

Abstract
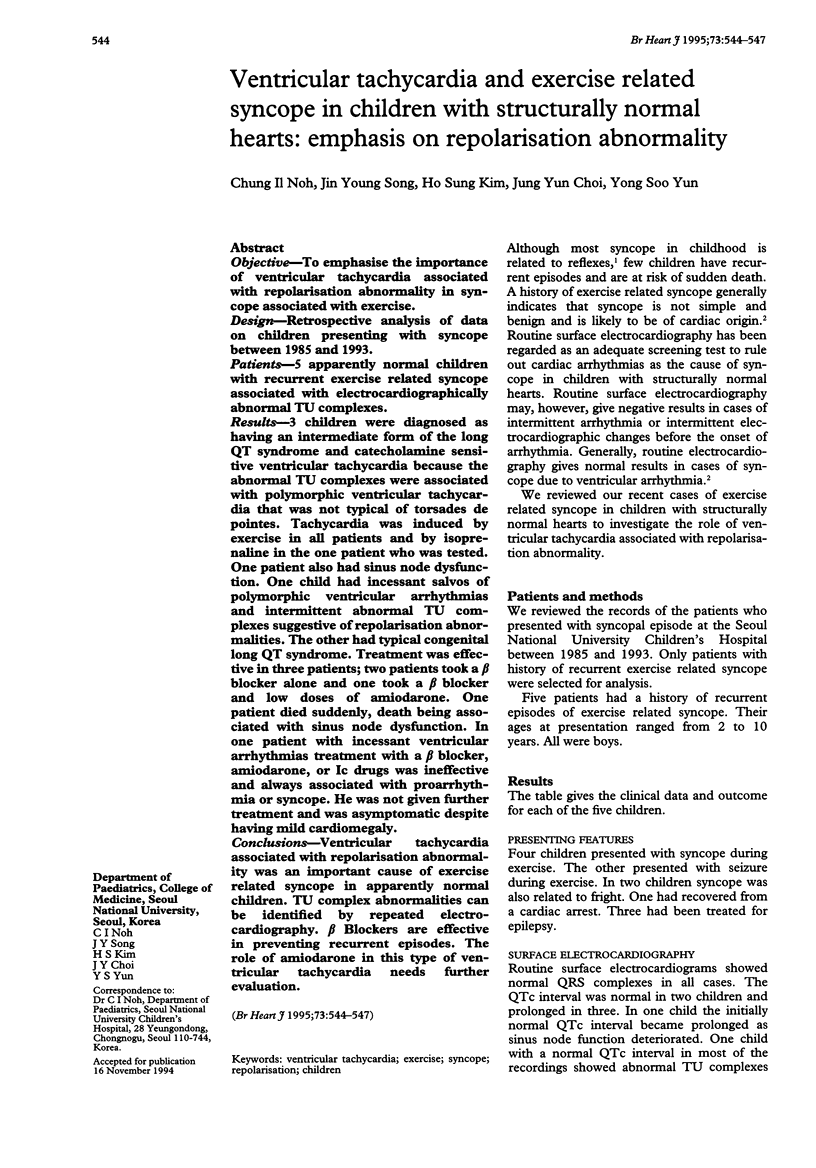
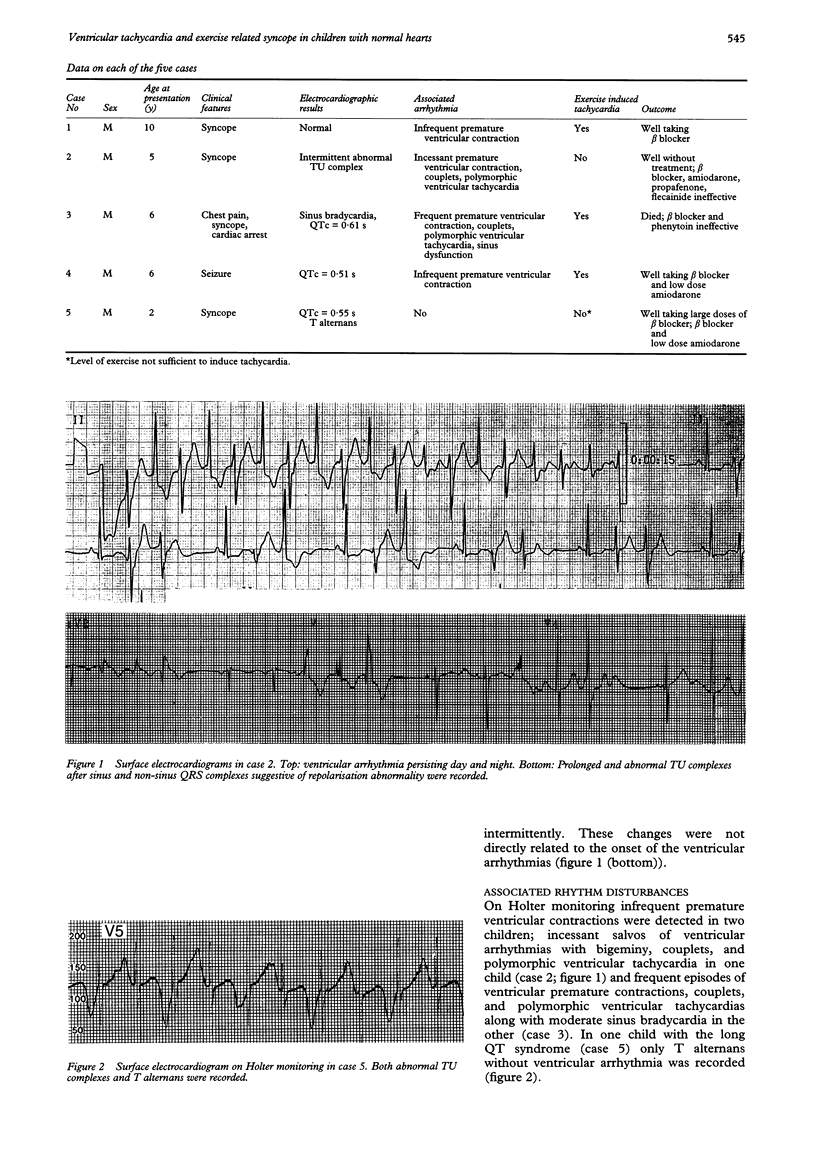
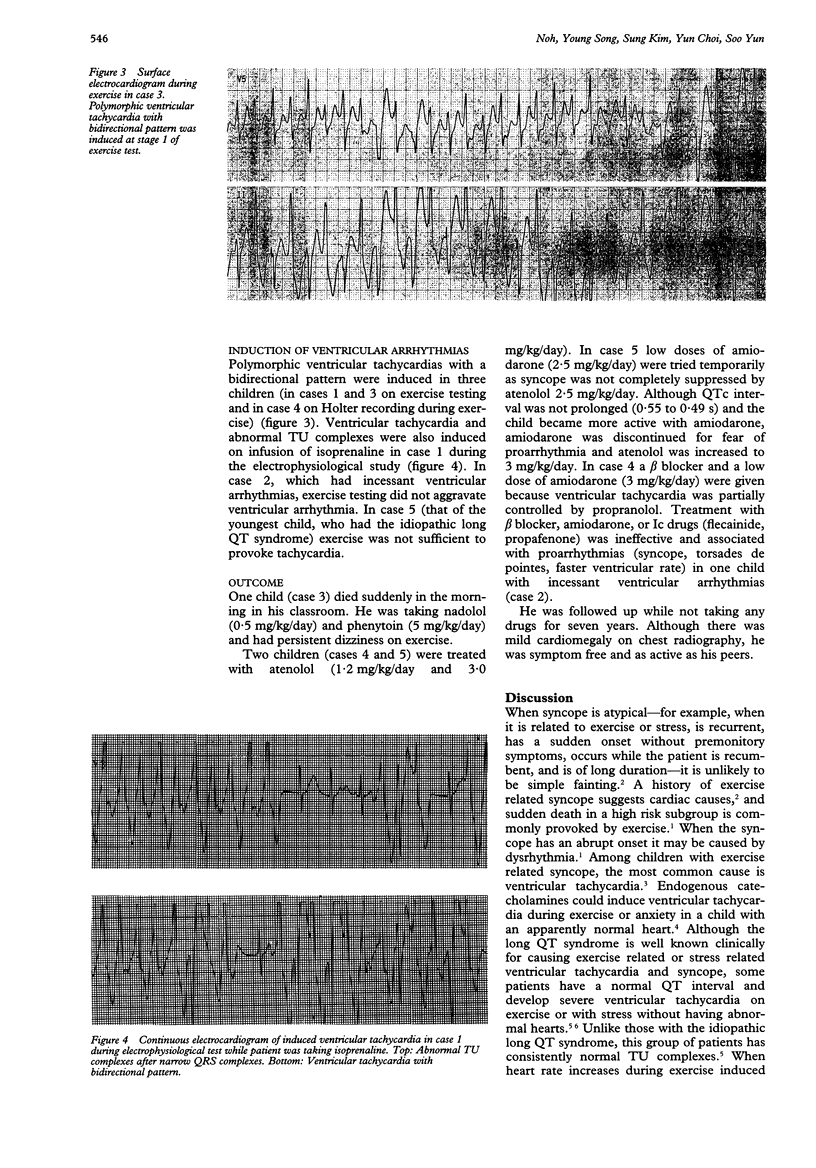
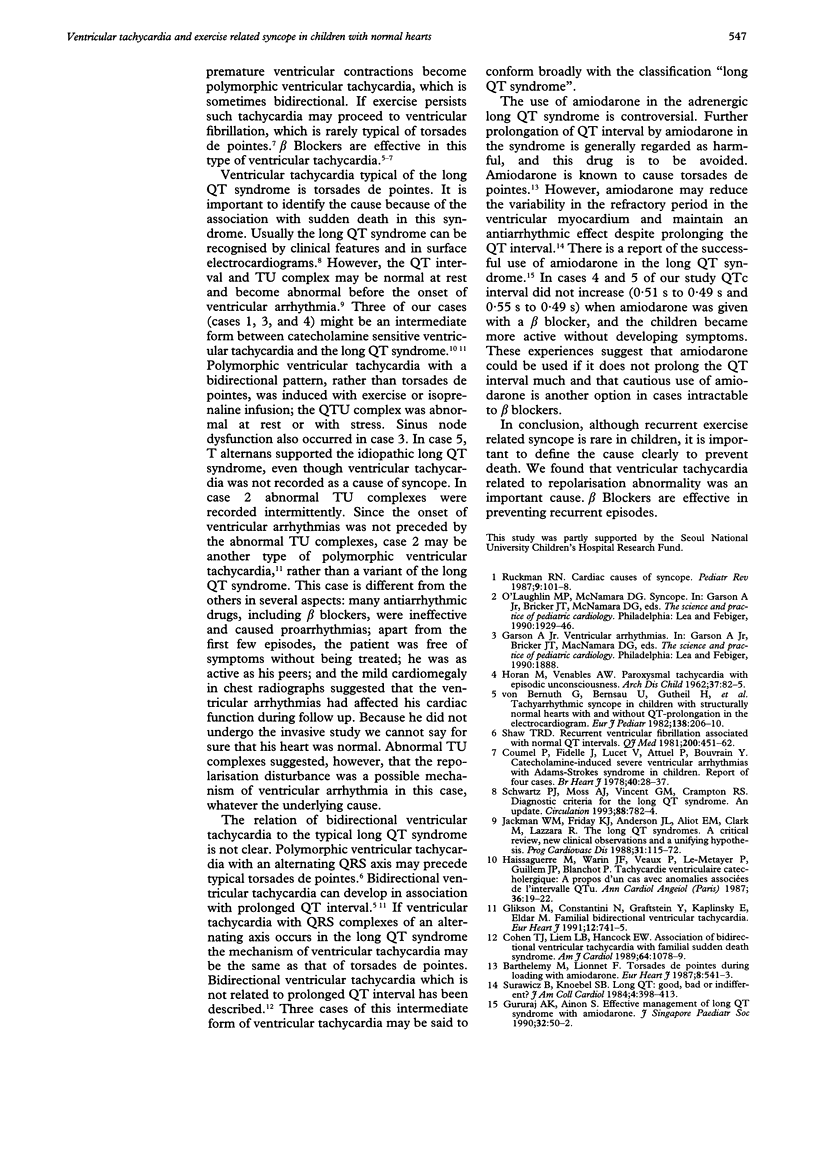
OBJECTIVE--To emphasize the importance of ventricular tachycardia associated with repolarisation abnormality in syncope associated with exercise. DESIGN--Retrospective analysis of data on children presenting with syncope between 1985 and 1993. PATIENTS--5 apparently normal children with recurrent exercise related syncope associated with electrocardiographically abnormal TU complexes. RESULTS--3 children were diagnosed as having an intermediate form of the long QT syndrome and catecholamine sensitive ventricular tachycardia because the abnormal TU complexes were associated with polymorphic ventricular tachycardia that was not typical of torsades de pointes. Tachycardia was induced by exercise in all patients and by isoprenaline in the one patient who was tested. One patient also had sinus node dysfunction. One child had incessant salvos of polymorphic ventricular arrhythmias and intermittent abnormal