

Abstract
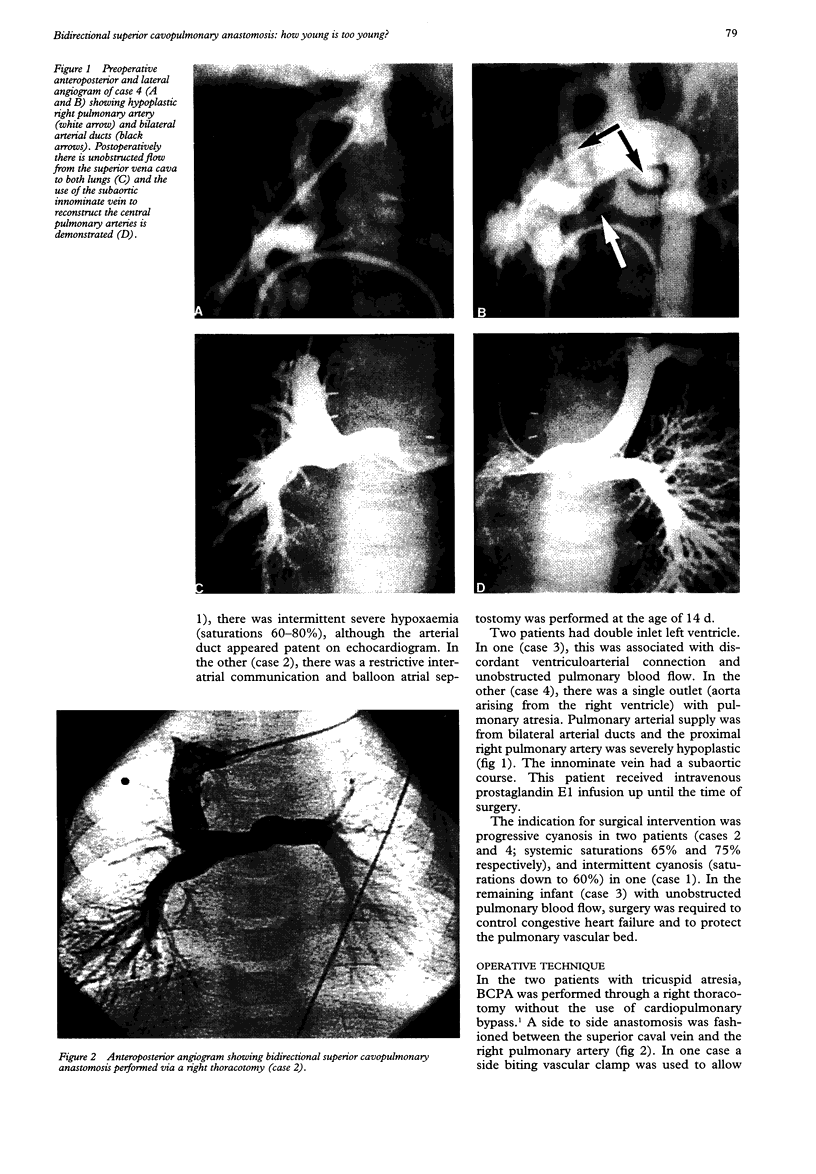
OBJECTIVE--To define the lowest age at which the bidirectional superior cavopulmonary anastomosis can safely be used in infants with complex congenital heart defects. DESIGN--A retrospective analysis of clinical, echocardiographic, haemodynamic, and angiographic data in four consecutive patients undergoing bidirectional superior cavopulmonary anastomosis below the age of 2 months. PATIENTS--Between November 1990 and September 1993, four infants less than 8 weeks of age (3, 4, 6, and 7 weeks) underwent bidirectional superior cavopulmonary anastomosis as a primary palliation for complex heart disease. The indication for early surgical intervention was progression of cyanosis (n = 3) and high pulmonary blood flow causing heart failure (n = 1). In two infants with tricuspid atresia, surgery was performed through a right thoracotomy without the use of cardiopulmonary bypass. In one infant with double inlet left ventricle and discordant ventriculoarterial connection, cavopulmonary anastomosis was combined with an arterial switch procedure. The final infant had double inlet left ventricle with pulmonary atresia; the central pulmonary arteries were virtually discontinuous and each branch was supplied by a separate arterial duct. The central pulmonary arteries were reconstructed using the subaortic innominate vein. Temporary prostacyclin infusion was used in three patients in the immediate postoperative period. RESULTS--Early postoperative extubation (5, 7, and 48 h) was successful in three patients. The youngest child required ligation of the ductus arteriosus four days later because of severe upper body oedema. The postoperative course was complicated by prolonged effusions in two patients. All were alive and well 14-48 months postoperatively, with satisfactory systemic saturations (80-87%) and haemodynamic indices. CONCLUSIONS--This limited experience challenges the widely held belief that the bidirectional superior cavopulmonary anastomosis cannot be used as a primary palliation for complex heart disease in early infancy. A wider experience is required to determine the safety and indications for this approach.
