

Abstract
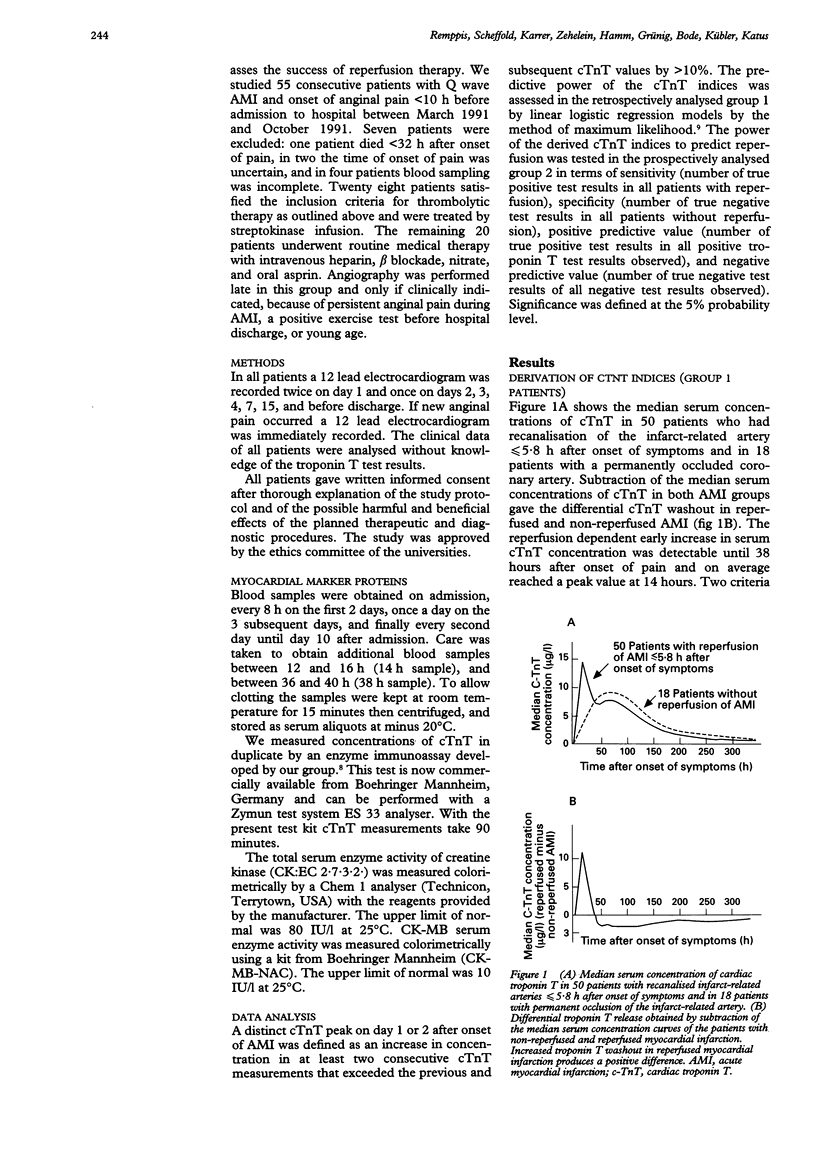
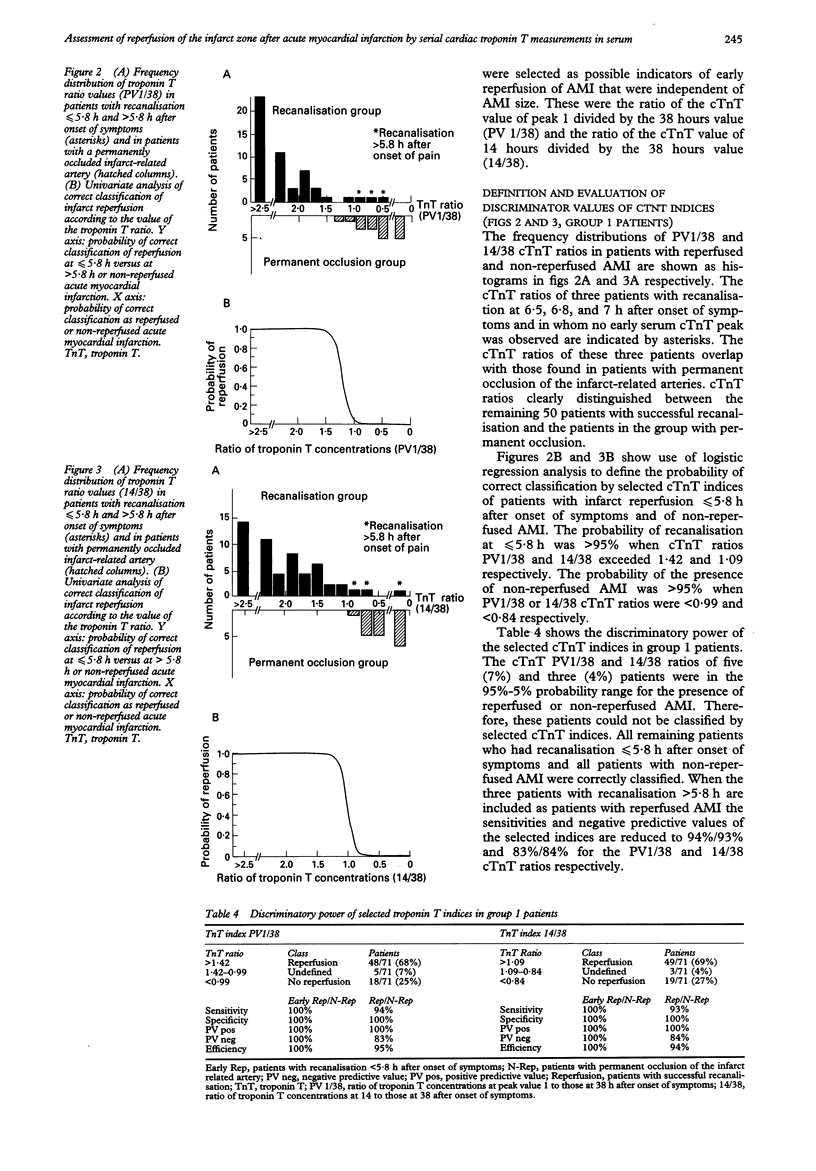
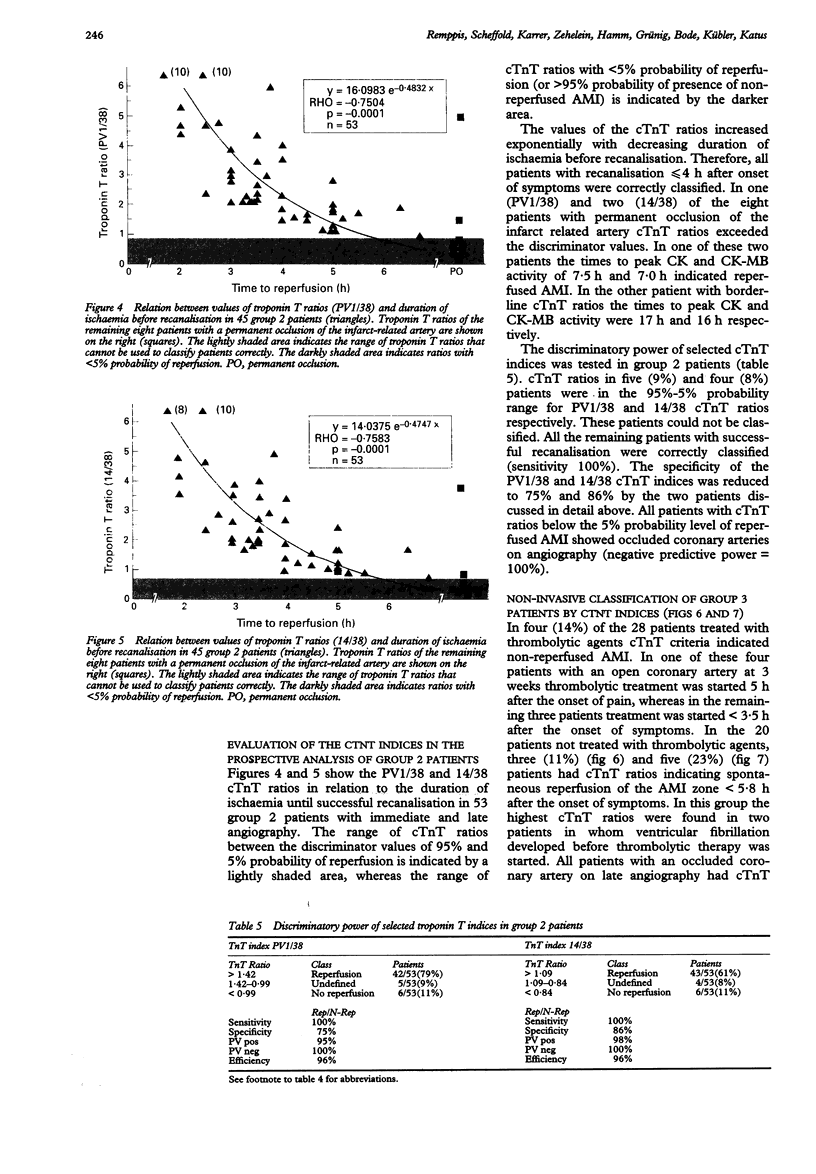
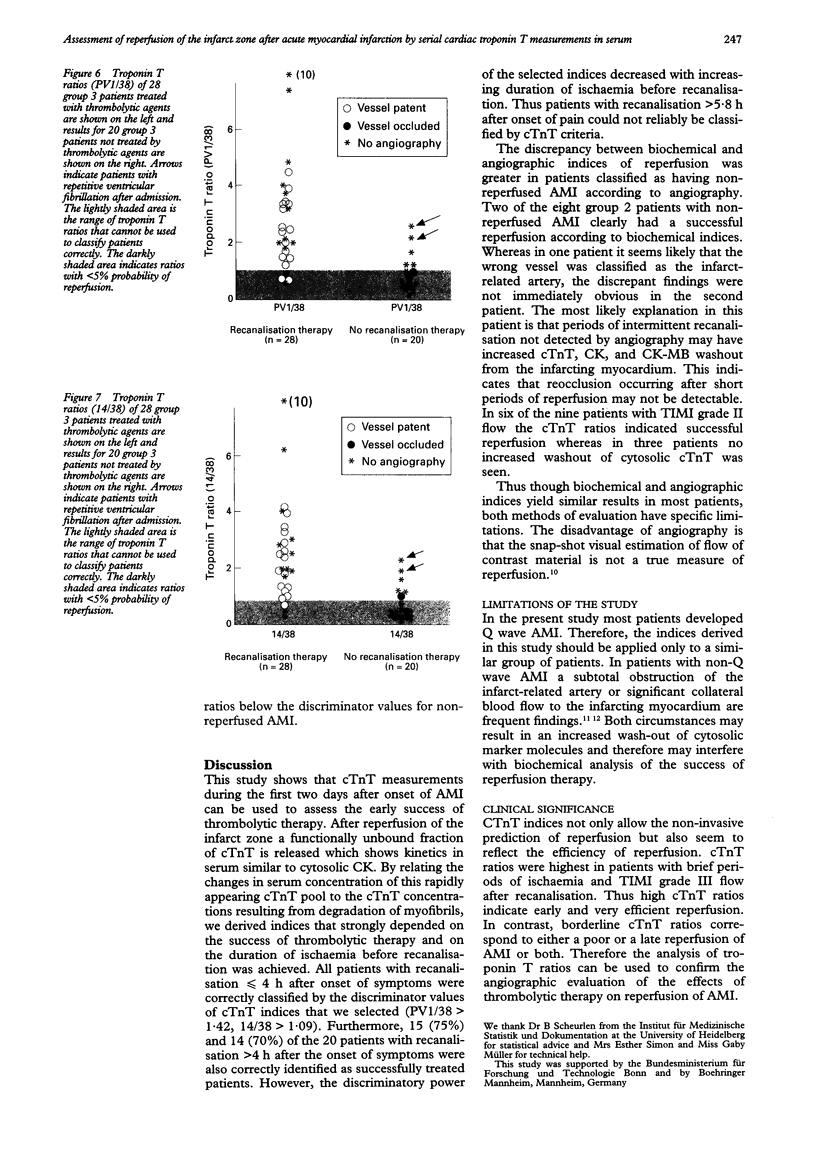
BACKGROUND--The purpose of this study was to derive indices of reperfusion and non-reperfusion after acute myocardial infarction (AMI) from changes in serum concentrations of cardiac troponin T and to test the predictive value of these indices. METHODS--The indices were derived from a retrospective analysis of changes in serum troponin T concentration in 71 patients given thrombolytic treatment who had immediate and late angiography (group 1). These troponin T indices were first tested in a blinded and prospective study of 53 