pseudoaneurysms in a patient with Takayasu's arteritis, which healed in response to conservative treatment, and review the literature on the prevention and treatment of femoral pseudoaneurysm.
Introduction
Pseudoaneurysms can arise either spontaneously or iatrogenically. In both cases they are a major cause for concern as they can rupture, bleed or cause sudden death.1 A pseudoaneurysm is a pulsating encapsulated haematoma in communication with a ruptured vessel.1 We describe here the development of femoral pseudoaneurysms in a patient with Takayasu's arteritis, and review the literature.
Case report
A 49-year-old woman presented with no pulse in both arms and her blood pressure could not be recorded in either arm. She had systemic hypertension and because she had difficulty in holding a spoon or eating with her right hand, balloon angioplasty of her right subclavian artery was performed (see online supplementary figures S1–S3) and she concomitantly received high-dose steroids. She complained of recurrent pain in the arm and it was assumed that she had restenosis of the right subclavian artery; an angiogram was scheduled. Her baseline haemoglobin was 10.9 g/dL. She underwent a right femoral puncture and was catheterised with a 6 F JR 3.5 diagnostic catheter. This was the third procedure that used a right femoral arterial puncture in the same leg. The angiogram showed that her right subclavian artery had developed tubular 90% concentric restenosis. The ostial-proximal vertebral artery had an eccentric 90% disease with flow reversal into the right subclavian artery (see online supplementary videos).
After the procedure, a small haematoma was noted in the right groin, which resolved on compression. However, after 3 h she complained of pain in the right groin. At this time her heart rate was 100/min and her systolic blood pressure 80 mm Hg. On inspection, a huge haematoma with discolouration of the skin was found. She was given just over 1 L (2 pints) of normal saline and her haemoglobin had decreased to 9.3 g/dL. After another hour, the patient stabilised and her echocardiogram showed no pericardial effusion.
Two days later while walking about, she suddenly had recurrent right groin pain. At this time her systolic blood pressure was 90 mm Hg, and her heart rate was 120/min. Her haemoglobin was 8.7 g/dL and she was given volume replacement with normal saline and one pint of packed red blood cells. By evening the haemoglobin level had fallen further to 6.8 g/dL. Emergency Doppler imaging of the right femoral artery showed a femoral pseudoaneurysm with an overlying haematoma (see figure 1). A surgical opinion was obtained and conservative management was advised. A compression bandage was applied and she was given 2 pints of packed red blood cells and 3 units of fresh frozen plasma. All antiplatelet drugs were stopped. A CT scan with contrast was done the next day (figures 2–4). Figure 4 shows both thighs, with the right thigh greatly enlarged owing to the presence of a large haematoma.
Figure 1.
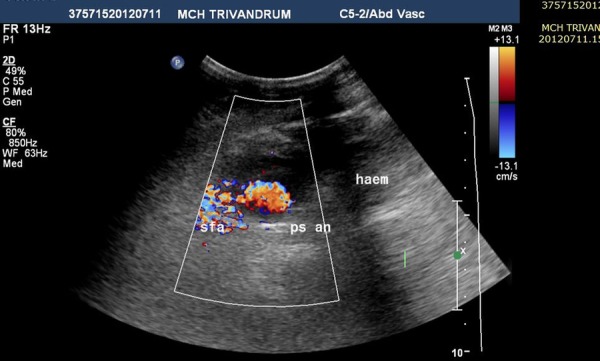
Doppler ultrasound image showing colour flow in the pseudoaneurysm and the femoral artery and the haematoma. haem, haematoma; psan, pseudoaneurysm, sfa, superficial femoral artery.
Figure 2.
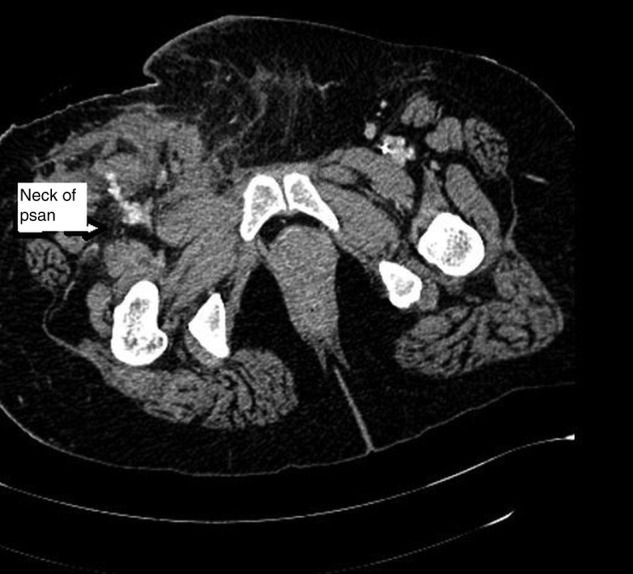
CT scan showing contrast in the neck of the pseudoaneurysm (psan).
