

Abstract
Background:
Smoking is a major public health problem, especially in Iraq. There is very little information had been documented regarding smoking risk factors and quit intention among Iraqi smokers.
Objectives:
The main objectives of this study are to determine smokers' knowledge and perception about smoking health risks; and to determine smoking behavior and quitting intentions among Iraqi smokers; as well as to predict the factors that may associate with quit intentions.
Methods:
A cross-sectional study was conducted at the outpatient clinic in Tikrit Teaching Hospital, Tikrit City, Iraq. Adult smokers who are smoking cigarette everyday and able to communicate with the researcher were invited to participate in the study. A self-administered questionnaire was used to collect data from 386 participants.
Results:
This study showed that smokers had low awareness about some risk effects of smoking such as lung cancer in nonsmokers (30.1%), impotence in male smokers (52.6%), premature ageing (64%), and stroke (66.3%). In addition, the high score of knowledge and perception was significantly associated with quitting intention.
Conclusion:
Smokers' knowledge and perception regarding smoking health effects were low, especially in terms of secondhand smokers. Many efforts needed from health policy-makers and health care professionals to disseminate information about the risks of smoking and health benefits of give up smoking.
KEY WORDS: Health risks, knowledge, perception, smoking, quit intentions
Smoking cigarettes is a major public health problem around the world, especially in developing countries.[1] Despite the prevalence of smoking has decreased in many countries, through increasing the awareness of its risks and through tobacco control policies, smoking is still spreading widely.[1] There are 1.3 billion smokers around the world. Furthermore, 5 million people die worldwide from smoking each year. Smoking still continues to rise, especially in the low and middle-income countries as well as the high-income countries.[2] The prevalence of smoking among the young people in some Arab countries are 7% in Oman, 18% in Kuwait, 23% in Iraq, 25% in Saudi Arabia and Jordan, 31% in Syrian Arab Republic, 43% in Yemen, and 53% in Lebanon.[3] Tobacco use in the Middle East is reported to be the highest rate of smoking internationally with smoking rates from 40% to 60% for cigarettes and reaching rates of 77% for men and 35% in women, in some Arab countries.[4] Health knowledge about the risk effects of smoking is a very important factor to motivate smokers to quit smoking. Although increasing the awareness of smoking risks are not always sufficient to reduce the smoking on their own. While increasing the health knowledge is strongly associated with a reduction in smoking and increases the cessation behavior and long-term abstinence from smoking.[5,6,7,8] Quitting smoking at any age leading to immediate health benefits, including reduced risks of stroke, cardiovascular disease, and smoking-related cancers.[9,10,11]
In Jordon, a survey was carried out to explore the quitting intention among Jordanian adults which reported that the quitting intention was high with the majority of smokers who have had previous quitting attempts. More than one-third of the smokers had intentions to quit in the next month. Interest in quitting was significantly associated with the heaviness of smoking, exposure to the antismoking message, medical education, previous quit attempts, and smoker's mental health.[12] Another study was conducted among patients with coronary heart disease, to determine the reasons that discourage the quitting of smoking and resources of advice about quitting. This study reported that only 29.7% of the patients quit smoking after disease occurrence, while 60.7% continued smoking and 9.6% relapsed. Doctors' advice was a reason associated with quit smoking.[13] In Iraq, around 44% of mortality in the country occurs as a result of noncommunicable diseases. The most chronic diseases that cause mortality in Iraq include heart disease, stroke, cancer, respiratory diseases, and diabetes.[14] Regarding the risk factors of chronic diseases, a survey in 2006 reported that 41.4% of the adult population (aged 25–65 years) suffered from high blood pressure, 10.8% had hyperglycemia, and 37.7% had high lipid profiles. Furthermore, around 66% of the adult population was overweight and 33% were obese while the consumption of fruits and vegetables was very low (90.5%) as well as the low level of physical activity (56.7%). However, the prevalence of smoking represents 21.9% of the adult population.[15] Moreover, the Global Youth Tobacco Survey in 2008 showed that 7.4% of the school students of both genders aged 13–15 years in Baghdad had smoked cigarettes (males 7.4%, females 6.8%).[16] Consequently, very little is known about the awareness of smoking risk effects and quitting intentions among smokers in Iraq. The main objectives of this study are to determine smokers' knowledge and perception of smoking health effects; and to determine smoking behavior and quitting intentions among Iraqi smokers; as well as to predict the factors that may associate with quitting intentions.
