

Abstract
Background
Pregnancy-related low back pain is a common condition during pregnancy. Kinesio tape is a drug-free elastic therapeutic tape used for treating various musculoskeletal problems. The aim of this study was to investigate the short-term effects of lumbar Kinesio taping on pain intensity and disability in women with pregnancy-related low back pain.
Material/Methods
A total of 65 patients with pregnancy-related low back pain were randomly allocated into either Kinesio taping (n=33) or control (n=32) groups. The intervention group was treated with paracetamol plus Kinesio taping, while the control group received only paracetamol. Kinesio taping was applied in the lumbar flexion position, and four I-shaped bands were used. Two bands were attached horizontally, with space correction technique. The remaining 2 bands, 1 on each side of the lumbar spine, were placed vertically, with inhibition technique. Low back pain intensity was measured on a 10-cm visual analogue scale (VAS), and the Roland-Morris Disability Questionnaire (RMDQ) was used for evaluation of disability.
Results
Pain intensity and RMDQ scores improved significantly in both groups at 5 days compared with baseline. Considering the degree of treatment effect (the change from baseline to day 5), the Kinesio taping group was significantly superior than the control group in all outcome measures (for all, P<0.001).
Conclusions
The results of this study indicate that Kinesio taping can be used as a complementary treatment method to achieve effective control of pregnancy-related low back pain.
MeSH Keywords: Disability Evaluation; Kinesiology, Applied; Low Back Pain
Background
Low back pain is a common condition during pregnancy, affecting more than two-thirds of pregnant women [1]. However, prevalence estimates vary among studies due to different definitions and study methodologies [2]. It has been reported that low back pain affects between 45% and 75% of women at some time during their pregnancy [3].
Pregnancy-related low back pain can be classified as lumbar pain, pelvic girdle pain, or their combination [4]. While low back pain is experienced between the twelfth rib and the gluteal fold, pelvic girdle pain occurs between the posterior iliac crest and the gluteal fold [2,4]. However, most of the literature does not distinguish between low back pain and pelvic girdle pain [5].
Although pregnancy-related low back pain may be due to changes in ligament laxity and posture, there are several causes of low back pain during pregnancy, including lumbosacral disc herniation, musculoskeletal diseases, pregnancy-related osteoporosis, and sacral stress fractures [4,6]. In addition, studies have shown that pregnancy-related low back pain is associated with poor quality of life, sleep disturbances, and sick leave from work [1,3], but it is often accepted as a normal, painful process of pregnancy [3,7] because patients and clinicians have inadequate information about treatment options and fear of possible harmful effects of treatment on the developing fetus [1,3,5].
Kinesio tape is a drug-free elastic therapeutic tape used for treating various musculoskeletal problems such as injury, pain, dysfunction, and a variety of other disorders [8,9]. Kinesio taping applications were created by a Japanese chiropractor, Dr Kenso Kase, in the 1970s. Although the exact mechanisms of the effects are not yet clear, some investigators claimed that Kinesio taping has multiple functions: 1) supporting injured muscles and joints; 2) improvement of fascia function and position; 3) increasing segmental stability; 4) activation of the blood and lymph flow by lifting the skin; and 5) deactivation of the pain by reducing nociceptive stimuli [8–10].
Although some studies have examined the effects of Kinesio taping application in non-pregnant patients with non-specific low back pain [10–13], there is very little clinical experience and only limited documentation for effectiveness of Kinesio taping on pregnancy-related low back pain. Because the existing treatments for pregnancy-related low back pain are not adequately known and are not found to be reliable by patients and clinicians, Kinesio taping may be a potential treatment if it is an effective and tolerable method. Therefore, the aim of the present study was to determine the influence of Kinesio taping on pregnancy-related low back pain.
Material and Methods
The present study was performed on pregnant women applying to the obstetrics outpatient clinic of a university hospital between July 27, 2015 and December 1, 2015. The study protocol was approved by the university’s ethics review board (23.07.2015/05). Written informed consent was obtained from all participants prior to their involvement.
