

Abstract
Providing optimal care to patients with recent‐onset psychosis can improve outcomes and reduce relapse. However, there is a lack of consistency of the implementation of guidelines for such patients across the Asia‐Pacific region. We determined a pragmatic set of recommendations for use on a day‐to‐day basis to help provide optimal care at this crucial stage of illness. The recommendations were developed over a series of meetings by an international faculty of 15 experts from the Asia‐Pacific region, Europe, and South Africa. A structured search of the PubMed database was conducted. This was further developed based on the faculty's clinical experience and knowledge of the literature into 10 key aspects of optimal care for patients during the first five years of a diagnosis of a psychotic disorder, with particular relevance to the Asia‐Pacific region. Several common principles emerged: adherence to antipsychotic medications is crucial; substance abuse, psychiatric and medical comorbidities should be addressed; psychosocial interventions play a pivotal role; and family members can play a vital role in overall patient care. By following these recommendations, clinicians may improve outcomes for patients with recent‐onset psychosis.
Keywords: adherence, evidence‐based practice, expert consensus, first‐episode, schizophrenia
Introduction
Evidence is emerging that relapse prevention after the initial onset of psychosis may confer significant clinical and functional benefits (Andreasen et al., 2013). Also, longer duration of untreated psychosis (DUP) is associated with worse long‐term outcome (Tang et al., 2014). For example, Fraguas et al. (2014) reported longer DUP to be associated with a lower Children's Global Assessment of Functioning (C‐GAF) score at two years, less improvement in C‐GAF, and lower rates of clinical remission in early‐onset psychosis. There is also evidence that brain‐derived neurotrophic factor (BDNF) levels are negatively correlated with DUP and may reflect both an acute neurodegenerative reaction during the untreated phase of psychosis (Rizos et al., 2010); and development of psychosis has itself been associated with progressive structural brain changes around the time of onset (Ziermans et al., 2012). Thus, prompt initiation of antipsychotic medication is a vital component of optimal care early in the course of psychosis. Of particular importance is medication adherence as non‐adherence to antipsychotic medication has a significant negative impact on treatment response (Lindenmayer et al., 2009). Poor adherence leads to an increase in hospitalization rates (Ascher‐Svanum et al., 2006; Novick et al., 2010), impaired functioning (Ascher‐Svanum et al., 2006), and an increased risk of relapse (Novick et al., 2010). Problems with adherence are particularly common during the early stages of schizophrenia, with as many as 59% of patients becoming partially adherent or non‐adherent within 12 months of their first psychotic episode (Coldham et al., 2002). Non‐adherence to antipsychotic medication during the first year following diagnosis is a significant predictor of poorer outcomes in the subsequent two years (Ascher‐Svanum et al., 2006) and the biggest predictive factor of relapse after a first episode of psychosis (Caseiro et al., 2012).
These findings highlight the importance of providing optimal care in a timely fashion to patients in the early stages of their disease. There is compelling literature on optimal care in recent‐onset psychosis; however, these guidelines may not have been uniformly adopted in the Asia‐Pacific (A‐P) region. Therefore, there is a need to evaluate the available evidence and identify the key aspects of optimal care for patients during recent‐onset psychosis which are applicable in the A‐P region. The A‐P region is extremely diverse with different health care systems, levels of socioeconomic development and cultural attitudes, and we recognize that it is not possible to provide that same level of treatment throughout the region. To this end, we aimed to evaluate the recent evidence relating to the first five years of a diagnosis of psychosis and reach consensus about general principles of care that could become expected clinical practice across the A‐P region.
Methods
An international group of 15 clinicians from the A‐P region, Europe and South Africa (Australia [DC, MW]; mainland China [YH, TS]; Hong Kong [TLL]; India [SK, MT]; Indonesia [NA]; Malaysia [AH]; Philippines [TB]; Singapore [CL]; South Africa [RE]; Spain [JO]; Taiwan [YKY], and Thailand [RK]) with extensive experience of treating patients with schizophrenia and an interest in recent‐onset psychosis convened to propose a concise set of principles aimed at helping psychiatrists within the A‐P region to provide optimal care to recent‐onset psychosis patients.
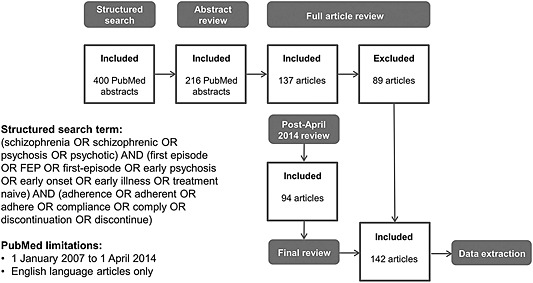
A structured literature search was conducted focusing on the impact of adherence, as this was considered one of the key influences on treatment outcomes on recent‐onset psychosis. The search of PubMed used the following search terms: (schizophrenia OR schizophrenic OR psychosis OR psychotic) AND (first episode OR FEP OR first‐episode OR early psychosis OR early onset OR early illness OR treatment naive) AND (adherence OR adherent OR adhere OR compliance OR comply OR discontinuation OR discontinue) limited to English language articles published between 1 January 2007 and 1 April 2014. Initially, 400 abstracts were identified and subsequently reviewed by a medical writer against the search criteria. Of these, 216 were retained for abstract review by the core group of clinicians (TLL, RE, JO, DC). Ultimately, 137 full articles were selected and reviewed to evaluate the level of evidence and identify key themes.
Articles previously highlighted for rejection at full article review stage were also reassessed (see Figure 1).
Figure 1.
Structured literature search. FEP, first episode psychosis.
In addition, based on their clinical experience and knowledge of the literature, the core group considered that a number of additional aspects beyond treatment adherence were relevant in providing optimal care and outcomes for patients with recent‐onset psychosis. They delineated nine proposed themes for consideration and discussion with the wider group of clinicians. The wider group revised the proposed themes and reached agreement on 10 aspects of care that should be the focus for delivering optimal benefits for patients following the first five years of a diagnosis of psychosis with a particular focus on their feasibility and applicability in the diverse settings of the A‐P region. At this stage, an additional 94 articles were included and 89 of the original full articles were discarded, leaving a total of 142 articles. The 10 themes and our recommendations are shown in Table 1. The rationale for their inclusion is discussed below.
Table 1.
Themes and recommendations
| Theme | Recommendation |
|---|---|
| 1. Strategic engagement of patients with recent‐onset psychosis is important to the success of subsequent care | Treating positive symptoms with a reactive admission‐based approach and little or no follow‐up is a suboptimal approach. It is not enough to manage an episode of psychosis as an isolated event. Once a patient is discharged, ongoing continuity of community care, together with consistency within the treatment team, where possible, are crucial. This approach will facilitate a deeper level of engagement with the patient and their family and a greater understanding of the patient's individual needs and broader issues, thereby assisting with the selection of optimum interventions to promote continued recovery. This theme reflects a need for willingness, on the part of patients, HCPs and families, to engage in continuous and monitored treatment and acknowledges the importance of a combined approach that includes both family members and HCPs. |
| 2. Effective symptom control in recent‐onset psychosis can usually be achieved with antipsychotics | While we acknowledge that the availability, cost, and reimbursement status of different antipsychotics varies throughout the A‐P region, patients and their families should be informed of the pharmacological treatment options available to them including possible AEs. |
| 3. Restoring psychosocial function in recent‐onset psychosis is an essential component in recovery | Remission and recovery are achievable for many patients providing they are well informed, adequately treated, and closely monitored. The expectations of patients and their caregivers should be taken into account when evaluating remission and recovery, together with a realistic and culturally sensitive outlook provided by the HCP. |
| 4. Medication adherence is a critical contributor to relapse reduction in recent‐onset psychosis | Adherence to medication is crucial in preventing relapse and improving outcomes in schizophrenia. Patients should be warned of the dangers of stopping their medication and that they may be required to keep taking medication despite improvement in their symptoms. Care should be taken by HCPs when conveying this information as poor timing and/or bad phrasing can reduce the patient's willingness to comply. Interventions that directly improve adherence behavior, especially those that target substance abuse and depressive symptoms, should be developed. Measures to improve patient insight could be a specific target of treatment in early intervention programs. |
| 5. Long‐acting injectable antipsychotics should be considered in recent‐onset schizophrenia | While we acknowledge that there is a need for a large‐scale, randomized controlled trial comparing oral and LAI APs in recent‐onset psychosis, to assess long‐term outcomes, we believe LAI APs may play a role in relapse prevention via increased rates of adherence and should be considered as an early stage treatment. LAI APs are frequently perceived by patients and family members as an indication that the patient has a severe mental illness and are therefore reluctant to use them. However, many first‐episode patients respond well to LAI APs and, once provided with balanced information, are open to their use. |
| 6. Psychosocial interventions contribute much to desirable clinical outcomes in recent‐onset psychosis | A number of culturally adapted psychosocial therapies are now available throughout the A‐P region. Psychosocial therapies, together with continuous antipsychotic therapy, facilitate recovery and improve adherence to treatment, thereby offering significant benefits to recent‐onset patients in social and vocational aspects. Psychosocial therapies should be implemented early to prevent deterioration of psychosocial and cognitive functions. |
| 7. Involvement of families and carers is an integral part of comprehensive patient management in recent‐onset psychosis | As already highlighted in themes 1, 2, and 6, family members and carers play an important role in supporting patients with medication adherence and day‐to‐day tasks. Stigma may prevent patients and family members seeking help during the early stages of the disease and beyond. Efforts should be made to reduce stigmatizing behavior within health care services and society as a whole particularly in countries where there is strong stigma attached to mental illness. The sociocultural context is important to take into account in discussions with family members. |
| 8. Substance abuse in recent‐onset psychosis impacts negatively on outcomes and needs to be addressed | Comorbid substance abuse can worsen symptoms and outcomes and is a growing problem in the A‐P region, despite the variability in the rates and types of substances abused. The negative contribution that illicit drugs and alcohol make to the course of the illness, not least the legal complications, including a heightened risk of incarceration should be emphasized early in the treatment pathway. Patients should be offered interventions that address comorbid substance abuse in a culturally sensitive manner. |
| 9. Psychiatric comorbidities are common and should be addressed in recent‐onset psychosis | Psychiatric comorbidities such as depression and anxiety disorders can have a negative impact on outcomes. We recommend that psychiatric comorbidities be given high priority during treatment planning in the context of the socioeconomic and cultural background. |
| 10. Medical comorbidities are common and should be monitored and addressed fastidiously in recent‐onset psychosis | Psychiatrists should be conscious of the physical conditions and metabolic issues associated with the use of antipsychotic drugs and the potential for antipsychotic therapies to worsen existing conditions such as diabetes and compromised lipid metabolism. Strategies to improve health and well‐being should be promoted early on, and all patients should be screened regularly for metabolic abnormalities. |
AE, adverse event; A‐P, Asia‐Pacific; HCP, healthcare professional; LAI AP, long‐acting injectable antipsychotic.
