

Abstract
Management of renal stone in crossed fused renal ectopia (CFRE) is difficult because of abnormal location, malrotation, and its relations with vertebral column and small bowel. Management is not standardized because of the paucity of literature and variable anatomy. We managed an 8-year-old boy with multiple renal stones in right side crossed kidney by laparoscopic pyelolithotomy and nephro pyeloscopy with the help of ureteroscope. Until now, there is only one prior report of laparoscopic pyelolithotomy in CFRE. We share our experience in this case and review the literature regarding the management of kidney stones in this rare anomaly.
Keywords: Crossed fused renal ectopia, laparoscopy, pyelolithotomy, renal stone
INTRODUCTION
Crossed fused renal ectopia (CFRE) is a rare congenital anomaly, occurring in one in two thousand (autopsy series) in which one kidney is located on the side opposite from which its ureter inserts into the bladder and is fused with opposite kidney.[1] There are total six forms of CFRE with variable clinical presentation. The abnormal kidney position and the anomalous blood supply may impede drainage from the collecting system, creating a predisposition to urinary tract infection and calculus formation.[1]
Because of the rarity of cases, optimal approach for renal stone in crossed kidney is not standardized. Various approaches for management of renal in CFRE have been described in the literature. We, herein describe a case of multiple renal stones in crossed fused ectopic kidney managed via transperitoneal transmesocolic laparoscopic pyelolithotomy and intraoperative pyelonephroscopy by ureteroscope in an 8-year-old child. There was no option of percutaneous nephrolithotomy (PCNL) or shock wave lithotripsy (SWL) because of the location of the kidney in the abdomen. By laparoscopic approach, it could be managed in the minimally invasive way.
CASE REPORT
An 8-year-old boy was admitted with complaints of left lower abdominal pain of 6 months duration. Ultrasonography was suggestive of the right ectopic kidney with multiple renal stones. A contrast-enhanced computed tomography (CT) with three-dimensional reconstruction showed right kidney crossing the midline and fused with lower pole of the left kidney with anteriorly rotated renal pelvis [Figure 1] and 2 cm stone impacted at pelvi ureteric junction (PUJ) and few secondary calculi. There were three renal arteries arising from aorta supplying the right ectopic kidney, all entering into hilum on the right side of renal pelvis of ectopic kidney [Figure 1]. Blood investigations were within normal limits, and the urine culture was sterile.
Figure 1.
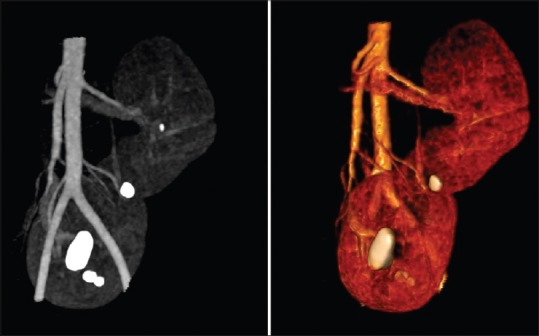
Left-hand photograph shows contrast-enhanced computed tomography showing right crossed fused ectopic kidney with anteriorly rotated renal pelvis with stone impacted at pelvi ureteric junction and few secondary calculi in upper and lower pole of ectopic kidney. Right hand photograph shows computed tomography angiography revealing three renal arteries arising from aorta supplying the right ectopic kidney with two upper polar arteries and one lower polar artery, all entering into hilum on right side of renal pelvis of the ectopic kidney
We planned for cystoscopy, right retrograde pyelography (RGP) and proceed after that. Under general anesthesia, cystoscopy/RGP revealed bilateral ureteric orifices in normal location and impacted stone just proximal to PUJ with small anteriorly rotated pelvis with no obvious PUJ narrowing [Figure 2]. A double-J stent of size 4.5 Fr was inserted. The patient was then placed in right lateral position, and three ports were put: One 10 mm (periumbilical) camera port and two 5 mm working port lateral to left rectus muscle above and below the camera port in a triangular fashion.
Figure 2.
