

Highlights
-
•
The management of medication-related osteonecrosis of the jaw (MRONJ) is controversial.
-
•
To date, there is no established treatment for cases of advanced stage 3 MRONJ osteoporosis in elderly patients.
-
•
We describe a case in which a pathological mandible fracture induced by MRONJ was healed and functional recovery of the occlusion was obtained by complete dentures after treatment with teriparatide.
Keywords: MRONJ, Teriparatide, Osteoporosis, Elderly
Abstract
Introduction
The management of medication-related osteonecrosis of the jaw (MRONJ) is controversial. To date, there is no established treatment for cases of advanced stage 3 MRONJ osteoporosis in elderly patients.
Presentation
An 87-year-old osteoporotic woman with osteonecrosis-induced left mandible fracture related to minodronate therapy was referred to us for treatment. She had a vertebral compression fracture concurrently and had started subcutaneous injection of teriparatide. After 18 months of treatment with teriparatide the pathological mandible fracture was healed and functional recovery of the occlusion was obtained by complete dentures.
Discussion
Teriparatide may have a powerful anabolic effect on bone, and promote bone regeneration against pathologic mandible fracture induced by MRONJ.
Conclusion
Based upon these findings, teriparatide might be beneficial for advanced stage 3 MRONJ osteoporosis in elderly patients.
1. Introduction
Since bisphosphonate-related osteonecrosis of the jaw (BRONJ) was first reported [1], numerous cases have been identified [2]. The American Association of Oral and Maxillofacial surgery (AAOMS) updated their position paper on BRONJ in 2014, in which the term BRONJ was replaced with “medication-related osteonecrosis of the jaw” (MRONJ) [3]. Management of advanced MRONJ is both challenging and controversial. An AAOMS position paper described that these patients benefit from debridement, including resection, in combination with antibiotic therapy, which can offer long-term palliation with resolution of acute infection and pain. Symptomatic patients with stage 3 disease may require resection and immediate reconstruction. However, there is occasionally a case in which mandilectomy is not indicated because of age and primary illness.
Teriparatide (recombinant human PTH 1–34) is an osteoanabolic agent which induces bone formation [4], and is approved for the treatment of postmenopausal osteoporosis, male osteoporosis and glucocorticoid-induced osteoporosis. Administration of teriparatide for the treatment of MRONJ resistant to conventional treatment was first introduced by Harper and Fung [5]. Subsequently, several case reports have disclosed favorable therapeutic outcomes from teriparatide in MRONJ [6], [7], [8]. We report here an 87-year-old osteoporotic woman with an MRONJ-induced mandible fracture that was successfully treated with teriparatide.
2. Case presentation
An 87-year-old woman with a 2-year history of minodronic acid hydrate (50 mg/4 w orally) for the treatment of osteoporosis was referred to us in 2013 for treatment of a pathological mandibular fracture. She had undergone extraction of the left mandibular first molar 5 months earlier, and underwent oral irrigation for the intraoral fistula at another hospital. She had an incomplete occlusion of the denture, and movement of the mandible bony fragment. The infection of the soft tissue and mandible had extended to the inferior border of the left mandible and emerged as an extraoral fistula (Fig. 1). Computed tomography revealed osteolysis extending to the inferior border resulting in a pathological fracture of the left mandible (Fig. 2). A biopsy was done and the histology revealed chronic inflammation and sequestrum. She was diagnosed with stage 3 BRONJ. She had a vertebral compression fracture concurrently and had started subcutaneous injection of teriparatide (56.5 μg/week) 1 month earlier. After discussion with the family physician, teriparatide treatment was continued and conservative treatment including amoxicillin hydrate administration (750 mg/d) initiated. Six months after the initiation of teriparatide therapy, bone sequestration of the left mandible had occurred, and the patient was receiving intraoral sequestrectomy under local anesthesia. After 7 months of the treatment, her symptoms had resolved and the intraoral and extraoral fistula had been converted to normal mucosa and skin respectively; therefore, administration of the antibiotic was discontinued. After 18 months of treatment with teriparatide, computed tomography showed significant bone regeneration and recovery of the mandible bone continuity (Fig. 3). Thereafter, she obtained functional recovery of the occlusion by complete dentures (Fig. 4).
Fig. 1.

