

Abstract
[Purpose] The purpose of this study was to analyze the biomechanical changes and patterns of the lower extremities after gait termination in middle-aged and elderly women. [Subjects] The study population comprised an elderly group and middle-aged group. [Methods] To collect kinematic and kinetic data related to gait termination, six infrared cameras and one force platform were used, and variables were calculated by using Visual 3D. [Results] During the termination phase, the elderly group generated less braking force than the middle-aged group. During initiation of the termination phase and after the center of gravity completely stopped moving, there was a difference between the two groups in the hip joint angle. During the termination phase, the maximum angular velocity and extension moment of the ankle joint and those of the knee joint were higher in the elderly group than in the middle-aged group. [Conclusion] In contrast to the middle-aged group that showed a rapid increase and then decrease of the initial extension moment during gait termination, the maximum extension moment that was created during the early stage of the termination phase in the elderly group continued until the center of gravity completely stopped.
Key words: Gait termination, Unexpected termination, Joint moment
INTRODUCTION
Each year, about 30% of the elderly population (aged 65 years and older) experience falls, and 10–12% of those who sustain hip fractures die of complications1). The accident rate is twice as high in women than in men2). In the elderly, falls do not only cause trauma but also cause a tendency to develop a fear of falling again, causing those affected to limit their daily activities3). Falls in the elderly cause soft tissue damage and musculoskeletal fractures, as well as a loss of morale, activity, and, consequently, muscular strength and stability as a result of the reduction in daily activities and movements because of the fear of experiencing another fall4). For these reasons, various studies are being conducted to improve the quality of life and reduce the social costs, including medical costs, of the elderly by quantifying the dynamic stability of this population1, 5, 6).
Elderly persons generally fall when they lose their balance while standing or walking7). A fall can occur while the elderly are performing very simple actions because the muscular strength of the lower extremities decreases with age, and older persons are more likely to lose their balance when changing positions because of their degenerative changes8).
Decreased muscular strength of the lower extremities is very closely related to falls, and the prevalence of falls among the elderly who have weak lower-extremity muscles is three to four times higher than in those who have healthy lower-extremity muscles9, 10). Furthermore, the decrease of muscle strength and flexibility in the lower extremity as a result of aging has an effect on stability11). Therefore, many studies are investigating the threats to stability factors in the elderly, who have decreased balance ability, including during turning, obstacle crossing, stair climbing, and gait termination8, 12, 13). These methods are used to evaluate individual motor ability by changing the stable gait patterns in individual subjects by using external stimuli.
Gait termination is commonly used as a scale to assess motor ability, as it changes gait patterns and thereby threatens the stability of the elderly; this is because balance can be maintained without additional steps when the center of gravity is within the base of support of the feet14, 15). In particular, gait termination makes it difficult for the elderly to maintain stability because the braking force increases in the final supporting phase compared with in the normal gait and the elderly have relatively low muscular strength16, 17). However, among various methods that threaten the stability of the elderly, the mechanism for stopping the center of gravity has been relatively less researched than other mechanisms.
To avoid colliding with an unexpected obstacle while walking, a person must either stop moving or make a change in direction. Both options reduce the momentum of the forward-moving center of mass and must be controlled within the base of support in the body. This sudden change of center of gravity reduces stability and can cause a fall to occur18, 19). To stop the center of gravity while walking, the velocity of the center of gravity must be reduced by about 90% in the last step, and the increased load on the joint of the stopping foot requires more activation of the extensors of the lower extremity16). This type of change requires fast deceleration of the center of gravity in unexpected situations and, therefore, increases the risks of falls and other injuries20).
However, despite the rapid increase of the elderly population in South Korea, very few studies have investigated gait termination, which can cause a fall event, and most previous studies have required subjects to stop with their feet positioned next to each other. As a result, these studies do not fully explain the gait interruption patterns found in unexpected situations in daily settings, and because they designated a point at which subjects were asked to stop, the subjects could reduce their velocity or prepare to stop after learning the routine in previous of the tasks.
