

Abstract
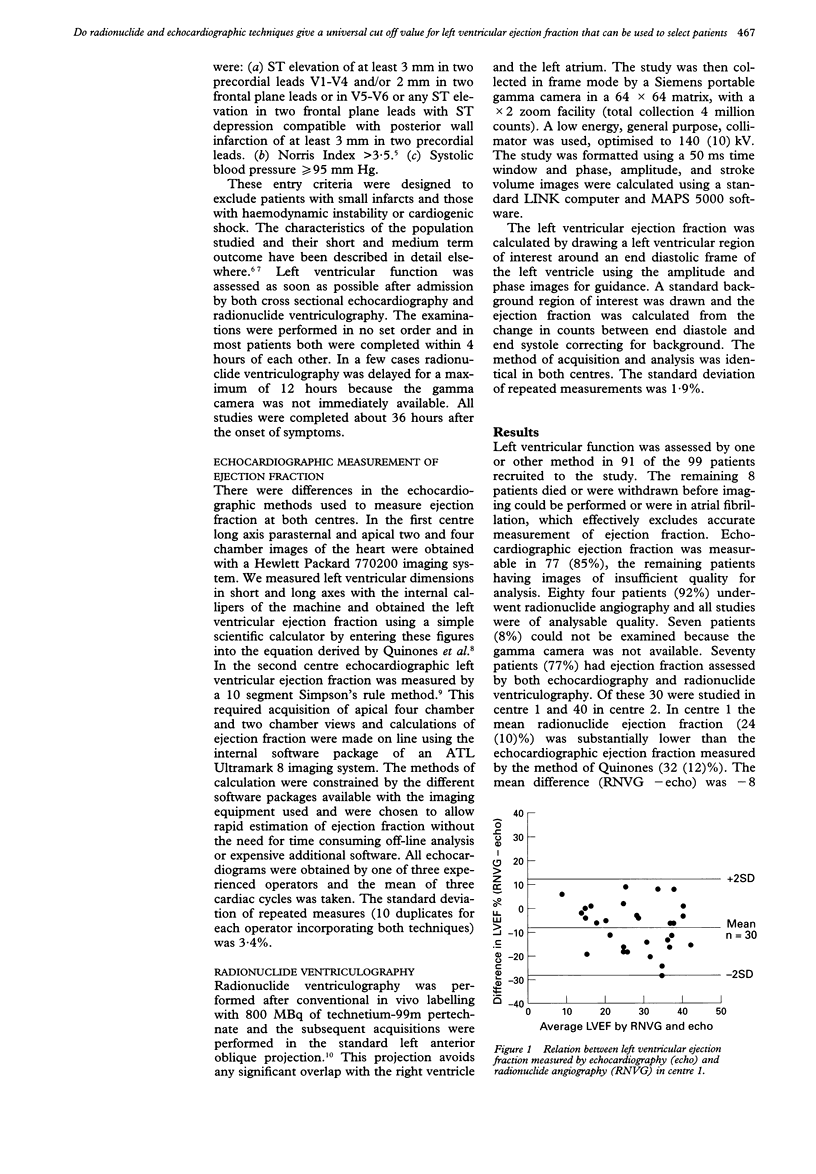
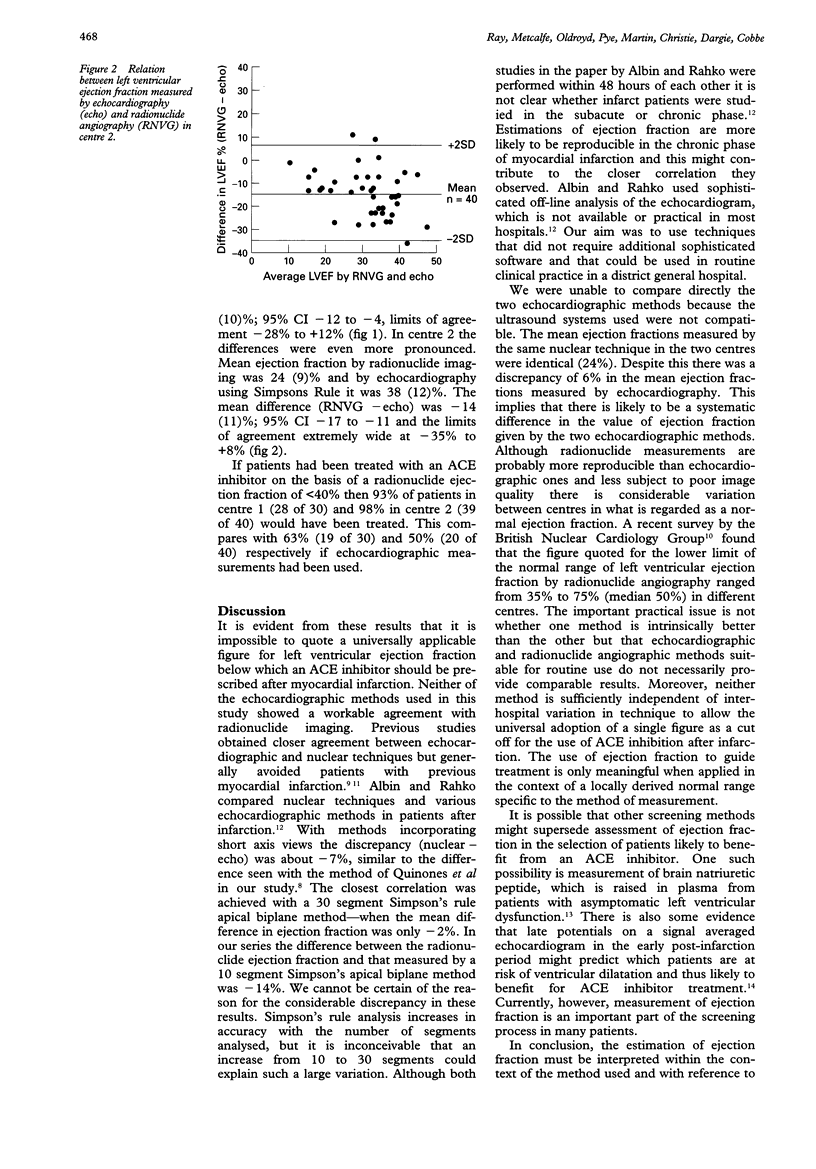
OBJECTIVE--To determine whether echocardiography and radionuclide angiography give comparable results when the left ventricular ejection fraction is measured early after myocardial infarction and thus whether, irrespective of the method used, a single value for the ejection fraction could be used as a guide for starting treatment with an angiotensin converting enzyme inhibitor. DESIGN--Prospective comparison of measurement of left ventricular ejection fraction by echocardiography and radionuclide angiography. SETTING--Coronary care units of two university teaching hospitals in Glasgow. PATIENTS--99 patients studied within 36 hours of acute myocardial infarction. OUTCOME MEASURES--Left ventricular ejection fraction assessed by echocardiography and radionuclide angiography. RESULTS--70 (77%) of the 99 patients had ejection fraction measured by both echocardiographic and radionuclide techniques, 30 in centre 1 and 40 in centre 2. In centre 1 the mean difference (SD) in ejection fraction (radionuclide angiography--echocardiography) was -8 (10%); 95% CI -12 to -4%. In centre 2 the mean difference was -14 (11%); 95% CI -17 to -11%. If patients had been treated with an ACE inhibitor on the basis of a radionuclide ejection fraction of < 40% then 93% in centre 1 (28 of 30) and 98% in centre 2 (39 of 40) would have been treated. This compares with 63% (19 of 30) and 50% (20 of 40), respectively if echocardiography had been used as a guide. CONCLUSION--Measurement of ejection fraction is highly dependent on the method used and it is therefore impossible to quote a universally applicable figure for left ventricular ejection fraction below which an ACE inhibitor should be used after myocardial infarction.