

Abstract
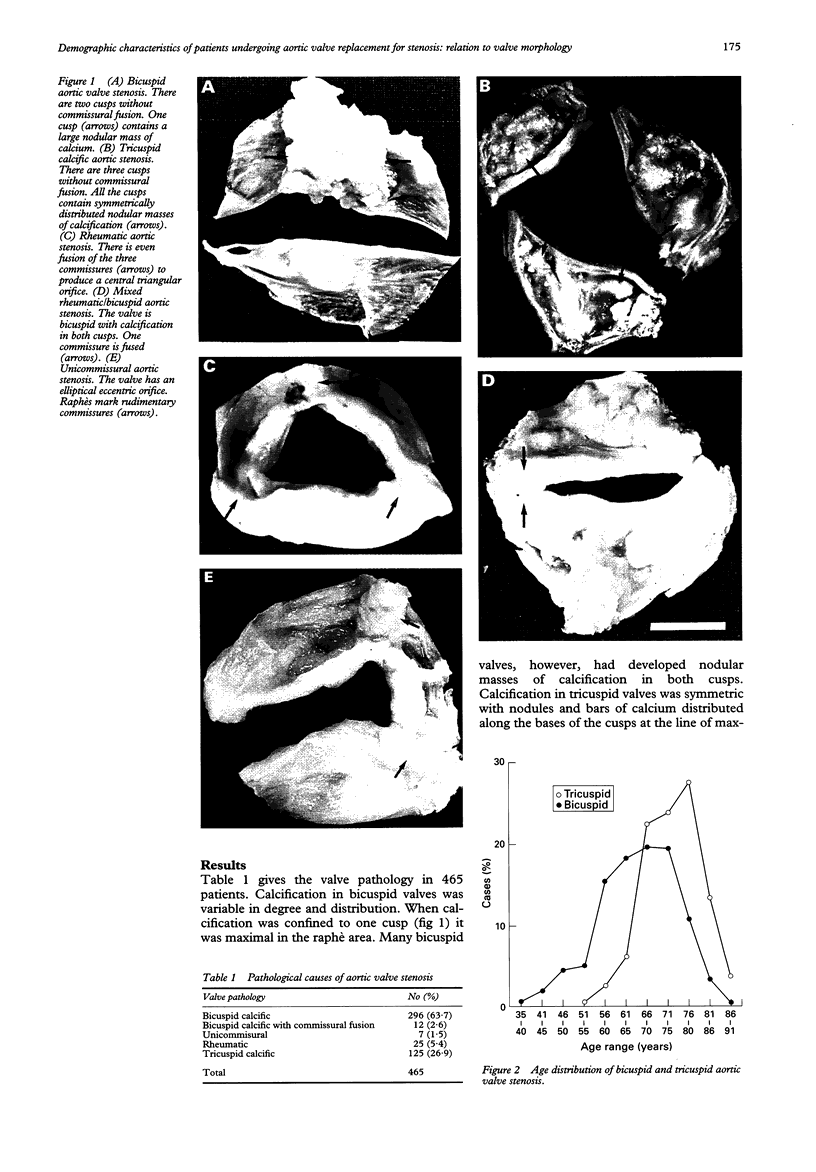
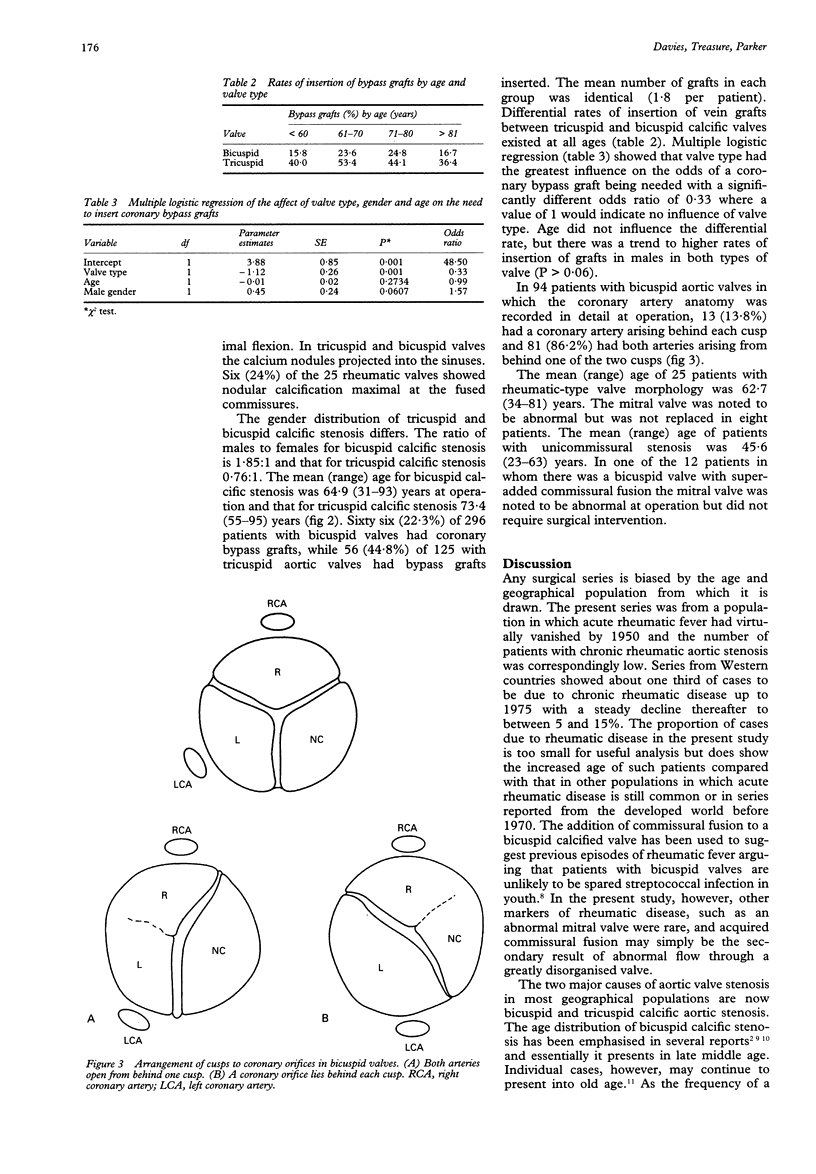
OBJECTIVE: To determine the relative importance of the different causes of isolated aortic valve stenosis in a surgical series, and to relate these to patient characteristics including the rate of insertion of bypass grafts for coronary artery disease. DESIGN: Survey of the clinical and pathological data on patients undergoing aortic valve replacement for isolated stenosis. SETTING: Tertiary care cardiothoracic surgical unit. PATIENTS AND METHODS: 465 adult patients undergoing aortic valve replacement representing a consecutive series in one surgical unit. Retrospective review of patients records and classification of cause of aortic stenosis based on pathological examination of excised valve cusps. RESULTS: 63.7% patients had calcific bicuspid valves, 26.9% tricuspid calcific valves, and 5.4% rheumatic, 2.6% mixed pathology and 1.5% unicommissural valves. The ratio of males to females for bicuspid valves was 1.85:1 and for tricuspid calcific valves 0.76:1. The mean age of patients with bicuspid valves was 64.9 years compared with 73.4 years for those with tricuspid valves. Some 22.3% of patients with bicuspid valves and 44.8% of those with tricuspid valves had sufficient coronary artery disease to necessitate insertion of coronary bypass grafts. The differential rate of insertion of coronary bypass grafts was independent of age. CONCLUSIONS: Bicuspid calcified aortic valves are the predominant cause of isolated aortic valve stenosis followed by tricuspid calcified aortic valves. The sex and age distribution of bicuspid and tricuspid calcific aortic valve stenosis is different. The higher rate of insertion of vascular grafts in tricuspid calcific aortic valves may indicate that risk factors for atherosclerosis enhance cusp calcification in these patients.
Full text
PDF


Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Aronow W. S., Schwartz K. S., Koenigsberg M. Correlation of serum lipids, calcium, and phosphorus, diabetes mellitus and history of systemic hypertension with presence or absence of calcified or thickened aortic cusps or root in elderly patients. Am J Cardiol. 1987 Apr 15;59(9):998–999. doi: 10.1016/0002-9149(87)91144-1. [DOI] [PubMed] [Google Scholar]
