

Abstract
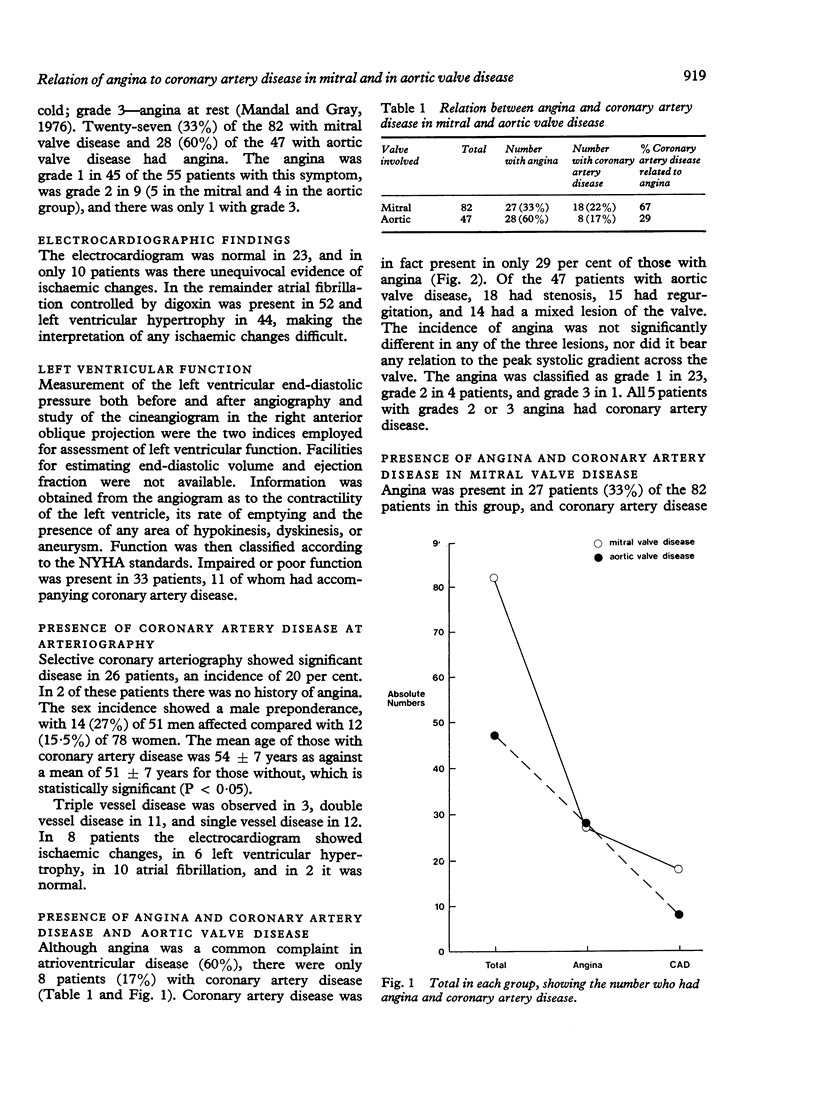
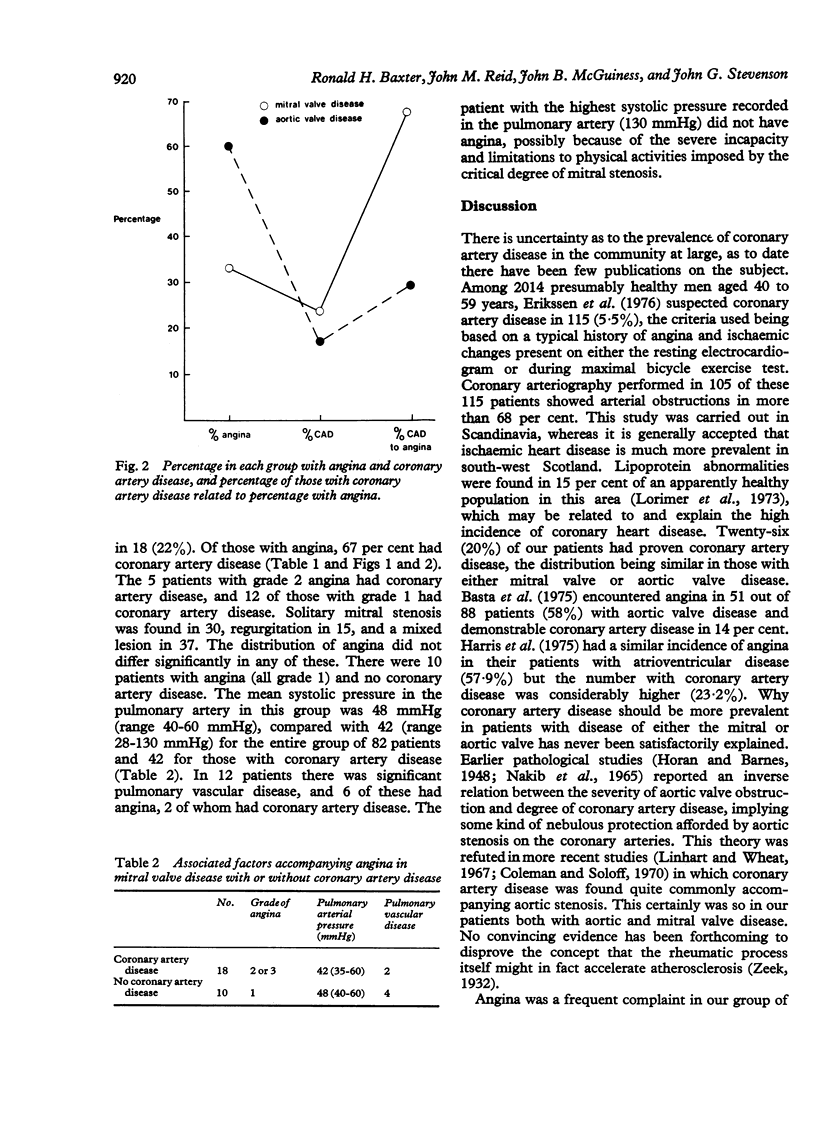
Of 129 patients with either mitral or aortic valve disease angina was present in 55 (42%). It was more frequent in aortic (60%) than in mitral valve disease (33%). The standard 12-lead electrocardiogram was not helpful in distinguishing underlying occlusive coronary artery disease. Coronary arteriography demonstrated coronary artery disease in 26 patients (20%), only 2 of whom had no angina. The incidence of coronary artery disease was almost identical in both the mitral and aortic groups (22% and 17%, respectively), but the percentage of those with demonstrable coronary artery disease accompanying angina was much higher in the mitral group (67% as against 29%). Angina in mitral valve disorders is thus much more likely to be the result of disease of the coronary arteries. Coronary arteriography is mandatory in all patients in both groups who have angina. Otherwise it seems unnecessary as coronary artery disease was found in only 2 patients who did not have angina.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Basta L. L., Raines D., Najjar S., Kioschos J. M. Clinical, haemodynamic, and coronary angiographic correlates of angina pectoris in patients with severe aortic valve disease. Br Heart J. 1975 Feb;37(2):150–157. doi: 10.1136/hrt.37.2.150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Benchimol A., Harris C. L., Desser K. B., Kwee B. T., Promisloff S. D. Resting electrocardiogram in major coronary artery disease. JAMA. 1973 Jun 11;224(11):1489–1492. [PubMed] [Google Scholar]
- Bodenheimer M. M., Banka V. S., Trout R. G., Pasdar H., Helfant R. H. Correlation of pathologic Q waves on the standard electrocardiogram and the epicardial electrogram of the human heart. Circulation. 1976 Aug;54(2):213–218. doi: 10.1161/01.cir.54.2.213. [DOI] [PubMed] [Google Scholar]