Results
Theme 1: Strategic engagement of patients with recent‐onset psychosis is important to the success of subsequent care
Poor therapeutic alliance predicts poor service engagement (Lecomte et al., 2008) and poor adherence (Tunis et al., 2007; Montreuil et al., 2012) in recent‐onset psychosis. In turn, the severity of positive symptoms, agreeableness as a personality trait, and poor capacity in building an alliance, all have a negative impact on treatment adherence and service engagement (Lecomte et al., 2008). The patient's decision to stay with treatment is dependent upon relationships between clinicians who embrace patient‐centered perspectives and peers who have also experienced first‐episode psychosis (FEP) (Stewart, 2013). A critical time for engagement is the transition between initial treatment and community care (Tiihonen et al., 2011). Success of this transition is marked by patient contact with patient‐centered care providers and a supportive peer group. Patient‐centered early intervention staff is important for engagement (Stewart, 2013).
Patients have different needs based on their age, education, and support systems; older first‐episode patients tend to have an increase in metabolic and mood disorder comorbidity, and a longer DUP (Selvendra et al., 2014). Patients who are older at initial diagnosis often achieve better outcomes than younger patients (Rabinowitz et al., 2006).
Within the A‐P region, the patient's family plays a particularly important role in many aspects of care. For example, Filipino psychiatrists always seek actively to engage with, and seek the help of, the patient's family, especially to provide an understanding of the nature of the illness. Family members are trained to assist patients with recovering psychosocial functions and play a key role with medication adherence. Due to the stigma associated with schizophrenia, peer group interventions are unpopular and patients and families seek to keep the illness a private, family matter wherever possible (Bautista T, 2015 personal communication).
Treating positive symptoms with a reactive admission‐based approach and little or no follow‐up is a sub‐optimal approach. It is not enough to manage an episode of psychosis as an isolated event. Once a patient is discharged, ongoing continuity of community care, together with consistency within the treatment team, where possible, are crucial. This approach will facilitate a deeper level of engagement with the patient and their family and a greater understanding of the patient's individual needs and broader issues, thereby assisting with the selection of optimum interventions to promote continued recovery. This theme reflects a need for willingness, on the part of patients, health care professionals (HCPs) and families, to engage in continuous and monitored treatment and acknowledges the importance of a combined approach that includes both family members and HCPs.
Theme 2: Effective symptom control in recent‐onset psychosis can usually be achieved with antipsychotics
Patterns of prescribing differ widely across the A‐P region. The Health Insurance Review & Assessment Service‐National Patients Sample was a stratified sampling from the entire population under the South Korean national health security system in 2009 (Park et al., 2014). The 26,254 patients who were prescribed first‐generation antipsychotics (FGAs) only were significantly older, more likely to be male and on Medicaid, had higher total medical costs and lower rates of self‐payment, and higher co‐medication rates of anti‐Parkinsonian agents and anxiolytics than the 67,361 patients prescribed second‐generation antipsychotics (SGAs) only (Park et al., 2014). Japan has a high frequency of polypharmacy (Kishimoto et al., 2013b). Singapore has a high utilization of depot injections (Chong et al., 2004). Owing to the availability of inexpensive generics, clozapine has been extensively used in China for the treatment of resistant and non‐resistant schizophrenia for longer than in any other East Asian country (Chong et al., 2004). Haloperidol is the most commonly prescribed antipsychotic in Malaysia and a third of patients are prescribed SGAs, with olanzapine the most common (Yoon and Aziz, 2014). Strict regulations for the use of SGAs, including clozapine, have been implemented in other countries, making it difficult to prescribe these drugs; however, there has been an increase in their use in recent years (Shinfuku and Tan, 2008; Tan et al., 2008).
Positive symptoms are more readily addressed by antipsychotic treatments and the negative and cognitive symptoms which often remain are a considerable impairment for patients (Citrome, 2014). Meta‐analysis of the efficacy and tolerability of FGAs versus SGAs in FEP shows that, when pooled, SGAs are similar to FGAs regarding total psychopathology change, depression, treatment response, and metabolic changes (Zhang et al., 2013a). SGAs significantly outperformed FGAs regarding lower treatment discontinuation (irrespective of cause), negative symptoms and global cognition; and were associated with fewer extrapyramidal symptoms and akathisia. In contrast, SGAs tended to be associated with more weight gain (P < 0.05–0.01) (Zhang et al., 2013a). A meta‐analysis of the relapse rates associated with FGAs versus SGAs failed to demonstrate a consistent superiority of individual SGAs over FGAs. Nevertheless, SGAs as a group were associated with less study‐defined relapse, overall treatment failure and hospitalization, than FGAs, with a modest but clinically relevant effect size (Kishimoto et al., 2013a). Meta‐analysis of mid‐ to long‐term outcomes associated with SGAs showed efficacy not only during the acute phase but, more importantly, as maintenance treatments (Glick et al., 2011).
Some long‐term studies of FEP have found no difference between individual SGAs in clinical and functional outcomes, (Shrivastava et al., 2012) whereas others demonstrate benefits for particular SGAs. For instance, olanzapine might lead to longer treatment continuation in treatment‐naive FEP patients than haloperidol and, possibly, ziprasidone (San et al., 2012). What is clear is that appropriate antipsychotic options are available to address symptoms in recent‐onset psychosis (Schimmelmann et al., 2007; Gafoor et al., 2010).
Clozapine has a high maintenance rate (Noguera et al., 2013), and may have a marginally superior efficacy in the initial year of treatment of treatment‐naive FEP patients, which can be explained for the most part by greater adherence (Sanz‐Fuentenebro et al., 2013). Guidelines recommend that clozapine should be considered as a third‐line treatment as it leads to earlier and longer remission intervals (Remington et al., 2013); however, identification of true refractoriness should be made as early as possible and clozapine considered earlier rather than later. Antipsychotics are effective treatments in FEP at doses lower than those used in patients with long‐term schizophrenia (Gafoor et al., 2010; Zhang et al., 2013a) though they may be associated with a relatively higher incidence of adverse effects (AEs) such as tardive dyskinesia (Zhang et al., 2013a).
Current (UK) National Institute for Health and Care Excellence (NICE) guidelines recommend the integration of pharmacological and psychosocial treatments for optimal long‐term outcomes for patients with schizophrenia (NICE, 2014). Long‐acting injectable antipsychotics (LAI APs) should be considered for patients with recurrent relapses related to partial/non‐adherence. The oral form of the same medication is the logical choice for initial treatment (APA, 2004; Lehman et al., 2004).
Whilst we acknowledge that the availability, cost and reimbursement status of different antipsychotics varies throughout the A‐P region, patients and their families should be informed of the pharmacological treatment options available to them including possible AEs.
Theme 3: Restoring psychosocial function in recent‐onset psychosis is an essential component in recovery
Improvements in patient functioning have a considerable impact on patients' lives, which in turn will improve quality of life and reduce carer burden (Durmaz and Okanlı, 2014). Remission is significantly associated with adherence, and outcome is significantly associated with good adherence to medication (Bachmann et al., 2008; Hassan and Taha, 2011). While there has been some discussion around remission being able to be achieved with low dose or intermittent treatment (Wunderink et al., 2007, 2013), there is consistent evidence that relapse rates are high following discontinuation regardless of the preceding period of stabilization (Subotnik et al., 2011; Emsley et al., 2012, 2013; Zipursky et al., 2014). Relapse, following discontinuation, frequently occurs with little warning (Gaebel and Riesbeck, 2014) and once illness recurs, symptom severity rapidly returns to previous levels. Furthermore, treatment nonresponse may emerge in a subset of patients after relapse (Emsley et al., 2013).
Long‐term remission can be achieved in FEP patients for a relatively long follow‐up period (Üçok et al., 2011; Morgan et al., 2014). Strategies to reduce DUP and achieve early response could improve remission rates in FEP patients (Verma et al., 2012). Both negative symptoms (Austin et al., 2013) and neurocognitive deficits (Fervaha et al., 2014) play a central role in the process of recovery from schizophrenia.
Remission of symptoms alone is no longer considered sufficient and recovery is about a broader set of psychosocial outcomes (Andreasen et al., 2005). The physician's view of recovery (e.g. maintaining a job in a supermarket) does not always match with family/carer's views, where there is often an expectation that recovery will be reflected in a return to the pre‐disease state (Siu et al., 2012). Such views might be impacted by social role expectations that vary across the A‐P region. For instance, mental health nurses in Thailand (Kaewprom et al., 2011) tend to view recovery as symptomatic remission rather than the emerging, consumer‐based concept of personal recovery (Tse et al., 2014). Rates of functional recovery are lower than those of symptomatic remission (Menezes et al., 2009; Henry et al., 2010). Nevertheless, patients enrolled in specialized early intervention programs can achieve both social/vocational recovery and symptomatic remission (Henry et al., 2010).
Remission and recovery are achievable for many patients providing they are well informed, adequately treated, and closely monitored. The expectations of patients and their caregivers should be taken into account when evaluating remission and recovery.
Theme 4: Medication adherence is a critical contributor to relapse reduction in recent‐onset psychosis
In a recent survey, 56% of patients with psychosis in the A‐P region were judged by their psychiatrists to be partially or non‐adherent to medication, while only 32% of patients related clinical deterioration to antipsychotic non‐adherence (Olivares et al., 2013). Patients' insight and treatment adherence significantly predict the clinical course and functional outcome in FEP (Steger et al., 2012). A better attitude toward antipsychotic medication at the first lifetime psychiatric admission is significantly related to lower all‐cause antipsychotic treatment discontinuation following a first early‐onset psychotic episode (Fraguas et al., 2008). There are complex and often overlapping factors that influence non‐adherence. Ongoing substance abuse/dependence (Tunis et al., 2007; Perkins et al., 2008) and depressive symptoms (Perkins et al., 2008) are associated with poor adherence and are significant predictors of treatment discontinuation. Non‐adherence early after discharge is associated with a higher risk or hospitalization (Bodén et al., 2011); however, adherence and outcome are similar irrespective of whether a patient's first hospitalization was involuntary or voluntary (Opjordsmoen et al., 2010). Medication costs have also been associated with poor adherence especially in developing countries such as India (Shoib et al., 2014) and Pakistan (Tharani et al., 2013).
