

Abstract
In the past 15 years, the use of endoscopic evaluations in patients with obscure gastrointestinal bleeding has become more common. Indications for further endoscopic interventions include iron deficiency anemia, suspicion of Crohn’s disease or small-bowel tumors, assessment of celiac disease or of ulcers induced by nonsteroidal anti-inflammatory drugs, and screening for familial adenomatous polyposis. Often, capsule endoscopy is performed in concert with other endoscopic studies and can guide decisions regarding whether enteroscopy should be carried out in an anterograde or a retrograde approach. Retrograde endoscopy is beneficial in dealing with disease of the more distal small bowel. Multiple studies have examined the diagnostic yield of balloon-assisted deep enteroscopy and have estimated a diagnostic yield of 40% to 80%. Some of the studies have found that diagnostic yields are higher when capsule endoscopy is performed before balloon-assisted deep enteroscopy in a search for small-bowel bleeds. Each of these procedures has a role when performed alone; however, research suggests that they are especially effective as complementary techniques and together can provide better-directed therapy. Both procedures are relatively safe, with high diagnostic and therapeutic yields that allow evaluation of the small bowel. Because both interventions are relatively new to the world of gastroenterology, much research remains to be done regarding their overall efficacy, cost, and safety, as well as further indications for their use in the detection and treatment of diseases of the small bowel.
Keywords: Capsule endoscopy, balloon-assisted deep enteroscopy, obscure gastrointestinal bleeding, occult gastrointestinal bleeding
In the past 15 years, the use of endoscopic evaluations in patients with obscure gastrointestinal bleeding (OGIB) has become more common. A gastrointestinal (GI) bleed is considered to be obscure occult if the patient has a positive fecal occult blood test result or iron deficiency anemia without visible blood loss, whereas it is obscure overt if it persists without an obvious cause in a patient who has undergone upper GI endoscopy, colonoscopy, and small-bowel imaging.1 Patients with such presentations warrant further evaluation for both the diagnosis and treatment of their disease. Common indications for further endoscopic interventions include iron deficiency anemia, suspicion of Crohn’s disease or small-bowel tumors, assessment of celiac disease or of ulcer disease induced by nonsteroidal anti-inflammatory drugs, and screening for familial adenomatous polyposis and other familial polyposis syndromes.2-7
Capsule Endoscopy
The first capsule used to evaluate small-bowel bleeding was approved by the US Food and Drug Administration (FDA) in 2001. The subsequent generation, the PillCam (PillCam SB; Given Imaging), is now in its third form. The PillCam SB3 has improved resolution and can adapt the number of frames per second based on the rate of transit. In 2007, another small-bowel capsule, the EndoCapsule (Olympus America), was approved by the FDA. In a comparison study, the 2 devices demonstrated similar rates of detection of normal and abnormal features.8-10 A newer-generation capsule, the MiroCam capsule (IntroMedic), was approved by the FDA in 2013 and travels through the GI tract via electrical field propagation. The MiroCam capsule can acquire 3 images per second, whereas the PillCam can acquire 2 images per second, which are of a lower resolution than that of the MiroCam images. The MiroCam capsule has demonstrated diagnostic capabilities similar to those of the previously mentioned capsules.11 The OMOM capsule (Jinshan Science and Technology Group) is a newer capsule on the market. It has the ability to acquire 2 images per second with a 140-degree viewing angle. The CapsoCam SV1 capsule (CapsoVision) is another new capsule; it has the ability to store all of its images on a microchip and provides a 360-degree viewing angle with completely wire-free technology. This allows a patient who has a pacemaker or defibrillator to undergo capsule endoscopy without interference. In addition, the patient does not need to wear any external devices.12 A potential downside to this wireless capsule is that patients must retrieve it on their own at home with a special kit and then return the capsule to the physician for reading.
The Procedure
A video capsule endoscopy study is usually conducted in an outpatient setting. The patient will typically present to the doctor’s office after completing a modified bowel preparation the prior evening. Sensors are placed over the patient’s abdomen and connected to a mobile recording system. The capsule is activated, and then the patient swallows it with water. The patient can subsequently carry out his or her usual activities while wearing the equipment and can even eat a light meal several hours after the capsule has been swallowed. Later that same day, the equipment is removed, and the data are uploaded onto a computer system for interpretation and evaluation of pathology. There is no need for sedation, and the procedure is painless.
For patients with certain conditions, it may be necessary to place the capsule endoscopically. In particular, endoscopic placement should be considered for patients with dysphagia, gastroparesis, or abnormal upper GI anatomy. Furthermore, swallowing the capsule can some times be difficult for children and is not feasible in sedated patients who cannot protect their airway. As a result of these limitations, the FDA approved the AdvanCE capsule endoscopy delivery device (US Endoscopy) in 2007. A study from 2007 looked at 16 patients at a university hospital, ranging in age from 3 to 74 years, who were unable to swallow the capsule or who had altered upper GI anatomy or gastroparesis. The patients with altered upper GI anatomy had undergone a Billroth II procedure, Whipple surgery, or a bypass procedure. The study found that endoscopic placement of the PillCam SB video capsule with the AdvanCE delivery device was safe and easily performed in patients who otherwise would have had difficulty swallowing the capsule, and complete small- intestinal imaging was achieved.13 It should be noted that most children, patients with dysphagia, and patients with altered anatomy are often able to complete capsule study without the need for endoscopic placement.
Advantages and Disadvantages of Capsule Endoscopy
Capsule endoscopy has provided an additional diagnostic tool to evaluate obscure bleeds. The capsule traverses the entire mucosa, imaging most of the small bowel. Although there are advantages to this intervention, the inability to obtain tissue specimens for biopsy and administer treatment is a clear limitation. Studies have also demonstrated factors that predict decreased rates of detection with capsule endoscopy. Detection rates are decreased in patients who have previously undergone small-bowel surgery, who have a gastric transit time longer than 45 minutes or poor bowel cleansing, or who are hospitalized.14 Slow gastric transit times and poor preparation may indicate narcotic use, decreased mobility, or hospitalization. This shows the impact of inpatient vs outpatient studies and the propensity for inpatient cases to be more complex. Furthermore, approximately 1 in 6 capsules do not reach the cecum within recording time.15 Newer models provide a longer battery life and can overcome this limitation.
Factors Predicting the Likelihood of a Positive Study Result
The timing of a study has been found to be significant. A previous study showed that the source of bleeding was more likely to be identified in patients who had capsule endoscopy in the setting of active bleeding or recent bleeding than in those who had more distant bleeding.16 Moreover, a source of bleeding is less likely to be identified in patients evaluated for a positive fecal occult blood test result or for the workup of iron deficiency anemia. Specifically, one study noted that the diagnostic yield of capsule endoscopy for overt bleeding was 92%, whereas the yield for chronic iron deficiency anemia was 44%. Interestingly, other factors that predict a greater likelihood of a positive study result include male sex, older age, hospitalization, and a requirement for packed red blood cell transfusions.17 Another study, from 2013, found that the earlier a patient with OGIB underwent capsule endoscopy during a hospitalization, the more likely it was that the study would detect an active bleed. Importantly, capsule endoscopy also reduced the length of hospitalization by 40%. If the capsule was deployed more than 3 days after admission, the chance of identifying a source of bleeding was equal to that of an outpatient study.18
Order of Capsule Endoscopy and Push Enteroscopy
Often, capsule endoscopy is performed along with other endoscopic studies. Opinions vary regarding which order of the procedures results in the highest yield and if performing capsule endoscopy before mechanical endoscopy provides helpful information. A study from 2007 found that performing capsule endoscopy before push enteroscopy was more effective than performing push enteroscopy first, and that performing capsule endoscopy first decreased the need for push enteroscopy by approximately two-thirds. However, capsule endoscopy is not as sensitive in some parts of the GI tract, particularly the proximal duodenum, and enteroscopy is required if pathology is suspected in this area. Interestingly, however, at 1 year after treatment, the clinical outcomes of patients were similar regardless of whether they had undergone capsule endoscopy before push enteroscopy or push enteroscopy first with or without subsequent capsule endoscopy.19
Capsule Endoscopy in Obscure Gastrointestinal Bleeding and Other Conditions
The ability of video capsule endoscopy to detect the source of small-bowel bleeding has been studied in a variety of pathologic conditions. Most capsule endoscopy studies (70%-80%) are performed for obscure small-bowel bleeding (Figure 1).20 A review from 2013 looked at the rate of rebleeding in patients with a negative result of capsule endoscopy performed as part of an evaluation for OGIB.21 The authors looked at nearly 700 cases of patients who had OGIB that had been evaluated with capsule endoscopy. A source of bleeding was detected in 70% of the patients and was not detected in 30%. The patients were followed for 2 years, and it was found that only 16% of the patients with negative studies had subsequent bleeding. This shows the ability to defer further invasive procedures after a negative result of capsule endoscopy in most cases as well as the high negative predictive value of negative capsule endoscopy results.