Figure 3.
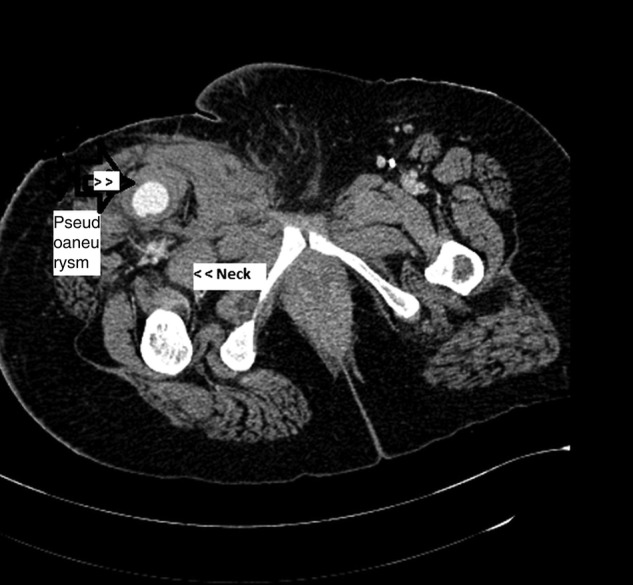
Contrast in the pseudoaneurysm and the femoral artery and the large haematoma. Neck of the pseudoaneurysm is labelled.
Figure 4.

CT scan of both thighs showing a large right thigh haematoma.
Thrombin injection was considered after digital subtraction angiography (DSA) 2 days later. DSA showed that the pseudoaneurysm had resolved. The patient wore a compression elastocrepe bandage for 17 days after the puncture. A follow-up Doppler ultrasound scan showed a hypoechoic heterogeneous haematoma measuring 9.4 cm×5.3 cm with multiple septations and thick walls. No evidence of colour flow was seen and there was no communication with the superficial femoral artery. This was consistent with a thrombosed pseudoaneurysm. The hard haematoma was seen to resolve gradually during follow-up visits.
Causes of pseudoaneurysms
Pseudoaneurysms can occur after cardiac catheterisation,1 usually when the femoral arterial puncture is too low. Puncture of the profunda femoris artery causes a pseudoaneurysm because the vessel is not supported by the femoral head or bone. When the operator looks for the femoral neck and then punctures the artery, the incidence of femoral pseudoaneurysm is less. Looking for the neck of the femur and puncturing by the Seldinger technique is an accepted method of preventing pseudoaneurysm.
The femoral artery should be compressed after removal of the femoral arterial sheath. Numerous devices for femoral closure are available, but manual compression is still the ‘gold standard’. The correct method for compression is as follows: compress the artery until no pulses are felt for 4 min, then release the pressure for 1 min so that the distal pulses are felt. This cycle should be repeated until all bleeding stops. After this, a further compression of 5 min is thought to suppress the formation of pseudoaneurysms.
If the cut made on the anterior wall of the artery is too large or if dilatation of the access track is carried out with an artery forceps, a pseudoaneurysm may develop. This procedure should be used sparingly and the limb should be immobilised. The incidence of pseudoaneurysms after catheterisation ranges from 0.5% to 14%.1
A common cause of pseudoaneurysm is trauma to the aorta, at the junction of the fixed aorta and the descending thoracic aorta—the aortic isthmus. Sheering and bending stress may injure this section of the aorta. Either blunt or penetrating trauma may cause pseudoaneurysms. Pseudoaneurysms may occur secondary to invasion of a blood vessel by a tumour —for example, a malignant lymphoma or even an osteochondroma or a neurofibroma.
Pseudoaneurysms can also occur after aortic surgery, after myocardial infarction and septic emboli owing to Salmonella infection.1 Vasculitis and Behçet's disease may present as a pseudoaneurysm. Pseudoaneurysms may also occur after liver transplantation, heart transplantation and other biopsy diagnostic procedures.2 Dilatation and curettage of the uterus and caesarean section are a further cause of pseudoaneurysms.