Methods
Study design and setting
This study was conducted between November 2013 and May 2014 in the Tikrit Province, Iraq. A cross-sectional survey was conducted at the outpatient clinic of Tikrit Teaching Hospital. Tikrit Teaching Hospital is the main General Hospital in the City, where a substantially large population is attending.
Study population
All adult cigarette smokers (18 years and above) of both genders who attend the outpatient clinic as a patient or attendant was eligible to participate in this study. Adult smokers who reported smoking cigarette everyday and agree to participate were eligible for this study. However, those who declined to participate in the study, have cognitive impairment and/or could not complete the interview were excluded.
Sampling technique and sample size
A convenience sampling method was used to recruit the participants from different age groups. The sample size was calculated according to Raosoft sample size calculator with 95% of confidence level and 5% margin of error; with 377 respondents. The sample size does not change much for a population larger than 20,000. For convenience and possibility of dropping out, 20% of the sample was added to the required sample. All of the 453 participants were approached consecutively as being eligible for the inclusion criteria in this study. The response rate was 85.2 resulting in a total of 386 participants.
Data collection instrument
The questionnaire was used to obtain the data from participants in the survey. The questionnaire consisted of a list of knowledge and perception items, which were developed according to the previous studies from the International Tobacco Control Project.[8,17,18] The questionnaire consisted of three parts: (1) Questions on sociodemographic data, (2) questions to determine smoking behavior and quitting intentions of the respondents, (3) questions to determine smokers' knowledge and perception of smoking health effects. The questionnaire was translated into the Arabic language to be close to the concept of the original questionnaire. Translation was performed by two authors that their mother tongue is Arabic language. Back translation from Arabic to English was done by a bilingual translator. After that, the translated version was discussed with the researchers to reword some statements to be ready for testing. The final translated version was pretested and piloted with 54 Iraqi smokers to get feedback about the clarity of the questions. Subsequently, the face and content validity of the questionnaire were checked by two health care professionals who are an expert in the field. Then, the final Arabic version was completed and recommended for the study.
Data collection procedure
A validated questionnaire was used to obtain the data from the participants. Approval for this study was obtained from the Medical Committee of Tikrit Teaching Hospital. After explaining the aims of the study and ensuring the confidentiality of responses, all participants were asked to give their consent before obtaining the data. The Arabic version questionnaire was used for data collection through close-ended questions. The questionnaire was used to obtain the data from all the participants in Arabic language. Face to face interview was conducted by the researchers to obtain the data from all the participants. The questionnaire was completed by the researchers during the time of the interview.
Data analysis
The results were analyzed using the Statistical Package for Social Sciences (SPSS, Version 15, SPSS Inc., Chicago, IL). Knowledge of the health risk effects of smoking was determined by seven health outcomes of smoking (stroke, impotence in male smokers, lung cancer, and decay in the lung of smokers, stained teeth, premature aging, and lung cancer in non-smokers). Responses were coded as “yes” =1, no/don't know = 0. The range of knowledge score was 0–7, where high score represents the high level of knowledge. For the perception items, there were two scaling methods. The score was “Not at all” =1, “Somewhat” =2, and “Very Much” =3. However, for the items “Cigarette smoke is dangerous to nonsmokers;” “tobacco is addictive;” “Every cigarette you take damages your body” the scores were “Disagree = 1, “Neither” =2, and “Agree” =3. Thus, the high score reflected a good perception.
Quitting intentions was assessed by the question “Are you planning to quit smoking.” For the scoring method, responses “within the next month,” “within the next 6 months,” and “sometimes in the future, beyond 6 months” given a score of 1 (intention); “not planning to quit” given a score of 0 (no intention). The data were described using frequency distribution. Chi-square test was used to measure the association between the perception of health effects of smoking and intentions to quit. While the Mann–Whitney test was used to find the association between the knowledge of health effects and intentions to quit. The value of P < 0.05, confidence interval 95% was considered significant. Logistic regression was carried out to examine the predictors for quitting intentions.