Figure 1.
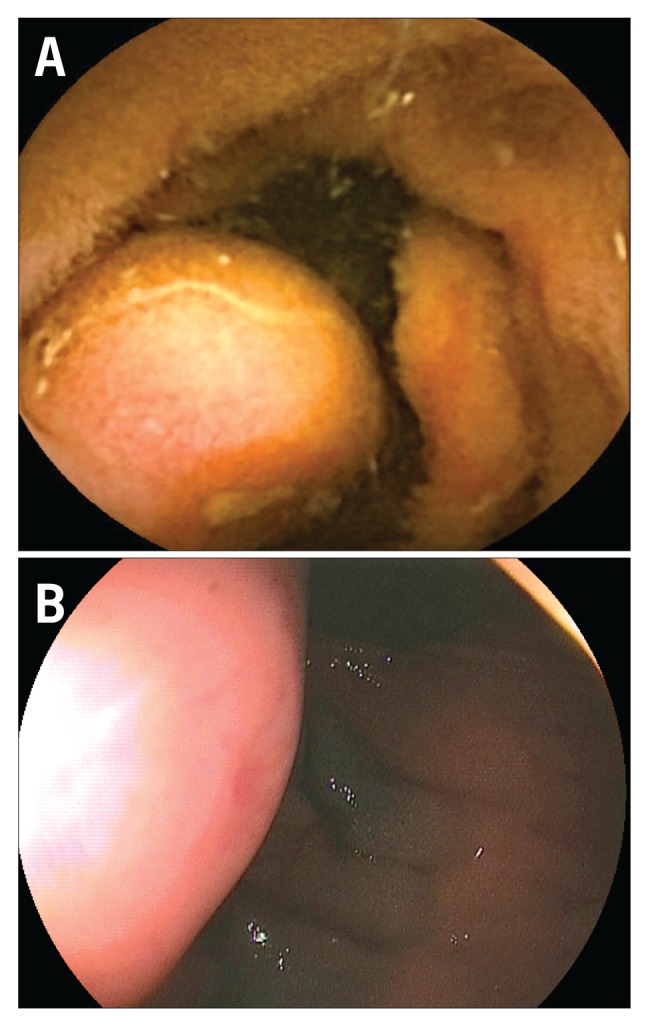
Obscure jejunal bleeding noted on a capsule endoscopy in a 63-year-old man (A). A double-balloon enteroscopy revealed the source of obscure gastrointestinal bleeding to be an ulcerated submucosal tumor (B).
As mentioned previously, video capsule endoscopy is used in the evaluation of conditions other than GI bleeding, including Crohn’s disease, small-bowel tumors, celiac disease, and familial polyposis syndromes. The detection rate of capsule endoscopy in celiac disease has been shown to be equal to that of esophagogastroduodenoscopy when clear villous changes are present.22 Notably, however, celiac disease is often evaluated with capsule endoscopy only if a practitioner suspects complications of the disease. In regard to small-bowel tumors, computed tomographic enterography has been shown to have a sensitivity greater than that of capsule endoscopy by a significant margin.23 One explanation is the fact that capsules traverse the duodenum and proximal jejunum at a relatively fast rate. Another issue regarding the ability of capsule endoscopy to detect small-bowel tumors is that it is difficult to differentiate tumors from natural undulations in the small bowel.24 Capsule endoscopy has not been clearly shown to have a significant role in the detection and surveillance of polyposis syndromes. Studies have caused some practitioners to be concerned that capsule endoscopy cannot identify the number and size of polyps as well as colonoscopy or push enteroscopy.25 In fact, it has been noted that capsule endoscopy does not image the duodenum well; therefore, subsequent endoscopic imaging via endoscopy is valuable when a disease such as familial adenomatous polyposis is suspected and there is a possibility that polyps are present in the duodenum. In Peutz-Jeghers syndrome, capsule endoscopy plays a role in surveillance. It is recommended that patients with this condition undergo capsule endoscopy at the age of 8 years and every 3 years thereafter if polyps are found. If polyps are not found on the initial examination, the capsule study should be repeated at the age of 18 years and every 3 years thereafter. Capsule endoscopy is used in addition to surveillance with upper and lower GI endoscopy, also begun at the age of 8 years.26
Capsule Endoscopy in Crohn’s Disease
Capsule endoscopy has multiple indications in Crohn’s disease. It has a role in monitoring disease activity and response to therapy as well as in assisting the diagnosis of suspected Crohn’s disease. Consensus from the International Conference on Capsule Endoscopy showed that capsule endoscopy was able to detect Crohn’s disease more than 50% of the time.27 However, there is a possibility of strictures in patients with Crohn’s disease, which may cause the capsules to become trapped. Even after negative results of small-bowel follow-through imaging, capsules can still become trapped in these patients more than 10% of the time. It is recommended that patients undergo a patency capsule study before video capsule endoscopy if there is a concern for strictures (Figure 2). The diagnostic yield of video capsule endoscopy in evaluating for recurrence in patients with known Crohn’s disease is higher than the yield of evaluating patients suspected of Crohn’s disease.28
Figure 2.
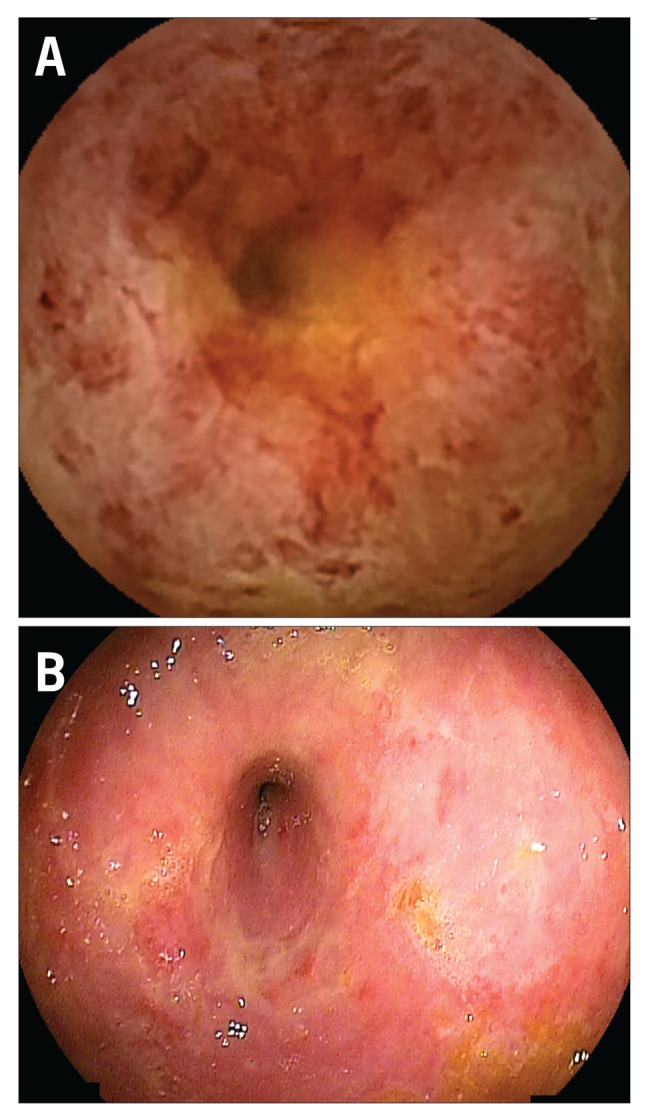
An ulcerated ischemic stricture secondary to Crohn’s disease noted on a capsule endoscopy (A) and then on a double-balloon enteroscopy (B) in a 53-year-old woman.