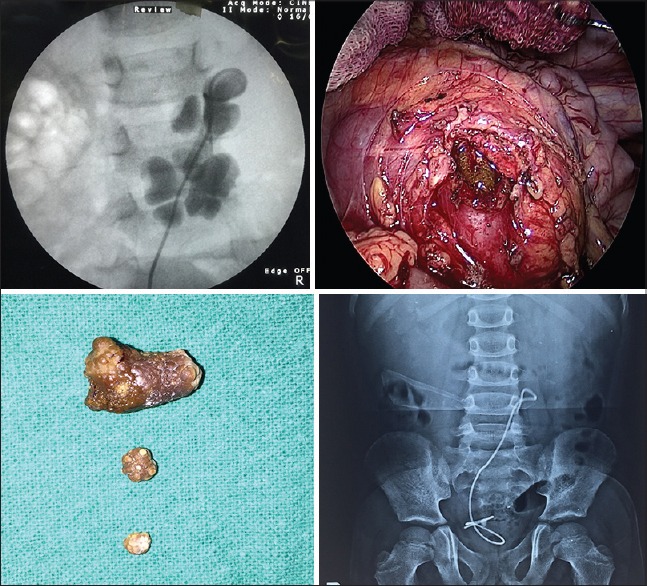
Upper left: Retrograde pyelography with double-J stent insertion, upper right: Ectopic kidney with incised pelvis revealing impacted stone, lower right: Extracted calculi. Lower left: Follow-up plain X-ray showing complete clearance of calculi from the ectopic kidney
The anterior surface of the ectopic kidney was indentified easily through the mesocolon, and mesocolon was incised with hook cautery avoiding inferior mesenteric vessels. The renal pelvis was indentified, and the stone was palpated with a laparoscopic instrument. Renal pelvis over the impacted stone was palpated and incised with hook monopolar cautery on the left side of PUJ thus avoiding the injury to renal vessels and PUJ. Larger stone was manipulated out of the kidney and bagged in no. 8 glove finger. Intraoperative nephro pyeloscopy was done with the help of 8/9.8 Fr storz ureteroscope to locate and remove calyceal calculi. It was put through 10 mm port, pyelotomy was identified and scope was introduced in the pelvicalyceal system. Pyelotomy incision was closed with continuous 4–0 Vicryl suture on round body needle. Peripelvic fat and mesocolic window were closed separately with 4–0 Vicryl. A 20 F abdominal drain was left through 5 mm lower abdominal port. The estimated blood loss was <50 ml and the procedure was completed in 170 min.
Periurethral catheter and drain were removed on 2nd and 3rd postoperative day consecutively. The patient was discharged on the 3rd postoperative day. The stent was removed after 1 month with plain X-ray film showing complete clearance of the stones from the kidney.
DISCUSSION
CFRE is the second common fusion anomaly after horseshoe kidney.[1] Routinely, diseases of these kidneys are managed with open surgery. However, laparoscopic approach for these anomalies has been described.[2,3,4,5] Transperitoneal and retroperitoneoscopic[4] approaches have been used for various indications. Most of the authors have used transperitoneal access as it provides more space, better visibility, and direct access to vasculature.
Management of renal stone in CFRE is difficult because of abnormal location, malrotation, and its relations with vertebral column and small bowel. Usual treatment options such as SWL and PCNL, though described may not be effective and not applicable in all the cases. SWL has been described, but it may be technically difficult because of underlying bone and overlying bowel gases.[6,7] Clearance of stone may also be suboptimal after fragmentation because of malrotation and associated PUJ obstruction. Tunc et al. have described SWL in 150 cases of the anomalous kidney with a renal stone in which three cases were CFRE.[7] The result was only 25% in these cases. There are reports of PCNL in CFRE, but they do not mention the side of PCNL (whether done in crossed kidney or orthotopic kidney) and type of CFRE.[8,9] Rana and Bhojwani have reported three cases of PCNL, but the side was mentioned only in one case where PCNL was done in noncrossed kidney.[8] Similarly, Gupta et al. have reported four cases of PCNL but there is no mention of the side and type of CFRE.[9] Theoretically, PCNL may be possible in inferior ectopia (which is the commonest type) and inferior ectopia where the kidney is completely crossed and does not lie over vertebral column. In L-shaped kidney like in our case, PCNL is not an option. Therefore, laparoscopic pyelolithotomy is best. Laparoscopic-assisted PCNL can be done but has not been described for crossed kidney.