For these reasons, the biomechanical changes and patterns of the lower extremities were analyzed in the study to understand the characteristics of gait termination in the elderly, to examine the difference between elderly and middle-aged subjects, and, finally, to help reduce the prevalence of falls in the elderly through appropriate correction.
SUBJECTS AND METHODS
The subjects who participated in the test were 10 elderly women aged 70 years and older (age, 73.1 ± 2.13 years; height, 155 ± 5.06 cm; weight, 61.67 ± 6.19 kg) and 10 middle-aged women aged 40 years and older (age, 44.9 ± 6.12 years, height, 163.50 ± 4.30 cm; weight, 58.52 ± 5.83 kg) who had no orthopedic history in the last 6 months. The study purpose and procedure were explained to all the participants prior to study participation, and all participants signed a consent form. The study protocol was approved by the Institutional Review Board of the University of Sahmyook. To record the stopping motion of the subjects, six infrared cameras (Oqus 1 series, Qualisys, Göteborg, Sweden) were used, with a sampling rate of 100 Hz. One force plate (9260AA, Kistler, Winterthur, Switzerland) was used for measuring the impulsive force while stopping, with a sampling rate of 1,000 Hz, and data were obtained in association with the infrared cameras. To induce natural motions, all subjects were asked to walk sufficiently on a runway before the test without controlling their walking speed. The test was conducted at the speed preferred by the subjects.
Before the test, a standing calibration was performed to measure the anatomical alignment of the subjects.
The subjects were asked to stop walking as quickly as they could when an LED (light-emitting diode) light installed at the front of the runway turned on. To eliminate the learning effect, the points at which the subjects stopped were varied, and attempts to stop walking were randomized. To calculate the kinesiological variables, only the data obtained when stopping with the left foot placed successfully on the force platform were collected and analyzed.
For gait termination, only the data for the termination phase (i.e., from event 1 when the heel of the stopping left foot contacted the force plate until event 2 when the center of gravity completely stopped) was analyzed, considering the nature of the motion for 90% of the center-of-gravity velocity of gait within the final step (Fig. 1). Excluding unnatural trials in which the subjects took an extra step after failing to stop or seemed to have predicted the stopping point and reduced their walking speed, three trials were analyzed for each subject.
Fig. 1.
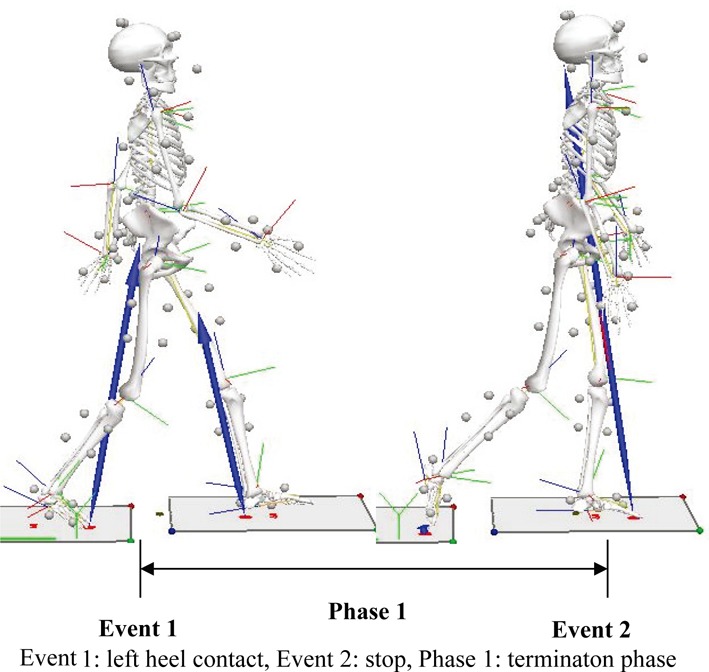
Phase and events
Event 1: left heel contact, Event 2: stop, Phase 1: terminaton phase
The two-dimensional plane data obtained from the six cameras were converted through nonlinear transformation into three-dimensional coordinates, and the position coordinates were obtained by using Qualisys Track Manager (Qualisys Inc., Göteborg, Sweden).
