

Abstract
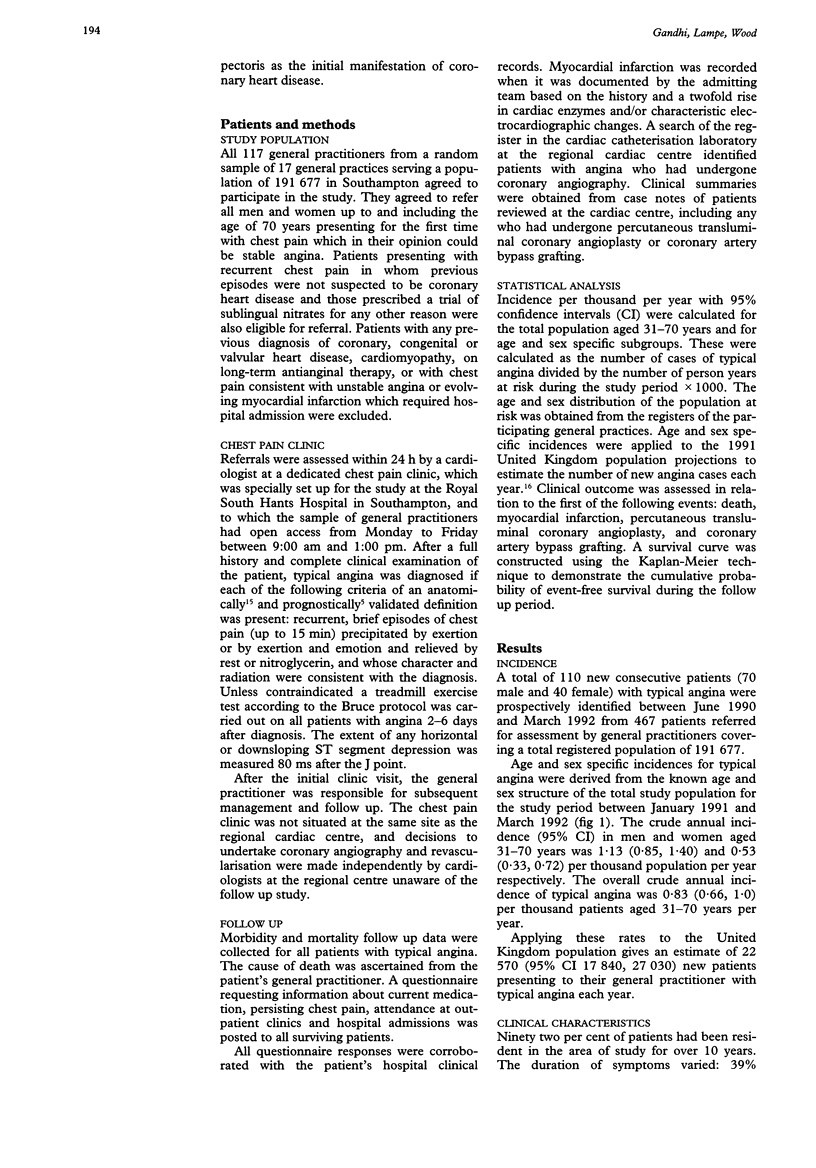
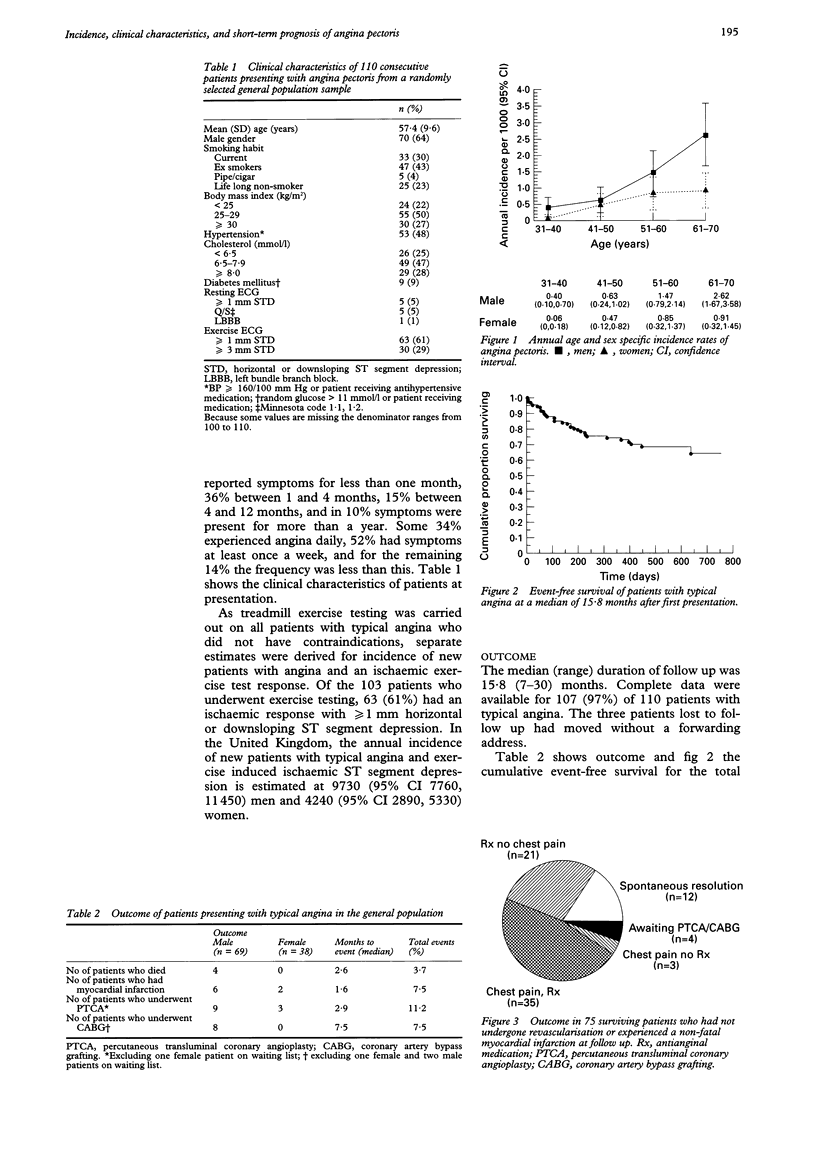
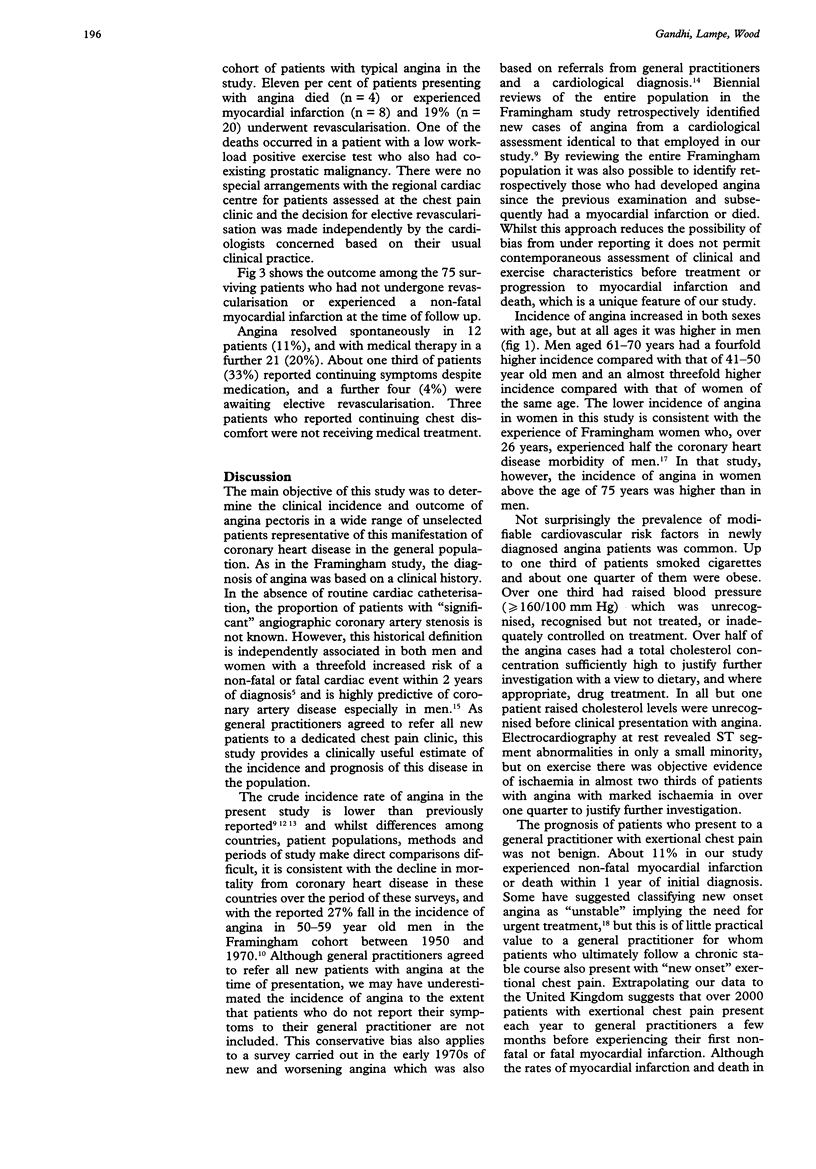
OBJECTIVES--To estimate the clinical incidence and short-term prognosis of patients presenting with typical angina pectoris in the general population. DESIGN--Prospective survey of all patients referred by 117 general practitioners from a random sample of 17 general practices serving a population of 191,677 with a median follow up of 16 months. SETTING--A special open access chest pain clinic, based in the non-invasive cardiology department of a teaching hospital, set up for this study. PATIENTS--110 consecutive patients < or = 70 years age with no history of coronary heart disease presenting for the first time with typical angina. MAIN OUTCOME MEASURES--Age and sex specific incidences, persistence of chest pain, revascularisation procedures, myocardial infarction, and death. RESULTS--The crude annual incidence of angina pectoris (95% confidence interval) was 0.83 (0.66 to 1.0) per thousand population aged 31-70 years; the rates were 1.13 (0.85 to 1.40) for men and 0.53 (0.33 to 0.72) for women. On resting electrocardiography 5% of patients had > or = 1 mm horizontal or downsloping ST depression, 5% had Q/QS patterns, and in one (1%) there was complete left bundle branch block. Among the 103 patients who underwent a Bruce protocol exercise test, 29% had > or = 3 mm ST segment depression induced at a low workload. Of 107 patients at a median (range) follow up of 15.8 (7-30) months, angina remitted spontaneously in 12 patients (11%), 20 (19%) underwent revascularisation, eight (7%) sustained a non-fatal myocardial infarction, and four (4%) died. CONCLUSION--Incidence of new cases of angina pectoris in the United Kingdom is conservatively estimated from this