A poor treatment response may cause some patients to stop medications prematurely (Perkins et al., 2008), while others may become non‐adherent if their symptoms improve – presumably because they believe that they no longer require treatment (Steger et al., 2012). Of these, FEP patients who experience a rapid reduction of negative symptoms are at particularly high risk of non‐adherence and should be closely monitored (Steger et al., 2012). There is also a subgroup of patients who refuse medication altogether; a medical file audit of 605 FEP patients revealed that almost 20% were persistent medication refusers (Lambert et al., 2010). In this group, poor premorbid functioning, comorbid substance use, poor insight, forensic history, and a lack of previous contact with psychiatric care predicted medication refusal (Lambert et al., 2010).
Relapse rates in the three years following the first psychotic episode are high at around 50% (Gearing et al., 2009; Hui et al., 2013). Non‐adherence to medication is highly predictive of relapse (Gearing et al., 2009; Novick et al., 2010; Alvarez‐Jimenez et al., 2012; Caseiro et al., 2012; Hui et al., 2013) and even brief periods of partial non‐adherence (2–4 weeks) lead to a greater risk of relapse (Subotnik et al., 2011). Relapse prevention after the initial onset of schizophrenia may convey a significant clinical benefit (Andreasen et al., 2013). Therefore, strategies to enhance treatment adherence, as a way of preventing relapse, should be implemented at the time of illness onset. This is especially important since early warning signs of relapse are often unreliable (Gaebel and Riesbeck, 2014) and “rescue” medication may prove ineffective in preventing a full‐blown psychotic recurrence (Emsley et al., 2013).
Adherence to medication is crucial in preventing relapse and improving outcomes in schizophrenia. Patients should be warned of the dangers of stopping their medication and that they may be required to keep taking medication despite improvement in their symptoms. Care should be taken by HCPs when conveying this information as poor timing and/or bad phrasing can reduce the patient's willingness to comply. Interventions that directly improve adherence behavior, especially those that target substance abuse and depressive symptoms, should be developed. Measures to improve patient insight could be a specific target of treatment in early intervention programs.
Theme 5: Long‐acting injectable antipsychotics should be considered in recent‐onset schizophrenia
Despite their potential advantages, most treatment guidelines advise limiting the use of LAI APs to multiple‐episode or non‐adherent patients, with controversy in relation to their role in early schizophrenia (Kim et al., 2012); however, recommendations for LAI AP use early in the disease course are emerging, not least during the first two to five years following diagnosis (Malla et al., 2013) and as maintenance treatment following the initial episode (Llorca et al., 2013). Using LAI APs as the initial therapeutic treatment can reduce relapse rates and improve prognosis (Viala et al., 2012), and many first‐episode patients taking oral antipsychotics will accept a recommendation of the corresponding LAI therapy (Weiden et al., 2009). Recent‐onset psychosis patients receiving LAIs show more symptom reduction and better health‐related quality of life and functional outcomes (Emsley et al., 2008) as well as significantly lower 1‐ and 2‐year relapse rates than patients receiving oral therapy (Kim et al., 2008). LAI APs may be useful in the treatment of recent‐onset psychosis in terms of symptom control and relapse reduction, particularly if chosen by the patient or when medication adherence is a priority (Taylor and Ng, 2013). However, in a recent survey, only one in three psychiatrists from mainland China, India, Australia, Taiwan, Vietnam, New Zealand, Indonesia, Hong Kong, the Philippines, Thailand, Singapore, Malaysia, and South Korea favored switching to or adding an LAI AP as their preferred treatment option for addressing adherence problems, compared with three in five psychiatrists practicing in Europe (Olivares et al., 2013). A survey conducted in 2004 in East Asia showed that LAI APs were prescribed in 15.3% (368/2399) of patients, rates were highest in Singapore (75.0%), followed by Taiwan (20.3%), Japan (6.2%), mainland China (5.9%), and Hong Kong (4.7%) (Sim et al., 2004). The current prescription rate of LAI APs is less than 1% in South Korea which may reflect negative attitudes, inexperience, or reluctance of psychiatrists rather than patient resistance (Kim et al., 2013).
While we acknowledge that there is a need for a large‐scale, randomized controlled trial comparing oral and LAI APs in recent‐onset psychosis, to assess long‐term outcomes, we believe LAI APs may play a role in relapse prevention via increased rates of adherence and should be considered as an early‐stage treatment. LAI APs are frequently perceived by patients and family members as an indication that the patient has a severe mental illness and are therefore reluctant to use them. However, many first‐episode patients respond well to LAI APs and, once provided with balanced information, are open to their use.
Theme 6: Psychosocial interventions contribute much to desirable clinical outcomes in recent‐onset psychosis
Community psychosocial interventions for schizophrenia have been found to be effective in reducing positive and negative symptoms and general psychopathology, both after the first psychotic episode and at other stages of the illness (Armijo et al., 2013). Both long‐term psychosocial therapies (Zaytseva et al., 2010) and peer support initiatives (Boardman et al., 2014) can be effective in improving medication adherence. Specific adherence coping education therapy is well accepted and associated with significant decreases in symptoms, as well as trend‐level improvements in attitudes toward treatment (Uzenoff et al., 2008). Cognitive Behavioral Therapy (CBT) is widely accepted as an effective intervention for the treatment of FEP (Fanning et al., 2012). However, when CBT is available as part of a package of phase‐specific interventions within an early intervention service, it appears that individuals who have fewer years in education and more negative symptoms are less likely to engage with and complete the treatment (Fanning et al., 2012). A longer DUP and a low level of insight also predict poor adherence to CBT (Alvarez‐Jiménez et al., 2009). Treatment in specially designed early detection and intervention centers may improve functioning of people with an early initial prodromal state of psychosis, and although both CBT and supportive counseling (SC) led to significant social adjustment improvements, CBT was not superior to SC at the end of treatment (Bechdolf et al., 2007). CBT has been culturally adapted for low and middle‐income countries and has been effective in reducing psychopathology and improving insight in Pakistani patients (Naeem et al., 2015). Phase‐specific early psychosocial interventions in Hong Kong have been shown to substantially reduce hospitalization and symptoms (Chen et al., 2012).
Meta‐analysis shows that interventions that include families are more effective in reducing symptoms by the end of treatment and preventing relapse at 7–12 month follow‐up (Lincoln et al., 2007). Furthermore, young people and their parents are more likely to endorse informal social supports, generic counseling, and general stress reduction methods than taking antipsychotic medication, using mental health services, or the helpfulness of seeing a psychiatrist (Jorm et al., 2008). Interventions involving family members have been shown to improve outcomes in mainland China, Hong Kong, and Australia (in both English and Vietnamese families (Bradley et al., 2006; Chien and Wong, 2007; Chien and Chan, 2013; Chien and Thompson, 2013; Chen et al., 2014).
Interventions of a purely educational nature are the least successful at improving antipsychotic adherence, and the greatest improvements are seen with interventions employing combinations of educational, behavioral, and affective (designed to optimize social and emotional support) strategies (Dolder et al., 2003). Combination strategies also reduce relapse, decrease hospitalization, decrease psychopathology, improve social function, provide gains in medication knowledge, and improve insight into the need for treatment. Longer interventions and a good therapeutic alliance are also important for successful outcomes (Dolder et al., 2003). Vocational programs, especially the individual placement and support model, are effective in schizophrenia and have been validated in many different cultures (Mueser and McGurk, 2014) including in Hong Kong (Kin Wong et al., 2008), Australia (Killackey et al., 2008), and Japan (Sato et al., 2013).
A number of culturally adapted psychosocial therapies are now available throughout the A‐P region. Psychosocial therapies, together with continuous antipsychotic therapy, facilitate recovery and improve adherence to treatment, thereby offering significant benefits to recent‐onset patients in social and vocational aspects. Psychosocial therapies should be implemented early to prevent deterioration of psychosocial and cognitive functions.
Theme 7: Involvement of families and carers is an integral part of comprehensive patient management in recent‐onset psychosis
In recent years, the responsibility of care has seen a global shift in emphasis from the hospital setting to patients' families (Gutiérrez‐Maldonado et al., 2005; Awad and Voruganti, 2008). Families have traditionally been the mainstay of care for the mentally ill in the A‐P region (Chakrabarti, 2011), and the move toward greater deinstitutionalization has resulted in about 70% of East Asian patients with schizophrenia being cared for in the community by their families (Chan, 2011). Recent initiatives including psychoeducational programs involving family members improve relapse rates (Lincoln et al., 2007).
Within the A‐P region, case management and mutual support groups involving family members have been shown to reduce symptoms and improve functioning in patients in mainland China, Hong Kong, and Australia (in both English and Vietnamese speaking families) (Bradley et al., 2006; Chien and Wong, 2007; Chien and Chan, 2013; Chien and Thompson, 2013; Chen et al., 2014).
However, non‐professional carers of patients with schizophrenia experience a considerable level of burden due to the significant demands imposed by the condition, which impacts detrimentally on their quality of life. In 1937, the Japanese Society of Psychiatry and Neurology approved the translation of the term schizophrenia as “seishin‐bunretsu‐byo” (Chinese pronunciation “jing‐shen‐fen‐lie‐zheng,” Korean pronunciation “jungshinbunyeolbyung”). The Japanese Society of Psychiatry and Neurology replaced the old term with “togo‐shitcho‐sho (integration disorder)” in 2002 at the request of the National Federation of Families of the mentally ill in Japan (Sato, 2008). In Hong Kong, the term “si‐jue‐shi‐diao” (dysregulation of thought and perception), which means psychosis, has been used instead of “jing‐shen‐bing” in an effort to make psychiatric services more accessible to young people with psychosis (Chung and Chan, 2004). Taiwan uses the term “si‐jue‐shi‐diao” (Sartorius et al., 2014). In 2011, the Korean Neuropsychiatric Association and the Korean Society of Schizophrenia Research replaced the old term with “johyeonbyung” (metaphorically describing schizophrenia as a disease of inadequate tuning of the neural network or the mind) following a South Korean Internet schizophrenia advocacy group petition (Lee et al., 2014). Despite these and other efforts throughout the A‐P region to reduce the stigma associated with schizophrenia, patients and families continue to be stigmatized and discriminated against.
