

Abstract
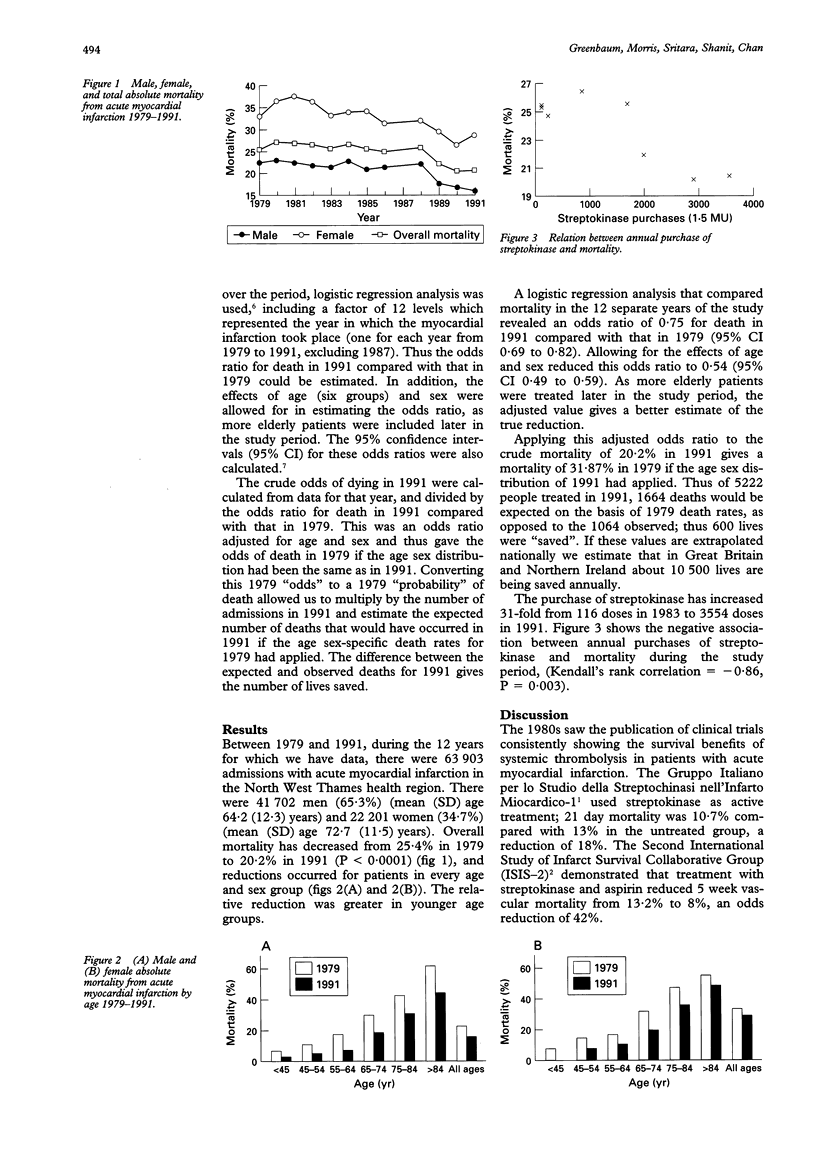
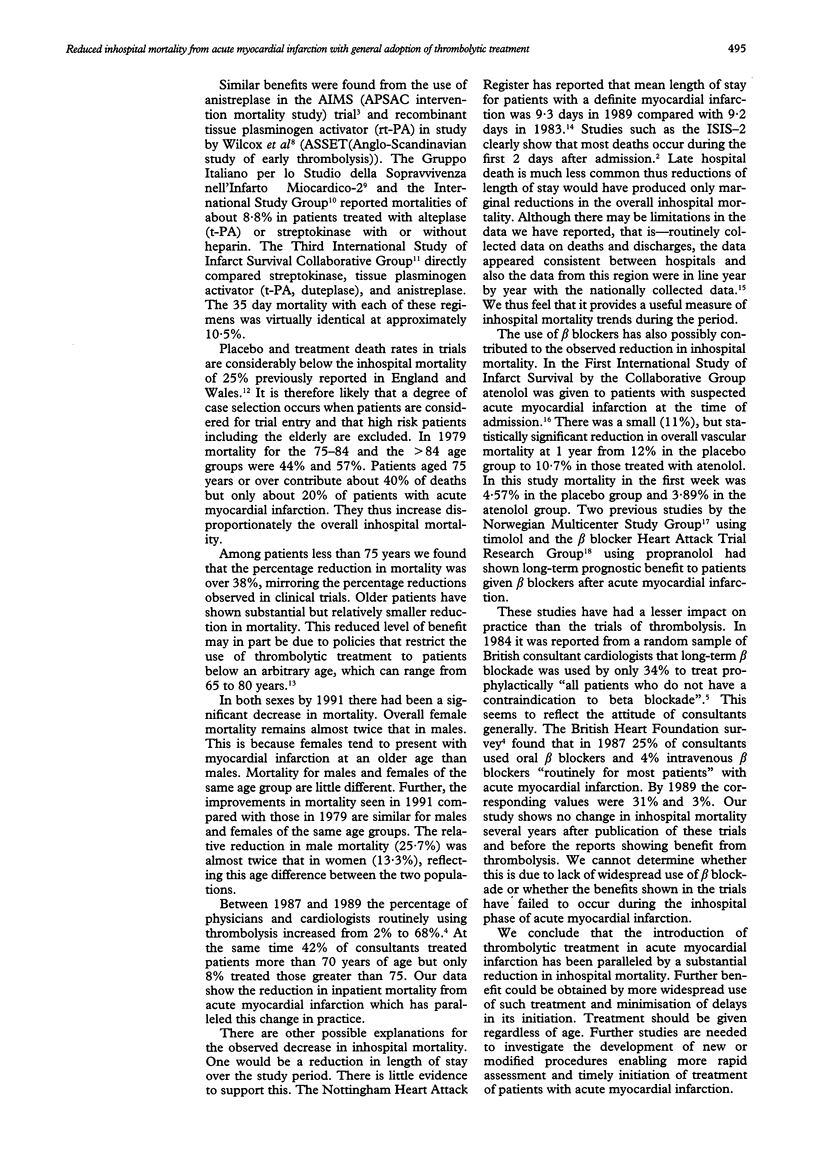
OBJECTIVE--To determine the impact of studies of thrombolytic treatment in acute myocardial infarction on inhospital mortality. DESIGN--Retrospective study. SETTING--All 21 major hospitals in the North West Thames health region. PATIENTS--63,903 patients with acute myocardial infarction. STUDY PERIOD--1979-1991. MAIN OUTCOME MEASURES--in-hospital mortality. RESULTS--Overall mortality decreased by 5.2% from 25.4% to 20.2% (P < 0.0001) (95% confidence interval (CI) 3.4 to 6.6). Male mortality decreased by 6.5% from 22.3% to 15.8% (P < 0.0001) (95% CI 4.8 to 8.4); female mortality decreased by 4.3% from 32.6% to 28.3% (P < 0.01) (95% CI 1.3 to 7.4). Reductions in mortality occurred in all age and sex groups but were greater in younger patients. Logistic regression analysis of death rates showed that the odds ratio of death in 1991 compared with that in 1979 was 0.75 (95% CI 0.69 to 0.82). After allowing for the effects of age and sex, this odds ratio became 0.54 (95% CI 0.49 to 0.59), as more elderly patients were treated in 1991. Purchase of streptokinase increased 31-fold from 116 doses in 1983 to 3554 doses in 1991. There was a pronounced negative association between annual purchases of streptokinase and mortality (Kendall's rank correlation = -0.86, P = 0.003). Changes in clinical practice resulted in the saving of the lives of an estimated 600 patients with acute myocardial infarction in 1991. This extrapolates to an annual saving of 10,500 lives in the United Kingdom. CONCLUSIONS--In the past few years thrombolytic treatment has been widely adopted for the management of acute myocardial infarction. This has been paralleled by a substantial reduction in in-hospital mortality.
