

Summary
The objective of the study was to describe epidemiologic features of suicidal behavior by burns among women in two bordering provinces in Iran. A prospective hospital-based study of all suicidal behaviors by burns among women was carried out in the Iranian provinces of Khorasan (which borders Afghanistan) and Ilam (which borders Iraq) in 2006. These two provinces suffered from war and economic instability with high rates of poverty and unemployment. Data were obtained from patients, family members, and/or significant others through interviews during the course of hospitalization. Of 181 hospitalized patients, 130 (71.8%) were female, representing a hospital separation rate of 5.4 per 100,000 person-year (P-Y). The rate of suicidal behavior involving burns among the rural population was higher than that in the urban population (6.3 vs. 4.7 per 100,000 P-Y, P = 0.09). The median age of the patients was 23 years old, with a mean (±SD) of 27.9 (±14.3) years old. Approximately 68.5% of women were married. Quarrels with “a family member, spouse, a relative, or a friend” (marital plus other conflicts) was identified as the most common precipitating factor (88.5%) in attempting suicide. More than one third of women were abused (physically and/or verbally) by family members (i.e. spouse, father-in-law). Case fatality rate in this study was 52.3% (68/130). Suicide by burns is still a socio-epidemiological problem in Iran, particularly among young, married women in rural areas. Social and economic conditions, as well as violence against women, play a major role in the high rate of suicide by burns. The findings of this study highlight the need for the implementation of a well-organized approach to reduce the rate of suicide by burns among the most vulnerable populations in Iran.
Keywords: epidemiology, burn, suicide, woman
Abstract
L’objectif de l’étude était de décrire les caractéristiques épidémiologiques de comportements suicidaires par brûlures chez les femmes dans deux provinces frontalières de l’Iran. Une étude prospective en milieu hospitalier de tous les phénomènes suicidaires par brûlures chez les femmes a été réalisée dans les provinces iraniennes du Khorasan (qui borde l’Afghanistan) et Ilam (frontalière de l’Irak) en 2006. Ces deux provinces ont souffert de la guerre et de l’instabilité économique avec des taux élevés de pauvreté et de chômage. Les données ont été obtenues à partir de patients, membres de la famille et / ou d’ autres au cours de l’hospitalisation. Sur les 181 patients hospitalisés, 130 (71,8%) étaient des femmes et environ 68,5% d’entre elles étaient mariées. Le taux de comportement suicidaire par brûlures chez la population rurale était supérieur à celui de la population urbaine. L’âge médian des patients était de 23 ans, avec une moyenne (± SD) de 27,9 (± 14,3) ans. Les querelles avec «un membre de la famille ou un ami» ont été identifiées comme le facteur le plus déterminant (88,5%) dans une tentative de suicide. Plus d’un tiers des femmes ont été victimes de violence (physique et / ou verbale) par les membres de la famille. Le taux de létalité dans cette étude était de 52,3% (68/130).Le suicide par brûlure est toujours un problème socio-épidémiologique en Iran, en particulier chez les jeunes femmes mariées dans les zones rurales. Les conditions sociales et économiques, ainsi que la violence contre les femmes, jouent un rôle majeur dans le taux élevé de suicide par brûlures. Les résultats de cette étude soulignent la nécessité de la mise en oeuvre d’une approche bien organisée pour réduire le taux de suicide par brûlures chez les populations les plus vulnérables en Iran.
Introduction
Suicide is a growing global challenge. It is an important and preventable public health problem which is associated with high economic burden in both primary and secondary health care settings. Although individuals commit suicide for various reasons, communities are often not willing to discuss the issue.