The 97 FEP patients surveyed as part of the Italian Psychosis Incident Cohort Outcome Study reported experiencing discrimination in several key life areas; in relationships with family members (43%), making friends (32%), relationships with neighbors (25%), keeping a job (25%), finding a job (24%), and intimate relationships (23%) (Lasalvia et al., 2014). Patients' awareness of the negative consequences of symptoms and disabilities led them to perceive discrimination more easily and anticipated discrimination further limited their access to life opportunities; 37% had stopped seeking a close relationship and 34% had stopped looking for work, 58% felt the need to conceal their diagnosis, and 37% reported that other people avoided them (Lasalvia et al., 2014). Relatives may experience “stigma by association,” and this can be greater in relatives experiencing mental health problems of their own (Ostman and Kjellin, 2002).
In a study of 441 patients in urban northern China, the majority sought nonmental health pathways first rather than contacting mental HCPs directly. On average, each patient consulted 3.4 carers, and the vast majority first visited local tertiary general hospitals (56.4%) or local secondary general hospitals (24.8%) (Zhang et al., 2013b). Mental health stigmatizing attitudes in Japan are stronger than in countries such as Taiwan or Australia, possibly due to institutionalism, lack of national campaigns to tackle stigma, and/or society's valuing of conformity in Japan (Ando et al., 2013). Stigma toward patients with schizophrenia among the Malay community is strong, and individuals who have been exposed to patients with schizophrenia or neurotic illnesses tend to have better perceptions toward schizophrenia than the general public (Razali and Ismail, 2014). A survey of 133 Chinese patients with schizophrenia revealed that education level impacts on the perception of stigma (Ren et al., 2014); therefore, more psychoeducation should be undertaken to improve patients' knowledge about schizophrenia.
As already highlighted in themes 1, 2, and 6, family members and carers play an important role in supporting patients with medication adherence and day‐to‐day tasks. Stigma may prevent patients and family members seeking help during the early stages of the disease and beyond. Efforts should be made to reduce stigmatizing behavior within healthcare services and society as a whole particularly in countries where there is strong stigma attached to mental illness. The socio‐cultural context is important to take into account in discussions with family members.
Theme 8: Substance abuse in recent‐onset psychosis impacts negatively on outcomes and needs to be addressed
Relative to the general population, individuals with severe psychotic disorders have increased risks for smoking (odds ratio [OR] 4.6, 95% confidence CI 4.3–4.9), heavy alcohol use (OR 4.0, 95% CI 3.6–4.4), heavy cannabis use (OR 3.5, 95% CI 3.2–3.7), and recreational drug use (OR 4.6, 95% CI 4.3–5.0) (Hartz et al., 2014). Around half of patients have a lifetime diagnosis of comorbid substance abuse (Buckley et al., 2009). Patients with comorbid substance abuse have more positive symptoms, a greater risk of relapse, heightened risk of violence and suicide, more medical comorbidities, and a greater propensity to antipsychotic‐related side‐effects (Buckley et al., 2009). There are high rates of substance misuse in recent‐onset psychosis. For example, in the Spanish Child and Adolescent First Episode Psychosis study, rates were: tobacco 30.9%, cannabis 29.1%, alcohol 21.8%, cocaine 8.2%, amphetamines 2.7%, lysergic acid diethylamide (LSD) 1.8%, and opiates 0.9% (Baeza et al., 2009), and persistent substance misuse is associated with poor outcome in the first year after presentation (Turkington et al., 2009). Cannabis, alcohol, and tobacco/nicotine are the most commonly used substances in those at clinical high risk of developing psychosis, although there is limited evidence to suggest that increased rates of substance use may be associated with transition to psychosis (Addington et al., 2014).
Greater doses of cannabis have been associated with subsequent higher depression and anxiety (Barrowclough et al., 2015), and cannabis use may be related to higher positive symptom scores for FEP patients (Baeza et al., 2009). Cannabis use is associated with discontinuation of antipsychotic medication in recent‐onset psychosis (van Nimwegen‐Campailla et al., 2010), and cannabis abusing FEP patients may be making two crucial decisions during treatment: whether to reduce or cease consumption of cannabis, and whether or not to continue to take medications (Faridi et al., 2012).
Cocaine and ecstasy use is relatively uncommon in the A‐P region, and cannabis use is below the global average. But opioid and amphetamine‐type stimulant use is common, and there is an emerging trend in the use of ketamine, particularly in Hong Kong where use increased from 9.8% of total drug users in 2000 to 37.6% in 2009 (Dargan and Wood, 2012). These differences are reflected in the varied rates of substance abuse seen in patients with recent‐onset psychosis in the A‐P region. For instance, among first‐episode treatment‐naive patients with psychosis in Bangalore, Southern India, the rate of alcohol dependence was 17.3% and cannabis dependence 3.6%; lifetime and current use of cannabis was less than 6% (Chand et al., 2014). Self‐reported cannabis use among 3644 patients receiving treatment for schizophrenia or schizoaffective disorder at the Provincial General Hospital, Ratnapura, Sri Lanka, over five years (2000–2004) was less than 3%, and all cannabis users were men (Rodrigo et al., 2010). Nevertheless, there is within‐country variation, with an 11‐year study of psychiatric comorbidity in patients with substance abuse disorders attending an addiction treatment center in Northern India reporting that inhalant and cannabis use was more likely to be found with psychotic disorders and that 71.5% of patients with a psychotic disorder had more than one substance abuse disorder (Basu et al., 2013).
There is some evidence that dual diagnosis patients might have a better outcome when prescribed clozapine, with less relapse into abuse of drugs or alcohol (Buckley et al., 2009). Identification and treatment of substance misuse should be a key component of early intervention services with implications for staff training and structure of services (Turkington et al., 2009).
Comorbid substance abuse can worsen symptoms and outcomes and is a growing problem in the A‐P region, despite the variability in the rates and types of substances abused. The negative contribution that illicit drugs and alcohol make to the course of the illness, not least the legal complications, including a heightened risk of incarceration, should be emphasized early in the treatment pathway. Patients should be offered interventions that address comorbid substance abuse in a culturally sensitive manner.
Theme 9: Psychiatric comorbidities are common and should be addressed in recent‐onset psychosis
Psychiatric comorbidities are common among patients with schizophrenia at all phases of the illness. There is an estimated prevalence of 15% for panic disorder, 29% for post‐traumatic stress disorder (PTSD), and 23% for obsessive–compulsive disorder. Comorbid panic and PTSD symptoms may be associated with more severe psychopathology, as well as increased risks of suicidal ideation and behavior (Buckley et al., 2009). Panic symptoms may also increase vulnerability to comorbid substance use (Buckley et al., 2009). It is estimated that comorbid depression occurs in 50% of patients and is associated with a heightened risk of relapse (Buckley et al., 2009). Aripiprazole and quetiapine in particular may improve depressive symptoms in FEP (Crespo‐Facorro et al., 2013).
Clozapine has established antisuicidal effects (Kasckow et al., 2011; Meltzer, 2012), but it may take several months for this to become apparent, and a high dose may be required (Kasckow et al., 2011). The use of high doses is associated with a higher risk of developing AEs (Kasckow et al., 2011); however, many of clozapine's side‐effects can be detected, prevented, minimized, and treated (Meltzer, 2012). For example, when one considers the hematological AEs, it is estimated that one in 10,000 people treated with clozapine will die from agranulocytosis. Among patients at high risk of suicide, approximately one in 10–20 will die from suicide. Thus, the relative risk favors clozapine when comparing only the suicide risk with risk from agranulocytosis (Kasckow et al., 2011). The reduced suicide risk in most patients also outweighs the low risk (0.015–0.188%) of a serious adverse cardiac event (Merrill et al., 2005).
Psychiatric comorbidities such as depression and anxiety disorders can have a negative impact on outcomes. We recommend that psychiatric comorbidities be given high priority during treatment planning in the context of the socioeconomic and cultural background.
Theme 10: Medical comorbidities are common and should be monitored and addressed fastidiously in recent‐onset psychosis
Patients diagnosed with schizophrenia have an increased mortality rate compared with the general population (hazard ratio 2.05, 95% CI 2.01–2.09); around two thirds of this excess is associated with increased rates of cardiovascular risk factors, including obesity, smoking, diabetes, hypertension, and dyslipidemia (Nielsen et al., 2013). All SGAs are associated with weight gain compared with placebo treatment, although some (e.g. olanzapine, clozapine, and quetiapine) are more problematic than others (e.g. ziprasidone and aripiprazole) (Das et al., 2012); however, non‐pharmacological factors also contribute to obesity development in schizophrenia (Megna et al., 2011). Diet, exercise and CBT, alone or in combination, can improve physical health and reduce body weight in patients with schizophrenia (Das et al., 2012; Hjorth et al., 2014).
There is a significantly lower cardiovascular risk in early schizophrenia than in chronic schizophrenia, and both diabetes and prediabetes appear uncommon in the early stages, especially in never‐medicated (NM) patients (Mitchell et al., 2013). Meta‐analysis shows that in both NM and FE patients, the overall rate of metabolic syndrome (MetS) using standardized criteria is approximately 10% compared with 30–40% in medicated patients not in their first episode (Mitchell et al., 2013). Rates of MetS are high among medicated patients in Malaysia (46.7%), and those with MetS have a greater cardiovascular risk (Said et al., 2012). At least 40% of patients in South Korea exhibit MetS, with the greatest prevalence associated with the use of a combination of SGAs (Ko et al., 2013). Elsewhere, the rate of MetS among medicated patients has been estimated to be 46.0% in Singapore (Lee et al., 2012), 27.5% in Japan (Sugawara et al., 2010), 20.0% in Thailand (Srisurapanont et al., 2007), and 44–45% in India (Grover et al., 2012).