- Coleman E. H., Soloff L. A. Incidence of significant coronary artery disease in rheumatic valvular heart disease. Am J Cardiol. 1970 Apr;25(4):401–404. doi: 10.1016/0002-9149(70)90004-4. [DOI] [PubMed] [Google Scholar]
- Erikssen J., Enge I., Forfang K., Storstein O. False positive diagnostic tests and coronary angiographic findings in 105 presumably healthy males. Circulation. 1976 Sep;54(3):371–376. doi: 10.1161/01.cir.54.3.371. [DOI] [PubMed] [Google Scholar]
- Flowers N. C., Horan L. G., Sohi G. S., Hand R. C., Johnson J. C. New evidence for inferoposterior myocardial infarction on surface potential maps. Am J Cardiol. 1976 Nov 4;38(5):576–581. doi: 10.1016/s0002-9149(76)80005-7. [DOI] [PubMed] [Google Scholar]
- Friesingerg G. C., Smith R. F. Correlation of electrocardiographic studies and arteriographic findings with angina pectoris. Circulation. 1972 Dec;46(6):1173–1184. doi: 10.1161/01.cir.46.6.1173. [DOI] [PubMed] [Google Scholar]
- Gahl K., Sutton R., Pearson M., Caspari P., Lairet A., McDonald L. Mitral regurgitation in coronary heart disease. Br Heart J. 1977 Jan;39(1):13–18. doi: 10.1136/hrt.39.1.13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gray W., Corbin M., King J., Dunn M. Diagnostic value of vectorcardiogram in strictly posterior infarction. Br Heart J. 1972 Nov;34(11):1163–1169. doi: 10.1136/hrt.34.11.1163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harris C. N., Kaplan M. A., Parker D. P., Dunne E. F., Cowell H. S., Ellestad M. H. Aortic stenosis, angina, and coronary artery disease. Interrelations. Br Heart J. 1975 Jun;37(6):656–661. doi: 10.1136/hrt.37.6.656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Horan L. G., Flowers N. C., Johnson J. C. Significance of the diagnostic Q wave of myocardial infarction. Circulation. 1971 Mar;43(3):428–436. doi: 10.1161/01.cir.43.3.428. [DOI] [PubMed] [Google Scholar]
- Lorimer A. R., Hawthorne V. M., Morgan H. G., Lawrie T. D. Prevalence of lipoprotein abnormalities in the west of Scotland. Br Heart J. 1973 Aug;35(8):862–862. [PubMed] [Google Scholar]