consecutive patients eligible for thrombolytic therapy (group 2). They were then used for the non-invasive assessment of reperfusion of AMI in 48 patients (group 3). RESULTS--In group 1 troponin T serum concentration curves were biphasic in patients who had reperfusion < or = 5.8 h after the onset of symptoms. Release of the cytosolic troponin T pool resulted in a peak at 14 h and ended at 38 h. The probability of reperfusion was > 95% when the ratio of peak cytosolic troponin T concentration to concentration at 38 h (PV1/38) exceeded 1.42 or the ratio of troponin T concentration at 14 h to that at 38 hours (14/38) exceeded 1.09. The probability of the presence of non-reperfused AMI was < 5% when troponin T PV1/38 and 14/38 ratios were < 0.99 and < 0.84 respectively. These discriminatory values of troponin T indices correctly classified (efficiency 96%) 48 of the 53 group 2 patients in whom immediate and late angiography were performed. When troponin T indices were used to classify 48 group 3 patients who were not studied by immediate angiography, thrombolytic therapy was deemed to have been successful in 82% of the treated patients, with spontaneous recanalisation in 11% and 23% of the non-treated patients assessed by PV1/38 and 14/38 respectively. CONCLUSION--The PV1/38 or 14/38 ratios of serum troponin T concentration indicated the effectiveness of thrombolytic therapy in achieving reperfusion of AMI.