Extraoral view showing left submandibular extraoral fistula.
Fig. 2.
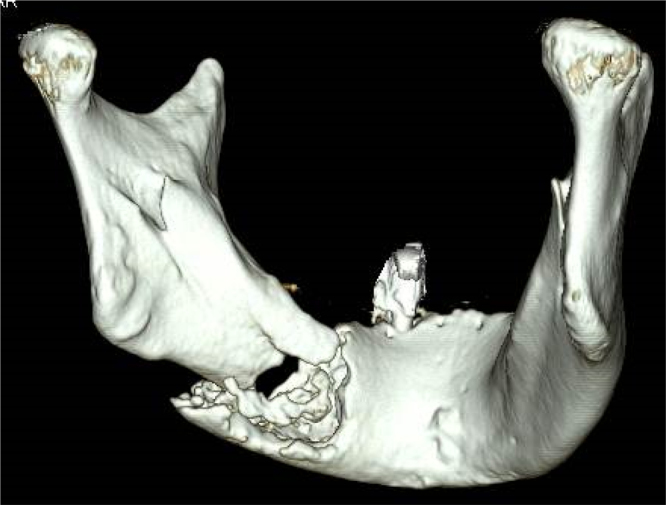
Computed tomography at the first medical examination.
Fig. 3.

Computed tomography after 18 months of teriparatide treatment.
Fig. 4.

Extraoral view after 18 months of teriparatide treatment.
3. Discussion
Teriparatide has been approved for osteoporosis management [9]. In addition to its effect on osteoporosis of increasing bone mineral density and bone strength, it has the potential to allow correction of unstable vertebral fractures without surgical intervention [10], and it promotes typical femoral fracture healing after long-term bisphosphonate administration [11]. Teriparatid is able to reverse the anti-resorptive effect of bisphosphonates. It has been shown to stimulate the activity and viability of osteoblasts from the alveolar bone of chronic bisphosphonate users [12], while indirectly increasing the metabolic activity and number of osteoclasts by affecting osteoblast function [13]. Therefore, teriparatide therapy has the effect of improving bone formation and modulating bone resorption at bisphosphonate therapy-induced pathological fractured sites of the mandible. In this case, mobile bone sequester was revealed 6 months after the teriparatide therapy was initiated. These results suggested that teriparatide can effectively enhance bone remodeling and separate the bone sequester for up to 6 months.
Successful cases of surgical resection of the mandible were reported by Carson and Basile in 2009 [14]. Recently, resection of MRONJ produced healing in patients taking oral bisphosphonate more successfully than conservative management [15]. However, aggressive resection of the jaw creates a difficult problem of delayed soft tissue coverage because osteoporosis patients are usually elderly and their wound-healing ability impaired. Elderly persons especially, i.e., those more than 80 years, have a characteristic decrease in body functions and various kinds of coexistent underlying disease. Therefore, when complications occur once, there is the risk that a vital organ will fall into malfunction in a chain reaction, and particularly careful operative adaptation and perioperative care are required.
In conclusion, teriparatide therapy can provide an important treatment option for advanced MRONJ stage 3 osteoporosis in elderly patients.
Conflict of interest
None.
Source of funding
None.
Ethical approval
N/A.
Consent
Informed consent was taken.
Author contribution
Tsuyoshi Shimo and Mayumi Yao contributed to data and writing. Yuko Ono, Kyoichi Obata, Norie Yoshioka, and Akira Sasaki contributed to data collectio`ns.
Guarantor
N/A.