Risks and Complications of Capsule Endoscopy
Although capsule endoscopy is very safe, some risks are associated with the study. The main adverse event is retention of the capsule. If this occurs, plain radiographs can be used to try to identify the capsule. Retention occurs in less than 1% to 2% of patients, and the capsule can be removed either surgically or endoscopically.14 However, long-term retention nearly always indicates underlying pathology that will need to be investigated with further endoscopy or surgery.
Comparison of Capsule Endoscopy With Push Enteroscopy and Intraoperative Enteroscopy
Video capsule endoscopy is able to detect OGIB at a higher rate than push enteroscopy or barium studies.29 A systematic review from 2010 that included more than 22,000 procedures found capsule endoscopy to have a detection rate of 61% for OGIB.15 Of the lesions found during capsule endoscopy, just over half are thought to be the cause of bleeding.16 Overall, capsule endoscopy is approximately 2 to 3 times more likely than push enteroscopy to find the source of a small-bowel bleed, and 7 to 8 times more likely than a barium study.30
As previously mentioned, although capsule endoscopy is a high-yield study with relatively minimal risk, it does not always lead to a clinically valuable explanation of a patient’s GI bleeding. Commonly, a second upper or lower GI endoscopy can detect bleeds that were originally missed. Furthermore, the sensitivity of push enteroscopy is approximately equal to that of capsule endoscopy, and push enteroscopy allows intervention. Push enteroscopy with entrance through the mouth allows visualization past the ligament of Treitz. Up to 80 cm of jejunum can be visualized to detect bleeds, and potentially more if an overtube is used to reduce coiling.31 Studies have demonstrated sensitivities of push enteroscopy in identifying small-bowel bleeding ranging from 3% to 70%. The lesions most frequently found by push enteroscopy are secondary to angiodysplasia.32 Another study of push enteroscopy demonstrated that intervention during the procedure was possible for nearly half of the lesions found. Interestingly, many of the lesions found by push enteroscopy were within reach of standard endoscopy.33
Another method used to detect a source of bleeding, although more aggressive, is intraoperative endoscopy. This process allows the bowel to be evaluated both internally and externally during a laparotomy. The rate of detection with this method is high; however, there is also a high risk of rebleeding. Therefore, intraoperative endoscopy should be undertaken only if a specific site is known to require intervention with this method. Furthermore, intraoperative endoscopy is associated with higher morbidity and mortality rates than those of other endoscopic interventions.34
Balloon-Assisted Deep Enteroscopy
Balloon-assisted deep enteroscopy includes single-balloon enteroscopy (SBE), double-balloon enteroscopy (DBE), and spiral enteroscopy. DBE (Fujifilm Endoscopy) was first used in 2001; SBE (Olympus) came later, in 2007; and spiral enteroscopy (Spirus Medical) came in 2008.35-37 These techniques are most commonly used to investigate OGIB. As previously mentioned, balloon-assisted deep enteroscopy is often performed in conjunction with capsule endoscopy. Frequently, capsule endoscopy is performed first because it is less invasive and can provide guidance on the possible sources of a GI bleed.38 If disease is noted that is significantly distal to the ligament of Treitz, deep small-bowel enteroscopy is the ideal method of treatment. Balloon-assisted deep enteroscopy may also be a first-line intervention for patients known to have strictures (ie, Crohn’s disease) because a capsule can become trapped within the GI lumen (Figure 3).
Figure 3.

A Crohn’s disease (CD) stricture was noted on a capsule endoscopy in a 36-year-old man (A). He underwent a double-balloon enteroscopy to locate the capsule (B), which was found at the partially obstructing CD stricture (C) and removed (D).
The standard double-balloon endoscope has a 200- cm working length and a 145-cm overtube. The diameter varies from 8.5 mm within the working length of the tube to 12.2 mm at the overtube. Anterograde procedures can advance the tube on average from 220 to 360 cm into the small bowel, and retrograde procedures can provide visualization from 120 to 180 cm into the small bowel. Patients should not take anything by mouth after the midnight before the procedure and should undergo bowel preparation if a retrograde approach is to be used. Conscious sedation or general anesthesia can be administered, given the often long procedure time. Studies have shown that on average the procedure lasts 1 to 2 hours.31
When performing balloon-assisted deep enteroscopy, the scope is inserted orally (anterograde) or per rectum (retrograde) and advanced in repetitive cycles of inflation and deflation. The tube is advanced to its maximum length or until a lesion is identified. The point of maximal insertion is often tattooed so that it can be identified on subsequent studies or used to guide further interventions. At that point, the tube is slowly withdrawn to remove loops and pleat the small bowel over the overtube. The inflation and deflation technique is performed while the tube is removed.
Because of the length and the contractility of the small bowel, it is a difficult area in which to identify and treat disease. As mentioned, many different modalities are used to find the source of an obscure or occult GI bleed. The notable advantage of enteroscopy over capsule endoscopy is the ability to intervene when disease is found. Although enteroscopy is overall a safe procedure, its risks are greater than those of capsule endoscopy. Therefore, this test is often performed as a complementary procedure to maximize the detection and treatment of disease while minimizing risk for the patient. Specifically, of the tests mentioned thus far, capsule endoscopy can examine the entire small bowel but has no interventional capabilities. Push enteroscopy allows intervention but does not visualize the distal aspect of the small bowel. Intraoperative enteroscopy allows the identification and treatment of disease; however, it is significantly more invasive than the other methods for examining the small bowel. Multiple modalities within the class of deep small-bowel enteroscopy attempt to provide evaluation of the entire small bowel, with less risk than intraoperative enteroscopy and with the ability to treat disease. Deep small-bowel enteroscopy makes visualization of the entire bowel possible by pleating the bowel over an overtube. This technique also limits stretching of the bowel and allows better therapeutic technique.