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Albin G., Rahko P. S. Comparison of echocardiographic quantitation of left ventricular ejection fraction to radionuclide angiography in patients with regional wall motion abnormalities. Am J Cardiol. 1990 Apr 15;65(15):1031–1032. doi: 10.1016/0002-9149(90)91009-u. [DOI] [PubMed] [Google Scholar]
- Folland E. D., Parisi A. F., Moynihan P. F., Jones D. R., Feldman C. L., Tow D. E. Assessment of left ventricular ejection fraction and volumes by real-time, two-dimensional echocardiography. A comparison of cineangiographic and radionuclide techniques. Circulation. 1979 Oct;60(4):760–766. doi: 10.1161/01.cir.60.4.760. [DOI] [PubMed] [Google Scholar]
- McMurray J. ACE inhibitors after myocardial infarction. Lancet. 1993 Dec 4;342(8884):1418–1418. [PubMed] [Google Scholar]
- Motwani J. G., McAlpine H., Kennedy N., Struthers A. D. Plasma brain natriuretic peptide as an indicator for angiotensin-converting-enzyme inhibition after myocardial infarction. Lancet. 1993 May 1;341(8853):1109–1113. doi: 10.1016/0140-6736(93)93126-l. [DOI] [PubMed] [Google Scholar]
- Norris R. M., Brandt P. W., Caughey D. E., Lee A. J., Scott P. J. A new coronary prognostic index. Lancet. 1969 Feb 8;1(7589):274–278. doi: 10.1016/s0140-6736(69)91035-6. [DOI] [PubMed] [Google Scholar]
- Oldroyd K. G., Pye M. P., Ray S. G., Christie J., Ford I., Cobbe S. M., Dargie H. J. Effects of early captopril administration on infarct expansion, left ventricular remodeling and exercise capacity after acute myocardial infarction. Am J Cardiol. 1991 Sep 15;68(8):713–718. doi: 10.1016/0002-9149(91)90641-w. [DOI] [PubMed] [Google Scholar]