References
- 1.Marx R.E. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic. J. Oral Maxillofac. Surg. 2003;61:1115–1117. doi: 10.1016/s0278-2391(03)00720-1. [DOI] [PubMed] [Google Scholar]
- 2.Fliefel R., Troltzsch M., Kuhnisch J., Ehrenfeld M., Otto S. Treatment strategies and outcomes of bisphosphonate-related osteonecrosis of the jaw (BRONJ) with characterization of patients: a systematic review. Int. J. Oral Maxillofac. Surg. 2015;44:568–585. doi: 10.1016/j.ijom.2015.01.026. [DOI] [PubMed] [Google Scholar]
- 3.Ruggiero S.L., Dodson T.B., Fantasia J., Goodday R., Aghaloo T., Mehrotra B. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw-2014 update. J. Oral Maxillofac. Surg. 2014;72:1938–1956. doi: 10.1016/j.joms.2014.04.031. [DOI] [PubMed] [Google Scholar]
- 4.Jiang Y., Zhao J.J., Mitlak B.H., Wang O., Genant H.K., Eriksen E.F. Recombinant human parathyroid hormone (1–34) [teriparatide] improves both cortical and cancellous bone structure. J. Bone Miner. Res. 2003;18:1932–1941. doi: 10.1359/jbmr.2003.18.11.1932. [DOI] [PubMed] [Google Scholar]
- 5.Harper R.P., Fung E. Resolution of bisphosphonate-associated osteonecrosis of the mandible: possible application for intermittent low-dose parathyroid hormone [rhPTH(1–34)] J. Oral Maxillofac. Surg. 2007;65:573–580. doi: 10.1016/j.joms.2006.10.076. [DOI] [PubMed] [Google Scholar]
- 6.Lee J.J., Cheng S.J., Jeng J.H., Chiang C.P., Lau H.P., Kok S.H. Successful treatment of advanced bisphosphonate-related osteonecrosis of the mandible with adjunctive teriparatide therapy. Head Neck. 2011;33:1366–1371. doi: 10.1002/hed.21380. [DOI] [PubMed] [Google Scholar]
- 7.Kim K.M., Park W., Oh S.Y., Kim H.J., Nam W., Lim S.K. Distinctive role of 6-month teriparatide treatment on intractable bisphosphonate-related osteonecrosis of the jaw. Osteoporos. Int. 2014;25:1625–1632. doi: 10.1007/s00198-014-2622-8. [DOI] [PubMed] [Google Scholar]
- 8.Yamachika E., Matsubara M., Ikeda A., Matsumura T., Moritani N., Iida S. Treatment of osteonecrosis of the jaw. J. Craniofac. Surg. 2015;26:e575–577. doi: 10.1097/SCS.0000000000002127. [DOI] [PubMed] [Google Scholar]
- 9.Lim S.Y., Bolster M.B. Current approaches to osteoporosis treatment. Curr. Opin. Rheumatol. 2015;27:216–224. doi: 10.1097/BOR.0000000000000169. [DOI] [PubMed] [Google Scholar]
- 10.Miyakoshi N., Horikawa A., Shimada Y. Nonsurgical corrective union of osteoporotic vertebral fracture with once-weekly teriparatide. Case Rep. Orthop. 2015;2015:784360. doi: 10.1155/2015/784360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gomberg S.J., Wustrack R.L., Napoli N., Arnaud C.D., Black D.M. Teriparatide vitamin D, and calcium healed bilateral subtrochanteric stress fractures in a postmenopausal woman with a 13-year history of continuous alendronate therapy. J. Clin. Endocrinol. Metab. 2011;96:1627–1632. doi: 10.1210/jc.2010-2520. [DOI] [PubMed] [Google Scholar]
- 12.Rao M.V., Berk J., Almojaly S.A., Goodloe Iii S., Margarone Iii J., Sullivan M. Effects of platelet-derived growth factor, vitamin D and parathyroid hormone on osteoblasts derived from cancer patients on chronic bisphosphonate therapy. Int. J. Mol. Med. 2009;23:407–413. doi: 10.3892/ijmm_00000145. [DOI] [PubMed] [Google Scholar]
- 13.Charles J.F., Aliprantis A.O. Osteoclasts: more than ‘bone eaters’. Trends Mol. Med. 2014;20:449–459. doi: 10.1016/j.molmed.2014.06.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Carlson E.R., Basile J.D. The role of surgical resection in the management of bisphosphonate-related osteonecrosis of the jaws. J. Oral Maxillofac. Surg. 2009;67:85–95. doi: 10.1016/j.joms.2009.01.006. [DOI] [PubMed] [Google Scholar]
- 15.Silva L.F., Curra C., Munerato M.S., Deantoni C.C., Matsumoto M.A., Cardoso C.L. Surgical management of bisphosphonate-related osteonecrosis of the jaws: literature review. Oral Maxillofac. Surg. 2015 doi: 10.1007/s10006-015-0538-x. [DOI] [PubMed] [Google Scholar]