Full text
PDF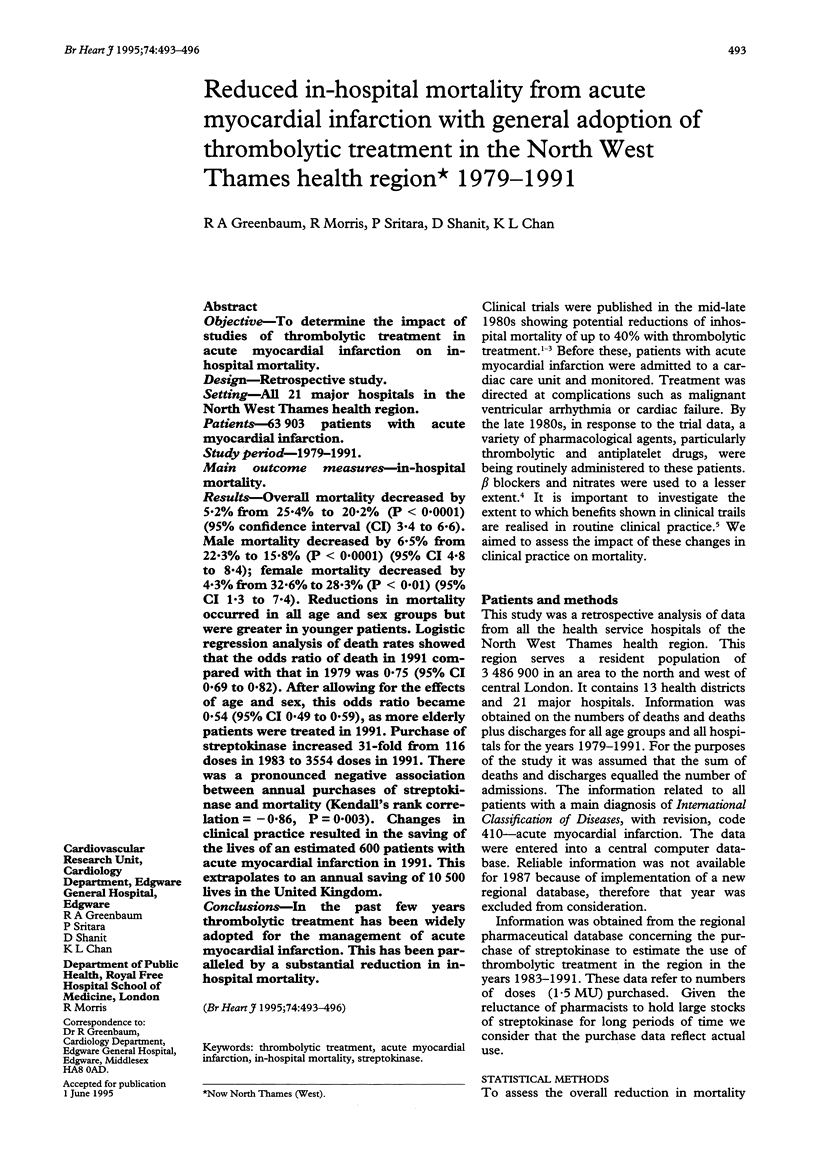
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Burrell C. J., Skehan J. D., Cowley M. L., Barrett C. W., Mills P. G. Districts' use of thrombolytic agents. BMJ. 1990 Jan 27;300(6719):237–238. doi: 10.1136/bmj.300.6719.237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Colling A. Beta blockers after myocardial infarction: have trials changed practice? Br Med J (Clin Res Ed) 1985 Jan 26;290(6464):322–322. doi: 10.1136/bmj.290.6464.322-a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Collins R., Julian D. British Heart Foundation surveys (1987 and 1989) of United Kingdom treatment policies for acute myocardial infarction. Br Heart J. 1991 Sep;66(3):250–255. doi: 10.1136/hrt.66.3.250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greenbaum R. A. Routine use of beta-blockers following myocardial infarction: a note of dissent. J R Soc Med. 1987 Jul;80(7):402–403. doi: 10.1177/014107688708000702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hampton P., Harrison L., Gray D. Demand for hospital services following admission with suspected myocardial infarction in 1983 and 1989. Health Trends. 1993;25(3):91–94. [PubMed] [Google Scholar]
- Wilcox R. G., von der Lippe G., Olsson C. G., Jensen G., Skene A. M., Hampton J. R. Trial of tissue plasminogen activator for mortality reduction in acute myocardial infarction. Anglo-Scandinavian Study of Early Thrombolysis (ASSET). Lancet. 1988 Sep 3;2(8610):525–530. doi: 10.1016/s0140-6736(88)92656-6. [DOI] [PubMed] [Google Scholar]