This was a short-term, prospective, observer-blinded, randomized controlled study with 2 measurement points (baseline and day 5). All participants were randomly assigned to 2 treatment groups and were assessed by an observer blinded to the treatment group assignments. In both groups, the low back pain severity was measured on a visual analogue scale (VAS), and the scores of the Turkish version of the Roland-Morris Disability Questionnaire (RMDQ) were used for evaluation of functional ability and disability [14]. The VAS consisted of a 10-cm line scale from 0 to 10. The 0-cm end corresponded to ‘no pain’, while the 10-cm end represented the ‘worst pain ever’. We provided an explanation of the VAS to each patient before the treatment. The VAS scores of the 2 groups were evaluated after resting for 5 minutes and after 5 minutes of movement. Clinical improvement over time can be graded based on the analysis of serial RMDQ scores. For example, if a patient’s baseline score was 10 and at the end of treatment her score was 2 (8 points of improvement), we would calculate an 80% (8/10×100) improvement.
All participants were given paracetamol (Parol®, Atabay, Turkey) 1500 mg/day for 5 days. The control group received no additional treatment, while the intervention group received 5 days of additional Kinesio taping therapy. Kinesio tape is an elastic waterproof bandage with acrylic adhesive produced from a special material that allows motion. All participants in the Kinesio taping group were taped by the same physician. Kinesio taping was applied when the lumbar flexion reached its maximum point. Four I-shaped Kinesio bands (Kinesio tape®, Libor, Turkey) with a width of 5 cm and thickness of 0.5 mm were used. Two bands, 1 on each side of the lumbar spine, were applied vertically from the lower posterior iliac crest region to the upper twelfth rib region, with inhibition technique. The remaining 2 bands were attached horizontally, with space correction technique. All 4 bands were placed to allow for 50% longitudinal stretching. The stretching directions for the vertical and horizontal applications were bottom-up and sideways, respectively (Figure 1). The aim of these applications was to relieve both lumbar and pelvic girdle pain.
Figure 1.
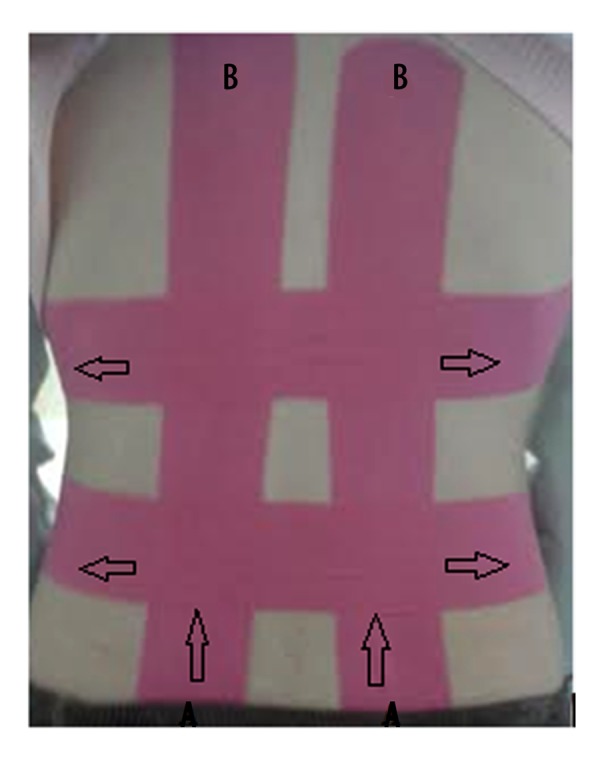
Application of Kinesio taping. A. Starting location. B. Ending location. Arrows show the stretching directions for the vertical and horizontal applications.
Inclusion criteria for the study were maternal age between 18 and 40 years, any parity, gestational age between 10 and 30 weeks, low back pain experienced anywhere from T12 to the gluteal fold without leg pain, and at least moderate pain intensity (scoring ≥4 on VAS). Exclusion criteria were known or suspected orthopedic or rheumatologic disorders including scoliosis, spine injuries, ankylosing spondylitis or rheumatoid arthritis; intervertebral disc pathology; a history of low back pain prior to pregnancy; twin pregnancy or fetal anomaly; and any uncontrolled medical condition.
Statistical analyses were performed using SPSS for Windows (version 16.0, SPSS Inc., Chicago, Illinois, USA), with statistical significance set at P<0.05. The normality of continuous variables was analyzed using Kolmogorov-Smirnov test. The t test was used for the comparison of normally distributed continuous variables between the groups, while the Mann-Whitney U test for variables with non-normal distribution. In the intra-group comparisons of continuous variables, the paired t test was used for normally distributed variables, while the Wilcoxon test was used for variables with non-normal distribution.