Psychiatrists should be conscious of the physical conditions and metabolic issues associated with the use of antipsychotic drugs and the potential for antipsychotic therapies to worsen existing conditions such as diabetes and compromised lipid metabolism. Strategies to improve health and well‐being should be promoted early on and all patients should be screened regularly for metabolic abnormalities.
Conclusions
Antipsychotics are effective in treating acute psychotic symptoms, particularly in patients with a recent onset of psychosis. However, in many cases outcomes remain far from satisfactory. Providing optimal care to recent‐onset psychosis patients can improve these outcomes and not only benefits the patient, but their families, friends, and society as a whole. The importance of optimal care in recent‐onset psychosis is well established, but clinical practice has yet to incorporate many of the more recent developments and there is a lack of consistency of approach across the A‐P region. We therefore developed a set of principles for clinicians across the region to use on a day‐to‐day basis throughout the patient journey. For instance, these principles could form the basis of a checklist of items to be discussed with patients and family members during initial consultations and at follow‐up appointments. These issues are dynamic and change over time. For instance, themes 1 and 2 are relevant for initial consultations, whereas substance abuse (theme 8), psychiatric (theme 9), and medical (theme 10) comorbidities will need to be revisited frequently. HCPs will need to review and reprioritize the issues at different stages of recovery, and adjust interventions appropriately. These principles could also be integrated into the initial training of junior HCPs and patient support group members.
Among the 10 themes, several common principles emerge: adherence to antipsychotic medications is crucial; substance abuse, psychiatric and medical comorbidities can and should be addressed; psychosocial interventions play a pivotal role in each of these areas; and family members can play a vital role in overall patient care. The application of the 10 themes and recommendations discussed in this expert consensus should help to raise awareness of the specific issues involved in the care of recent‐onset psychosis patients regardless of their socioeconomic and cultural backgrounds.
Limitations
The A‐P region is extremely diverse with different health care systems, levels of socioeconomic development and cultural attitudes, and we recognize that it is not possible to provide the same level of treatment throughout the region. We therefore focused primarily on general principles of care as a full analysis of treatment strategies within each country in the A‐P region was beyond the scope of this article. These recommendations should not be viewed as a comprehensive guide for treating schizophrenia. Our initial literature search was limited to articles published in the English language only however, non‐English articles were included after the initial review stage if appropriate.
Disclosures
TLL, TS, KS, MT, CL and RK have received honoraria for talks and consultancy from Janssen.
MW has received honoraria for talks and consultancy from Janssen and Lundbeck.
YH has received honoraria for talks and consultancy from Janssen and Lundbeck; and is a current or past advisory board member for Janssen and Pfizer.
NA has received honoraria for talks and consultancy from Janssen; and is a current or past advisory board member for Lundbeck.
AH has received grant monies for research from Lundbeck; honoraria for talks and consultancy from Janssen, Lundbeck, Eli Lilly, and Servier Pharmaceutical; has been involved in designing and participating in clinical trials organized by Janssen, Lundbeck, Dainippon Sumitomo, and Servier Pharmaceutical; and is a current or past advisory board member for Mitsubishi Tanabe Pharmaceutical.
TB has received grant monies for research from Johnson and Johnson, and is a current or past advisory board member for Johnson and Johnson.
RE has received grant monies for research clinical trials from Janssen; honoraria for talks and consultancy from Janssen, Lundbeck, Otsuka, AstraZeneca, and Servier; and is a current or past advisory board member for Janssen, Lundbeck, Otsuka, and Servier.
JO has received grant monies for research, honoraria, and travel support for talks and consultancy from Janssen‐Cilag, Lilly, AstraZeneca, Pfizer, Lundbeck Glaxo, Novartis, and Bristol‐Myers Squibb; has been involved in designing and participating in clinical trials for Janssen‐Cilag, Lilly, AstraZeneca, Pfizer, Lundbeck, Glaxo and Bristol‐Myers Squibb; and is a current or past advisory board member for Janssen‐Cilag, Lilly, AstraZeneca and Bristol‐Myers Squibb.
YKY has received grant monies for research from GlaxoSmithKline, Eli Lilly, Pfizer, Janssen‐Cilag (J&J), Sanofi‐Aventis, Wyeth, Otsuka, Astellas, Dai Nippon Sumitomo, Atomic Energy Council, Lundbeck, and Roche; honoraria for talks and consultancy from AstraZeneca, GlaxoSmithKline, Eli Lilly, Pfizer, Janssen‐Cilag (J&J), Wyeth, Otsuka, Fujisawa (Astellas), Sanofi‐Aventis, Organon (Schering‐Plough) and Servier; and is a current or past advisory board member for Janssen‐Cilag (J&J), Pfizer, Eli Lilly and Lundbeck.
DC has received grant monies for research from Eli Lilly, Janssen Cilag, Roche, Allergen, Bristol‐Myers Squibb, Pfizer, Lundbeck, AstraZeneca, Hospira; travel support and honoraria for talks and consultancy from Eli Lilly, Bristol‐Myers Squibb, AstraZeneca, Lundbeck, Janssen Cilag, Pfizer, Organon, Sanofi‐Aventis, Wyeth, Hospira, Servier; and is a current or past advisory board member for Lundbeck, Pfizer, AstraZeneca, and Roche.
Acknowledgments
Medical writing support was provided by Huntsworth Health Singapore Ltd., funded by Janssen Asia‐Pacific. Janssen Asia‐Pacific provided logistical support during the initial stages of this project. The authors have not received any honoraria or payment to participate in this project and the views expressed here are theirs alone.
Janssen Asia‐Pacific did not have a role in study design; in the analysis, and interpretation of data; in the writing of the manuscript; and in the decision to submit the manuscript for publication.
TLL, RE, JO, and DC contributed to the literature search, study design, data analysis, and interpretation, manuscript development, and review. MW, YH, TS, SK, MT, NA, AH, TB, CL, YKY, and RK contributed to the study design, data analysis and interpretation, manuscript development and review.
The authors would like to thank Nakao Iwata for contributing to initial discussions during the early stages of the project.
Lo, T. L. , Warden, M. , He, Y. , Si, T. , Kalyanasundaram, S. , Thirunavukarasu, M. , Amir, N. , Hatim, A. , Bautista, T. , Lee, C. , Emsley, R. , Olivares, J. , Yang, Y. K. , Kongsakon, R. , and Castle, D. (2016) Recommendations for the optimal care of patients with recent‐onset psychosis in the Asia‐Pacific region. Asia‐Pacific Psychiatry, 8: 154–171. doi: 10.1111/appy.12234.
References
- Addington J., Case N., Saleem M.M., et al (2014) Substance use in clinical high risk for psychosis: a review of the literature. Early Interv Psychiatry. 8, 104–112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alvarez‐Jiménez M., Gleeson J.F., Cotton S., et al (2009) Predictors of adherence to cognitive‐behavioural therapy in first‐episode psychosis. Can J Psychiatry. 54, 710–718. [DOI] [PubMed] [Google Scholar]
- Alvarez‐Jimenez M., Priede A., Hetrick S.E., et al (2012) Risk factors for relapse following treatment for first episode psychosis: a systematic review and meta‐analysis of longitudinal studies. Schizophr Res. 139, 116–128. [DOI] [PubMed] [Google Scholar]
- Ando S., Yamaguchi S., Aoki Y., Thornicroft G. (2013) Review of mental‐health‐related stigma in Japan. Psychiatry Clin Neurosci. 67, 471–482. [DOI] [PubMed] [Google Scholar]
- Andreasen N.C., Carpenter W.T., Kane J.M., et al (2005) Remission in schizophrenia: proposed criteria and rationale for consensus. Am J Psychiatry. 162, 441–449. [DOI] [PubMed] [Google Scholar]
- Andreasen N.C., Liu D., Ziebell S., Vora A., Ho B.‐C. (2013) Relapse duration, treatment intensity, and brain tissue loss in schizophrenia: a prospective longitudinal MRI study. Am J Psychiatry. 170, 609–615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- APA (2004) Practice guideline for the treatment of patients with schizophrenia. [Cited 18 November 2015.] Available from URL: http://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/schizophrenia.pdf
- Armijo J., Méndez E., Morales R., et al (2013) Efficacy of community treatments for schizophrenia and other psychotic disorders: a literature review. Front Psychiatry. 4, 116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ascher‐Svanum H., Faries D.E., Zhu B., et al (2006) Medication adherence and long‐term functional outcomes in the treatment of schizophrenia in usual care. J Clin Psychiatry. 67, 453–460. [DOI] [PubMed] [Google Scholar]
- Austin S.F., Mors O., Secher R.G., et al (2013) Predictors of recovery in first episode psychosis: the OPUS cohort at 10 year follow‐up. Schizophr Res. 150, 163–168. [DOI] [PubMed] [Google Scholar]
- Awad A.G., Voruganti L.N.P. (2008) The burden of schizophrenia on caregivers: a review. Pharmacoeconomics. 26, 149–162. [DOI] [PubMed] [Google Scholar]
- Bachmann S., Bottmer C., Schroder J. (2008) One‐year outcome and its prediction in first‐episode schizophrenia – a naturalistic study. Psychopathology. 41, 115–123. [DOI] [PubMed] [Google Scholar]
- Baeza I., Graell M., Moreno D., et al (2009) Cannabis use in children and adolescents with first episode psychosis: influence on psychopathology and short‐term outcome (CAFEPS study). Schizophr Res. 113, 129–137. [DOI] [PubMed] [Google Scholar]