The raw data were filtered by using a second-order Butterworth bidirectional filter to eliminate errors caused by noise. The obtained data were modeled by using the Visual 3D software (C-motion Inc., Germantown, MD, USA), and the variables were calculated. The data from all of the subjects were based on the average of three trials performed by each subject. To standardize the data, the number of frames for each stage was divided by the duration of the stage.
The kinematic and kinetic data obtained by using Visual 3D were used to construct an ensemble graph to compare the change patterns of different variables, and a paired t-test was performed to verify statistical differences between the two groups. The significance level was set at α = 0.05, and the SPSS 16.0 statistics package was used for statistical analysis.
RESULTS
When stopping, the middle-aged group generated a larger maximum ground reaction force in the anterior/posterior and vertical axes than the elderly group (Table 1). However, the differences in ground reaction force in the anterior/posterior axes were not statistically significant, unlike in the vertical axis.
Table 1. Max ground reaction force in termination phase (unit: Nm/kg).
| Ground reaction force - y | Ground reaction force - z | |
|---|---|---|
| Elderly group | −4.5 ± 1.0 | 12.0 ± 1.8* |
| Middle-aged group | −5.2 ± 0.7 | 14.0 ± 1.6* |
Values are expressed as the mean ± SD. *significant difference between group at p<0.05
Almost no difference was found between the two groups with respect to the initial impulse in the right foot before the termination phase, and the two groups showed the same ground reaction force used for controlling the body in the normal gait (Fig. 2a). However, neither of the two groups showed propulsive force to move the body forward at the end of the termination phase. In the left foot, which was used to stop the body, a large amount of braking force was observed during the initial termination phase, and then it quickly declined in both groups. However, both the amount and the reduction rate of the braking force were larger in the middle-aged group than in the elderly group (Fig. 2b).
Fig. 2.
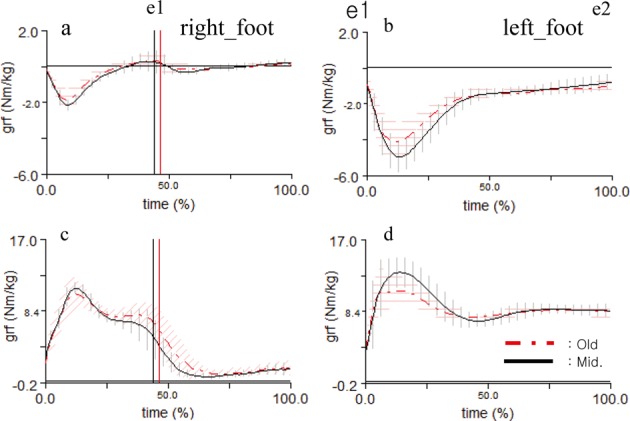
Variation pattern of grf
Concerning the maximum ground reaction force in the right foot, neither group showed a second peak unlike that in the normal gait (Fig. 2c), and the elderly group showed a larger ground reaction force in the initial termination phase than the middle-aged group (Fig. 2d).
Although the middle-aged group showed larger plantar flexion than the elderly group during the initial termination phase, in the latter part of the termination phase, there was almost no difference between the two groups (Table 2). The differences were not statistically significant. The angular velocity of the ankle joints of the middle-aged group was twice as fast as that of the elderly group, and the extension moment of the ankle joints of the middle-aged group was slightly larger than that of the elderly group. The differences were statistically significant.