- Pfeffer M. A., Braunwald E., Moyé L. A., Basta L., Brown E. J., Jr, Cuddy T. E., Davis B. R., Geltman E. M., Goldman S., Flaker G. C. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction. Results of the survival and ventricular enlargement trial. The SAVE Investigators. N Engl J Med. 1992 Sep 3;327(10):669–677. doi: 10.1056/NEJM199209033271001. [DOI] [PubMed] [Google Scholar]
- Quinones M. A., Waggoner A. D., Reduto L. A., Nelson J. G., Young J. B., Winters W. L., Jr, Ribeiro L. G., Miller R. R. A new, simplified and accurate method for determining ejection fraction with two-dimensional echocardiography. Circulation. 1981 Oct;64(4):744–753. doi: 10.1161/01.cir.64.4.744. [DOI] [PubMed] [Google Scholar]
- Ray S. G., Pye M., Oldroyd K. G., Christie J., Connelly D. T., Northridge D. B., Ford I., Morton J. J., Dargie H. J., Cobbe S. M. Early treatment with captopril after acute myocardial infarction. Br Heart J. 1993 Mar;69(3):215–222. doi: 10.1136/hrt.69.3.215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Starling M. R., Crawford M. H., Sorensen S. G., Levi B., Richards K. L., O'Rourke R. A. Comparative accuracy of apical biplane cross-sectional echocardiography and gated equilibrium radionuclide angiography for estimating left ventricular size and performance. Circulation. 1981 May;63(5):1075–1084. doi: 10.1161/01.cir.63.5.1075. [DOI] [PubMed] [Google Scholar]
- Underwood R., Gibson C., Tweddel A., Flint J. A survey of nuclear cardiological practice in Great Britain. The British Nuclear Cardiology Group. Br Heart J. 1992 Mar;67(3):273–277. doi: 10.1136/hrt.67.3.273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zaman A. G., Morris J. L., Smyllie J. H., Cowan J. C. Late potentials and ventricular enlargement after myocardial infarction. A new role for high-resolution electrocardiography? Circulation. 1993 Sep;88(3):905–914. doi: 10.1161/01.cir.88.3.905. [DOI] [PubMed] [Google Scholar]