Suicide by burns may be by far the most drastic, violent and tragic method of suicide and accounts for approximately 2% of all suicides.1 It is more frequent in economically underdeveloped and developing countries, particularly in Africa, Asia and the Middle East. In economically developed countries, previous studies have reported frequencies of suicide by burns from <0.5 to 2% for population under the age of 18 years, while in adults the rate was estimated as high as 25% of the total burn admissions. 2-4 In North America, suicide by burns is relatively rare. According to the most recent national Burn Repository Annual Report containing data from 1999 to 2008, 1,115 burn injuries in the United States were suspected self-inflicted injuries, accounting for 0.9% of all burn injuries in that period.5,6 The incidence rate of suicide by burns in the USA is reported 0.1 per 100,000 (only 0.5% of all suicides).7 It is also prevalent in immigrant communities. For instance, in the UK suicide by burns was mostly committed by immigrant women from Asia (for whom 20% were from India).8
The issue of suicidal behavior by burns has been a topic of great interest in Iran.9-20 Various studies on suicidal behavior by burns in Iran have shown that women are the primary victims of suicide by burns (>70% of suicide burn patients).9-22 The majority of these patients are young with an average age of younger than 29 years.9-15, 17-21 It has been suggested that suicide by burns is higher in rural areas and also in bordering provinces, particularly those that were directly affected by war (i.e. the Iran-Iraq 8-year war).17 Although there has been a considerable amount of literature on suicide by burns in Iran, there is still an urgent need for a better understanding of suicide among vulnerable, culturally different, and diverse populations. Considering that the majority of previous studies used a retrospective chart reviewing (or existing data sources) method,10,17,18,20,22 there may have been a potential source of bias in their findings. This is because both patients and health care providers may not voluntarily discuss and/or document factors associated with the events. It is important to note that Iran is a diverse country (divided into thirty provinces) consisting of people with many ethnic backgrounds. The ethnic diversity of the population may play a role in the epidemiologic features/patterns of suicide by burns in different provinces.
This study provides accurate information on suicide by burns and its associated factors in two bordering provinces of Ilam (bordered by Iraq) and Khorasan (bordered by Afghanistan). It should be noted that identifying underlying causes of suicide by burns is one of the most challenging problems researchers could face in conducting studies of this kind.
The authors initiated a collaborative effort to study the epidemiology of suicidal behaviors by burns through a prospective national multicenter study in various provinces across Iran.15,19 As a part of this collaborative work, this study was carried out to identify the scope of the problem, socio-epidemiological features, and associated socio-cultural factors among women in the two aforementioned bordering provinces. The authors intend to use the key findings of this study to develop preventive programs targeting the most vulnerable groups in the population. The key findings of this study along with appropriate recommendations for interventions will also be submitted to officials/ decision makers at the provincial and national levels to reduce the rate of suicide by burns. This will hopefully yield new directions for research, and assist health care professionals, as well as policy makers, in the development of more effective strategies and intervention programs.
Materials and methods
Patients and procedures
The province of Ilam (also called Elam in Kurdish) is one of the 30 provinces of Iran, located in south-west of the country, bordering Iraq and covering an area of approximately 20,000 km2. The population of the province is approximately 545,787 (0.8% of the national population), with 25% of the population under 15 years old (Statistical Center of Iran, 2011). The population of Ilam is predominantly Kurdish. During the Iran-Iraq war, the province of Ilam was heavily barraged, and Iraq’s intense bombings left no economic infrastructure for the province. Ilam has thus been one of Iran’s more undeveloped provinces with an unemployment rate of approximately 15.7% (Statistical Center of Iran, 2011).
The province of Khorasan was the largest province of Iran, located in the eastern part of the country, until 2004- 2005 when it was divided into the three provinces of North Khorasan, South Khorasan, and Razavi Khorasan. The population of all three provinces is over 7,000,000, but the total area of Khorasan is greater than the size of the United Kingdom which is 244,000 km2. The mean age of the population in Khorasan is 23.6 years, with a median of 18.5 years (Statistical Center of Iran, 2011). The major ethnic groups in this region are Persians with Kurdish, Turkish and Turkmen minorities. During the soviet invasion and civil wars in Afghanistan, Khorasan faced a number of challenges including displaced population from the neighboring country as well as economic and security problems. The unemployment rate in Khorasan is approximately 8.4% (Statistical Center of Iran, 2011).
The study is a prospective hospital-based study conducted from 2006 to 2007 at Taleghani Hospital, located in the city of Ilam (the capital of the province of Ilam), and Imam Reza Burn Center, located in Mashhad (the capital of the province of Khorasan). These represent the only referral burn centers for major burn injuries in Ilam and Khorasan respectively. Due to their designations as tertiary burn referral centers, all significant burn cases in their respective provinces are referred to these burn centers. Thus, the rosters of burn cases in these centers can be used to estimate the total number of major burn injuries occurring in these provinces.
All patients who were hospitalized for burn injuries were interviewed by a nurse practitioner among the burn center staff in each center during hospitalization. If a patient was in critical clinical condition (unable to communicate), or died during the first 24 hours of admission, the history and relevant information was obtained from a “significant other” (e.g., spouse, parents, siblings, other relatives, etc.) who knew the patient well. Training sessions were held by one of the authors (A.R. Lari), with the nursing staff explaining the purpose of the study and how to conduct the interviews. Regular visits were scheduled with the nurse practitioner [by A.R. Lari] to address possible concerns and/or challenges that may have been encountered during the course of the study.