Laparoscopic pyelolithotomy for renal stone seems to be effective minimally invasive option for this anomaly. Until date, only one case of laparoscopic pyeloplasty with pyelolithotomy has been described by Modi et al. in 2006.[5] Laparoscopic pyelolithotomy is easier as the pelvis is anteriorly rotated and can be identified easily. Preoperative CT angiography/urography is a must before surgery as it helps in surgical planning. One can plan the dissection and decide the location of pyelotomy based on CT finding. In our case, there were three vessels supplying the crossed kidney and were entering on the right side of renal sinus. Therefore, we made pyelotomy on the left side of PUJ. In children, transmesocolic approach is useful as it provides direct access to renal pelvis obviating the need for colon reflection.
CONCLUSION
Laparoscopic pyelolithotomy is a feasible option for management of stones in the crossed ectopic pelvic kidney with a laterally and anterior-directed pelvis. Preoperative workup with contrast-enhanced CT scan with CT angiography for the detailed anatomical and functional status is necessary before proceeding to surgery.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Shapiro E, Bauer SB, Chow JS. Anomalies of upper urinary tract. In: Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA, editors. Campbell-Walsh Urology. Philadelphia: Elsevier Saunders; 2012. pp. 3140–5. [Google Scholar]
- 2.Kumar S, Pandya S, Singh SK, Panigrahy B, Acharya N, Lal A, et al. Laparoscopic heminephrectomy in L-shaped crossed fused ectopia. J Endourol. 2008;22:979–83. doi: 10.1089/end.2007.0286. [DOI] [PubMed] [Google Scholar]
- 3.Aminsharifi A, Niroomand R, Kroup M, Hosseini MM. Laparoscopic nephrolithotomy in a patient with crossed fused renal ectopia. Nat Rev Urol. 2009;6:675–9. doi: 10.1038/nrurol.2009.198. [DOI] [PubMed] [Google Scholar]
- 4.Modi P, Rizvi SJ, Gupta R, Patel S. Retroperitoneoscopic nephrectomy for crossed-fused ectopic kidney. Indian J Urol. 2009;25:401–3. doi: 10.4103/0970-1591.56182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Modi P, Goel R, Dodia S. Case report: Laparoscopic pyeloplasty with pyelolithotomy in crossed fused ectopia. J Endourol. 2006;20:191–3. doi: 10.1089/end.2006.20.191. [DOI] [PubMed] [Google Scholar]
- 6.Kato M, Ioritani N, Aizawa M, Inaba Y, Watanabe R, Orikasa S. Extracorporeal shock wave lithotripsy for a ureteral stone in crossed fused renal ectopia. Int J Urol. 2000;7:270–3. doi: 10.1046/j.1442-2042.2000.00185.x. [DOI] [PubMed] [Google Scholar]
- 7.Tunc L, Tokgoz H, Tan MO, Kupeli B, Karaoglan U, Bozkirli I. Stones in anomalous kidneys: Results of treatment by shock wave lithotripsy in 150 patients. Int J Urol. 2004;11:831–6. doi: 10.1111/j.1442-2042.2004.00916.x. [DOI] [PubMed] [Google Scholar]
- 8.Rana AM, Bhojwani JP. Percutaneous nephrolithotomy in renal anomalies of fusion, ectopia, rotation, hypoplasia, and pelvicalyceal aberration: Uniformity in heterogeneity. J Endourol. 2009;23:609–14. doi: 10.1089/end.2007.0430. [DOI] [PubMed] [Google Scholar]
- 9.Gupta NP, Mishra S, Seth A, Anand A. Percutaneous nephrolithotomy in abnormal kidneys: Single-center experience. Urology. 2009;73:710–4. doi: 10.1016/j.urology.2008.10.070. [DOI] [PubMed] [Google Scholar]