SBE is very similar to DBE and can be used for many of the same indications mentioned throughout this review. Single-balloon enteroscopes also have a working length of 200 cm; the overtube has a length of 140 cm. The main difference is that in SBE, the tip of the scope rather than a second balloon (as in DBE) serves as an anchor when the overtube is extended. The diagnostic yield of SBE has been noted to be similar to that of DBE.39 One difference is that the rate of total enteroscopy is higher with DBE than with SBE because intubation of the terminal ileum is often more difficult with SBE than with DBE.40
Advantages of Balloon-Assisted Deep Enteroscopy
The most significant advantage of balloon-assisted deep enteroscopy over capsule endoscopy is the ability to intervene if a lesion is detected. DBE, SBE, and spiral enteroscopy can all be performed with an anterograde or retrograde approach. Traditionally, these techniques are used as a next step after capsule endoscopy. DBE can provide complete visualization of the small bowel. However, visualization can be limited in a patient with prior intestinal surgery. A study from Japan found that DBE could detect a source of GI bleeding nearly 80% of the time.41 As with capsule endoscopy, the yield of detection is higher when the procedure is performed closer to the time of bleeding. The same study showed that nearly 65% of bleeds could be controlled with DBE. A cost analysis study attempting to determine the best way to investigate a GI bleed found that DBE was a good first step for the workup of patients with OGIB.42 However, when capsule endoscopy was used to guide DBE, the long-term outcomes were better and complications fewer.43
Risks and Complications of Balloon-Assisted Deep Enteroscopy
Deep small-bowel enteroscopy is considered safe in those patients in whom traditional endoscopy is considered safe. Studies have shown that the most common complications of deep small-bowel enteroscopy are pancreatitis, bowel perforation, bleeding, and aspiration pneumonia. Pancreatitis is the most frequent complication and occurs in less than 0.5% of patients. Perforation also occurs in less than 0.5% of patients. A multicenter survey found that major complications can occur less than 1% of the time, while minor complications can occur up to 10% of the time. Overall, the rate of complications of deep small-bowel enteroscopy is less than 2%. There is a higher risk for complications if the procedure is therapeutic rather than strictly diagnostic, or if it is being performed in a patient with altered anatomy.44 For instance, perforation is more common after polypectomy or dilation.
Indications for Balloon-Assisted Deep Enteroscopy Besides Obscure Gastrointestinal Bleeding
In addition to the evaluation of OGIB, DBE has many other indications. These include identifying abnormalities seen on imaging, obtaining tissue for biopsy, evaluating small-bowel ulcer disease, evaluating and monitoring
Crohn’s disease, and evaluating celiac disease.45-47 Other uses include detecting polyps in patients with polyposis syndromes and performing endoscopic retrograde cholangiopancreatography in patients with Roux-en-Y anatomy.48,49 Therapeutic interventions include hemostasis, polypectomy, dilation, stenting, foreign body removal, and mucosal resection.50
Retrograde vs Anterograde Double-Balloon Enteroscopy
Capsule endoscopy can guide whether DBE should be performed in a retrograde or anterograde approach. In 2009, a study looked at 60 patients who underwent capsule endoscopy before DBE. The researchers determined that if a lesion was noted in the first 60% of a capsule study, an anterograde approach should be used, whereas if a lesion was seen in the last 40% of a capsule study, a retrograde approach should be employed. In the study, when these parameters were used, the lesion identified by capsule endoscopy could be reached on the first attempt with DBE.51
A study from the Cleveland Clinic examined both the diagnostic and therapeutic yields, as well as the complications, of anterograde and retrograde enteroscopy for OGIB. The authors looked at 250 enteroscopy procedures over nearly a 2-year period; approximately 75% were anterograde, and 25% were retrograde. They found that the diagnostic yield for anterograde enteroscopy was significantly higher than that for retrograde enteroscopy. They also noted that anterograde procedures were on average 15 minutes shorter and that the depth of maximal insertion was on average 2 times greater. The therapeutic yield was also significantly higher for anterograde enteroscopy. No significant difference in complication rates was found.52
Retrograde endoscopy has benefits in the investigation of more distal small-bowel disease. Examples include carcinoid tumors, which are often located in the more distal region of the small bowel; Crohn’s disease and ulcerative colitis; ulcers; and capsules retained as a result of strictures or arteriovenous malformations.53 Retrograde enteroscopy is more difficult to perform than anterograde enteroscopy because of the difficulty encountered in intubating the terminal ileum. Furthermore, adhesions often interfere with progression past the ileum into the small bowel.54 The entire small bowel is often evaluated with both anterograde and retrograde enteroscopy. This technique allows complete enteroscopy in 70% to 92% of patients.55
Diagnostic Yield of Double-Balloon Enteroscopy
Multiple studies have examined the diagnostic yield of DBE and have estimated it to be 40% to 80%, with interventions occurring in approximately over 1 in 10 to over 1 in 2 cases.56,57 In 2008, a meta-analysis looked at 11 studies that compared DBE with capsule endoscopy and demonstrated that the yields of the 2 modalities for significant small-bowel pathology were similar. The meta-analysis also demonstrated that both modalities were able to identify a variety of pathology, including vascular malformations, tumors, polyps, and inflammatory lesions, at similar rates.58 A study conducted at 2 centers in Wisconsin noted that in 80 of 133 patients who underwent both video capsule endoscopy and DBE, the results were found to have diagnostic agreement. The rate of diagnostic agreement was highest for angioectasia, at more than 80%, followed by ulcer disease, polyps, and normal findings.59 Another study, which looked at more than 2000 DBE procedures, found that DBE had a very high diagnostic yield for patients with polyposis syndromes, Crohn’s disease, or small-bowel GI bleeds. DBE was less effective for patients with nonspecific abdominal pain or diarrhea.60 A 2011 study looked at 300 DBE procedures that were performed for a variety of presentations and found DBE to have an overall detection rate of 70%. DBE was used in this study to evaluate small-bowel ulcers, chronic inflammation, Meckel diverticula, angiodysplasia, polyps, ulcerative lipomas, and tumors. DBE detected a source of bleeding in 86% of cases; a source of abdominal pain, distension, or malnutrition in 60%; an explanation for chronic diarrhea in 72%; and an explanation for hypoalbuminemia in 78%.61
A study from Ireland looked at 242 DBE procedures performed with or without a prior capsule endoscopy study.62 The authors found that the diagnostic yield was significantly higher when capsule endoscopy was performed before DBE in a search for the source of small-bowel bleeds. They also found a significantly higher rate of DBEs performed in an anterograde approach when capsule endoscopy preceded DBE; as previously mentioned, the anterograde approach is technically easier.
A meta-analysis from 2007 compared the diagnostic yield of capsule endoscopy with that of either retrograde or anterograde DBE and that of complete (both retrograde and anterograde) DBE in 8 studies including 277 patients.63 The authors noted no significant difference between the diagnostic yields of capsule endoscopy and complete DBE. On subanalysis, however, they found that the diagnostic yield of capsule endoscopy was higher than that of either retrograde or anterograde DBE alone. Another subanalysis, looking at OGIB, found that the diagnostic yield of capsule endoscopy was higher than that of either anterograde or retrograde DBE; however, the diagnostic yield of capsule endoscopy was lower than that of complete DBE.
A meta-analysis from 2013 looked at 12 prospective and retrospective studies encompassing 712 patients who had undergone either capsule endoscopy or DBE for OGIB.64 The study found that capsule endoscopy and DBE had similar diagnostic capabilities for vascular lesions, ulcerative and inflammatory lesions, tumors, and neoplasia. However, capsule endoscopy was noted to have a significantly better diagnostic ability for identifying fresh blood or clots, whereas DBE had a significantly better diagnostic ability for finding diverticular disease. In a subgroup analysis of 205 patients with OGIB who underwent both capsule endoscopy and DBE, the authors found that capsule endoscopy but not DBE detected a source of bleeding in 72%, whereas DBE but not capsule endoscopy detected a source of bleeding in 28%. Overall, the study demonstrated that each modality identified pathology that the other did not, and that when the source of OGIB could not be identified, these procedures were most effective if used to complement each other.