study to be 22,600 patients per annum. Almost one third of these patients will have positive exercise tests at low workload, so the potential for coronary angiography and revascularisation is considerable. With one in 10 patients experiencing a non-fatal myocardial infarction or coronary death within a year of presentation the prognosis of angina is not benign. Further research is required to identify those patients in the general population who would benefit most from coronary revascularisation.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Braunwald E. Unstable angina. A classification. Circulation. 1989 Aug;80(2):410–414. doi: 10.1161/01.cir.80.2.410. [DOI] [PubMed] [Google Scholar]
- Bulpitt C. J., Shipley M. J., Demirovic J., Ebi-Kryston K. L., Markowe H. L., Rose G. Predicting death from coronary heart disease using a questionnaire. Int J Epidemiol. 1990 Dec;19(4):899–904. doi: 10.1093/ije/19.4.899. [DOI] [PubMed] [Google Scholar]
- Cannon P. J., Connell P. A., Stockley I. H., Garner S. T., Hampton J. R. Prevalence of angina as assessed by a survey of prescriptions for nitrates. Lancet. 1988 Apr 30;1(8592):979–981. doi: 10.1016/s0140-6736(88)91790-4. [DOI] [PubMed] [Google Scholar]
- Duncan B., Fulton M., Morrison S. L., Lutz W., Donald K. W., Kerr F., Kirby B. J., Julian D. G., Oliver M. F. Prognosis of new and worsening angina pectoris. Br Med J. 1976 Apr 24;1(6016):981–985. doi: 10.1136/bmj.1.6016.981. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fry J. The natural history of angina in a general practice. J R Coll Gen Pract. 1976 Sep;26(170):643–646. [PMC free article] [PubMed] [Google Scholar]
- Fulton M., Lutz W., Donald K. W., Kirby B. J., Duncan B., Morrison S. L., Kerr F., Julian D. G., Oliver M. F. Natural history of unstable angina. Lancet. 1972 Apr 22;1(7756):860–865. doi: 10.1016/s0140-6736(72)90737-4. [DOI] [PubMed] [Google Scholar]
