

To the Editor: Sarcoidosis is a systemic granulomatous disorder that most commonly affects young or middle-aged women. Sarcoidosis can coexist with a wide range of autoimmune disorders and other granulomatous diseases.[1] Here, we describe a rare case of sarcoidosis coexisting with another granulomatous autoimmune disease, Takayasu arteritis (TA).
A 29-year-old woman was admitted to Department of Respiratory Medicine, Peking Union Medical College Hospital, because of aggravating shortness of breath and occasional exertional chest pain in July 2013. Since December 2011, she had suffered from a dry cough accompanied by low fever and exertional dyspnea. Laboratory results showed elevated erythrocyte sedimentation rate (ESR) (82 mm/h) and C-reactive protein (CRP) (46.4 mg/L). Antinuclear antibodies (ANA), antineutrophil cytoplasmic antibody (ANCA), and serum angiotensin converting enzyme (sACE) were all negative. Chest computed tomography (CT) showed subpleural nodules, with both hilar and mediastinal lymphadenopathy [Figure 1a]. Biopsy of the bronchial mucosa showed epithelioid cell granulomas without necrosis. She was diagnosed with tuberculosis (TB) in the local hospital. Isoniazid, Refampacin, Ethambutol plus Pyrazinamide had been prescribed to her for 6 months. But fever and cough continued, while repeated bronchoscopy and mucosal biopsy was consistent with epithelioid granulomas without necrosis in August 2012. She was diagnosed with sarcoidosis and was given prednisone in September 2012. She had no discomfort until June 2013. Her low-grade fever, dry cough, exertional dyspnea, and occasional chest pain recurred and she was admitted to our hospital. Her physical examination was unremarkable, except a slightly elevated heart rate of about 100 beats/min. Pulmonary function test, echocardiography, and repeated ECG during episodes of chest pain were normal. Holter monitoring showed no arrhythmias. Bronchoscopy showed scattered nodules in the left and right inferior basal bronchial mucosa. Bronchoalveolar lavage fliud (BALF) analysis showed a lymphocytic cellular pattern, with 16% lymphocytes and CD4/CD8 ratio of 1.0. Histology of the mucosal biopsy was still consistent with sarcoidosis [Figure 1b]. Tuberculosis polymerase chain reaction (TB-PCR) of the mucosa was negative. A positron emission tomography (PET)-CT scan was performed. The results showed thickening and hypermetabolism of the aortic wall, from the initial segment of ascending aorta to the aortic arch [Figure 1c]. These findings were considered typical for the diagnosis of TA, which was further confirmed by aortic CT angiography [CTA, Figure 1d]. The patient was then given prednisone 1 mg∙ kg-1∙ d-1 and methotrexate (MTX) 15 mg per week. Two weeks later, all of her discomfort was resolved. Prednisone was then tapered with 5 mg per week after 5 weeks of treatment. Currently, she is taking prednisone 15 mg and MTX 15 mg per week, and she remains free of symptoms and has normal ESR and CRP.
Figure 1.
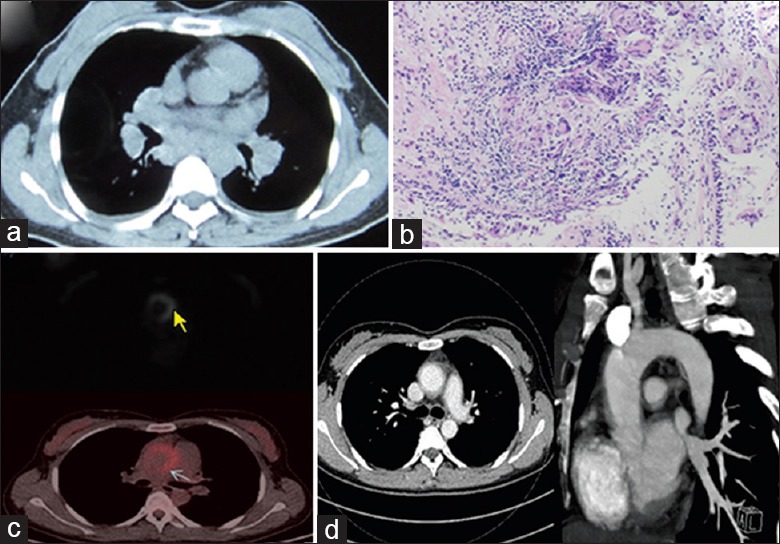
(a) The chest CT on 8 February 2012 showed hilar and mediastinal lymphadenopathy. (b) (HE staining, Original magnification ×100) Biopsy of the bronchial mucosa showed epithelioid cell granulomas without necrosis, which is consistent with sarcoidosis. (c) PET-CT scan showed thickening and hypermetabolism of the aortic wall in the ascending aorta. (d) CTA showed resolution of hilar and mediastinal lymphadenopathy and hypertrophy of the ascending aorta's wall.
Both sarcoidosis and TA are granulomatous diseases which usually affect young women. Concurrence of sarcoidosis and TA has been previously reported only in few cases.[2,3] Most of them are females under the age of 40. Large vessel manifestations, mainly inflammation and narrowing of the aortic arch and bifurcations, were usually preceded by sarcoidosis. With the earlier cases reported, it is suggested that TA and sarcoidosis may be related diseases.[3] As TA is too rare to indicate that the reported concurrence with sarcoidosis is merely governed by chance. Several common features had been found among these patients:[2] (a) Usually sarcoidosis preceded TA; (b) the time between the diagnosis of sarcoidosis and that of TA was several years (eight or more) in most of these patients; (c) the aorta and/or its major branches were affected; (d) 50% of the patients had uveitis; and (e) all patients responded well to glucocorticoid treatment.
The association of TA and sarcoidosis raises a number of questions as whether there is a possible etiologic link between these two disease entities. Or can TA or TA-like granulomatous vasculitis be considered in fact a complication of sarcoidosis? Till now, there was no definite answer to these questions. It appears reasonably important to check for large vessel inflammation in these patients. Since angiography is not a reliable method to assess for vascular inflammation, PET scan seems to be a better choice to look for these changes.
Footnotes
Edited by: Li-Shao Guo
Source of Support: This work was supported by a grant from the National Natural Science Foundation of China (No. 81170055).
Conflict of Interest: None declared.
REFERENCES
- 1.Sharma OP. Sarcoidosis and other autoimmune disorders. Curr Opin Pulm Med. 2002;8:452–6. doi: 10.1097/00063198-200209000-00019. [DOI] [PubMed] [Google Scholar]
- 2.Weiler V, Redtenbacher S, Bancher C, Fischer MB, Smolen JS. Concurrence of sarcoidosis and aortitis: Case report and review of the literature. Ann Rheum Dis. 2000;59:850–3. doi: 10.1136/ard.59.11.850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hamzaoui A, Salem R, Klii R, Harzallah O, Berriche O, Golli M, et al. Co-existing sarcoidosis and Takayasu arteritis: Report of a case. Int Arch Med. 2011;4:9. doi: 10.1186/1755-7682-4-9. [DOI] [PMC free article] [PubMed] [Google Scholar]