It is important to note that in order to collect information on those with minor burns and those who died at home, we contacted the chief medical examiners’ offices in each province as well as emergency rooms. However, the data were either not accessible (i.e. not in electronic format), or its quality and accuracy was of concern. We also recognized that some patients with minor burns were treated in outpatient clinics, which we could not obtain data from due to lack of electronic medical records (EMR).
All patient testimonials were collected using a standardized questionnaire. As part of the validation process and prior to data collection, the questionnaire was reviewed by the research team and piloted to assess its validity. Questions included pertained to age, sex, marital status, place of residence (rural area was defined as a community with a population less than 5000), level of education, employment status, precipitating factors, psychiatric history, method of self-immolation, total body surface area (TBSA) burned, as well as outcome. It should be noted that interviews were often conducted more than once during the course of hospitalization, given that a mutual trust relationship would have taken sometime to establish and, furthermore, patients may not have been psychologically prepared to discuss events and factors contributing to their suicide attempts at first interview. The main source of information was first and foremost the patient herself. Participants were interviewed face to face once their informed consent had been obtained, which was after they were stabilized in the burns units. Other sources following the patient’s interview were husband (if married), other adults in the households (e.g., parents, siblings) and/or neighbors who may have witnessed the event, patient’s relatives, and her husband’s relatives. In occasions where the patient was not able to communicate due to medical conditions or died, the collateral sources referred to above were interviewed. To have a more precise and reliable “story”, medical social worker information was also used, which thus acted as a form of data quality control. It was not surprising to us to learn that the testimonials of husbands and/or their relatives were not always consistent with the patient’s version of events.
In this study, any past psychiatric diagnoses were obtained either through the charts in case of a psychiatric consultation, or directly from the patients and/or their “significant other”. It is important to note that past psychiatric diagnoses obtained directly from the patients and/or their “significant other” were carefully assessed. Nursing staff assessed the reliability of information obtained during interviews.
The study was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Statistical Analysis
The Statistical Package for the Social Sciences (SPSS) version 19.0 was used to conduct the analyses (Statistical Program for Social Sciences, 2010). The Chi-square test was used to compare categorical data. A binary regression model was also used to examine the association between outcome (alive vs. deceased) and various other factors. Further we used a t-test given there were no co-variates, which produced the same results. The level of significance was set at 0.05. Hospital separation rates were calculated as the number of hospitalized patients with suicidal behaviors divided by the corresponding estimated population, multiplied by 100,000 (population aged 12 years and over). Denominators were taken from the 2006 census population.
Results
During the study period, 181 patients aged 12-83 years were hospitalized due to suicidal behavior by burns of whom 130 (71.8%) were female, representing a hospital separation rate of 5.4 per 100,000 person-year (P-Y) (95% confidence interval [CI]: 4.5-6.3 per 100,000 P-Y). The hospital separation rate in the province of Ilam was significantly higher than that for Khorasan (43.9 vs. 8.8 per 100,000 P-Y, respectively [p < 0.0001]). The mean (±SD) and median age for patients with suicidal behavior by burns was 27.9 (±14.3) and 23 years, respectively. The mean age (±SD) in Ilam and Khorasan was 28.6 (±10.7) and 27.6 (±15.5) years, respectively (p > 0.05).
The age-specific rate for suicidal behavior by burns peaked at the age group 20-29 years (11.8 per 100,000 PY; 95% CI: 8.9-14.8 per 100,000 P-Y) and decreased with increasing age. This was true in both provinces, albeit the rates were significantly higher in Ilam than Khorasan for all age groups (Ilam 43.9 vs. Khorasan 8.8 per 100,000 PY, p < 0.0001). The hospital separation rate of suicidal behavior involving burns among the rural population was higher than in the urban population (6.3 vs. 4.7 per 100,000 P-Y, p = 0.09). The rate of this behavior was also higher in rural areas among all age groups than in urban settings in both provinces, although the rates were much higher in Ilam than in Khorasan (Table I).
Table I. Hospital separation rate of suicidal behavior by burns by age in two bordering provinces in Iran.

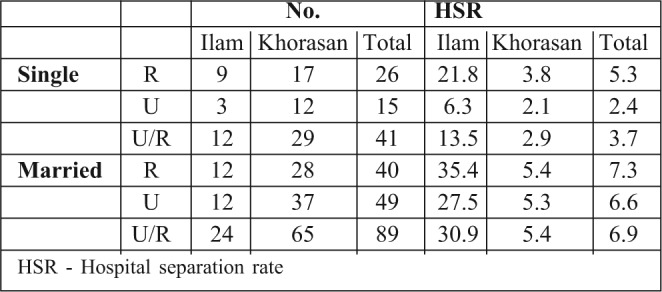
Approximately 68.5% (89/130) of the women were married. The overall rate of suicidal behaviors involving burns was significantly higher among those who were married than among single people (6.9 vs. 3.7 per 100,000 PY, respectively) (p < 0.0001). Further, the rate of suicidal behavior by burns among both married and single people was higher in rural areas than in urban areas (Table II).