Table 2. Kinetic and kinematic variables of ankle (unit: deg., deg/s, Nm/kg).
| Angle | Min_av. | Moment | ||
|---|---|---|---|---|
| Event 1 | Event 2 | Phase 1 | Phase 1 | |
| Elderly group | 17.5 ± 6.2 | 3.2 ± 2.8 | −178.1 ± 37.7* | 0.9 ± 0.2* |
| Middle-aged group | 22.0 ± 9.1 | 3.2 ± 4.6 | −308.1 ± 86.6* | 1.1 ± 0.2* |
Values are expressed as the mean ± standard deviation. *significant difference between group at p<0.05. Min_av: minimum angular velocity
In the initial termination phase, the plantar flexion angle of the ankle was smaller in the elderly group than in the middle-aged group; however, because of the smaller dorsiflexion angle, the plantar flexion angle throughout the termination phase was lager (Fig. 3a). Although the two groups showed similar patterns of change in the angular velocity of the ankle, the middle-aged group showed a larger change in angle than the elderly group (Fig. 3b). Both groups showed only plantar flexion moment in terms of the change in ankle joint moment, and although a larger amount of plantar flexion moment was found in the middle-aged group during the initial termination phase, there was no difference between the two groups after the 40% point of the termination phase (Fig. 3c).
Fig. 3.
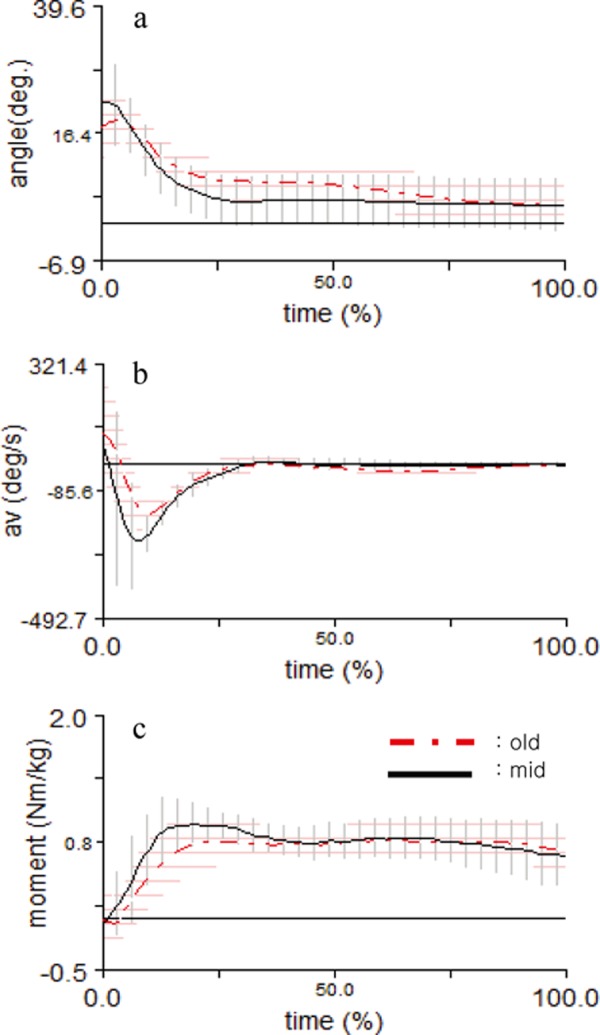
Variation pattern of principle variables in the ankle
Although, there was almost no difference in knee angle between the two groups during the initial termination phase, when the center of gravity completely stopped, the knee was slightly more bent in the elderly group than in the middle-aged group (Table 3). The difference between the two groups was not statistically significant.
Table 3. Kinetic and kinematic variables of knee (unit: deg., deg/s, Nm/kg).
| Angle | Min_av. | Moment | ||
|---|---|---|---|---|
| Event 1 | Event 2 | Phase 1 | Phase 1 | |
| Elderly group | −4.7 ± 4.8 | −15.3 ± 8.5 | −281.0 ± 56.7* | 0.4 ± 0.3* |
| Middle-aged group | −5.6 ± 6.2 | −11.9 ± 7.7 | −308.1 ± 86.6* | 0.9 ± 0.3* |
Values are expressed as the mean ± SD.