TU complexes suggestive of repolarisation abnormalities. The other had typical congenital long QT syndrome. Treatment was effective in three patients; two patients took a beta blocker alone and one took a beta blocker and low doses of amiodarone. One patient died suddenly, death being associated with sinus node dysfunction. In one patient with incessant ventricular arrhythmias treatment with a beta blocker, amiodarone, or Ic drugs was ineffective and always associated with proarrhythmia or syncope. He was not given further treatment and was asymptomatic despite having mild cardiomegaly. CONCLUSIONS--Ventricular tachycardia associated with repolarisation abnormality was an important cause of exercise related syncope in apparently normal children. TU complex abnormalities can be identified by repeated electrocardiography. beta Blockers are effective in preventing recurrent episodes. The role of amiodarone in this type of ventricular tachycardia needs further evaluation.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Cohen T. J., Liem L. B., Hancock E. W. Association of bidirectional ventricular tachycardia with familial sudden death syndrome. Am J Cardiol. 1989 Nov 1;64(16):1078–1079. doi: 10.1016/0002-9149(89)90821-7. [DOI] [PubMed] [Google Scholar]
- Glikson M., Constantini N., Grafstein Y., Kaplinsky E., Eldar M. Familial bidirectional ventricular tachycardia. Eur Heart J. 1991 Jun;12(6):741–745. [PubMed] [Google Scholar]
- Gururaj A. K., Ainon S. Effective management of long Q-T syndrome with amiodarone. J Singapore Paediatr Soc. 1990;32(1-2):50–52. [PubMed] [Google Scholar]
- HORAN M., VENABLES A. W. Paroxysmal tachycardia with episodic unconsciousness. Arch Dis Child. 1962 Feb;37:82–85. doi: 10.1136/adc.37.191.82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haïssaguerre M., Warin J. F., Veaux P., Le Métayer P., Guillem J. P., Blanchot P. Tachycardie ventriculaire catécholergique. A propos d'un cas avec anomalies associées de l'intervalle QTu. Ann Cardiol Angeiol (Paris) 1987 Jan;36(1):19–22. [PubMed] [Google Scholar]