Table II. Hospital separation rate of suicidal behavior by burns by literacy and age in two bordering provinces in Iran.
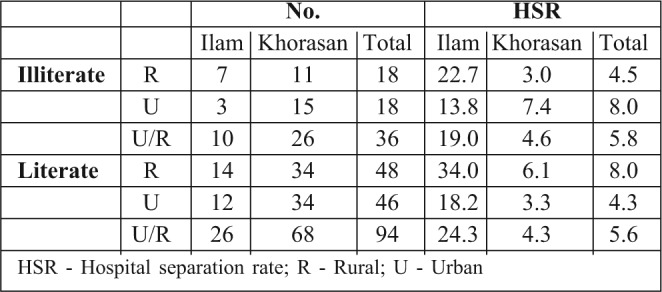
The rates of suicidal behavior by burns among the illiterate and literate populations were 5.8 and 5.6 per 100,000 P-Y, respectively (p > 0.05). While the rates of suicidal behavior by burns among the illiterate population in urban areas was higher than the literate population (4.5 vs. 8.0 per 100,000 P-Y) (p > 0.05), the opposite pattern was observed in rural areas, as the rate was higher among the literate population than those who were illiterate (8.0 vs. 4.3 per 100,000 P-Y) (p > 0.05) (Table III).
Table III. Hospital separation rate of suicidal behavior by burns by marital status and age in two bordering provinces in Iran.
Of the 130 patients hospitalized due to suicide attempts by self-immolation, 68 patients died resulting in a case fatality rate of 52.3% and a mortality rate of 2.8 per 100,000 P-Y; 62 patients were discharged alive (survival rate of 2.6 per 100,000 P-Y).
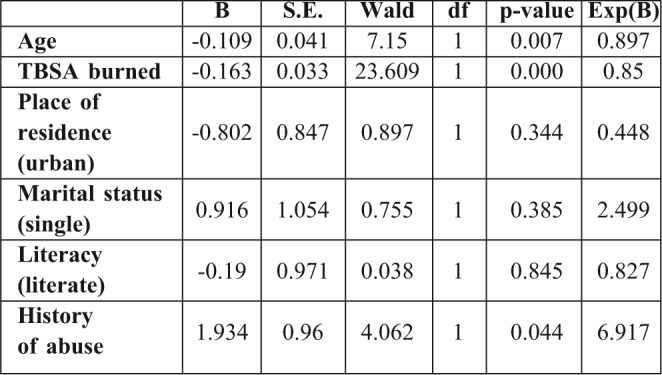
The overall mean (±SD) TBSA burned in this study was 65.9% (± 28.2). The mean TBSA burned among those who died was significantly higher than among those who survived (87.8% vs 41.8%, respectively) (p < 0.001). A statistically significant difference was found between mean TBSA burned and literacy (69.1% for literate vs. 57.4% for illiterate, p = 0.03). No significant associations were found between TBSA burned and place of residence or marital status. A binary logistic regression model demonstrated that a direct association existed between vital status (alive vs. deceased) with age, the degree of TBSA, and positive history of abuse (p < 0.05) (Table IV).
Table IV. Logistic regression model demonstrating association between various factors in two bordering provinces in Iran.
In this study, 97.7% of patients used an inflammable liquid, mainly kerosene, to set themselves on fire. The most frequent precipitating factor for suicidal behavior in this population (including both married and non-married women) was a quarrel with a family member, spouse (where applicable), a relative, or a friend (marital plus other conflicts) (115/130, 88.5%), followed by financial problems (6/130, 4.6%). Among the married population, marital conflict was the most common precipitating factor (88.7%, 79/89). Further, the causes of suicide attempts involving burns by age group is presented in Table V, which shows a quarrel with a family member, spouse, a relative, or a friend (marital plus other conflicts) to be the most common precipitating factor for suicidal behavior in all age groups (p > 0.05). It should be noted that some of the patients may have had more than one precipitating factor for their suicidal behaviors due to burns. At least one-third of female patients reported to be physically or emotionally/ mentally abused by their husband, husband’s family, or even their own family members such as their father, brother, etc. Fifty-three of the 130 patients (40.8%) were identified as having a history of psychiatric disease. Depression (34/130, 26.2%) and psychotic disorders (e.g., schizophrenia) (10/130, 7.7%) were found to be the most common psychiatric diagnoses associated with suicidal behaviors in this study.