Results
Sociodemographic characteristics
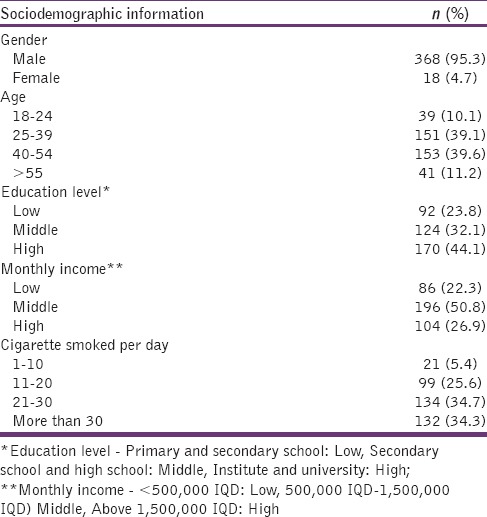
The response rate was 85.2%. The sociodemographic data for the respondents showed that the majority of the respondents were male (95.3%). The prevalence of smoking among female was low. The age group of the respondents was highly distributed between the range of 25–39 (39.1%) and 40–54 (39.6%). Table 1 shows the sociodemographic characteristics of the sample.
Table 1.
Sociodemographic characteristics of the sample
Knowledge and perception toward smoking health effects
Figure 1 shows the percentages of smokers who had awareness toward seven health risk effects of smoking outcome. The knowledge score was high for lung cancer (80.6%), decay in the lung of smokers (80.3%), and stained teeth in the smokers (72.3%); and low knowledge score for lung cancer in non-smokers (30.1%), impotence in the male smokers (52.6%), premature aging (64%), and stroke (66.3%).
Figure 1.
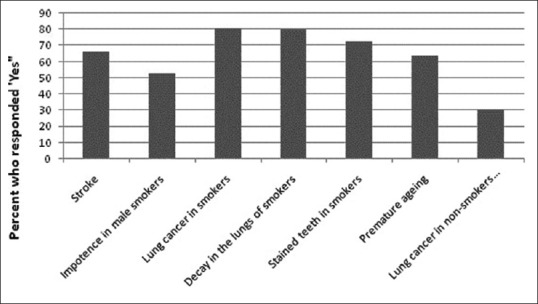
Knowledge of health risk effects
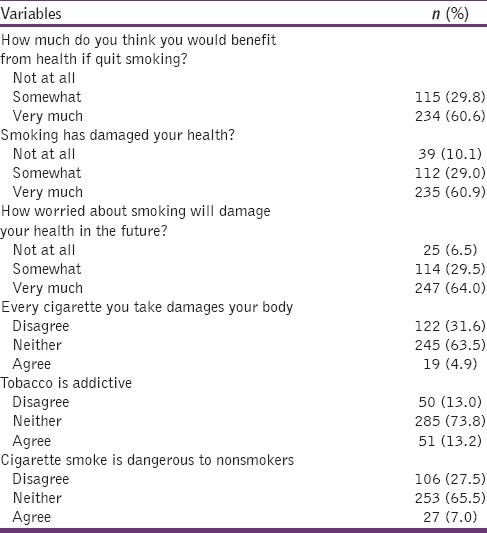
According to the perception toward smoking, Table 2 showed that smokers had a poor perception toward the health effects of smoking. The majority of them (60.9%) reported that smoking has damaged their health and worried about the effects of smoking on their health in future. However, only 7% of the sample perceived that smoking is dangerous to nonsmokers.
Table 2.
Perception towards smoking health effects
Association between knowledge of health risks effects of smoking and quit intention
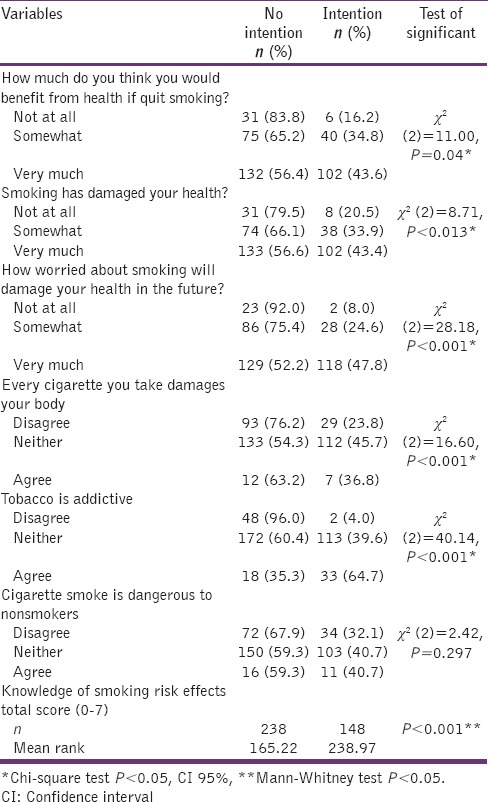
Table 3 shows the association among quitting intention and knowledge and perception of smoking health effects. The Chi-Square test showed that there were significant associations between quitting intention and smokers who had good perception toward the health effects of smoking, P < 0.05. Most of the respondents did not perceive about the harm of smoking to nonsmokers. However, there was a significant difference in quitting intention due to the health knowledge. Smokers with a high score of knowledge had more intention to quit as compared to smokers with a low score of knowledge.