Therapeutic Impact of Double-Balloon Enteroscopy
A study from 2012 looked at DBE procedures performed in 118 patients over a 3-year period at a tertiary care center.65 Of the DBEs, 81 were anterograde and 26 were retrograde. Complete enteroscopy was performed in 16 patients. DBE was found to have had a diagnostic or therapeutic impact in 53% of the cases. OGIB was the most common indication for DBE, followed by treatment for polyps, inflammation, or vascular lesions. Another study from 2012 compared the use of DBE and its therapeutic impact from 2004 to 2006 with its use and therapeutic impact from 2006 to 2011 in 133 patients.66 During both time periods, the most common indication for DBE was OGIB, and the most common findings were mucosal lesions. However, during the latter time period, the performance of DBE as a result of the detection of abnormalities on other studies (eg, capsule endoscopy) increased. The study also noted an increase in the use of computed tomography (CT) and capsule endoscopy over the 2 time periods. Unlike the study cited earlier, which found a 53% rate of diagnostic or therapeutic impact of DBE, this study noted higher rates. In the first time period, DBE found 86% of pathology that was missed by other tests, and in the second time period, DBE found 100% of pathology missed by other tests. The diagnostic yield of DBE was 89% in the first time period and 93% in the second, and overall a therapeutic plan was determined for 90% of the patients only after DBE.
In regard to small-bowel bleeds, DBE allows the treatment of angiodysplastic lesions, which are a common source of small-bowel bleeds. The treatment consists of argon plasma coagulation (APC) therapy, which is effective in the short term; studies show a significant increase in the hemoglobin level during the 5 years after treatment. Furthermore, the need for blood transfusions is significantly decreased in patients who undergo APC therapy. However, studies have also shown that nearly half of patients who are treated with APC have a recurrent bleed within 3 years. Recurrent bleeds were more likely if patients had valvular heart disease or had originally been found to have multiple lesions on DBE.67,68 Interestingly, a study of 163 patients with OGIB examined their packed red blood cell transfusion requirements before and after DBE. The majority of the patients in this study underwent APC for arteriovenous malformations identified on examination. The study found that on average patients with OGIB received 6.6 units of packed red blood cells in the 6 months before DBE, compared with 1.6 units in the 6 months after DBE.69
DBE also plays a role in the diagnosis and evaluation of Crohn’s disease. It is estimated that approximately 10% to 30% of patients with Crohn’s disease have small-bowel involvement. In 2009, a study looked at 52 DBE procedures in 40 patients with Crohn’s disease in whom small-bowel disease was suspected because of persistent abdominal pain, iron deficiency anemia, or hypomagnesemia. Of the patients who underwent DBE, 60% were found to have small-bowel involvement, and 75% of them subsequently had their therapy changed as a result of this finding. At a 13-month follow-up, 83% of the patients whose therapy had been changed as a result of their findings on DBE showed sustained clinical improvement, with an average overall drop in their Crohn’s Disease Activity Index (CDAI) score from 178 to 90.70 Another study looked at patients with Crohn’s disease in whom small-bowel involvement was suspected and in whom distal involvement had been excluded. Of 50 patients who underwent DBE, 35 were found to have small-bowel lesions, and 46% of the lesions could not be seen by conventional endoscopy. Therapy was changed in 74% of the patients who were found to have small-bowel lesions, and 1 year later, 88% were in clinical remission, with a decrease in their CDAI score and mucosal repair noted on a subsequent DBE examination.71
In 2013, a retrospective study looked at 25 patients over a 6-year period who underwent polypectomy via DBE for Peutz-Jeghers syndrome.72 A total of 46 DBE procedures were performed in this patient population, with a total of 214 polypectomies. The average polyp size was 30 mm. In 7 DBE procedures, no polypectomy was performed because of small polyp size or polyps that were unresectable, and 6 patients underwent elective surgery for polyps that could not be resected endoscopically. At a nearly 5-year follow-up, no complications related to the small bowel had occurred as a result of DBE (Figure 4).
Figure 4.

In a 27-year-old man with Peutz-Jeghers syndrome, multiple polyps were noted throughout the small bowel on a capsule endoscopy (A). A polyp was seen in the proximal jejunum on a double-balloon enteroscopy (DBE; B). A polypectomy was performed in the proximal jejunum, seen on a DBE (C).
DBE can also play a role in preoperative planning and in the identification of tumor types before surgery. Before endoscopists were able to evaluate the entire small bowel, tumors in this region could be definitively diagnosed only by laparotomy. DBE makes possible the tissue biopsy of a tumor that is found on CT or capsule endoscopy, allowing a definitive and early diagnosis. These tumors can also be tattooed in order to guide subsequent surgical procedures and allow a more minimally invasive approach with less surgical morbidity.73 Earlier authors have stated that DBE should be the gold standard in the diagnosis of small-bowel tumors, given its safety and diagnostic capabilities.74 One study compared the ability of DBE with that of CT and positron emission tomography (PET) for detecting the spread of follicular lymphoma to the jejunum and ileum. DBE identified lesions and was able to provide demonstrative histology in 6 of 7 patients: 3 in the jejunum and 3 in the ileum. Neither CT nor PET was able to identify these lesions, which had the appearance of small white nodules and white villi on enteroscopy75 (Figure 5).
Figure 5.

A 45-year-old woman with a lesion suspicious for lymphoma on a capsule endoscopy (A). Follicular lymphoma was diagnosed on a double-balloon enteroscopy (B).
Studies have also looked at DBE in the setting of emergency small-bowel bleeding. In 2009, a study examined 17 DBE procedures in 10 patients with emergency overt OGIB.76 Causes of bleeding, including Dieulafoy lesions of the small bowel, tumors, angiodysplasia, multiple ulcers, and large arteriovenous malformations, were identified in 9 of the 10 patients (Figure 6). In all 10 patients, therapeutic intervention could be performed with APC, epinephrine injection, or fibrin glue placement. Further work needs to be done in this area; however, the study demonstrated that DBE can be performed in an emergency setting and can both diagnose and treat overt OGIB.
Figure 6.

A 60-year-old woman with an arteriovenous malformation (AVM) seen on a capsule endoscopy (A). A bleeding AVM was found within a jejunal diverticulum on a double-balloon enteroscopy (DBE; B). The AVM in the distal jejunum was treated via a DBE (C).
Conclusion
The goal of this article was to elucidate the roles of both capsule endoscopy and balloon-assisted deep enteroscopy in the diagnosis and treatment of a variety of small-bowel diseases. Each of these procedures has a role when performed alone; however, research suggests that they are especially effective as complementary techniques and together can provide more comprehensive answers and better-directed therapy. Both are relatively safe procedures that allow examination of the small bowel with high diagnostic and therapeutic yields; before these interventions became available, the small bowel was a difficult part of the GI tract to evaluate with minimally invasive, safe techniques. Both interventions are relatively new to the world of gastroenterology, and much research remains to be done regarding their overall efficacy, cost, and safety, as well as further indications for their use in the detection and treatment of diseases of the small bowel.
Footnotes
The authors have no relevant conflicts of interest to disclose.