- Garg R., Madans J. H., Kleinman J. C. Regional variation in ischemic heart disease incidence. J Clin Epidemiol. 1992 Feb;45(2):149–156. doi: 10.1016/0895-4356(92)90007-a. [DOI] [PubMed] [Google Scholar]
- Kannel W. B., Feinleib M. Natural history of angina pectoris in the Framingham study. Prognosis and survival. Am J Cardiol. 1972 Feb;29(2):154–163. doi: 10.1016/0002-9149(72)90624-8. [DOI] [PubMed] [Google Scholar]
- Kannel W. B., Sorlie P. D. Remission of clinical angina pectoris: the Framingham study. Am J Cardiol. 1978 Jul;42(1):119–123. doi: 10.1016/0002-9149(78)90995-5. [DOI] [PubMed] [Google Scholar]
- Lerner D. J., Kannel W. B. Patterns of coronary heart disease morbidity and mortality in the sexes: a 26-year follow-up of the Framingham population. Am Heart J. 1986 Feb;111(2):383–390. doi: 10.1016/0002-8703(86)90155-9. [DOI] [PubMed] [Google Scholar]
- Medalie J. H., Goldbourt U. Angina pectoris among 10,000 men. II. Psychosocial and other risk factors as evidenced by a multivariate analysis of a five year incidence study. Am J Med. 1976 May 31;60(6):910–921. doi: 10.1016/0002-9343(76)90921-9. [DOI] [PubMed] [Google Scholar]
- Murabito J. M., Anderson K. M., Kannel W. B., Evans J. C., Levy D. Risk of coronary heart disease in subjects with chest discomfort: the Framingham Heart Study. Am J Med. 1990 Sep;89(3):297–302. doi: 10.1016/0002-9343(90)90341-a. [DOI] [PubMed] [Google Scholar]
- Murphy J. J., Connell P. A., Hampton J. R. Predictors of risk in patients with unstable angina admitted to a district general hospital. Br Heart J. 1992 May;67(5):395–401. doi: 10.1136/hrt.67.5.395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rose G., Baxter P. J., Reid D. D., McCartney P. Prevalence and