Table V. Precipitating factors associated with suicide by burns according to age groups in two bordering provinces in Iran.

Discussion
It has well been established and reported that Iran has one of the highest rates of suicidal behavior by burns worldwide. 9,13-15,17This is also true for other nations in the Middle East region as well as Asia where suicide by burns is a significant public health challenge and burden.23-26 A nation- wide epidemiological study of deaths due to injuries in Iran revealed that the death rate of all intentional injuries was 10.1 per 100,000 (2.5% of all annual deaths), with 61% being associated with suicide-related events (6.2 per 100,000) of which 2.3 per 100,000 were due to intentional self-harm by burns.27 Ahmadi et al.17 reported that 27% of suicide cases in Iran were via self-immolation. Suicidal behavior by burns comprises up to 40% of total burn care facilities’ hospitalizations in Iran.14 One of the most unique and tragic aspects of such phenomenon in Iran, as well as other countries in the region is the overrepresentation of women, particularly young and married.9,11,13,15,17,19,21 This indeed prompted us to carry out this study with focus on women in the two bordering provinces in Iran. Our findings showed that women comprised more than 70% of hospitalization admissions due to suicidal attempt/deliberate self-harm by burns with a hospital separation rate of 5.4 per 100,000 P-Y. Mean age of these patients was 27.9 with a median of 23 years, which is comparable with other studies in Iran.9,11,13,15,17,19,21 Of note was the significant difference between the rates of suicide by burns in the two provinces (Ilam 43.9 vs. Khorasan 8.8 per 100,000 P-Y, p < 0.0001). These two provinces are geopolitically unique in that both are bordering provinces. Ilam shares a border with Iraq and was intensively affected during the 8-year Iran-Iraq war, in addition to experiencing postwar problems. This province still suffers a great deal of economic impoverishment, underdevelopment, and has a higher than the national unemployment rate. Khorasan, on the other hand, faced many challenges during decades of war and post-war between neighboring Afghanistan, including displaced populations, economic difficulties and drug trafficking, although economically Khorasan is in a better position than Ilam. It should be noted that drug trafficking is a major problem in Afghanistan which has had a significant impact on the neighboring Khorasan province. In addition to the abovementioned geopolitical factors, socio-culturally the two are different; Ilam is among the few provinces with a high proportion of people with Kurdish ethnicity. Previous studies by the authors and other researchers in Iran have suggested that people of Kurdish ethnicity were more likely to engage in suicide by burns.13,17,20
The majority of people engaging in self-immolation in Iran were young (mean age = 29),17 which is similar to our findings. Almost all studies on suicidal behavior by burns in Iran reported a remarkably significant overrepresentation of women.10-21 Akbari et al.27 found that the national rates of intentional injuries were more common among men than women except for intentional self-harm by burns (0.8 vs. 4.0 per 100,000 for males and females, respectively). Ahmadi et al.17 found gender differences in self-immolation rates to be particularly notable, with women having an overall rate 2.4 times that of men in Iran. In Kurdistan, for example, the rate was found to be as high as 23.0.17 From our experiences in various burn care facilities in Iran, we found that women who were hospitalized due to self-immolation did not really intend to commit suicide and, in fact, in one of our previous studies it was demonstrated that over 85% of patients, mainly women, regretted their attempts.13 Moreover, Ahamadi’s study14 clearly showed the gender difference that most of the women who successfully committed suicide by self-burning only intended to attempt suicide but did not realize the consequences of setting themselves on fire. A few studies suggested that people of Kurdish ethnicity were more likely to engage in suicide by burns.13,17,19 Some studies identified unemployment as a risk factor for suicide by burns.13,15,17,19 A number of studies reported that marital conflict with spouse and conflict with other members of the family was associated with increased risk of suicide by burns.13,15-17,19-21
Women may make more suicide attempts than men because of gender-related vulnerability to psychopathology and to psychosocially disadvantageous circumstances. In addition, reproductive, hormonal, and other gender-specific factors may increase risk of suicide in women. More specifically, depression is the most common risk factor for serious suicidal behavior in both men and women, but occurs twice as often in women as in men. In our study more than 40% of patients had a history of psychiatric illness, of which depression was the most common psychiatric diagnosis. Generally, marriage appears to be less protective against suicide for women than for men. This seems to be particularly the case for young women in economically developing countries. The life and marital circumstances of these women may make them vulnerable to suicidal behavior. Stresses may include arranged and early marriage, young motherhood, low social status, domestic violence, and economic dependence. Social, cultural, and religious constraints may discourage women from employment, careers, and financial and social independence, and encourage them to remain within unhappy marriages in dependent living arrangements with extended family.