Results
Figure 2 is a flow diagram showing the design of the study and participants’ distribution between groups. Out of the 120 pregnant women with low back pain, 71 met the selection criteria and were randomly allocated to the Kinesio taping (n=36) or control group (n=35). Due to local allergic reaction to Kinesio tape, 2 patients in the Kinesio taping group did not complete the study. Additionally, 1 patient in the Kinesio taping group and 2 patients in the control group failed to come to their follow-up visit at day 5. As result, out of all eligible cases (n=71), 65 patients completed the study, and only their data were included in the statistical analysis.
Figure 2.
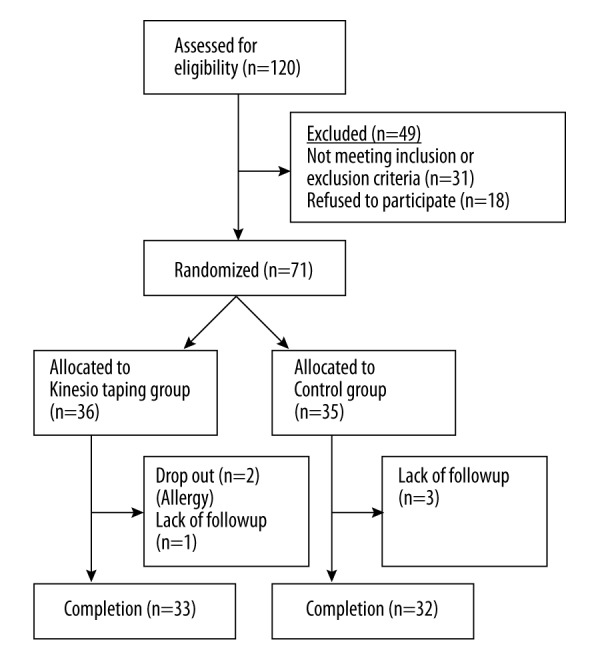
Flow of study participants.
There were no significant differences between the groups with regards to participant age, parity, gravidas, week of gestation, or body mass index at baseline (for all P>0.05) (Table 1). At study entry, the pain intensity during rest, pain intensity during movement, and functional ability scores were comparable between the 2 groups (P=0.357, P=0.590, and P=0.085, respectively) (Table 2).
Table 1.
Baseline characteristics of participants.
| KT group (n=33) | Control group (n=32) | P | |
|---|---|---|---|
| Age, y | 24.30 (4.96) | 25.09 (4.95) | 0.522 |
| Parity | 1.06 (1.12) | 1.41 (1.36) | 0.267 |
| Gravidas | 2.36 (1.64) | 2.72 (1.49) | 0.363 |
| Gestation, wk | 21.79 (5.47) | 21.91 (3.86) | 0.920 |
| BMI | 26.50 (3.46) | 25.60 (3.08) | 0.121 |
BMI – body mass index (kg/m2); KT – kinesio taping. Values are given as mean (standard deviation).
Table 2.
Pain intensity and functional ability.
| KT group (n=33) | Control group (n=32) | P1 | |
|---|---|---|---|
| VAS (rest) | |||
| Baseline | 7.57 (1.49) (4–9) | 7.27 (1.13) | 0.357 |
| Fifth day | 1.36 (1.98) (0–8.2) | 3.28 (1.71) | |
| Difference | 6.21 (2.06) | 3.98 (1.48) | <0.001 |
| P2 | <0.001 | <0.001 | |
| VAS (motion) | |||
| Baseline | 7.63 (1.18) (5–9) | 7.46 (1.32) (5–9.9) | 0.590 |
| Fifth day | 1.26 (1.81) (0–6.5) | 3.25 (1.48) (1–7) | |
| Difference | 6.37 (1.96) | 4.21 (1.71) | <0.001 |
| P2 | <0.001 | <0.001 | |
| RMDQ | |||
| Baseline | 13.42 (3.82) (7–23) | 15.03 (3.56) | 0.085 |
| Fifth day | 3.85 (3.01) (1–15) | 7.78 (2.95) | |
| Improvement (%) | 70.30 (22.78) (9.1–95.7) | 48.45 (14.32) (16.7–75.0) | <0.001 |
| P2 | <0.001 | <0.001 | |
KT – kinesio taping; VAS – visual analogue scale; RMDQ – Roland-Morris Disability Questionnaire. P1 – difference at baseline or difference in change between groups; P2 – difference in each group at baseline and fifth day. Values are given as mean (standard deviation) when used the parametric test, and given as mean (standard deviation) (min.-max.) when used the non-parametric test.