Full text
PDF

Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Collinson P. O., Stubbs P. J. The prognostic value of serum troponin T in unstable angina. N Engl J Med. 1992 Dec 10;327(24):1760–1761. doi: 10.1056/NEJM199212103272415. [DOI] [PubMed] [Google Scholar]
- DeWood M. A., Stifter W. F., Simpson C. S., Spores J., Eugster G. S., Judge T. P., Hinnen M. L. Coronary arteriographic findings soon after non-Q-wave myocardial infarction. N Engl J Med. 1986 Aug 14;315(7):417–423. doi: 10.1056/NEJM198608143150703. [DOI] [PubMed] [Google Scholar]
- Gerhardt W., Katus H., Ravkilde J., Hamm C., Jørgensen P. J., Peheim E., Ljungdahl L., Löfdahl P. S-troponin T in suspected ischemic myocardial injury compared with mass and catalytic concentrations of S-creatine kinase isoenzyme MB. Clin Chem. 1991 Aug;37(8):1405–1411. [PubMed] [Google Scholar]
- Hamm C. W., Ravkilde J., Gerhardt W., Jørgensen P., Peheim E., Ljungdahl L., Goldmann B., Katus H. A. The prognostic value of serum troponin T in unstable angina. N Engl J Med. 1992 Jul 16;327(3):146–150. doi: 10.1056/NEJM199207163270302. [DOI] [PubMed] [Google Scholar]
- Ito H., Tomooka T., Sakai N., Yu H., Higashino Y., Fujii K., Masuyama T., Kitabatake A., Minamino T. Lack of myocardial perfusion immediately after successful thrombolysis. A predictor of poor recovery of left ventricular function in anterior myocardial infarction. Circulation. 1992 May;85(5):1699–1705. doi: 10.1161/01.cir.85.5.1699. [DOI] [PubMed] [Google Scholar]
- Katus H. A., Looser S., Hallermayer K., Remppis A., Scheffold T., Borgya A., Essig U., Geuss U. Development and in vitro characterization of a new immunoassay of cardiac troponin T. Clin Chem. 1992 Mar;38(3):386–393. [PubMed] [Google Scholar]
- Katus H. A., Remppis A., Neumann F. J., Scheffold T., Diederich K. W., Vinar G., Noe A., Matern G., Kuebler W. Diagnostic efficiency of troponin T measurements in acute myocardial infarction. Circulation. 1991 Mar;83(3):902–912. doi: 10.1161/01.cir.83.3.902. [DOI] [PubMed] [Google Scholar]
- Katus H. A., Remppis A., Scheffold T., Diederich K. W., Kuebler W. Intracellular compartmentation of cardiac troponin T and its release kinetics in patients with reperfused and nonreperfused myocardial infarction. Am J Cardiol. 1991 Jun 15;67(16):1360–1367. doi: 10.1016/0002-9149(91)90466-x. [DOI] [PubMed] [Google Scholar]
- Sheehan F. H., Braunwald E., Canner P., Dodge H. T., Gore J., Van Natta P., Passamani E. R., Williams D. O., Zaret B. The effect of intravenous thrombolytic therapy on left ventricular function: a report on tissue-type plasminogen activator and streptokinase from the Thrombolysis in Myocardial Infarction (TIMI Phase I) trial. Circulation. 1987 Apr;75(4):817–829. doi: 10.1161/01.cir.75.4.817. [DOI] [PubMed] [Google Scholar]