All previous studies in Iran demonstrated that the predominant causes or precipitating factors of self-immolation identified by survivors or contacts were various forms of oppression or violence against women in their families. 11,13-17,19 In this study, chronic marital and interpersonal conflicts were the leading precipitating factors of suicidal behavior by burns. Interpersonal conflicts, including marital disharmony with spouses and domestic violence, have an important role in suicide risk in low-middle income countries.21 In a case-control study, Ahmadi et al. showed that marital conflict with a spouse might have a role in self-immolation. They indicated that patients who reported conflict with other members of the family were much more likely to be victims of self-immolation (10 times more likely).21 In our study at least 30% of patients reported being physically or emotionally/mentally abused by their husband, husband’s family, or even their own family members, which is mainly attributed to the patriarchal ideologies present in these families.13,15,19 We believe that the rate of abuse reported in this study may well be underestimated as the importance of preserving the honor of the family leads abusers, victims, and even health care professionals to avoid disclosing these offences. The tragedy of self-burning, which has driven mainly young women to a fiery death in Iran, has been earlier interpreted by the authors as a “cry for help”.14,15 Women and girls appear to see this horrifying act both as a means of escaping from intolerable conditions and speaking out against abuse in their families, since their actual voices do not bring about changes that would allow them to lead safe and secure lives. We found it gravely tragic that the majority of these women, who were mainly young and married regretted their suicide attempts, while more than half of them succumbed to their injuries. The remainder had to live with the physical and mental scars left from their suicide attempts, inevitably having a significantly negative psychosocial impact.
The rate of suicidal behavior by burns was found to be similar among the illiterate and literate populations in this study. Ahmadi’s study17 suggested that literacy is not a significant risk factor for suicide by burns in Iran, in that they did not find a significant difference in the literacy rate between societies that have higher rates of suicide by burns compared with those who did not. In contrast, other studies from Iran demonstrated that the rate of suicidal behavior by burns decreases as the level of education increases. 13,14,19
In this study the rate of suicidal behavior due to burns was higher among the rural population than the urban. In a nation-wide study on self-immolation in Iran using administrative databases, Ahmadi et al.17 showed that the rate of suicide by burns was higher in rural areas than in urban areas except in Khuzestan, Gazvin, and East Azarbayejan provinces. It was suggested that this may be attributed to a lower rate of unemployment among rural female populations in these three provinces compared with the national rate, as well as a higher rate of depression among the urban male population. A similar observation was reported by Akbari et al.27 where they reported a higher rate of suicide due to burns in the rural areas of Iran compared with urban areas (2.8 vs. 2.0 per 100,000). It should be noted that the predominance of socio-cultural factors in rural areas as opposed to urban, such as a patriarchal structure, women’s lack of independent sources of income (economic dependency), and lack of respect from society, significantly contribute towards such social tragedy.
We believe that many of these women mistakenly think that death as a result of self-immolation will be instant. However, it is sometime later that they come to know the truth. There are some patients who die instantly but the majority either die during the course of hospitalization after suffering a great deal of agony, or survive with both physical and mental scars for the rest of their lives. Furthermore, it seems that there is a culture of suicide by burning. Self-immolation by women may be seen as a symbol of protest against violence and aggression that has formed in society, as stories of such women are often heard in neighborhoods and communities, which could perpetuate the culture of suicide by self-burning.
This study has some limitations. We did not include cases in which the victims died at the scene, nor cases of less severe injuries that were treated in emergency rooms or were not treated at all. For these reasons, any generalization of the findings of this study may be limited. We estimated that less than 5% of patients with suicidal behavior might not have arrived at hospital (died at scene), which are unlikely to impact our results. Furthermore, since suicide is a sensitive subject which is also strongly condemned and regarded negatively by society, victims may not be willing to openly discuss it with care providers for social and cultural reasons. Although we used a high degree of commitment, persistence and diligence to establish a true story in each case, we realized that there were in fact highly suspicious cases of suicide by burning for which all parties, including the patient, denied any suicide attempt. Thus, we believe our findings may well underrepresent the true picture of this social tragedy across our society.