References
- 1.Raju GS, Gerson L, Das A, Lewis B. American Gastroenterological Association. American Gastroenterological Association (AGA) Institute medical position statement on obscure gastrointestinal bleeding. Gastroenterology. 2007;133(5):1694–1696. doi: 10.1053/j.gastro.2007.06.008. [DOI] [PubMed] [Google Scholar]
- 2.Petroniene R, Dubcenco E, Baker JP, et al. Given capsule endoscopy in celiac disease: evaluation of diagnostic accuracy and interobserver agreement. Am J Gastroenterol. 2005;100(3):685–694. doi: 10.1111/j.1572-0241.2005.41069.x. [DOI] [PubMed] [Google Scholar]
- 3.Culliford A, Daly J, Diamond B, Rubin M, Green PH. The value of wireless capsule endoscopy in patients with complicated celiac disease. Gastrointest Endosc. 2005;62(1):55–61. doi: 10.1016/s0016-5107(05)01566-x. [DOI] [PubMed] [Google Scholar]
- 4.Cellier C, Green PH, Collin P, Murray J. ICCE. ICCE consensus for celiac disease. Endoscopy. 2005;37(10):1055–1059. doi: 10.1055/s-2005-870310. [DOI] [PubMed] [Google Scholar]
- 5.Cobrin GM, Pittman RH, Lewis BS. Increased diagnostic yield of small bowel tumors with capsule endoscopy. Cancer. 2006;107(1):22–27. doi: 10.1002/cncr.21975. [DOI] [PubMed] [Google Scholar]
- 6.Gastineau S, Viala J, Caldari D, et al. Contribution of capsule endoscopy to Peutz-Jeghers syndrome management in children. Dig Liver Dis. 2012;44(10):839–843. doi: 10.1016/j.dld.2012.05.018. [DOI] [PubMed] [Google Scholar]
- 7.Akin E, Demirezer Bolat A, Buyukasik S, Algin O, Selvi E, Ersoy O. Comparison between capsule endoscopy and magnetic resonance enterography for the detection of polyps of the small intestine in patients with familial adenomatous polyposis. Gastroenterol Res Pract. 2012;2012:215028. doi: 10.1155/2012/215028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Iddan G, Meron G, Glukhovsky A, Swain P. Wireless capsule endoscopy. Nature. 2000;405(6785):417. doi: 10.1038/35013140. [DOI] [PubMed] [Google Scholar]
- 9.Gong F, Swain P, Mills T. Wireless endoscopy. Gastrointest Endosc. 2000;51(6):725–729. doi: 10.1067/mge.2000.105724. [DOI] [PubMed] [Google Scholar]
- 10.Cave DR, Fleischer DE, Leighton JA, et al. A multicenter randomized comparison of the Endocapsule and the Pillcam SB. Gastrointest Endosc. 2008;68(3):487–494. doi: 10.1016/j.gie.2007.12.037. [DOI] [PubMed] [Google Scholar]
- 11.Bang S, Park JY, Jeong S, et al. First clinical trial of the “MiRo” capsule endoscope by using a novel transmission technology: electric-field propagation. Gastrointest Endosc. 2009;69(2):253–259. doi: 10.1016/j.gie.2008.04.033. [DOI] [PubMed] [Google Scholar]
- 12.Friedrich K, Gehrke S, Stremmel W, Sieg A. First clinical trial of a newly developed capsule endoscope with panoramic side view for small bowel: a pilot study. J Gastroenterol Hepatol. 2013;28(9):1496–1501. doi: 10.1111/jgh.12280. [DOI] [PubMed] [Google Scholar]
- 13.Holden JP, Dureja P, Pfau PR, et al. Endoscopic placement of the small-bowel video capsule by using a capsule endoscope delivery device. Gastrointest Endosc. 2007;65(6):842–847. doi: 10.1016/j.gie.2007.01.033. [DOI] [PubMed] [Google Scholar]
- 14.Westerhof J, Weersma RK, Koornstra JJ. Risk factors for incomplete small-bowel capsule endoscopy. Gastrointest Endosc. 2009;69(1):74–80. doi: 10.1016/j.gie.2008.04.034. [DOI] [PubMed] [Google Scholar]
- 15.Liao Z, Gao R, Xu C, Li ZS. Indications and detection, completion, and retention rates of small-bowel capsule endoscopy: a systematic review. Gastrointest Endosc. 2010;71(2):280–286. doi: 10.1016/j.gie.2009.09.031. [DOI] [PubMed] [Google Scholar]
- 16.Pennazio M, Santucci R, Rondonotti E, et al. Outcome of patients with obscure gastrointestinal bleeding after capsule endoscopy: report of 100 consecutive cases. Gastroenterology. 2004;126(3):643–653. doi: 10.1053/j.gastro.2003.11.057. [DOI] [PubMed] [Google Scholar]
- 17.Lepileur L, Dray X, Antonietti M, et al. Factors associated with diagnosis of obscure gastrointestinal bleeding by video capsule enteroscopy. Clin Gastroenterol Hepatol. 2012;10(12):1376–1380. doi: 10.1016/j.cgh.2012.05.024. [DOI] [PubMed] [Google Scholar]
- 18.Singh A, Marshall C, Chaudhuri B, et al. Timing of video capsule endoscopy relative to overt obscure GI bleeding: implications from a retrospective study. Gastrointest Endosc. 2013;77(5):761–766. doi: 10.1016/j.gie.2012.11.041. [DOI] [PubMed] [Google Scholar]
- 19.de Leusse A, Vahedi K, Edery J, et al. Capsule endoscopy or push enteroscopy for first-line exploration of obscure gastrointestinal bleeding? Gastroenterology. 2007;132(3):855–862. doi: 10.1053/j.gastro.2006.12.002. [DOI] [PubMed] [Google Scholar]
- 20.Nakamura T, Terano A. Capsule endoscopy: past, present, and future. J Gastroenterol. 2008;43(2):93–99. doi: 10.1007/s00535-007-2153-6. [DOI] [PubMed] [Google Scholar]
- 21.Riccioni ME, Urgesi R, Cianci R, et al. Negative capsule endoscopy in patients with obscure gastrointestinal bleeding reliable: recurrence of bleeding on long-term follow-up. World J Gastroenterol. 2013;19(28):4520–4525. doi: 10.3748/wjg.v19.i28.4520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Rondonotti E, Spada C, Cave D, et al. Video capsule enteroscopy in the diagnosis of celiac disease: a multicenter study. Am J Gastroenterol. 2007;102(8):1624–1631. doi: 10.1111/j.1572-0241.2007.01238.x. [DOI] [PubMed] [Google Scholar]
- 23.Hakim FA, Alexander JA, Huprich JE, Grover M, Enders FT. CT-enterography may identify small bowel tumors not detected by capsule endoscopy: eight years experience at Mayo Clinic Rochester. Dig Dis Sci. 2011;56(10):2914–2919. doi: 10.1007/s10620-011-1773-0. [DOI] [PubMed] [Google Scholar]
- 24.Girelli CM, Porta P, Colombo E, Lesinigo E, Bernasconi G. Development of a novel index to discriminate bulge from mass on small-bowel capsule endoscopy. Gastrointest Endosc. 2011;74(5):1067–1074. doi: 10.1016/j.gie.2011.07.022. [DOI] [PubMed] [Google Scholar]
- 25.Wong RF, Tuteja AK, Haslem DS, et al. Video capsule endoscopy compared with standard endoscopy for the evaluation of small-bowel polyps in persons with familial adenomatous polyposis (with video) Gastrointest Endosc. 2006;64(4):530–537. doi: 10.1016/j.gie.2005.12.014. [DOI] [PubMed] [Google Scholar]
- 26.Beggs AD, Latchford AR, Vasen HF, et al. Peutz-Jeghers syndrome: a systematic review and recommendations for management. Gut. 2010;59(7):975–986. doi: 10.1136/gut.2009.198499. [DOI] [PubMed] [Google Scholar]