In both groups, all the outcome measures (pain intensity during rest, pain intensity during movement, and Roland-Morris Disability Questionnaire) were significantly reduced at day 5 compared with baseline (for all P<0.001). Nevertheless, considering the change data from baseline to day 5, the Kinesio tape group was significantly superior than the control group in all the outcome measures (for all P<0.001) (Table 2).
Discussion
According to the results of this single-blind, randomized, controlled study, Kinesio taping added to the classical analgesic therapy of paracetamol is more effective than the paracetamol therapy alone in improving pain and disability in the treatment of pregnancy-related low back pain. Kinesio taping for 5 days was generally well tolerated by the pregnant women, and there were no serious adverse events except a few local allergic reactions resulting from the Kinesio tape.
As low back pain is a condition with high incidence and prevalence in the general population, pregnancy-related low back pain is common during pregnancy [1,11]. Studies provide conflicting results for the effect of Kinesio taping on pain and disability outcomes in non-pregnant patients with low back pain [10–13]. However, we were able to find only anecdotal evidence on the application of Kinesio taping in pregnancy-related low back pain [1]. Therefore, our study provides a valuable contribution to the existing literature regarding the subject, and can guide future studies.
Although the actual pathophysiologic mechanism of pregnancy-related low back pain is not precisely known, it may result from changes in ligament laxity and posture during pregnancy [4]. It may also be related to previous pregnancies and deliveries, hormonal contraceptive use before first pregnancy, physically demanding work, and emotional distress [15]. Pregnancy-related low back pain is related to poor quality of life, decreased sleep quality, and sick leave from work [1,3]. Despite these negative effects, pregnancy-related low back pain is often accepted as a natural, painful process of pregnancy [3,7]. This may be due to inadequate knowledge about treatment options and concerns about the impact of some medications on the developing fetus [1,3,5]. Given that patients and clinicians tend to avoid pharmacological treatment during pregnancy, Kinesio taping, which is a drug-free and safe alternative, appears to be an acceptable treatment option for the management of pregnancy-related low back pain.
There are several treatment options for pregnancy-related low back pain, such as multi-modal intervention (manual therapy, exercise and education), craniosacral therapy, osteomanipulative therapy, and acupuncture, although exercise, in a variety of formats, is the most frequently used intervention [1,3]. However, a recent systematic review has reported that the level of evidence is low for exercises, while the evidence is strong for positive effects of acupuncture and pelvic belts [16]. Although both treatment groups in the current study demonstrated significant improvement, the combination of Kinesio taping and paracetamol provided an optimizing treatment that can minimize the development of chronic pain, which accounts for serious costs related to low back pain. It has been proposed that Kinesio taping provides multiple benefits via multiple functions [8–10]. The effects of Kinesio taping on relieving pain were described by its inventor as including: changes in muscle activation, reduction of pain, joint repositioning, and reduction of abnormal muscular tension [9]. Kachanathu et al. [10] studied Kinesio taping in treatment of non-specific low back pain and reported a highly significant reduction in disability, measured using the RMDQ, in the Kinesio taping group. Kelle et al. [11] reported that Kinesio taping provided significant improvements in pain and disability of patients suffering from acute low back pain and commented that it can be used as a complementary method. Because of the changes in ligament laxity and posture during pregnancy [4], stability deteriorates and the center of gravity shifts as the body position changes. Therefore, the effectiveness of Kinesio taping application on the pain and disability in patients with pregnancy-related low back pain may be via supporting lumbosacral structures and increasing stability, reduction of paraspinal stress, and stimulation of connective tissues, resulting in pain relief.
There are some limitations in the present study. We did not use a sham taping application; therefore, the placebo effect of the procedure cannot be ignored. Indeed, the lack of literature on how taping relieves pain and assessment of pain with VAS score, which is a subjective tool, are the other important limitations. Another limitation of our study was that it studied short-term results, so we were unable to assess the long-term effects of Kinesio taping.
Conclusions
When compared with paracetamol therapy alone, combined Kinesio taping and paracetamol therapy seems to be more effective to reduce pain and improve functional ability in the treatment of pregnancy-related low back pain. Thus, we conclude that Kinesio taping can be used as a complementary treatment method to achieve effective control of pregnancy-related low back pain. However, our findings should be supported by further studies with better methodological quality, longer follow-up period, and larger sample size.
Footnotes
Competing interests
We declare that we have no conflicts of interest.