prognosis of electrocardiographic findings in middle-aged men. Br Heart J. 1978 Jun;40(6):636–643. doi: 10.1136/hrt.40.6.636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shaper A. G., Cook D. G., Walker M., Macfarlane P. W. Prevalence of ischaemic heart disease in middle aged British men. Br Heart J. 1984 Jun;51(6):595–605. doi: 10.1136/hrt.51.6.595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith W. C., Kenicer M. B., Tunstall-Pedoe H., Clark E. C., Crombie I. K. Prevalence of coronary heart disease in Scotland: Scottish Heart Health Study. Br Heart J. 1990 Nov;64(5):295–298. doi: 10.1136/hrt.64.5.295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sytkowski P. A., Kannel W. B., D'Agostino R. B. Changes in risk factors and the decline in mortality from cardiovascular disease. The Framingham Heart Study. N Engl J Med. 1990 Jun 7;322(23):1635–1641. doi: 10.1056/NEJM199006073222304. [DOI] [PubMed] [Google Scholar]
- The investigation and management of stable angina. Report of a working party of the Joint Audit Committee of the British Cardiac Society and the Royal College of Physicians of London. J R Coll Physicians Lond. 1993 Jul;27(3):267–273. [PMC free article] [PubMed] [Google Scholar]
- Varnauskas E. Twelve-year follow-up of survival in the randomized European Coronary Surgery Study. N Engl J Med. 1988 Aug 11;319(6):332–337. doi: 10.1056/NEJM198808113190603. [DOI] [PubMed] [Google Scholar]
- Weiner D. A., Ryan T. J., McCabe C. H., Kennedy J. W., Schloss M., Tristani F., Chaitman B. R., Fisher L. D. Exercise stress testing. Correlations among history of angina, ST-segment response and prevalence of coronary-artery disease in the Coronary Artery Surgery Study (CASS). N Engl J Med. 1979 Aug 2;301(5):230–235. doi: 10.1056/NEJM197908023010502. [DOI] [PubMed] [Google Scholar]