- 27.Kornbluth A, Colombel JF, Leighton JA, Loftus E. ICCE. ICCE consensus for inflammatory bowel disease. Endoscopy. 2005;37(10):1051–1054. doi: 10.1055/s-2005-870315. [DOI] [PubMed] [Google Scholar]
- 28.Cheifetz AS, Kornbluth AA, Legnani P, et al. The risk of retention of the capsule endoscope in patients with known or suspected Crohn’s disease. Am J Gastroenterol. 2006;101(10):2218–2222. doi: 10.1111/j.1572-0241.2006.00761.x. [DOI] [PubMed] [Google Scholar]
- 29.Beejay UA, Haber GB, Rasul I, et al. A pilot trial comparing the diagnostic utility and reproducibility of Given diagnostic imaging system to conventional enteroscopy in the evaluation of chronic obscure gastrointestinal bleeding [abstract] Am J Gastroenterol. 2002;97(9):S299. [Google Scholar]
- 30.Triester SL, Leighton JA, Leontiadis GI, et al. A meta-analysis of the yield of capsule endoscopy compared to other diagnostic modalities in patients with obscure gastrointestinal bleeding. Am J Gastroenterol. 2005;100(11):2407–2418. doi: 10.1111/j.1572-0241.2005.00274.x. [DOI] [PubMed] [Google Scholar]
- 31.DiSario JA, Petersen BT, Tierney WM, et al. ASGE Technology Committee. Enteroscopes. Gastrointest Endosc. 2007;66(5):872–880. doi: 10.1016/j.gie.2007.07.032. [DOI] [PubMed] [Google Scholar]
- 32.Foutch PG, Sawyer R, Sanowski RA. Push-enteroscopy for diagnosis of patients with gastrointestinal bleeding of obscure origin. Gastrointest Endosc. 1990;36(4):337–341. doi: 10.1016/s0016-5107(90)71060-7. [DOI] [PubMed] [Google Scholar]
- 33.Zaman A, Katon RM. Push enteroscopy for obscure gastrointestinal bleeding yields a high incidence of proximal lesions within reach of a standard endoscope. Gastrointest Endosc. 1998;47(5):372–376. doi: 10.1016/s0016-5107(98)70221-4. [DOI] [PubMed] [Google Scholar]
- 34.Zaman A, Sheppard B, Katon RM. Total peroral intraoperative enteroscopy for obscure GI bleeding using a dedicated push enteroscope: diagnostic yield and patient outcome. Gastrointest Endosc. 1999;50(4):506–510. doi: 10.1016/s0016-5107(99)70073-8. [DOI] [PubMed] [Google Scholar]
- 35.Yamamoto H, Sekine Y, Sato Y, et al. Total enteroscopy with a nonsurgical steerable double-balloon method. Gastrointest Endosc. 2001;53(2):216–220. doi: 10.1067/mge.2001.112181. [DOI] [PubMed] [Google Scholar]
- 36.Yamamoto H, Yano T, Kita H, Sunada K, Ido K, Sugano K. New system of double-balloon enteroscopy for diagnosis and treatment of small intestinal disorders. Gastroenterology. 2003;125(5):1556. doi: 10.1016/j.gastro.2003.03.004. [DOI] [PubMed] [Google Scholar]
- 37.Gerson LB, Flodin JT, Miyabayashi K. Balloon-assisted enteroscopy: technology and troubleshooting. Gastrointest Endosc. 2008;68(6):1158–1167. doi: 10.1016/j.gie.2008.08.012. [DOI] [PubMed] [Google Scholar]
- 38.Westerhof J, Weersma RK, Koornstra JJ. Investigating obscure gastrointestinal bleeding: capsule endoscopy or double balloon enteroscopy? Neth J Med. 2009;67(7):260–265. [PubMed] [Google Scholar]
- 39.Aktas H, de Ridder L, Haringsma J, Kuipers EJ, Mensink PB. Complications of single-balloon enteroscopy: a prospective evaluation of 166 procedures. Endoscopy. 2010;42(5):365–368. doi: 10.1055/s-0029-1243931. [DOI] [PubMed] [Google Scholar]
- 40.Tsujikawa T, Saitoh Y, Andoh A, et al. Novel single-balloon enteroscopy for diagnosis and treatment of the small intestine: preliminary experiences. Endoscopy. 2008;40(1):11–15. doi: 10.1055/s-2007-966976. [DOI] [PubMed] [Google Scholar]
- 41.Yamamoto H, Kita H, Sunada K, et al. Clinical outcomes of double-balloon endoscopy for the diagnosis and treatment of small-intestinal diseases. Clin Gastroenterol Hepatol. 2004;2(11):1010–1016. doi: 10.1016/s1542-3565(04)00453-7. [DOI] [PubMed] [Google Scholar]
- 42.Gerson L, Kamal A. Cost-effectiveness analysis of management strategies for obscure GI bleeding. Gastrointest Endosc. 2008;68(5):920–936. doi: 10.1016/j.gie.2008.01.035. [DOI] [PubMed] [Google Scholar]
- 43.Jackson CS, Gerson LB. Management of gastrointestinal angiodysplastic lesions (GIADs): a systematic review and meta-analysis. Am J Gastroenterol. 2014;109(4):474–483. doi: 10.1038/ajg.2014.19. [DOI] [PubMed] [Google Scholar]
- 44.Mensink PB, Haringsma J, Kucharzik T, et al. Complications of double balloon enteroscopy: a multicenter survey. Endoscopy. 2007;39(7):613–615. doi: 10.1055/s-2007-966444. [DOI] [PubMed] [Google Scholar]
- 45.Yen HH, Chen YY, Soon MS. Nonsteroidal anti-inflammatory drug-associated ileal ulcers: an evaluation by double-balloon enteroscopy. Gastrointest Endosc. 2006;63(2):328. doi: 10.1016/j.gie.2005.06.063. [DOI] [PubMed] [Google Scholar]
- 46.Oshitani N, Yukawa T, Yamagami H, et al. Evaluation of deep small bowel involvement by double-balloon enteroscopy in Crohn’s disease. Am J Gastroenterol. 2006;101(7):1484–1489. doi: 10.1111/j.1572-0241.2006.00648.x. [DOI] [PubMed] [Google Scholar]
- 47.Hadithi M, Al-toma A, Oudejans J, van Bodegraven AA, Mulder CJ, Jacobs M. The value of double-balloon enteroscopy in patients with refractory celiac disease. Am J Gastroenterol. 2007;102(5):987–996. doi: 10.1111/j.1572-0241.2007.01122.x. [DOI] [PubMed] [Google Scholar]
- 48.Matsumoto T, Esaki M, Yanaru-Fujisawa R, et al. Small-intestinal involvement in familial adenomatous polyposis: evaluation by double-balloon endoscopy and intraoperative enteroscopy. Gastrointest Endosc. 2008;68(5):911–919. doi: 10.1016/j.gie.2008.02.067. [DOI] [PubMed] [Google Scholar]
- 49.Sakai P, Kuga R, Safatle-Ribeiro AV, et al. Is it feasible to reach the bypassed stomach after Roux-en-Y gastric bypass for morbid obesity? The use of the double-balloon enteroscope. Endoscopy. 2005;37(6):566–569. doi: 10.1055/s-2005-861444. [DOI] [PubMed] [Google Scholar]
- 50.Kita H, Yamamoto H. New indications of double balloon endoscopy. Gastrointest Endosc. 2007;66(3 suppl):S57–S59. doi: 10.1016/j.gie.2007.03.1038. [DOI] [PubMed] [Google Scholar]
- 51.Li X, Chen H, Dai J, Gao Y, Ge Z. Predictive role of capsule endoscopy on the insertion route of double-balloon enteroscopy. Endoscopy. 2009;41(9):762–766. doi: 10.1055/s-0029-1215009. [DOI] [PubMed] [Google Scholar]
- 52.Sanaka MR, Navaneethan U, Kosuru B, Yerneni H, Lopez R, Vargo JJ. Antegrade is more effective than retrograde enteroscopy for evaluation and management of suspected small-bowel disease. Clin Gastroenterol Hepatol. 2012;10(8):910–916. doi: 10.1016/j.cgh.2012.04.020. [DOI] [PubMed] [Google Scholar]