Table 3.
Association between knowledge and perception of smoking health risks and intention to quit
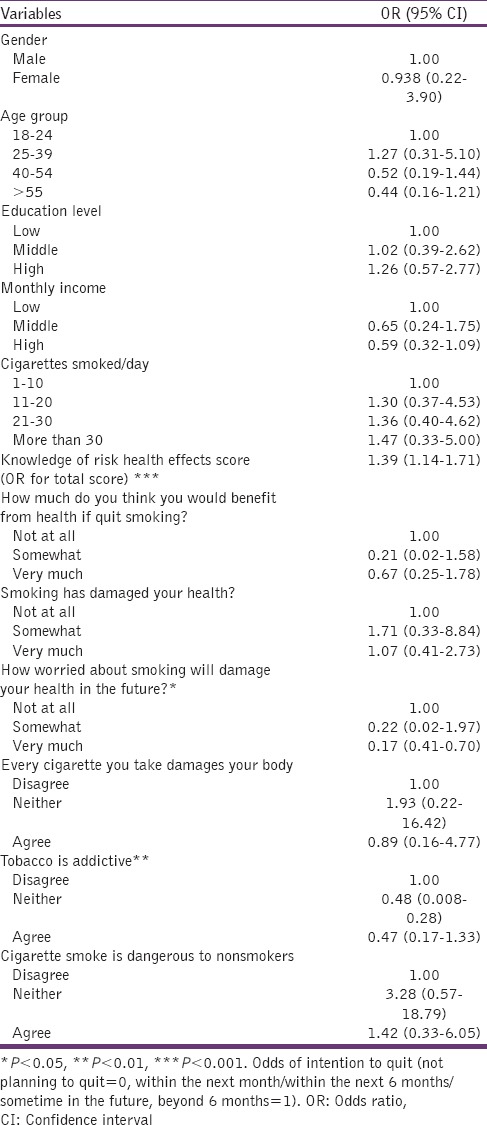
Predictors of intention to quit among current smokers
Table 4 explained the predictor factors for quitting intentions among smokers. From the sample, around 38% had the intention to quit and most of them intended to quit in the future. The knowledge of specific risk factors of smoking was significantly associated with quitting intention. In this model, the total score of knowledge and perception of smoking predicts the intention to quit.
Table 4.
Logistic regression to predict the variables of intention to quit
Discussion
The findings of this study indicated in general that the majority of Iraqi smokers have a moderate level of awareness toward the health risk effects of smoking. The majority of smokers believed that smoking causes lung cancer and decay in the lung of the smokers. Previous studies showed that smokers were aware toward smoking health effects such as lung cancer.[7,8] The results indicated that there was a low awareness in other health effects of smoking. For example, smoking is a risk factor for stroke, stained teeth, causes impotence in male smokers, and lung cancer for non-smokers from secondhand smoking. Similar results were found in a survey from India, which indicated that smokers were not aware of harms caused by smoking such as lung cancer, coronary heart disease, and lung cancer for nonsmokers.[18] A study in China reported that only half of the smokers were aware about the harm of secondhand smoking. This finding is similar to the other studies in the Western countries, where smokers reported their personal risk from smoking, most probably to minimize cognitive dissonance from smoking and protect themselves from worry.[8,19,20,21] These findings indicate that in spite of the evidence for the health risk effects of smoking, the majority of smokers worldwide have low awareness on the risks of smoking.[2]
Regarding intentions to quit, only 6.5% of the smokers had the intention to quit in the next month and 14.5% in the next 6 months. The same finding was reported in China where 24% of smokers in six states had the intention to quit,[8] and 10% of current smokers in India had the intention to quit in the next month.[18] The level of quit intention in this study was very low compared to other countries such as Canada and Australia, where around three-quarters of smokers had plans to quit smoking.[22] This might be due to the low awareness of health effects of tobacco use among Iraqi smokers.