Patients with Takayasu’s arteritis have localised arterial segments of severe stenosis that are often dilated by cardiologists, increasing the likelihood of developing pseudoaneurysms (figures 1–3).
Suspecting a pseudoaneurysm after catheterisation
Always inspect the site. If any swelling is felt over the femoral region, auscultate the vessel. If a bruit is heard, send the patient for further evaluation. Further, if a fall in haemoglobin level occurs after a simple catheterisation look for a pseudoaneurysm. Swelling at the site of sheath removal in a site with repeated punctures on the same side of the artery (either all right or all left femoral artery) should lead to suspicion of a pseudoaneurysm, and early tests should be done. Thinner people or a low punctures should also make one suspect that there might be a pseudoaneurysm.
Detection of a pseudoaneurysm
Inspect the groin site for three main signs.3 The first sign is an expanding pulsatile mass; assess the pulse width between the fingers carefully and monitor for increasing size. The other two signs are the presence of a bruit over the femoral artery and tenderness over the catheterisation site. If two of these three signs are present, then either an arteriovenous fistula or a pseudoaneurysm should be suspected.3 Pseudoaneurysms of <2 cm that are not enlarging can often be managed conservatively.3
Screening for a pseudoaneurysm
Colour Doppler ultrasound scanning is a simple bedside test (figure 1). Occasionally, in obese patients, it may be difficult to locate the neck of the pseudoaneurysm with this method. Locating the neck of the pseudoaneurysm is important, however, for therapeutic reasons. Compression with ultrasonic guidance has been found to be useful in small pseudoaneurysms. Various authors have claimed that necks of <10 mm and with a blood flow velocity of <100 cm/s can be ultrasonically compressed. If the pseudoaneurysm is large then blood transfusion must be given and the patient should then be sent for a CT scan (figures 2–4). CT or MRI can indicate the position of the pseudoaneurysm well.
Treatment of a pseudoaneurysm
The first step towards managing a femoral pseudoaneurysm is ultrasound-guided compression.4 Since 1991 ultrasound-guided compression repair (UGCR) has become the initial mode of treatment of pseudoaneurysms. With this treatment compression of the neck of the aneurysm should result in thrombosis of the blood within the sac while ultrasound monitors the flow through the vessel and the sac. Reported compression times have varied from 10 min to 300 min.4 In our experience, even for small femoral pseudoaneurysms, multiple episodes of compression over a few days or weeks may be required.
Failure of UGCR may result in the need for embolisation of the neck of the aneurysm, which is achieved by filling the aneurysm with thrombin or multiple small coils.4 This procedure has been used since 1996. However, thrombin injection may cause anaphylactic shock, pruritus or intra-arterial thrombosis. Rarely, injection of prions may cause chronic degenerative brain disease as the thrombin is from bovine sources.5 Recently, autologous thrombin has been tried in some centres.4 Dr Labropoulos describes the technique as follows: a small 21 or 22 gauge spinal needle is attached to a small syringe containing thrombin at 1000 U/mL. A spinal tap needle, etched near the tip to make it more echogenic, is generally used (Echotip, Cook, Bloomington, Indiana, USA). The skin is cleaned near the ultrasound tip, and the needle placed in the pseudoaneurysm by direct vision. The colour flow is turned off until the tip is seen clearly. The colour flow is turned on again and thrombin is slowly injected. The thrombus can be seen filling the cavity and once the entire cavity is filled the colour flow usually stops. A volume of thrombin solution of <5 mL is usually sufficient. Some authors have used the contralateral femoral artery to inject the thrombin by another catheter. This technique requires fluoroscopy and is more invasive.
Both UGCR and thrombin injection are painful procedures.6 Before thrombin injections are started, contraindications to thrombin injection should be excluded.7
If the sac has tissue vibration around the neck of the pseudoaneurysm this implies an underlying high-velocity flow. This is suggestive of an arteriovenous fistula and is a contraindication for thrombin injection. The presence of pulsatile flow in the femoral vein and low-resistance flow in the artery are warning signs that there may be an arteriovenous fistula. Hanson et al7 have listed the precautions to be taken before injecting thrombin. These include ensuring that the pseudoaneurysm is not multilobed and excluding the presence of local infection or an arteriovenous fistula. Identify the neck of the aneurysm by the area of maximum ‘to and fro’ waveform. This reduces the risk of embolism if thrombin is injected into the neck of the aneurysm. The presence of diastolic forward flow indicates the presence of an arteriovenous fistula. If multiple lobes are present, the lobe closest to the neck should be injected first. Complete thrombosis should be confirmed by colour Doppler ultrasound imaging. The native artery and vein should be examined and the ankle pulses should be felt. Lenartova and Tak8 have described the use of collagen injection into the pseudoaneurysm. Purified bovine collagen in the form of a biodegradable paste has been used. It is believed that once the collagen comes in contact with the blood it initiates platelet aggregation and release of clotting factors. Bovine collagen is preferred to bovine thrombin because, being a paste, it does not embolise into the parent vessel, and it also allows faster mobilisation.