*significant difference between group at p<0.05. Min_av: minimum angular velocity
In the termination phase, the maximum flexion angular velocity of the knee joints was faster in the middle-aged group than in the elderly group, and the extension moment of the knee joints of the middle-aged group was twice as high than that of the elderly group. The differences were statistically significant.
In the termination phase in both groups, the knee angle was rapidly flexed in the beginning and then extended. However, although the knee joint of the middle-aged group was more bent in the initial termination phase and more extended after the 50% point of the termination phase (Fig. 4a), the change in angular velocity for both flexion and extension was larger in this group (Fig. 4b). Concerning the change of knee joint moment, both groups showed a slight flexion moment in the initial phase, and the extension moment increased until about the 20% point of the supporting stage before it decreased. There was a substantial difference in extension moment between the two groups (Fig. 4c).
Fig. 4.
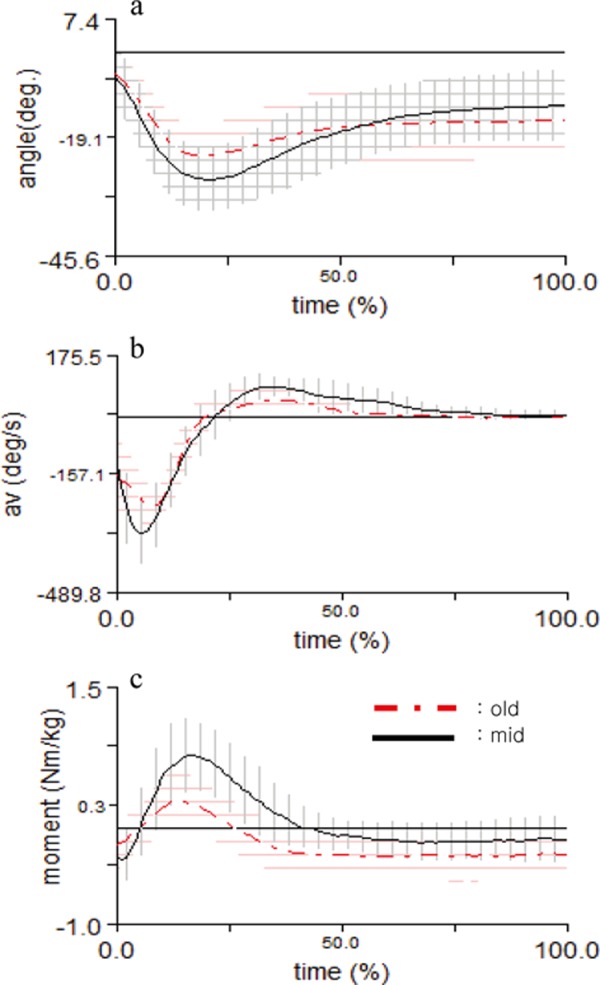
Variation pattern of principle variables in the knee
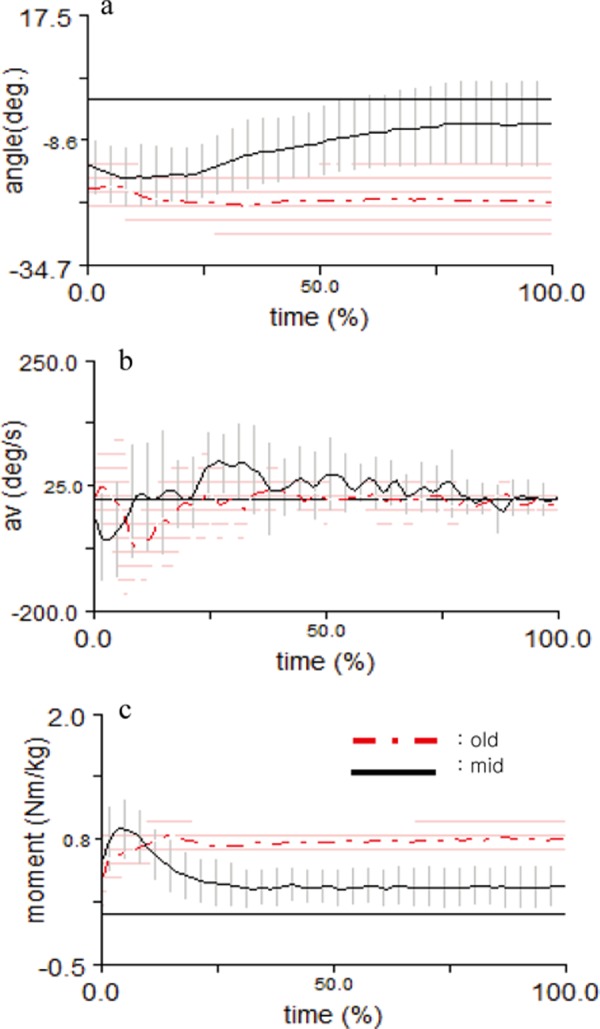
Concerning the change in hip joint angles, the hip joints of both groups were bent during the initial termination phase, with the hip joint of the elderly group being slightly more bent than that of the middle-aged group (Table 4). The difference was statistically significant. However, when the center of gravity completely stopped, the hip joint of the elderly group was more bent than in the initial termination phase, whereas the hip joint of the middle-aged group was extended. The difference was statistically significant.
Table 4. Kinetic and kinematic variables of hip (unit: deg., deg/s, Nm/kg).
| Angle | Min_av. | Moment | ||
|---|---|---|---|---|
| Event 1 | Event 2 | Phase 1 | Phase 1 | |
| Elderly group | −19.7 ± 4.0* | −22.4 ± 6.7* | −183.7 ± 69.6 | 1.0 ± 0.2 |
| Middle-aged group | −15.2 ± 3.2* | −7.2 ± 5.5* | −157.0 ± 53.8 | 0.9 ± 0.3 |
Values are expressed as the mean ± SD. *significant difference between group at p<0.05. Min_av: minimum angular velocity