Source of support: Departmental sources
References
- 1.Liddle SD, Pennick V. Interventions for preventing and treating low-back and pelvic pain during pregnancy. Cochrane Database Syst Rev. 2015;9:CD001139. doi: 10.1002/14651858.CD001139.pub4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Vleeming A, Albert HB, Ostgaard HC, et al. European guidelines for the diagnosis and treatment of pelvic girdle pain. Eur Spine J. 2008;17(6):794–819. doi: 10.1007/s00586-008-0602-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bishop A, Holden MA, Ogollah RO, Foster NE EASE Back Study Team. Current management of pregnancy-related low back pain: A national cross-sectional survey of UK physiotherapists. Physiotherapy. 2016;102(1):78–85. doi: 10.1016/j.physio.2015.02.003. [DOI] [PubMed] [Google Scholar]
- 4.Kluge J, Hall D, Louw Q, et al. Specific exercises to treat pregnancy-related low back pain in a South African population. Int J Gynaecol Obstet. 2011;113(3):187–91. doi: 10.1016/j.ijgo.2010.10.030. [DOI] [PubMed] [Google Scholar]
- 5.Vermani E, Mittal R, Weeks A. Pelvic girdle pain and low back pain in pregnancy: A review. Pain Pract. 2010;10(1):60–71. doi: 10.1111/j.1533-2500.2009.00327.x. [DOI] [PubMed] [Google Scholar]
- 6.Deschamps Perdomo A, Tome-Bermejo F, Piñera AR, Alvarez L. Misdiagnosis of sacral stress fracture: An underestimated cause of low back pain in pregnancy? Am J Case Rep. 2015;16:60–64. doi: 10.12659/AJCR.892631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mota MJ, Cardoso M, Carvalho A, et al. Women’s experiences of low back pain during pregnancy. J Back Musculoskelet Rehabil. 2015;28(2):351–57. doi: 10.3233/BMR-140527. [DOI] [PubMed] [Google Scholar]
- 8.Mostafavifar M, Wertz J, Borchers J. A systematic review of the effectiveness of kinesio taping for musculoskeletal injury. Phys Sportsmed. 2012;40:33–40. doi: 10.3810/psm.2012.11.1986. [DOI] [PubMed] [Google Scholar]
- 9.Williams S, Whatman C, Hume PA, Sheerin K. Kinesio taping in treatment and prevention of sports injuries: A meta-analysis of the evidence for its effectiveness. Sports Med. 2012;42(2):153–64. doi: 10.2165/11594960-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 10.Kachanathu SJ, Alenazi AM, Seif HE, et al. Comparison between kinesio taping and a traditional physical therapy program in treatment of nonspecific low back pain. J Phys Ther Sci. 2014;26(8):1185–88. doi: 10.1589/jpts.26.1185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kelle B, Güzel R, Sakallı H. The effect of Kinesio taping application for acute non-specific low back pain: A randomized controlled clinical trial. Clin Rehabil. 2015 doi: 10.1177/0269215515603218. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 12.Luz MA, Júnior, Sousa MV, Neves LA, et al. Kinesio Taping® is not better than placebo in reducing pain and disability in patients with chronic non-specific low back pain: A randomized controlled trial. Braz J Phys Ther. 2015;19(6):482–90. doi: 10.1590/bjpt-rbf.2014.0128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Castro-Sánchez AM, Lara-Palomo IC, Matarán-Peñarrocha GA, et al. Kinesio Taping reduces disability and pain slightly in chronic non-specific low back pain: A randomised trial. J Physiother. 2012;58(2):89–95. doi: 10.1016/S1836-9553(12)70088-7. [DOI] [PubMed] [Google Scholar]
- 14.Küçükdeveci AA, Tennant A, Elhan AH, Niyazoglu H. Validation of the Turkish version of the Roland-Morris Disability Questionnaire for use in low back pain. Spine (Phila Pa 1976) 2001;26(24):2738–43. doi: 10.1097/00007632-200112150-00024. [DOI] [PubMed] [Google Scholar]
- 15.Thorell E, Kristiansson P. Pregnancy related back pain, is it related to aerobic fitness? A longitudinal cohort study. BMC Pregnancy Childbirth. 2012;12:30. doi: 10.1186/1471-2393-12-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Gutke A, Betten C, Degerskär K, et al. Treatments for pregnancy-related lumbopelvic pain: A systematic review of physiotherapy modalities. Acta Obstet Gynecol Scand. 2015;94(11):1156–67. doi: 10.1111/aogs.12681. [DOI] [PubMed] [Google Scholar]