- Jackman W. M., Friday K. J., Anderson J. L., Aliot E. M., Clark M., Lazzara R. The long QT syndromes: a critical review, new clinical observations and a unifying hypothesis. Prog Cardiovasc Dis. 1988 Sep-Oct;31(2):115–172. doi: 10.1016/0033-0620(88)90014-x. [DOI] [PubMed] [Google Scholar]
- Leroy G., Haiat R., Barthelemy M., Lionnet F. Torsade de pointes during loading with amiodarone. Eur Heart J. 1987 May;8(5):541–543. doi: 10.1093/oxfordjournals.eurheartj.a062315. [DOI] [PubMed] [Google Scholar]
- Ruckman R. N. Cardiac causes of syncope. Pediatr Rev. 1987 Oct;9(4):101–108. doi: 10.1542/pir.9-4-101. [DOI] [PubMed] [Google Scholar]
- Schwartz P. J., Moss A. J., Vincent G. M., Crampton R. S. Diagnostic criteria for the long QT syndrome. An update. Circulation. 1993 Aug;88(2):782–784. doi: 10.1161/01.cir.88.2.782. [DOI] [PubMed] [Google Scholar]
- Shaw T. R. Recurrent ventricular fibrillation associated with normal QT intervals. Q J Med. 1981 Autumn;50(200):451–462. [PubMed] [Google Scholar]
- Surawicz B., Knoebel S. B. Long QT: good, bad or indifferent? J Am Coll Cardiol. 1984 Aug;4(2):398–413. doi: 10.1016/s0735-1097(84)80232-6. [DOI] [PubMed] [Google Scholar]