Conclusion
The findings of this study show that suicidal behavior by burns is an important public health problem in the two bordering provinces of Ilam and Khorasan (particularly in Ilam). It is more common among the young and married female population. We believe that our study only shows the tip of the iceberg in demonstrating the scope of aggression and abuse against women, mainly young and married, in Iran. The majority of this cohort still suffers horrific and unbearable life situations and is at risk of attempting suicide. Such a social pathology is comparable to a “dead canary in a coal mine”. One of coal mining’s earliest systems for warning of the presence of methane gas was to send a canary down into the coal mine. Although low-tech, it was extremely effective and rather easy to read; if the bird died, miners had to immediately evacuate the shaft. As far as suicidal behaviour by burns is concerned, we believe that “the bird has died”, and that society, government agencies and the international community must act now. Our studies, as well as others from Iran suggest that despite substantial efforts toward improving health in Iran, persistent conditions permit violence against women, and Iranian women and girls continue to turn to the desperate remedy of self-burning. We acknowledge that addressing socio-cultural aspects of suicide in Iran requires time and resources, but we also believe that the time to act is now in order to protect and prevent more unnecessary deaths.
Acknowledgments
Ethical approval. Obtained.
Conflict of interest. The authors declare they have no conflicts of interest.
Funding. None.
Contributions of authors. R Alaghehbandan was responsible for the design, data access, data analysis and interpretation, and drafting the study manuscript. NA Dinn was responsible for write up and editing of the study manuscript. AR Lari was responsible for the design, data access, reviewing and editing of the study manuscript.
References
- 1.O’Donoghue JM, Panchal JL, O’Sullivan ST, O’Shaughnessy M, O’Connor TP, Keeley H, Kelleher MJ. A study of suicide and attempted suicide by self-immolation in an Irish psychiatric population: an increasing problem. Burns. 1998;24:144–6. doi: 10.1016/s0305-4179(97)00096-x. [DOI] [PubMed] [Google Scholar]
- 2.Greenbaum AR, Donne J, Wilson D, Dunn KW. Intentional burn injury: An evidence-based, clinical and forensic review. Burns. 2004;30:628–42. doi: 10.1016/j.burns.2004.03.019. [DOI] [PubMed] [Google Scholar]
- 3.Cameron DR, Pegg SP, Muller M. Self-inflicted burns. Burns. 1997;23:519–21. doi: 10.1016/s0305-4179(97)00039-9. [DOI] [PubMed] [Google Scholar]
- 4.Wallace KL, Pegg SP. Self-inflicted burn injuries: An 11-year retrospective study. J Burn Care Rehabil. 1999;20:191–4. [PubMed] [Google Scholar]
- 5.Hahn AP, Jochai D, Caufield-Noll CP, Hunt CA, Allen LE, Rios R, Cordts GA. Self-inflicted burns: A systematic review of the literature. J Burn Care Res. 2014;35:102–19. doi: 10.1097/BCR.0b013e31828b0a46. [DOI] [PubMed] [Google Scholar]
- 6.Laloë V. Patterns of deliberate self-burning in various parts of the world. A review. Burns. 2004;30:207–15. doi: 10.1016/j.burns.2003.10.018. [DOI] [PubMed] [Google Scholar]
- 7.Thombs BD, Bresnick MG, Russell GM. Who attempts suicidesuicide by burning? An analysis of age patterns of mortality by self-inflicted burning in the United States. Gen Hosp Psychiatry. 2007;29:244–50. doi: 10.1016/j.genhosppsych.2007.01.012. [DOI] [PubMed] [Google Scholar]
- 8.Cave Bondi G, Cipolloni L, Parroni E, Cecchi R. A review of suicides by burning in Rome between 1947 and 1997 examined by the Pathology Department of the Institute of Forensic Medicine, University of Rome ‘La Sapienza’. Burns. 2001;27:227–31. doi: 10.1016/s0305-4179(00)00108-x. [DOI] [PubMed] [Google Scholar]