- Mandal A. B., Gray I. R. Significance of angina pectoris in aortic valve stenosis. Br Heart J. 1976 Aug;38(8):811–815. doi: 10.1136/hrt.38.8.811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McConahay D. R., McCallister B. D., Hallermann F. J., Smith R. E. Comparative quantitative analysis of the electrocardiogram and the vectorcardiogram. Correlations with the coronary arteriogram. Circulation. 1970 Aug;42(2):245–259. doi: 10.1161/01.cir.42.2.245. [DOI] [PubMed] [Google Scholar]
- McGuinness J. B., Begg T. B., Semple T. First electrocardiogram in recent myocardial infarction. Br Med J. 1976 Aug 21;2(6033):449–451. doi: 10.1136/bmj.2.6033.449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murray R. G., Lorimer A. R., Dunn F. G., Macfarlane P. W., Hutton I., Lawrie T. D. Comparison of 12-lead and computer-analysed 3 orthogonal lead electocardiogram in coronary artery disease. Br Heart J. 1976 Aug;38(8):773–778. doi: 10.1136/hrt.38.8.773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nakib A., Lillehei C. W., Edwards J. E. The degree of coronary atherosclerosis in aortic valvular disease. Arch Pathol. 1965 Nov;80(5):517–520. [PubMed] [Google Scholar]
- Proudfit W. L., Shirey E. K., Sones F. M., Jr Selective cine coronary arteriography. Correlation with clinical findings in 1,000 patients. Circulation. 1966 Jun;33(6):901–910. doi: 10.1161/01.cir.33.6.901. [DOI] [PubMed] [Google Scholar]
- Resnekov L., Falicov R. E. Thyrotoxicosis and lactate-producing angina pectoris with normal coronary arteries. Br Heart J. 1977 Oct;39(10):1051–1057. doi: 10.1136/hrt.39.10.1051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- WOOD P., McGREGOR M., MAGIDSON O., WHITTAKER W. The effort test in angina pectoris. Br Heart J. 1950 Oct;12(4):363–371. doi: 10.1136/hrt.12.4.363. [DOI] [PMC free article] [PubMed] [Google Scholar]