- Barrowclough C., Gregg L., Lobban F., Bucci S., Emsley R. (2015) The impact of cannabis use on clinical outcomes in recent onset psychosis. Schizophr Bull. 41, 382–390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Basu D., Sarkar S., Mattoo S.K. (2013) Psychiatric comorbidity in patients with substance use disorders attending an addiction treatment center in India over 11 years: case for a specialized “dual diagnosis clinic”. J Dual Diagn. 9, 23–29. [Google Scholar]
- Bechdolf A., Wagner M., Veith V., et al (2007) Randomized controlled multicentre trial of cognitive behaviour therapy in the early initial prodromal state: effects on social adjustment post treatment. Early Interv Psychiatry. 1, 71–78. [DOI] [PubMed] [Google Scholar]
- Boardman G., McCann T., Kerr D. (2014) A peer support programme for enhancing adherence to oral antipsychotic medication in consumers with schizophrenia. J Adv Nurs. 70, 2293–2302. [DOI] [PubMed] [Google Scholar]
- Bodén R., Brandt L., Kieler H., Andersen M., Reutfors J. (2011) Early non‐adherence to medication and other risk factors for rehospitalization in schizophrenia and schizoaffective disorder. Schizophr Res. 133, 36–41. [DOI] [PubMed] [Google Scholar]
- Bradley G.M., Couchman G.M., Perlesz A., et al (2006) Multiple‐family group treatment for English‐ and Vietnamese‐speaking families living with schizophrenia. Psychiatr Serv. 57, 521–530. [DOI] [PubMed] [Google Scholar]
- Buckley P.F., Miller B.J., Lehrer D.S., Castle D.J. (2009) Psychiatric comorbidities and schizophrenia. Schizophr Bull. 35, 383–402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caseiro O., Pérez‐Iglesias R., Mata I., et al (2012) Predicting relapse after a first episode of non‐affective psychosis: a three‐year follow‐up study. J Psychiatr Res. 46, 1099–1105. [DOI] [PubMed] [Google Scholar]
- Chakrabarti S. (2011) Family interventions in schizophrenia: issues of relevance for Asian countries. World J Psychiatry. 1, 4–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chan S.W. (2011) Global perspective of burden of family caregivers for persons with schizophrenia. Arch Psychiatr Nurs. 25, 339–349. [DOI] [PubMed] [Google Scholar]
- Chand P., Thirthalli J., Murthy P. (2014) Substance use disorders among treatment naïve first‐episode psychosis patients. Compr Psychiatry. 55, 165–169. [DOI] [PubMed] [Google Scholar]
- Chen E.Y., Tang J.Y., Chan S.K., et al (2012) Three‐year outcome of phase‐specific early intervention for first‐episode psychosis: a cohort study in Hong Kong. Hong Kong Med J. 18(Suppl 6), S7–S13. [PubMed] [Google Scholar]
- Chen M., Wu G., Wang Z., et al (2014) Two‐year prospective case‐controlled study of a case management program for community‐dwelling individuals with schizophrenia. Shanghai Arch Psychiatry. 26, 119–128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chien W.T., Chan S.W.C. (2013) The effectiveness of mutual support group intervention for Chinese families of people with schizophrenia: a randomised controlled trial with 24‐month follow‐up. Int J Nurs Stud. 50, 1326–1340. [DOI] [PubMed] [Google Scholar]
- Chien W.T., Thompson D.R. (2013) An RCT with three‐year follow‐up of peer support groups for Chinese families of persons with schizophrenia. Psychiatr Serv. 64, 997–1005. [DOI] [PubMed] [Google Scholar]
- Chien W.T., Wong K.F. (2007) A family psychoeducation group program for Chinese people with schizophrenia in Hong Kong. Psychiatr Serv. 58, 1003–1006. [DOI] [PubMed] [Google Scholar]
- Chong M.‐Y., Tan C.H., Fujii S., et al (2004) Antipsychotic drug prescription for schizophrenia in East Asia: rationale for change. Psychiatry Clin Neurosci. 58, 61–67. [DOI] [PubMed] [Google Scholar]
- Chung K.F., Chan J.H. (2004) Can a less pejorative Chinese translation for schizophrenia reduce stigma? A study of adolescents' attitudes toward people with schizophrenia. Psychiatry Clin Neurosci. 58, 507–515. [DOI] [PubMed] [Google Scholar]
- Citrome L. (2014) Unmet needs in the treatment of schizophrenia: new targets to help different symptom domains. J Clin Psychiatry. 75(Suppl 1), 21–26. [DOI] [PubMed] [Google Scholar]
- Coldham E.L., Addington J., Addington D. (2002) Medication adherence of individuals with a first episode of psychosis. Acta Psychiatr Scand. 106, 286–290. [DOI] [PubMed] [Google Scholar]
- Crespo‐Facorro B., Ortiz‐García de la Foz V., Mata I., et al (2013) Aripiprazole, Ziprasidone and Quetiapine in the treatment of first‐episode nonaffective psychosis: a 12‐week randomized, flexible‐dose, open‐label trial. Schizophr Res. 147, 375–382. [DOI] [PubMed] [Google Scholar]
- Dargan P.I., Wood D.M. (2012) Recreational drug use in the Asia Pacific region: improvement in our understanding of the problem through the UNODC programmes. J Med Toxicol. 8, 295–299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Das C., Mendez G., Jagasia S., Labbate L.A. (2012) Second‐generation antipsychotic use in schizophrenia and associated weight gain: a critical review and meta‐analysis of behavioral and pharmacologic treatments. Ann Clin Psychiatry. 24, 225–239. [PubMed] [Google Scholar]
- Dolder C.R., Lacro J.P., Leckband S., Jeste D.V. (2003) Interventions to improve antipsychotic medication adherence: review of recent literature. J Clin Psychopharmacol. 23, 389–399. [DOI] [PubMed] [Google Scholar]
- Durmaz H., Okanlı A. (2014) Investigation of the effect of self‐efficacy levels of caregiver family members of the individuals with schizophrenia on burden of care. Arch Psychiatr Nurs. 28, 290–294. [DOI] [PubMed] [Google Scholar]
- Emsley R., Medori R., Koen L., et al (2008) Long‐acting injectable risperidone in the treatment of subjects with recent‐onset psychosis: a preliminary study. J Clin Psychopharmacol. 28, 210–213. [DOI] [PubMed] [Google Scholar]
- Emsley R., Oosthuizen P.P., Koen L., Niehaus D.J.H., Martinez G. (2012) Symptom recurrence following intermittent treatment in first‐episode schizophrenia successfully treated for 2 years: a 3‐year open‐label clinical study. J Clin Psychiatry. 73, e541–e547. [DOI] [PubMed] [Google Scholar]
- Emsley R., Chiliza B., Asmal L., Harvey B.H. (2013) The nature of relapse in schizophrenia. BMC Psychiatry. 13, 50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fanning F., Foley S., Lawlor E., et al (2012) Group cognitive behavioural therapy for first episode psychosis: who's referred, who attends and who completes it? Early Interv Psychiatry. 6, 432–441. [DOI] [PubMed] [Google Scholar]
- Faridi K., Joober R., Malla A. (2012) Medication adherence mediates the impact of sustained cannabis use on symptom levels in first‐episode psychosis. Schizophr Res. 141, 78–82. [DOI] [PubMed] [Google Scholar]
- Fervaha G., Foussias G., Agid O., Remington G. (2014) Motivational and neurocognitive deficits are central to the prediction of longitudinal functional outcome in schizophrenia. Acta Psychiatr Scand. 130, 290–299. [DOI] [PubMed] [Google Scholar]
- Fraguas D., Llorente C., Rapado‐Castro M., et al (2008) Attitude toward antipsychotic medication as a predictor of antipsychotic treatment discontinuation in first‐episode early‐onset psychosis. Rev Psiquiatr Salud Ment. 1, 10–17. [DOI] [PubMed] [Google Scholar]
- Fraguas D., Del Rey‐Mejías A., Moreno C., et al (2014) Duration of untreated psychosis predicts functional and clinical outcome in children and adolescents with first‐episode psychosis: a 2‐year longitudinal study. Schizophr Res. 152, 130–138. [DOI] [PubMed] [Google Scholar]
- Gaebel W., Riesbeck M. (2014) Are there clinically useful predictors and early warning signs for pending relapse? Schizophr Res. 152, 469–477. [DOI] [PubMed] [Google Scholar]
- Gafoor R., Landau S., Craig T.K.J., et al (2010) Esquire trial: efficacy and adverse effects of quetiapine versus risperidone in first‐episode schizophrenia. J Clin Psychopharmacol. 30, 600–606. [DOI] [PubMed] [Google Scholar]
- Gearing R.E., Mian I., Sholonsky A., et al (2009) Developing a risk‐model of time to first‐relapse for children and adolescents with a psychotic disorder. J Nerv Ment Dis. 197, 6–14. [DOI] [PubMed] [Google Scholar]
- Glick I.D., Correll C.U., Altamura A.C., et al (2011) Mid‐term and long‐term efficacy and effectiveness of antipsychotic medications for schizophrenia: a data‐driven, personalized clinical approach. J Clin Psychiatry. 72, 1616–1627. [DOI] [PubMed] [Google Scholar]
- Grover S., Aggarwal M., Dutt A., et al (2012) Prevalence of metabolic syndrome in patients with schizophrenia in India. Psychiatry Res. 200, 1035–1037. [DOI] [PubMed] [Google Scholar]
- Gutiérrez‐Maldonado J., Caqueo‐Urízar A., Kavanagh D.J. (2005) Burden of care and general health in families of patients with schizophrenia. Soc Psychiatry Psychiatr Epidemiol. 40, 899–904. [DOI] [PubMed] [Google Scholar]
- Hartz S.M., Pato C.N., Medeiros H., et al (2014) Comorbidity of severe psychotic disorders with measures of substance use. JAMA Psychiatry. 71, 248–254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hassan G.A.M., Taha G.R.A. (2011) Long term functioning in early onset psychosis: two years prospective follow‐up study. Behav Brain Funct. 7, 28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Henry L.P., Amminger G.P., Harris M.G., et al (2010) The EPPIC follow‐up study of first‐episode psychosis: longer‐term clinical and functional outcome 7 years after index admission. J Clin Psychiatry. 71, 716–728. [DOI] [PubMed] [Google Scholar]
- Hjorth P., Davidsen A.S., Kilian R., Skrubbeltrang C. (2014) A systematic review of controlled interventions to reduce overweight and obesity in people with schizophrenia. Acta Psychiatr Scand. 130, 279–289. [DOI] [PubMed] [Google Scholar]