In association with smokers' knowledge of health risk effects and quit intention, this study shows that smokers who had a high score of knowledge were more likely to have plans to quit smoking. The same results were found in China and India that there was a relation between the knowledge of health risk effects of smoking and quit intentions,[8,18] and similar to other studies that quit intention was positively associated with the awareness of the health risk of smoking.[23,24] In fact, researches on the awareness of health risk effects among smokers are not well-established globally and very little information among low and middle-income countries.[2] All the available data from the low and middle-income countries explained that health knowledge is obviously lower compared to the high-income counties, consistent with the findings of this study.
In summary, smokers' knowledge of smoking health effects was a predictor factor for intentions to quit. In addition, smokers' perception in terms of smoking will damage their health in the future and addiction to tobacco was also predicted intention to quit among smokers.
Limitations
This study was limited only to adult smokers over 18 years old so responses might not explain the awareness of possible health effects of smoking in adolescents. The sampling method was convenience sampling to recruit the subjects. This sampling method may contribute biases into the study. Furthermore, the survey was carried out in the city of Tikrit and the results may not reflect the situation for all smokers in the country. Data collection was done using close-ended questions to obtain the data. This method may have increased the level of awareness in the study. However, other methods for data collection should be adapted to predict other factors that may be associated with quitting intentions.
Conclusion
The findings of this study showed that Iraqi smokers have low awareness level toward some specific health risks caused by smoking such as lung cancer to non-smokers from secondhand smoking, impotence in male smokers, and stroke. High level of education and high monthly income were associated with high knowledge score about the health effects of smoking. However, increasing the awareness is associated significantly with quitting intentions and the number of cigarettes smoked per day. This study is very important to explain the factors which can predict intentions to quit among Iraqi smokers. It's hoped that this study would be helpful for health policy-makers and health care professionals to understand the current knowledge and perception of smoking health effects.
However, health care professionals should play an active role in communicating with their patients about the health effects of smoking to persuade Iraqi smokers to quit smoking. In addition, health policy-makers should also take an active role in designing better strategies to increase the awareness on the health risk of smoking, especially among smokers with low education level and low income. Pictorial warning was implemented in some countries and showed to be an effective way to increase the awareness level among smokers. In addition, increasing the taxes is also effective to reduce the consumption among smokers, especially those with lower socioeconomic status.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
We would like to thank the medical staff of Tikrit General Hospital for their help to conduct this study. Many thanks go to all the participants for being a part of this study and for their time and help to complete the survey.
References
- 1.Shafey O, Dolwick S, Guindon GE, editors. Tobacco Control Country Profiles. Atlanta, GA: American Cancer Society; 2003. [Google Scholar]
- 2.Geneva: World Health Organization; 2008. World Health Organization. WHO Report on the Global Tobacco Epidemic, 2008: The MPOWER Package. [Google Scholar]
- 3.Economics of Tobacco for the Middle East and North Africa (MNA) Region. Regional Report: Middle East and North Africa (MNA); 18 May. 2001. [Last accessed on 2009 Nov 15]. Available from: http://www.siteresources.worldbank.org/INTETC/Resources/375990-1089913200558/MiddleEastandNorternAfrica.pdf .
- 4.Al-Omari H, Scheibmeir M. Arab Americans' acculturation and tobacco smoking. J Transcult Nurs. 2009;20:227–33. doi: 10.1177/1043659608330353. [DOI] [PubMed] [Google Scholar]
- 5.Curry SJ, Grothaus L, McBride C. Reasons for quitting: Intrinsic and extrinsic motivation for smoking cessation in a population-based sample of smokers. Addict Behav. 1997;22:727–39. doi: 10.1016/s0306-4603(97)00059-2. [DOI] [PubMed] [Google Scholar]