Full text
PDF
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Albanese S. B., Carotti A., Di Donato R. M., Mazzera E., Troconis C. J., Giannico S., Picardo S., Marcelletti C. Bidirectional cavopulmonary anastomosis in patients under two years of age. J Thorac Cardiovasc Surg. 1992 Oct;104(4):904–909. [PubMed] [Google Scholar]
- Franklin R. C., Sullivan I. D., Anderson R. H., Shinebourne E. A., Deanfield J. E. Is banding of the pulmonary trunk obsolete for infants with tricuspid atresia and double inlet ventricle with a discordant ventriculoarterial connection? Role of aortic arch obstruction and subaortic stenosis. J Am Coll Cardiol. 1990 Nov;16(6):1455–1464. doi: 10.1016/0735-1097(90)90392-3. [DOI] [PubMed] [Google Scholar]
- Freedom R. M., Benson L. N., Smallhorn J. F., Williams W. G., Trusler G. A., Rowe R. D. Subaortic stenosis, the univentricular heart, and banding of the pulmonary artery: an analysis of the courses of 43 patients with univentricular heart palliated by pulmonary artery banding. Circulation. 1986 Apr;73(4):758–764. doi: 10.1161/01.cir.73.4.758. [DOI] [PubMed] [Google Scholar]
- Glenn W. W. Superior vena cava-pulmonary artery shunt. By William W. L. Glenn, 1958. Ann Thorac Surg. 1989 Jan;47(1):62–64. doi: 10.1016/0003-4975(89)90238-5. [DOI] [PubMed] [Google Scholar]
- Hawkins J. A., Shaddy R. E., Day R. W., Sturtevant J. E., Orsmond G. S., McGough E. C. Mid-term results after bidirectional cavopulmonary shunts. Ann Thorac Surg. 1993 Oct;56(4):833–837. doi: 10.1016/0003-4975(93)90340-n. [DOI] [PubMed] [Google Scholar]
- Kirklin J. K., Blackstone E. H., Kirklin J. W., Pacifico A. D., Bargeron L. M., Jr The Fontan operation. Ventricular hypertrophy, age, and date of operation as risk factors. J Thorac Cardiovasc Surg. 1986 Dec;92(6):1049–1064. [PubMed] [Google Scholar]
- Kopf G. S., Laks H., Stansel H. C., Hellenbrand W. E., Kleinman C. S., Talner N. S. Thirty-year follow-up of superior vena cava-pulmonary artery (Glenn) shunts. J Thorac Cardiovasc Surg. 1990 Nov;100(5):662–671. [PubMed] [Google Scholar]
- Lamberti J. J., Spicer R. L., Waldman J. D., Grehl T. M., Thomson D., George L., Kirkpatrick S. E., Mathewson J. W. The bidirectional cavopulmonary shunt. J Thorac Cardiovasc Surg. 1990 Jul;100(1):22–30. [PubMed] [Google Scholar]
- Pridjian A. K., Mendelsohn A. M., Lupinetti F. M., Beekman R. H., 3rd, Dick M., 2nd, Serwer G., Bove E. L. Usefulness of the bidirectional Glenn procedure as staged reconstruction for the functional single ventricle. Am J Cardiol. 1993 Apr 15;71(11):959–962. doi: 10.1016/0002-9149(93)90914-x. [DOI] [PubMed] [Google Scholar]
- Salmon A. P., Sethia B., Silove E. D., Goh D., Mitchell I., Alton H., De Giovanni J. V., Wright J. G., Abrams L. D. Cavopulmonary anastomosis as long-term palliation for patients with tricuspid atresia. Eur J Cardiothorac Surg. 1989;3(6):494–498. doi: 10.1016/1010-7940(89)90107-3. [DOI] [PubMed] [Google Scholar]
- Seliem M., Muster A. J., Paul M. H., Benson D. W., Jr Relation between preoperative left ventricular muscle mass and outcome of the Fontan procedure in patients with tricuspid atresia. J Am Coll Cardiol. 1989 Sep;14(3):750–755. doi: 10.1016/0735-1097(89)90121-6. [DOI] [PubMed] [Google Scholar]
- Wessel D. L., Adatia I., Giglia T. M., Thompson J. E., Kulik T. J. Use of inhaled nitric oxide and acetylcholine in the evaluation of pulmonary hypertension and endothelial function after cardiopulmonary bypass. Circulation. 1993 Nov;88(5 Pt 1):2128–2138. doi: 10.1161/01.cir.88.5.2128. [DOI] [PubMed] [Google Scholar]
- Wessel D. L., Adatia I., Giglia T. M., Thompson J. E., Kulik T. J. Use of inhaled nitric oxide and acetylcholine in the evaluation of pulmonary hypertension and endothelial function after cardiopulmonary bypass. Circulation. 1993 Nov;88(5 Pt 1):2128–2138. doi: 10.1161/01.cir.88.5.2128. [DOI] [PubMed] [Google Scholar]