- Hui C.L.‐M., Tang J.Y.‐M., Leung C.‐M., et al (2013) A 3‐year retrospective cohort study of predictors of relapse in first‐episode psychosis in Hong Kong. Aust N Z J Psychiatry. 47, 746–753. [DOI] [PubMed] [Google Scholar]
- Jorm A.F., Morgan A.J., Wright A. (2008) A comparison of clinician, youth, and parent beliefs about helpfulness of interventions for early psychosis. Psychiatr Serv. 59, 1115–1120. [DOI] [PubMed] [Google Scholar]
- Kaewprom C., Curtis J., Deane F.P. (2011) Factors involved in recovery from schizophrenia: a qualitative study of Thai mental health nurses. Nurs Health Sci. 13, 323–327. [DOI] [PubMed] [Google Scholar]
- Kasckow J., Felmet K., Zisook S. (2011) Managing suicide risk in patients with schizophrenia. CNS Drugs. 25, 129–143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Killackey E., Jackson H.J., McGorry P.D. (2008) Vocational intervention in first‐episode psychosis: individual placement and support v. treatment as usual. Br J Psychiatry. 193, 114–120. [DOI] [PubMed] [Google Scholar]
- Kim B., Lee S.‐H., Choi T.K., et al (2008) Effectiveness of risperidone long‐acting injection in first‐episode schizophrenia: in naturalistic setting. Prog Neuropsychopharmacol Biol Psychiatry. 32, 1231–1235. [DOI] [PubMed] [Google Scholar]
- Kim B., Lee S.‐H., Yang Y.K., Park J.‐I., Chung Y.‐C. (2012) Long‐acting injectable antipsychotics for first‐episode schizophrenia: the pros and cons. Schizophr Res Treatment. 2012, 560836. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim S.‐W., Lee Y.‐H., Jang J.‐E., et al (2013) Comparison of attitudes toward long‐acting injectable antipsychotics among psychiatrists and patients. Int Clin Psychopharmacol. 28, 80–86. [DOI] [PubMed] [Google Scholar]
- Kin Wong K., Chiu R., Tang B., et al (2008) A randomized controlled trial of a supported employment program for persons with long‐term mental illness in Hong Kong. Psychiatr Serv. 59, 84–90. [DOI] [PubMed] [Google Scholar]
- Kishimoto T., Agarwal V., Kishi T., et al (2013a) Relapse prevention in schizophrenia: a systematic review and meta‐analysis of second‐generation antipsychotics versus first‐generation antipsychotics. Mol Psychiatry. 18, 53–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kishimoto T., Watanabe K., Uchida H., et al (2013b) Antipsychotic polypharmacy: a Japanese survey of prescribers' attitudes and rationales. Psychiatry Res. 209, 406–411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ko Y.‐K., Soh M.‐A., Kang S.‐H., Lee J.‐I. (2013) The prevalence of metabolic syndrome in schizophrenic patients using antipsychotics. Clin Psychopharmacol Neurosci. 11, 80–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lambert M., Conus P., Cotton S., et al (2010) Prevalence, predictors, and consequences of long‐term refusal of antipsychotic treatment in first‐episode psychosis. J Clin Psychopharmacol. 30, 565–572. [DOI] [PubMed] [Google Scholar]
- Lasalvia A., Zoppei S., Bonetto C., et al (2014) The role of experienced and anticipated discrimination in the lives of people with first‐episode psychosis. Psychiatr Serv. 65, 1034–1040. [DOI] [PubMed] [Google Scholar]
- Lecomte T., Spidel A., Leclerc C., et al (2008) Predictors and profiles of treatment non‐adherence and engagement in services problems in early psychosis. Schizophr Res. 102, 295–302. [DOI] [PubMed] [Google Scholar]
- Lee J., Nurjono M., Wong A., Salim A. (2012) Prevalence of metabolic syndrome among patients with schizophrenia in Singapore. Ann Acad Med Singap. 41, 457–462. [PubMed] [Google Scholar]
- Lee Y.S., Park I.H., Park S.‐C., Kim J.‐J., Kwon J.S. (2014) Johyeonbyung (attunement disorder): renaming mind splitting disorder as a way to reduce stigma of patients with schizophrenia in Korea. Asian J Psychiatr. 8, 118–120. [DOI] [PubMed] [Google Scholar]
- Lehman A.F., Kreyenbuhl J., Buchanan R.W., et al (2004) The Schizophrenia Patient Outcomes Research Team (PORT): updated treatment recommendations 2003. Schizophr Bull. 30, 193–217. [DOI] [PubMed] [Google Scholar]
- Lincoln T.M., Wilhelm K., Nestoriuc Y. (2007) Effectiveness of psychoeducation for relapse, symptoms, knowledge, adherence and functioning in psychotic disorders: a meta‐analysis. Schizophr Res. 96, 232–245. [DOI] [PubMed] [Google Scholar]
- Lindenmayer J.‐P., Liu‐Seifert H., Kulkarni P.M., et al (2009) Medication nonadherence and treatment outcome in patients with schizophrenia or schizoaffective disorder with suboptimal prior response. J Clin Psychiatry. 70, 990–996. [DOI] [PubMed] [Google Scholar]
- Llorca P.M., Abbar M., Courtet P., et al (2013) Guidelines for the use and management of long‐acting injectable antipsychotics in serious mental illness. BMC Psychiatry. 13, 340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malla A., Tibbo P., Chue P., et al (2013) Long‐acting injectable antipsychotics: recommendations for clinicians. Can J Psychiatry. 58, 30S–35S. [DOI] [PubMed] [Google Scholar]
- Megna J.L., Schwartz T.L., Siddiqui U.A., Herrera Rojas M. (2011) Obesity in adults with serious and persistent mental illness: a review of postulated mechanisms and current interventions. Ann Clin Psychiatry. 23, 131–140. [PubMed] [Google Scholar]
- Meltzer H.Y. (2012) Clozapine: balancing safety with superior antipsychotic efficacy. Clin Schizophr Relat Psychoses. 6, 134–144. [DOI] [PubMed] [Google Scholar]
- Menezes N.M., Malla A.M., Norman R.M., et al (2009) A multi‐site Canadian perspective: examining the functional outcome from first‐episode psychosis. Acta Psychiatr Scand. 120, 138–146. [DOI] [PubMed] [Google Scholar]
- Merrill D.B., Dec G.W., Goff D.C. (2005) Adverse cardiac effects associated with clozapine. J Clin Psychopharmacol. 25, 32–41. [DOI] [PubMed] [Google Scholar]
- Mitchell A.J., Vancampfort D., De Herdt A., Yu W., De Hert M. (2013) Is the prevalence of metabolic syndrome and metabolic abnormalities increased in early schizophrenia? A comparative meta‐analysis of first episode, untreated and treated patients. Schizophr Bull. 39, 295–305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Montreuil T.C., Cassidy C.M., Rabinovitch M., et al (2012) Case manager‐ and patient‐rated alliance as a predictor of medication adherence in first‐episode psychosis. J Clin Psychopharmacol. 32, 465–469. [DOI] [PubMed] [Google Scholar]
- Morgan C., Lappin J., Heslin M., et al (2014) Reappraising the long‐term course and outcome of psychotic disorders: the AESOP‐10 study. Psychol Med. 44, 2713–2726. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mueser K.T., McGurk S.R. (2014) Supported employment for persons with serious mental illness: current status and future directions. Encephale. 40(Suppl 2), S45–S56. [DOI] [PubMed] [Google Scholar]
- Naeem F., Saeed S., Irfan M., et al (2015) Brief culturally adapted CBT for psychosis (CaCBTp): a randomized controlled trial from a low income country. Schizophr Res. 164, 143–148. [DOI] [PubMed] [Google Scholar]
- Nielsen R.E., Uggerby A.S., Jensen S.O.W., McGrath J.J. (2013) Increasing mortality gap for patients diagnosed with schizophrenia over the last three decades – a Danish nationwide study from 1980 to 2010. Schizophr Res. 146, 22–27. [DOI] [PubMed] [Google Scholar]
- van Nimwegen‐Campailla L., van Beveren N., Laan W., et al (2010) Effect of early dysphoric response and cannabis use on discontinuation of olanzapine or risperidone in patients with early psychosis. Pharmacopsychiatry. 43, 281. [DOI] [PubMed] [Google Scholar]
- NICE (2014) Psychosis and schizophrenia in adults: treatment and management. [Cited 18 November 2015.] Available from URL: http://www.nice.org.uk/Guidance/CG178
- Noguera A., Ballesta P., Baeza I., et al (2013) Twenty‐four months of antipsychotic treatment in children and adolescents with first psychotic episode: discontinuation and tolerability. J Clin Psychopharmacol. 33, 463–471. [DOI] [PubMed] [Google Scholar]
- Novick D., Haro J.M., Suarez D., et al (2010) Predictors and clinical consequences of non‐adherence with antipsychotic medication in the outpatient treatment of schizophrenia. Psychiatry Res. 176, 109–113. [DOI] [PubMed] [Google Scholar]
- Olivares J.M., Alptekin K., Azorin J.‐M., et al (2013) Psychiatrists' awareness of adherence to antipsychotic medication in patients with schizophrenia: results from a survey conducted across Europe, the Middle East, and Africa. Patient Prefer Adherence. 7, 121–132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Opjordsmoen S., Friis S., Melle I., et al (2010) A 2‐year follow‐up of involuntary admission's influence upon adherence and outcome in first‐episode psychosis. Acta Psychiatr Scand. 121, 371–376. [DOI] [PubMed] [Google Scholar]
- Ostman M., Kjellin L. (2002) Stigma by association: psychological factors in relatives of people with mental illness. Br J Psychiatry. 181, 494–498. [DOI] [PubMed] [Google Scholar]
- Park S.‐C., Lee M.‐S., Kang S.‐G., Lee S.‐H. (2014) Patterns of antipsychotic prescription to patients with schizophrenia in Korea: results from the health insurance review & assessment service‐national patient sample. J Korean Med Sci. 29, 719–728. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perkins D.O., Gu H., Weiden P.J., et al (2008) Predictors of treatment discontinuation and medication nonadherence in patients recovering from a first episode of schizophrenia, schizophreniform disorder, or schizoaffective disorder: a randomized, double‐blind, flexible‐dose, multicenter study. J Clin Psychiatry. 69, 106–113. [DOI] [PubMed] [Google Scholar]
- Rabinowitz J., Levine S.Z., Häfner H. (2006) A population based elaboration of the role of age of onset on the course of schizophrenia. Schizophr Res. 88, 96–101. [DOI] [PubMed] [Google Scholar]
- Razali S.M., Ismail Z. (2014) Public stigma towards patients with schizophrenia of ethnic Malay: a comparison between the general public and patients' relatives. J Ment Health. 23, 176–180. [DOI] [PubMed] [Google Scholar]