- 9.Rastegar Lari A, Alaghehbandan R. Epidemiological study of selfinflicted burns in Tehran, Iran. J Burn Care Rehabil. 2003;24:15–20. doi: 10.1097/00004630-200301000-00005. [DOI] [PubMed] [Google Scholar]
- 10.Zarghami M, Khalilian A. Deliberate self-burning in Mazandaran, Iran. Burns. 2002;28:115–9. doi: 10.1016/s0305-4179(01)00092-4. [DOI] [PubMed] [Google Scholar]
- 11.Maghsoudi H, Garadagi A, Jafary GA, Azarmir G, Aali N, Karimian B, Tabrizi M. Women victims of self-inflicted burns in Tabriz, Iran. Burns. 2004;30:217–20. doi: 10.1016/j.burns.2003.10.010. [DOI] [PubMed] [Google Scholar]
- 12.Saadat M, Zendeh-Boodi Z. Correlation between incidences of self-inflicted burns and means of inbreeding coefficients, an ecologic study. Ann Epidemiol. 2006;16:708–11. doi: 10.1016/j.annepidem.2005.12.006. [DOI] [PubMed] [Google Scholar]
- 13.Groohi B, Rossignol AM, Barrero SP, Alaghehbandan R. Suicidal behavior by burns among adolescents in Kurdistan, Iran: a social tragedy. Crisis. 2006;27:16–21. doi: 10.1027/0227-5910.27.1.16. [DOI] [PubMed] [Google Scholar]
- 14.Ahmadi A. Suicide by self-immolation: Comprehensive overview, experiences and suggestions. J Burn Care Res. 2007;28:30–41. doi: 10.1097/BCR.0b013E31802C8878. [DOI] [PubMed] [Google Scholar]
- 15.Lari AR, Joghataei MT, Adli YR, Zadeh YA, Alaghehbandan R. Epidemiology of suicide by burns in the province of Isfahan, Iran. J Burn Care Res. 2007;28:307–11. doi: 10.1097/BCR.0B013E318031A27F. [DOI] [PubMed] [Google Scholar]
- 16.Ahmadi A, Ytterstad B. Prevention of self-immolation by community-based intervention. Burns. 2007;33:1032–40. doi: 10.1016/j.burns.2006.11.015. [DOI] [PubMed] [Google Scholar]
- 17.Ahmadi A, Mohammadi R, Stavrinos D, Almasi A, Schwebel DC. Self-immolation in Iran. J Burn Care Res. 2008;29:451–60. doi: 10.1097/BCR.0b013e31817112f1. [DOI] [PubMed] [Google Scholar]
- 18.Mohammadi AA, Danesh N, Sabet B, Amini M, Jalaeian H. Selfinflicted burn injuries in southwest Iran. J Burn Care Res. 2008;29:778–83. doi: 10.1097/BCR.0b013e31818481ac. [DOI] [PubMed] [Google Scholar]
- 19.Rastegar Lari A, Alaghehbandan R, Panjeshahin MR, Joghataei MT. Suicidal behavior by burns in the province of Fars, Iran: A socio-epidemiologic approach. Crisis. 2009;30:98–101. doi: 10.1027/0227-5910.30.2.98. [DOI] [PubMed] [Google Scholar]
- 20.Groohi B, Alaghehbandan R, Lari AR. Analysis of 1089 burn patients in province of Kurdistan, Iran. Burns. 2002;28:569–74. doi: 10.1016/s0305-4179(02)00099-2. [DOI] [PubMed] [Google Scholar]
- 21.Ahmadi A, Mohammadi R, Schwebel DC, Yeganeh N, Soroush A, Bazargan-Hejazi S. Familial risk factors for self-immolation: A case-control study. J Womens Health (Larchmt) 2009;18:1025–31. doi: 10.1089/jwh.2008.1192. [DOI] [PubMed] [Google Scholar]
- 22.Saadat M, Bahaoddini A, Mohabatkar H, Noemani K. High incidence of suicide by burning in Masjid-i-Sulaiman (southwest of Iran), a polluted area with natural sour gas leakage. Burns. 2004;30:829–32. doi: 10.1016/j.burns.2004.06.003. [DOI] [PubMed] [Google Scholar]
- 23.Raj A, Gomez C, Silverman JG. Driven to a fiery death—the tragedy of self-immolation in Afghanistan. N Engl J Med. 2008;358:2201–3. doi: 10.1056/NEJMp0801340. [DOI] [PubMed] [Google Scholar]
- 24.Othman N. Suicide by self-burning in Iraqi Kurdistan: Description and risk factors. Arch Suicide Res. 2011;15:238–49. doi: 10.1080/13811118.2011.589717. [DOI] [PubMed] [Google Scholar]
- 25.Chan RC, Burd A. Suicidal burn in Hong Kong. Burns. 2012;38:937–41. doi: 10.1016/j.burns.2012.01.009. [DOI] [PubMed] [Google Scholar]
- 26.Peck MD. Epidemiology of burns throughout the World. Part II: intentional burns in adults. Burns. 2012;38:630–7. doi: 10.1016/j.burns.2011.12.028. [DOI] [PubMed] [Google Scholar]
- 27.Akbari ME, Naghavi M, Soori H. Epidemiology of deaths from injuries in the Islamic Republic of Iran. East Mediterr Health J. 2006;12:382–90. [PubMed] [Google Scholar]