- 53.Lo SK. Technical matters in double balloon enteroscopy. Gastrointest Endosc. 2007;66(3 suppl):S15–S18. doi: 10.1016/j.gie.2007.05.046. [DOI] [PubMed] [Google Scholar]
- 54.Di Caro S, May A, Heine DG, et al. DBE-European Study Group. The European experience with double-balloon enteroscopy: indications, methodology, safety, and clinical impact. Gastrointest Endosc. 2005;62(4):545–550. doi: 10.1016/j.gie.2005.04.029. [DOI] [PubMed] [Google Scholar]
- 55.Mehdizadeh S, Ross A, Gerson L, et al. What is the learning curve associated with double-balloon enteroscopy? Technical details and early experience in 6 U.S. tertiary care centers. Gastrointest Endosc. 2006;64(5):740–750. doi: 10.1016/j.gie.2006.05.022. [DOI] [PubMed] [Google Scholar]
- 56.Heine GD, Hadithi M, Groenen MJ, Kuipers EJ, Jacobs MA, Mulder CJ. Double-balloon enteroscopy: indications, diagnostic yield, and complications in a series of 275 patients with suspected small-bowel disease. Endoscopy. 2006;38(1):42–48. doi: 10.1055/s-2005-921188. [DOI] [PubMed] [Google Scholar]
- 57.Gross SA, Stark ME. Initial experience with double-balloon enteroscopy at a U.S. center. Gastrointest Endosc. 2008;67(6):890–897. doi: 10.1016/j.gie.2007.07.047. [DOI] [PubMed] [Google Scholar]
- 58.Pasha SF, Leighton JA, Das A, et al. Double-balloon enteroscopy and capsule endoscopy have comparable diagnostic yield in small-bowel disease: a meta-analysis. Clin Gastroenterol Hepatol. 2008;6(6):671–676. doi: 10.1016/j.cgh.2008.01.005. [DOI] [PubMed] [Google Scholar]
- 59.Kalra AS, Walker AJ, Gopal DV, Guda NM, Soni A, Benson ME. Comparison of capsule endoscopy findings to the subsequent double balloon enteroscopy: a dual center experience. Am J Gastroenterol. 2012;107(suppl 1):S747. doi: 10.1155/2015/438757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Möschler O, May A, Müller MK, Ell C. German DBE Study Group. Complications in and performance of double-balloon enteroscopy (DBE): results from a large prospective DBE database in Germany. Endoscopy. 2011;43(6):484–489. doi: 10.1055/s-0030-1256249. [DOI] [PubMed] [Google Scholar]
- 61.Shi H, Ren J, Dong W. Double-balloon enteroscopy in the diagnosis and management of small-bowel diseases. Hepatogastroenterology. 2011;58(106):477–486. [PubMed] [Google Scholar]
- 62.McNamara D, Mahmud N, Alakkari A, et al. Double-balloon enteroscopy in Ireland in the capsule endoscopy era. Ir J Med Sci. doi: 10.1007/s11845-014-1097-0. In press. [DOI] [PubMed] [Google Scholar]
- 63.Chen X, Ran ZH, Tong JL. A meta-analysis of the yield of capsule endoscopy compared to double-balloon enteroscopy in patients with small bowel diseases. World J Gastroenterol. 2007;13(32):4372–4378. doi: 10.3748/wjg.v13.i32.4372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Zhang Q, He Q, Liu J, Ma F, Zhi F, Bai Y. Combined use of capsule endoscopy and double-balloon enteroscopy in the diagnosis of obscure gastrointestinal bleeding: meta-analysis and pooled analysis. Hepatogastroenterology. 2013;60(128):1885–1891. [PubMed] [Google Scholar]
- 65.Onal IK, Akdogan M, Arhan M, et al. Double balloon enteroscopy: a 3-year experience at a tertiary care center. Hepatogastroenterology. 2012;59(118):1851–1854. doi: 10.5754/hge10828. [DOI] [PubMed] [Google Scholar]
- 66.Jeon SR, Kim JO, Kim HG, et al. Changes over time in indications, diagnostic yield, and clinical effects of double-balloon enteroscopy. Clin Gastroenterol Hepatol. 2012;10(10):1152–1156. doi: 10.1016/j.cgh.2012.06.024. [DOI] [PubMed] [Google Scholar]
- 67.May A, Friesing-Sosnik T, Manner H, Pohl J, Ell C. Long-term outcome after argon plasma coagulation of small-bowel lesions using double-balloon enteroscopy in patients with mid-gastrointestinal bleeding. Endoscopy. 2011;43(9):759–765. doi: 10.1055/s-0030-1256388. [DOI] [PubMed] [Google Scholar]
- 68.Samaha E, Rahmi G, Landi B, et al. Long-term outcome of patients treated with double balloon enteroscopy for small bowel vascular lesions. Am J Gastroenterol. 2012;107(2):240–246. doi: 10.1038/ajg.2011.325. [DOI] [PubMed] [Google Scholar]
- 69.Walker AJ, Kalra AS, Benson ME, Guda NM, Soni A, Gopal DV. Impact of double balloon enteroscopy on red blood cell transfusion in patients with obscure gastrointestinal bleeding: a dual center experience. Am J Gastroenterol. 2012;107(suppl 1):S747. [Google Scholar]
- 70.Mensink PB, Groenen MJ, van Buuren HR, Kuipers EJ, van der Woude CJ. Double-balloon enteroscopy in Crohn’s disease patients suspected of small bowel activity: findings and clinical impact. J Gastroenterol. 2009;44(4):271–276. doi: 10.1007/s00535-009-0011-4. [DOI] [PubMed] [Google Scholar]
- 71.Mensink PB, Aktas H, Zelinkova Z, West RL, Kuipers EJ, van der Woude CJ. Impact of double-balloon enteroscopy findings on the management of Crohn’s disease. Scand J Gastroenterol. 2010;45(4):483–489. doi: 10.3109/00365520903563774. [DOI] [PubMed] [Google Scholar]
- 72.Serrano M, Mão-de-Ferro S, Pinho R, et al. Double-balloon enteroscopy in the management of patients with Peutz-Jeghers syndrome: a retrospective cohort multicenter study. Rev Esp Enferm Dig. 2013;105(10):594–599. doi: 10.4321/s1130-01082013001000004. [DOI] [PubMed] [Google Scholar]
- 73.Riccioni ME, Cianci R, Urgesi R, et al. Advance in diagnosis and treatment of small bowel tumors: a single-center report. Surg Endosc. 2012;26(2):438–441. doi: 10.1007/s00464-011-1896-6. [DOI] [PubMed] [Google Scholar]
- 74.Almeida N, Figueiredo P, Lopes S, Gouveia H, Leitão MC. Double-balloon enteroscopy and small bowel tumors: a South-European single-center experience. Dig Dis Sci. 2009;54(7):1520–1524. doi: 10.1007/s10620-008-0512-7. [DOI] [PubMed] [Google Scholar]
- 75.Higuchi N, Sumida Y, Nakamura K, et al. Impact of double-balloon endoscopy on the diagnosis of jejunoileal involvement in primary intestinal follicular lymphomas: a case series. Endoscopy. 2009;41(2):175–178. doi: 10.1055/s-0028-1119467. [DOI] [PubMed] [Google Scholar]
- 76.Mönkemüller K, Neumann H, Meyer F, Kuhn R, Malfertheiner P, Fry LC. A retrospective analysis of emergency double-balloon enteroscopy for small-bowel bleeding. Endoscopy. 2009;41(8):715–717. doi: 10.1055/s-0029-1214974. [DOI] [PubMed] [Google Scholar]