- Remington G., Agid O., Foussias G., et al (2013) Clozapine's role in the treatment of first‐episode schizophrenia. Am J Psychiatry. 170, 146–151. [DOI] [PubMed] [Google Scholar]
- Ren Z., Wang H., Feng B., et al (2014) A cross‐sectional study on perception of stigma by Chinese schizophrenia patients. Neuropsychiatr Dis Treat. 10, 535–540. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- Rizos E.N., Michalopoulou P.G., Siafakas N., et al (2010) Association of serum brain‐derived neurotrophic factor and duration of untreated psychosis in first‐episode patients with schizophrenia. Neuropsychobiology. 62, 87–90. [DOI] [PubMed] [Google Scholar]
- Rodrigo C., Welgama S., Gunawardana A., et al (2010) A retrospective analysis of cannabis use in a cohort of mentally ill patients in Sri Lanka and its implications on policy development. Subst Abuse Treat Prev Policy. 5, 16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Said M.A., Sulaiman A.H., Habil M.H., et al (2012) Metabolic syndrome and cardiovascular risk among patients with schizophrenia receiving antipsychotics in Malaysia. Singapore Med J. 53, 801–807. [PubMed] [Google Scholar]
- San L., Arranz B., Perez V., et al (2012) One‐year, randomized, open trial comparing olanzapine, quetiapine, risperidone and ziprasidone effectiveness in antipsychotic‐naive patients with a first‐episode psychosis. Psychiatry Res. 200, 693–701. [DOI] [PubMed] [Google Scholar]
- Sanz‐Fuentenebro J., Taboada D., Palomo T., et al (2013) Randomized trial of clozapine vs. risperidone in treatment‐naïve first‐episode schizophrenia: results after one year. Schizophr Res. 149, 156–161. [DOI] [PubMed] [Google Scholar]
- Sartorius N., Chiu H., Heok K.E., et al (2014) Name change for schizophrenia. Schizophr Bull. 40, 255–258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sato M. (2008) Influence of the Japanese name change for schizophrenia]. Seishin Shinkeigaku Zasshi. 110, 849–854. [PubMed] [Google Scholar]
- Sato S., Iwata K., Furukawa S.‐I., et al (2013) The effects of the combination of cognitive training and supported employment on improving clinical and working outcomes for people with schizophrenia in Japan. Clin Pract Epidemiol Ment Health. 10, 18–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schimmelmann B.G., Mehler‐Wex C., Lambert M., et al (2007) A prospective 12‐week study of quetiapine in adolescents with schizophrenia spectrum disorders. J Child Adolesc Psychopharmacol. 17, 768–778. [DOI] [PubMed] [Google Scholar]
- Selvendra A., Baetens D., Trauer T., Petrakis M., Castle D. (2014) First episode psychosis in an adult area mental health service‐a closer look at early and late‐onset first episode psychosis. Australas Psychiatry. 22, 235–241. [DOI] [PubMed] [Google Scholar]
- Shinfuku N., Tan C.‐H. (2008) Pharmacotherapy for schizophrenic inpatients in East Asia – changes and challenges. Int Rev Psychiatry. 20, 460–468. [DOI] [PubMed] [Google Scholar]
- Shoib S., Mushtaq R., Dar M., et al (2014) Psychosocial and medical factors affecting treatment compliance in patients attending psychiatric hospital: a study from Kashmir. Int J Basic Clin Pharmacol. 3, 220. [Google Scholar]
- Shrivastava A., Johnston M., Terpstra K., Stitt L., Shah N. (2012) Atypical antipsychotics usage in long‐term follow‐up of first episode schizophrenia. Indian J Psychiatry. 54, 248–252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sim K., Su A., Ungvari G.S., et al (2004) Depot antipsychotic use in schizophrenia: an East Asian perspective. Hum Psychopharmacol. 19, 103–109. [DOI] [PubMed] [Google Scholar]
- Siu B.W.M., Ng B.F.L., Li V.C.K., et al (2012) Mental health recovery for psychiatric inpatient services: perceived importance of the elements of recovery. East Asian Arch Psychiatry. 22, 39–48. [PubMed] [Google Scholar]
- Srisurapanont M., Likhitsathian S., Boonyanaruthee V., Charnsilp C., Jarusuraisin N. (2007) Metabolic syndrome in Thai schizophrenic patients: a naturalistic one‐year follow‐up study. BMC Psychiatry. 7, 14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steger K.A., Cassidy C., Rabinovitch M., Joober R., Malla A. (2012) Impact of symptom resolution on medication adherence in first episode psychosis. Psychiatry Res. 196, 45–51. [DOI] [PubMed] [Google Scholar]
- Stewart K.D. (2013) Factors contributing to engagement during the initial stages of treatment for psychosis. Qual Health Res. 23, 336–347. [DOI] [PubMed] [Google Scholar]
- Subotnik K.L., Nuechterlein K.H., Ventura J., et al (2011) Risperidone nonadherence and return of positive symptoms in the early course of schizophrenia. Am J Psychiatry. 168, 286–292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sugawara N., Yasui‐Furukori N., Sato Y., et al (2010) Prevalence of metabolic syndrome among patients with schizophrenia in Japan. Schizophr Res. 123, 244–250. [DOI] [PubMed] [Google Scholar]
- Tan C.‐H., Shinfuku N., Sim K. (2008) Psychotropic prescription practices in East Asia: looking back and peering ahead. Curr Opin Psychiatry. 21, 645–650. [DOI] [PubMed] [Google Scholar]
- Tang J.Y.‐M., Chang W.‐C., Hui C.L.‐M., et al (2014) Prospective relationship between duration of untreated psychosis and 13‐year clinical outcome: a first‐episode psychosis study. Schizophr Res. 153, 1–8. [DOI] [PubMed] [Google Scholar]
- Taylor M., Ng K.Y.B. (2013) Should long‐acting (depot) antipsychotics be used in early schizophrenia? A systematic review. Aust N Z J Psychiatry. 47, 624–630. [DOI] [PubMed] [Google Scholar]
- Tharani A.J., Farooq S., Saleem F., Naveed A. (2013) Compliance to antipsychotic medication: a challenge for client, family and health care providers. J Pak Med Assoc. 63, 516–518. [PubMed] [Google Scholar]
- Tiihonen J., Haukka J., Taylor M., et al (2011) A nationwide cohort study of oral and depot antipsychotics after first hospitalization for schizophrenia. Am J Psychiatry. 168, 603–609. [DOI] [PubMed] [Google Scholar]
- Tse S., Davidson L., Chung K., Ng K.L., Yu C.H. (2014) Differences and similarities between functional and personal recovery in an Asian population: a cluster analytic approach. Psychiatry. 77, 41–56. [DOI] [PubMed] [Google Scholar]
- Tunis S.L., Faries D.E., Stensland M.D., Hay D.P., Kinon B.J. (2007) An examination of factors affecting persistence with initial antipsychotic treatment in patients with schizophrenia. Curr Med Res Opin. 23, 97–104. [DOI] [PubMed] [Google Scholar]
- Turkington A., Mulholland C.C., Rushe T.M., et al (2009) Impact of persistent substance misuse on 1‐year outcome in first‐episode psychosis. Br J Psychiatry. 195, 242–248. [DOI] [PubMed] [Google Scholar]
- Uzenoff S.R., Perkins D.O., Hamer R.M., Wiesen C.A., Penn D.L. (2008) A preliminary trial of adherence‐coping‐education (ACE) therapy for early psychosis. J Nerv Ment Dis. 196, 572–575. [DOI] [PubMed] [Google Scholar]
- Üçok A., Serbest S., Kandemir P.E. (2011) Remission after first‐episode schizophrenia: results of a long‐term follow‐up. Psychiatry Res. 189, 33–37. [DOI] [PubMed] [Google Scholar]
- Verma S., Subramaniam M., Abdin E., Poon L.Y., Chong S.A. (2012) Symptomatic and functional remission in patients with first‐episode psychosis. Acta Psychiatr Scand. 126, 282–289. [DOI] [PubMed] [Google Scholar]
- Viala A., Cornic F., Vacheron M.‐N. (2012) Treatment adherence with early prescription of long‐acting injectable antipsychotics in recent‐onset schizophrenia. Schizophr Res Treatment. 2012, 368687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weiden P.J., Schooler N.R., Weedon J.C., et al (2009) A randomized controlled trial of long‐acting injectable risperidone vs continuation on oral atypical antipsychotics for first‐episode schizophrenia patients: initial adherence outcome. J Clin Psychiatry. 70, 1397–1406. [DOI] [PubMed] [Google Scholar]
- Wunderink L., Nienhuis F.J., Sytema S., et al (2007) Guided discontinuation versus maintenance treatment in remitted first‐episode psychosis: relapse rates and functional outcome. J Clin Psychiatry. 68, 654–661. [DOI] [PubMed] [Google Scholar]
- Wunderink L., Nieboer R.M., Wiersma D., Sytema S., Nienhuis F.J. (2013) Recovery in remitted first‐episode psychosis at 7 years of follow‐up of an early dose reduction/discontinuation or maintenance treatment strategy: long‐term follow‐up of a 2‐year randomized clinical trial. JAMA Psychiatry. 70, 913–920. [DOI] [PubMed] [Google Scholar]
- Yoon C.K., Aziz S.A. (2014) A review of schizophrenia research in Malaysia. Med J Malaysia. 69, 46–53. [PubMed] [Google Scholar]
- Zaytseva Y., Gurovich I.Y., Shmukler A. (2010) Effectiveness of the integrated long‐term program of management of patients after first psychotic episode in 5‐year follow‐up. Psychiatr Danub. 22(Suppl 1), S92–S94. [PubMed] [Google Scholar]
- Zhang J.‐P., Gallego J.A., Robinson D.G., et al (2013a) Efficacy and safety of individual second‐generation vs. first‐generation antipsychotics in first‐episode psychosis: a systematic review and meta‐analysis. Int J Neuropsychopharmacol. 16, 1205–1218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang W., Li X., Lin Y., et al (2013b) Pathways to psychiatric care in urban north China: a general hospital based study. Int J Ment Health Syst. 7, 22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ziermans T.B., Schothorst P.F., Schnack H.G., et al (2012) Progressive structural brain changes during development of psychosis. Schizophr Bull. 38, 519–530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zipursky R.B., Menezes N.M., Streiner D.L. (2014) Risk of symptom recurrence with medication discontinuation in first‐episode psychosis: a systematic review. Schizophr Res. 152, 408–414. [DOI] [PubMed] [Google Scholar]