Although the maximum flexion angular velocity of the hip joint was larger in the elderly group, the difference was not statistically significant. There was almost no difference in the maximum extension moment between the two groups, and the difference was not statistically significant.
The hip joint of the middle-aged group was bent in the initial termination phase before it became continuously extended, whereas that of the elderly group was bent in the initial phase and then remained bent, maintaining the same angle, throughout the termination phase (Fig. 5a). Both groups showed flexion angular velocity of the hip joint in the initial phase. Later, the middle-aged group showed extension angular velocity, whereas the elderly group did not show any change in angular velocity (Fig. 5b).
Fig. 5.
Variation pattern of principle variables in the hip
With respect to the patterns of change in the extension moment of the hip joint, the flexion moment of the middle-aged group, which increased during the initial termination phase, decreased to 20–25% of its initial value before and was then maintained at that level, whereas that of the elderly group gradually increased from the initial termination phase and was then maintained at an increased level until the center of gravity stopped (Fig. 5c).
DISCUSSION
The rapid increase of ground reaction force in the anterior/posterior and vertical axes in both groups during the termination phase can be explained by the strong pushing against the ground performed by the subjects as they attempted to stop walking unexpectedly. This supports the results of previous studies in which the walking speed was reduced by about 90% in the last step when subjects tried to stop walking unexpectedly17). This change in position can cause falls in the elderly by making them lose their balance21). The middle-aged group showed a larger maximum braking force and, subsequently, a larger decrease of the braking force than the elderly group because the younger group had a higher walking speed and response to external stimuli than the older group.