- Isner J. M., Chokshi S. K., DeFranco A., Braimen J., Slovenkai G. A. Contrasting histoarchitecture of calcified leaflets from stenotic bicuspid versus stenotic tricuspid aortic valves. J Am Coll Cardiol. 1990 Apr;15(5):1104–1108. doi: 10.1016/0735-1097(90)90249-o. [DOI] [PubMed] [Google Scholar]
- Karalis D. G., Wahl J. M., Mintz G. S., Chandrasekaran K. Severe stenosis involving a congenitally bicuspid aortic valve in the tenth decade of life. Am J Cardiol. 1990 Jan 15;65(3):264–265. doi: 10.1016/0002-9149(90)90102-7. [DOI] [PubMed] [Google Scholar]
- Lindroos M., Kupari M., Heikkilä J., Tilvis R. Prevalence of aortic valve abnormalities in the elderly: an echocardiographic study of a random population sample. J Am Coll Cardiol. 1993 Apr;21(5):1220–1225. doi: 10.1016/0735-1097(93)90249-z. [DOI] [PubMed] [Google Scholar]
- Lindroos M., Kupari M., Valvanne J., Strandberg T., Heikkilä J., Tilvis R. Factors associated with calcific aortic valve degeneration in the elderly. Eur Heart J. 1994 Jul;15(7):865–870. doi: 10.1093/oxfordjournals.eurheartj.a060602. [DOI] [PubMed] [Google Scholar]
- Maher E. R., Pazianas M., Curtis J. R. Calcific aortic stenosis: a complication of chronic uraemia. Nephron. 1987;47(2):119–122. doi: 10.1159/000184472. [DOI] [PubMed] [Google Scholar]
- Mautner G. C., Mautner S. L., Cannon R. O., 3rd, Hunsberger S. A., Roberts W. C. Clinical factors useful in predicting aortic valve structure in patients > 40 years of age with isolated valvular aortic stenosis. Am J Cardiol. 1993 Jul 15;72(2):194–198. doi: 10.1016/0002-9149(93)90159-a. [DOI] [PubMed] [Google Scholar]
- Niederle B., Stefenelli T., Glogar D., Woloszczuk W., Roka R., Mayr H. Cardiac calcific deposits in patients with primary hyperparathyroidism: preliminary results of a prospective echocardiographic study. Surgery. 1990 Dec;108(6):1052–1057. [PubMed] [Google Scholar]
- Nistal J. F., Garcia-Martinez V., Fernandez M. D., Hurle A., Hurle J. M., Revuelta J. M. Age-dependent dystrophic calcification of the aortic valve leaflets in normal subjects. J Heart Valve Dis. 1994 Jan;3(1):37–40. [PubMed] [Google Scholar]
- Otto C. M., Kuusisto J., Reichenbach D. D., Gown A. M., O'Brien K. D. Characterization of the early lesion of 'degenerative' valvular aortic stenosis. Histological and immunohistochemical studies. Circulation. 1994 Aug;90(2):844–853. doi: 10.1161/01.cir.90.2.844. [DOI] [PubMed] [Google Scholar]