- 6.Hyland A, Li Q, Bauer JE, Giovino GA, Steger C, Cummings KM. Predictors of cessation in a cohort of current and former smokers followed over 13 years. Nicotine Tob Res. 2004;6(Suppl 3):S363–9. doi: 10.1080/14622200412331320761. [DOI] [PubMed] [Google Scholar]
- 7.Siahpush M, McNeill A, Hammond D, Fong GT. Socioeconomic and country variations in knowledge of health risks of tobacco smoking and toxic constituents of smoke: Results from the 2002 International Tobacco Control (ITC) Four Country Survey. Tob Control. 2006;15(Suppl 3):iii65–70. doi: 10.1136/tc.2005.013276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Yang J, Hammond D, Driezen P, Fong GT, Jiang Y. Health knowledge and perception of risks among Chinese smokers and non-smokers: findings from the Wave 1 ITC China Survey. Tob Control. 2010;19(Suppl 2):i18–23. doi: 10.1136/tc.2009.029710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Godtfredsen NS, Lam TH, Hansel TT, Leon ME, Gray N, Dresler C, et al. COPD-related morbidity and mortality after smoking cessation: Status of the evidence. Eur Respir J. 2008;32:844–53. doi: 10.1183/09031936.00160007. [DOI] [PubMed] [Google Scholar]
- 10.Lam TH, Li ZB, Ho SY, Chan WM, Ho KS, Tham MK, et al. Smoking, quitting and mortality in an elderly cohort of 56,000 Hong Kong Chinese. Tob Control. 2007;16:182–9. doi: 10.1136/tc.2006.019505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Terres W, Becker P, Rosenberg A. Changes in cardiovascular risk profile during the cessation of smoking. Am J Med. 1994;97:242–9. doi: 10.1016/0002-9343(94)90007-8. [DOI] [PubMed] [Google Scholar]
- 12.Abughosh S, Wu IH, Hawari F, Peters RJ, Yang M, Crutchley R, et al. Predictors of intention to quit cigarette smoking among Jordanian adult. Epidemiology. 2011;1:1–7. [Google Scholar]
- 13.Abu-Baker NN, Haddad L, Mayyas O. Smoking behavior among coronary heart disease patients in Jordan: A model from a developing country. Int J Environ Res Public Health. 2010;7:751–64. doi: 10.3390/ijerph7030751. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Geneva: World Health Organization; 2011. [Last accessed on 2013 Jul 01]. Noncommunicable Disease Country Profiles 2011. Iraq. Available from: http://www.who.int/nmh/countries/irq_en.pdf . [Google Scholar]
- 15.World Health Organization; 2013. [Last accessed on 2014 Jun 16]. Cooperation Strategy for WHO and Iraq 2012-2017. Regional Office for the Eastern Mediterranean. Available from: http://www.who.int/countryfocus/cooperation_strategy/ccs_irq_en.pdf . [Google Scholar]
- 16.Atlanta, United States: Centers for Disease Control and Prevention (CDC); 2008. Centers for Disease Control and Prevention (CDC), World Health Organization (WHO). Iraq – Baghdad Global Youth Tobacco Survey 2008. [Google Scholar]
- 17.Fathelrahman AI, Omar M, Awang R, Cummings KM, Borland R, Bin Mohd Samin AS. Impact of the new Malaysian cigarette pack warnings on smokers' awareness of health risks and interest in quitting smoking. Int J Environ Res Public Health. 2010;7:4089–99. doi: 10.3390/ijerph7114089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sansone GC, Raute LJ, Fong GT, Pednekar MS, Quah AC, Bansal-Travers M, et al. Knowledge of health effects and intentions to quit among smokers in India: Findings from the Tobacco Control Policy (TCP) India pilot survey. Int J Environ Res Public Health. 2012;9:564–78. doi: 10.3390/ijerph9020564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Weinstein N, Slovic P, Waters E, Gibson G. Public understanding of the illnesses caused by cigarette smoking. Nicotine Tob Res. 2004;6:349–55. doi: 10.1080/14622200410001676459. [DOI] [PubMed] [Google Scholar]
- 20.Weinstein ND. Accuracy of smokers' risk perceptions. Ann Behav Med. 1998;20:135–40. doi: 10.1007/BF02884459. [DOI] [PubMed] [Google Scholar]
- 21.Slovic P. Smoking: Risk, perception and policy. Thousand Oaks: CA: Sage; 2001. [Google Scholar]
- 22.Chan SS, Sarna L, Wong DC, Lam TH. Nurses' tobacco-related knowledge, attitudes, and practice in four major cities in China. J Nurs Scholarsh. 2007;39:46–53. doi: 10.1111/j.1547-5069.2007.00142.x. [DOI] [PubMed] [Google Scholar]
- 23.Hammond D, Fong GT, McNeill A, Borland R, Cummings KM. Effectiveness of cigarette warning labels in informing smokers about the risks of smoking: Findings from the International Tobacco Control (ITC) Four Country Survey. Tob Control. 2006;15(Suppl 3):iii19–25. doi: 10.1136/tc.2005.012294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Romer D, Jamieson P. The Role of Perceived Risk in Starting and Stopping Smoking. In: Slovic P, editor. Smoking: Risk, Perception, and Policy. Thousand Oaks, CA: SAGE Publications, Inc; 2001. pp. 64–81. [Google Scholar]