

Abstract
The primary factor that determines the success of implant is the amount of available bone in the edentulous site. Diagnostic imaging and techniques help to develop and implement a cohesive and comprehensive treatment plan according to the available bone. In the following case report an innovative simplified method (poor man CT) is used to fabricate a three dimensional model to assess the available bone for implant placement in mandible.
Keywords: Extraoral impression, intraoral impression, three-dimensional model
INTRODUCTION
Many imaging options have been recommended for implant treatment planning. However, neither buccolingual width nor angulation can be properly visualized on the most traditional radiographs.[1] In the following case report, an innovative simplified method without radiation is used to fabricate a three-dimensional model to assess the available bone for implant placement in the mandible. Even a minor variation in comparison to ideal placement causes difficulties in fabrication of final prostheses.[2,3] Three-dimensional model achieved can be used to fabricate surgical guide. The surgical guide is essential to establish a logical continuity among diagnosis, prosthetic planning, and surgical phase.
CASE REPORT
A patient of age 27 years reported to the Department of Prosthodontics for the replacement of missing left first molar. Following steps were performed to achieve a three-dimensional model:
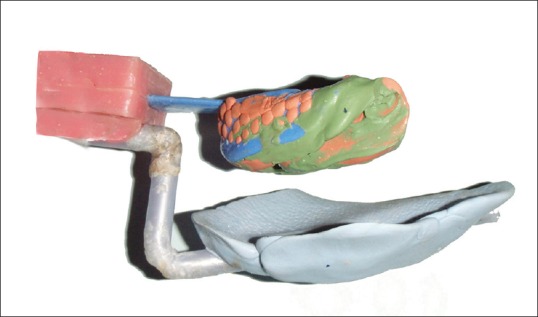
Intraoral impression was recorded with addition silicone putty and light body [Figure 1]
-
Fabrication of acrylic assembly for aligning both intraoral and extraoral impression
A rectangular block of acrylic was made to which impression tray was pressed to make indentations. After applying separating medium, the counter block of acrylic was made to which extraoral impression was attached [Figure 2]. In prototype, [Figures 2–4] plastic rod was used for supporting the extraoral impression
Replacing the plastic rod with metal plate and key system The plastic rod was replaced by a metal plate in the first generation [Figure 5] for better stability and better customization. A key system was incorporated to adjust the length and angulation according to each patient's mandible. On the top of the metal plate, acrylic was adapted. Addition silicone putty placed on the acrylic plate can be customized each time to record the extraoral impression. The extraoral impression should record the lower border of the mandible to the medial extent as much as possible [Figure 6]
Fabrication of three-dimensional model The intraoral impression was poured first to get a cast. After the initial setting was over, the entire assembly was poured, and a three dimensional model of the mandible was fabricated [Figure 7].
Figure 1.

Intraoral impression with acrylic assembly
Figure 2.
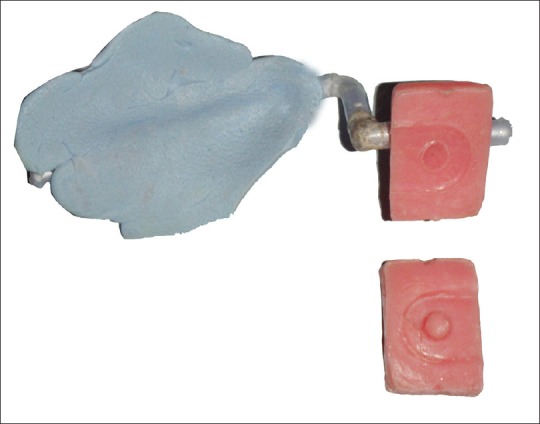
Prototype (extraoral impression)
Figure 4.

Prototype model
Figure 5.
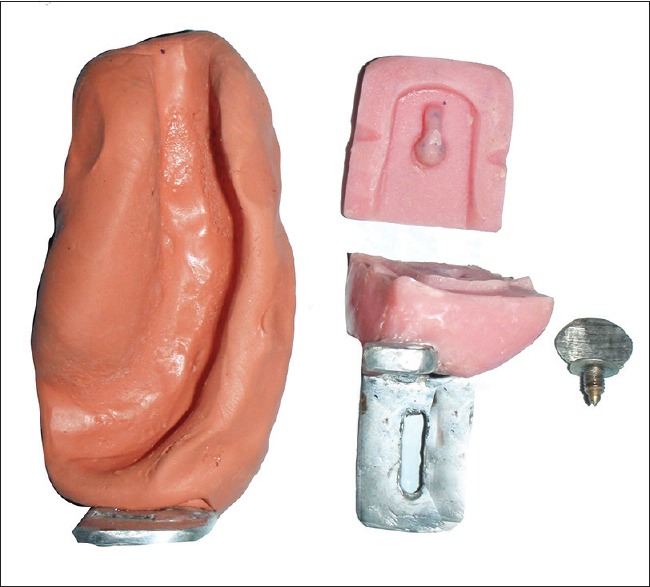
First generation metal plate
Figure 6.
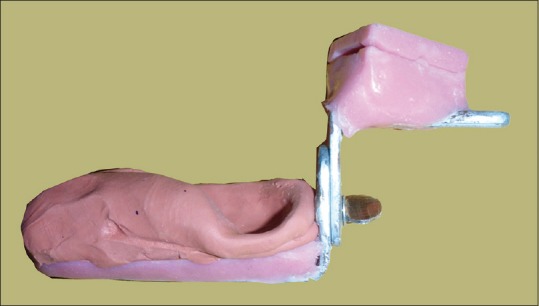
Assembled metal frame
Figure 7.

Three-dimensional model
Figure 3.
Prototype - Extraoral and intraoral impression together with acrylic assembly
The accuracy of this method was verified with computed tomography (CT) scan. The cross section where the mandibular premolar teeth were disappearing from the CT image was taken (14 mm depth) as a reference and measured to get the available bone width buccolingually (8.7 mm). This measurement was same when compared with the available bone in the sectioned cast at the premolar area, at a depth of 14 mm (premolar root length).
On the three-dimensional model, the surgical guide was fabricated [Figure 8]. This surgical template can dictate the implant body placement that offers the best combination of support for the repetitive forces of occlusion and esthetics.
Figure 8.

Three-dimensional model with surgical guide
This article had won the best table clinic award in 35th IPS conference conducted in New Delhi 2007 by Army Dental Corps.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
Aman Arora.
REFERENCES
- 1.Garg AK, Vicari A. Radiographic modalities for diagnosis and treatment planning in implant dentistry. Implant Soc. 1995;5:7–11. [PubMed] [Google Scholar]
- 2.Widmann G, Bale RJ. Accuracy in computer-aided implant surgery – A review. Int J Oral Maxillofac Implants. 2006;21:305–13. [PubMed] [Google Scholar]
- 3.Takeshita F, Suetsugu T. Accurate presurgical determination for implant placement by using computerized tomography scan. J Prosthet Dent. 1996;76:590–1. doi: 10.1016/s0022-3913(96)90434-5. [DOI] [PubMed] [Google Scholar]