- Ouchi Y., Akishita M., de Souza A. C., Nakamura T., Orimo H. Age-related loss of bone mass and aortic/aortic valve calcification--reevaluation of recommended dietary allowance of calcium in the elderly. Ann N Y Acad Sci. 1993 Mar 15;676:297–307. doi: 10.1111/j.1749-6632.1993.tb38743.x. [DOI] [PubMed] [Google Scholar]
- Pomerance A. Pathogenesis of aortic stenosis and its relation to age. Br Heart J. 1972 Jun;34(6):569–574. doi: 10.1136/hrt.34.6.569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roberts W. C. Anatomically isolated aortic valvular disease. The case against its being of rheumatic etiology. Am J Med. 1970 Aug;49(2):151–159. doi: 10.1016/s0002-9343(70)80070-5. [DOI] [PubMed] [Google Scholar]
- Roberts W. C. The congenitally bicuspid aortic valve. A study of 85 autopsy cases. Am J Cardiol. 1970 Jul;26(1):72–83. doi: 10.1016/0002-9149(70)90761-7. [DOI] [PubMed] [Google Scholar]
- Roberts W. C. The structure of the aortic valve in clinically isolated aortic stenosis: an autopsy study of 162 patients over 15 years of age. Circulation. 1970 Jul;42(1):91–97. doi: 10.1161/01.cir.42.1.91. [DOI] [PubMed] [Google Scholar]
- Sadée A. S., Becker A. E., Verheul J. A. The congenital bicuspid aortic valve with post-inflammatory disease--a neglected pathological diagnosis of clinical relevance. Eur Heart J. 1994 Apr;15(4):503–506. doi: 10.1093/oxfordjournals.eurheartj.a060534. [DOI] [PubMed] [Google Scholar]
- Strickberger S. A., Schulman S. P., Hutchins G. M. Association of Paget's disease of bone with calcific aortic valve disease. Am J Med. 1987 May;82(5):953–956. doi: 10.1016/0002-9343(87)90157-4. [DOI] [PubMed] [Google Scholar]
- Subramanian R., Olson L. J., Edwards W. D. Surgical pathology of pure aortic stenosis: a study of 374 cases. Mayo Clin Proc. 1984 Oct;59(10):683–690. doi: 10.1016/s0025-6196(12)62057-6. [DOI] [PubMed] [Google Scholar]
- Turri M., Thiene G., Bortolotti U., Milano A., Mazzucco A., Gallucci V. Surgical pathology of aortic valve disease. A study based on 602 specimens. Eur J Cardiothorac Surg. 1990;4(10):556–560. doi: 10.1016/1010-7940(90)90145-p. [DOI] [PubMed] [Google Scholar]
- Vollebergh F. E., Becker A. E. Minor congenital variations of cusp size in tricuspid aortic valves. Possible link with isolated aortic stenosis. Br Heart J. 1977 Sep;39(9):1006–1011. doi: 10.1136/hrt.39.9.1006. [DOI] [PMC free article] [PubMed] [Google Scholar]