For all patients with a pseudoaneurysm, the blood pressure should be controlled and anticoagulants stopped. If the patient does not improve, a covered stent may be an option.
Surgical closure of the femoral pseudoaneurysm is considered the ‘gold standard’ for treatment of pseudoaneurysms.5 A simple suture of the defect after evacuation of the haematoma may be enough or a surgical repair with a patch can be made.9 The indications for surgical repair of the pseudoaneurysm have been described by Webber et al.10 They also describe the ‘to and fro sign’ of a pseudoaneurysm. If blood flows in and out of a sac it is a pseudoaneurysm, but if there is no flow it is a haematoma. The surgical indications for intervention include infection of the pseudoaneurysm, rapid expansion, failure of other treatments, skin necrosis, compressive syndromes like neuropathy, claudication or critical limb ischaemia.10
Conclusions
In conclusion, we recommend that patients with arterial wall disease, such as Takayasu's arteritis, are better studied initially by CT angiography and not by direct angiography as this avoids punctures in an already diseased vessel. Direct puncture should be considered only for cardiac interventions; non-invasive tests are preferred for diagnosis of coronary artery disease.11
Acknowledgments
We acknowledge the help of Dr Deepak Paul in processing the figures.
Footnotes
Contributors: All authors helped take care of the patient and the patient work up. PNG wrote the manuscript. ASB, GGS, SP, PS, PV and BU helped retrieve the USS abdomen and CT scan pictures. Authors UM and JR agreed to operate on the patient but this was not required. Author UKK supplied the pictures and did the CT scan. SGN supplied the videos and additional figures.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; internally peer reviewed.
References
- 1.Sueyoshi E, Sakamoto I, Nakashima K, et al. Visceral and peripheral arterial pseudoaneurysms. AJR 2005;185:741–9. [DOI] [PubMed] [Google Scholar]
- 2.Saad NEA, Saad WEA, Davies MG, et al. Psuedoaneurysms and the role of minimally invasive techniques in their management. Radiographics 2005;25:S173–89. [DOI] [PubMed] [Google Scholar]
- 3. Complications of Cardiac Catheterization. Cornell Cardiology Curriculum 2003–2004. pgs 11–12. (Available online)
- 4.Labropoulos N. Techniques and Contraindications for Thrombin Injection of the Groin and Other Periphral Pseudoaneurysms. http://www.veithsymposium.com/index.php.
- 5.Tisi PV, Callam MJ. Surgery versus non-surgical treatment for femoral pseudoaneurysms. Cochrane Database Syst Rev 2006;(1):CD004981. [DOI] [PubMed] [Google Scholar]
- 6.Paulson EK, Nelson RC, Mayes CE, et al. Sonographically guided thrombin injection of iatrogenic femoral pseudoaneurysms: further experience of a single institution. AJR 2001;177:309–6. [DOI] [PubMed] [Google Scholar]
- 7.Hanson JM, Atri M, Power N. Ultrasound-guided thrombin injection of iatrogenic groin pseudoaneurysm: Doppler features and technical tips. Br J Radiol 2008;81:154–63. [DOI] [PubMed] [Google Scholar]
- 8.Lenartova M, Tak T. Iatrogenic pseudoaneurysm of femoral artery case report and literature review. Clin Med Res 2003;1:243–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Demirbas O, Batyraliev T, Eksi Z, et al. Femoral pseudoaneurysm due to diagnostic or interventional angiographic procedures. Angiology 2005;56:553–6. [DOI] [PubMed] [Google Scholar]
- 10.Webber GW, Jang J, Gustavson S, et al. Contemporary management of post catheterization pseudoaneurysms. Circulation 2007;115:2666–74. [DOI] [PubMed] [Google Scholar]
- 11.Joseph S, Madalam KR, Rajanikanth V, et al. Percutaneous transluminal angiography of the subclavian artery in non-specific aortoarteris. Results and long term followup. JVIR 1994;5:573–80. [DOI] [PubMed] [Google Scholar]