In the termination phase, the elderly group showed a smaller maximum flexion angular velocity of the ankle than the middle-aged group because their plantar flexion angle in the initial phase and the subsequent angle change during dorsiflexion was smaller than those of the middle-aged group. The rapid increase of the extension moment of the ankle during the initial phase can be explained by the large force generated to control the body, and the elderly group generated a smaller extension moment than the middle-aged group possibly because the older subjects had less muscular strength related to extension of the ankles than the younger subjects. The plantar flexion moment of the ankle contributes to supporting the body22) and is related to the reduction of muscular strength and the stability of the lower extremities10). Therefore, it is believed that the muscular strength related to flexion and extension of the ankle must be increased to increase the gait stability of the elderly and reduce their fall incidence rate.
The two groups showed similar knee joint angles during the termination phase; however, the joint angle range and maximum flexion and extension angular velocity of the elderly group were smaller than those of the middle-aged group. In particular, the difference in the extension moment of the knee joint between the two groups was more than twofold. To avoid a fall or collision in unexpected situations, the body can be stopped rapidly by effectively using the knee joints and thereby increasing bodily control. Furthermore, to increase the extension moment of the knees, the knee extensor needs to move more actively. However, elderly subjects have a low extension moment of the knee due to aging17, 23).
Concerning the change in hip joint angle, the middle-aged group showed slight flexion in the initial phase and then progressive extension, whereas the elderly group maintained the flexion angle. In particular, the extension moment of the elderly group was observed throughout the termination phase, unlike in the middle-aged group, and except in the early moments of the phase, the extension moment was much larger than that in the middle-aged group. These results are the opposite of the results found in relation to other joints and seemed to be related to the increase of energy consumption in certain joints to compensate for dysfunction in another joint24).
To stop while walking, the lower extremity making the last step must be extended without further accelerating the body or generating force in the flexion moment of joints. In comparison with the middle-aged group, the elderly group could not effectively use their ankles and knees while attempting to stop the body while walking. To compensate for the inefficiency of the ankle and knee joints, the elderly group used the hip joint more than the middle-aged group. The inefficiency of the ankle and knee joints can be explained by the weakened muscles in the lower extremities due to aging. In summary, decreased muscular strength in the lower extremities is closely related to falls; therefore, it is necessary to increase the muscular strength and flexibility of the lower limbs in order to prevent falls in the elderly. However, the variables that can contribute to falls in the elderly cannot be limited to a particular measure, and therefore, studies like require multilateral assessment and measurements. Future studies will need to include quantitative data related to threats to physical stability of the elderly and investigate muscle activities of the lower extremities on the basis of electromyographic evaluation.
REFERENCES
- 1.Gillespie LD, Robertson MC, Gillespie WJ, et al. : Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev, 2009, (2): CD007146. [DOI] [PubMed] [Google Scholar]
- 2.Prudham D, Evans JG: Factors associated with falls in the elderly: a community study. Age Ageing, 1981, 10: 141–146. [DOI] [PubMed] [Google Scholar]
- 3.Tinetti ME, Mendes de Leon CF, Doucette JT, et al. : Fear of falling and fall-related efficacy in relationship to functioning among community-living elders. J Gerontol, 1994, 49: M140–M147. [DOI] [PubMed] [Google Scholar]
- 4.O’Loughlin JL, Robitaille Y, Boivin JF, et al. : Incidence of and risk factors for falls and injurious falls among the community-dwelling elderly. Am J Epidemiol, 1993, 137: 342–354. [DOI] [PubMed] [Google Scholar]
- 5.Lee KJ, Shin SS, Song CH: The effect of biofeedback-based balance training while performing cognitive tasks on temporal and spatial parameters and gait stability of the elderly. J Phys Ther Sci, 2012, 24: 645–649. [Google Scholar]
- 6.Lee K, Lee S, Song C: Whole-body vibration training improves balance, muscle strength and glycosylated hemoglobin in elderly patients with diabetic neuropathy. Tohoku J Exp Med, 2013, 231: 305–314. [DOI] [PubMed] [Google Scholar]
- 7.Tinetti ME, Speechley M, Ginter SF: Risk factors for falls among elderly persons living in the community. N Engl J Med, 1988, 319: 1701–1707. [DOI] [PubMed] [Google Scholar]
- 8.Sparrow WA, Tirosh O: Gait termination: a review of experimental methods and the effects of ageing and gait pathologies. Gait Posture, 2005, 22: 362–371. [DOI] [PubMed] [Google Scholar]
- 9.Rao SS: Prevention of falls in older patients. Am Fam Physician, 2005, 72: 81–88. [PubMed] [Google Scholar]
- 10.Wolfson L, Judge J, Whipple R, et al. : Strength is a major factor in balance, gait, and the occurrence of falls. J Gerontol A Biol Sci Med Sci, 1995, 50: 64–67. [DOI] [PubMed] [Google Scholar]
- 11.Mills EM: The effect of low-intensity aerobic exercise on muscle strength, flexibility, and balance among sedentary elderly persons. Nurs Res, 1994, 43: 207–211. [PubMed] [Google Scholar]
- 12.Halliday SE, Winter DA, Frank JS, et al. : The initiation of gait in young, elderly, and Parkinson’s disease subjects. Gait Posture, 1998, 8: 8–14. [DOI] [PubMed] [Google Scholar]
- 13.Shin SS, An DH, Yoo WG: Comparison of gait velocity and center of mass during square and semicircular turning gaits between groups of elderly people with differing visual acuity. J Phys Ther Sci, 2015, 27: 387–388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Pai YC, Patton J: Center of mass velocity-position predictions for balance control. J Biomech, 1997, 30: 347–354. [DOI] [PubMed] [Google Scholar]
- 15.Tirosh O, Sparrow WA: Gait termination in young and older adults: effects of stopping stimulus probability and stimulus delay. Gait Posture, 2004, 19: 243–251. [DOI] [PubMed] [Google Scholar]
- 16.Bishop MD, Brunt D, Pathare N, et al. : The interaction between leading and trailing limbs during stopping in humans. Neurosci Lett, 2002, 323: 1–4. [DOI] [PubMed] [Google Scholar]
- 17.Bishop M, Brunt D, Pathare N, et al. : The effect of velocity on the strategies used during gait termination. Gait Posture, 2004, 20: 134–139. [DOI] [PubMed] [Google Scholar]
- 18.Braun BL: Knowledge and perception of fall-related risk factors and fall-reduction techniques among community-dwelling elderly individuals. Phys Ther, 1998, 78: 1262–1276. [DOI] [PubMed] [Google Scholar]
- 19.Jian Y, Winter DA, Ishac MG, et al. : Trajectory of the body COG and COP during initiation and termination of gait. Gait Posture, 1993, 1: 9–22. [Google Scholar]
- 20.Cao C, A Ashton-Miller J,Schultz AB, et al.: Effects of age, available response time and gender on ability to stop suddenly when walking. Gait Posture, 1998, 8: 103–109. [DOI] [PubMed] [Google Scholar]
- 21.Alexander NB: Postural control in older adults. J Am Geriatr Soc, 1994, 42: 93–108. [DOI] [PubMed] [Google Scholar]
- 22.Kepple TM, Siegel KL, Stanhope SJ: Relative contributions of the lower extremity joint moments to forward progression and support during gait. Gait Posture, 1997, 6: 1–8. [Google Scholar]
- 23.Riley PO, DellaCroce U, Kerrigan DC: Effect of age on lower extremity joint moment contributions to gait speed. Gait Posture, 2001, 14: 264–270. [DOI] [PubMed] [Google Scholar]
- 24.McGibbon CA, Krebs DE, Puniello MS: Mechanical energy analysis identifies compensatory strategies in disabled elders’ gait. J Biomech, 2001, 34: 481–490. [DOI] [PubMed] [Google Scholar]