

Abstract
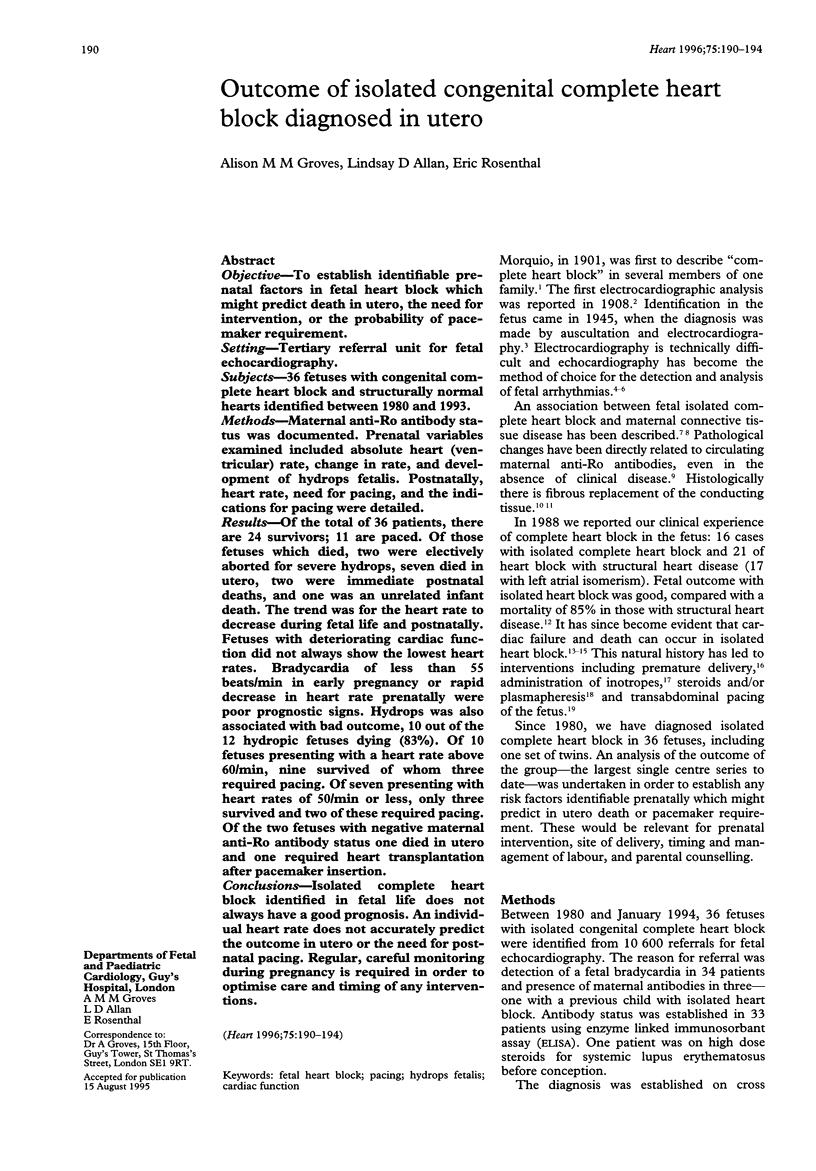
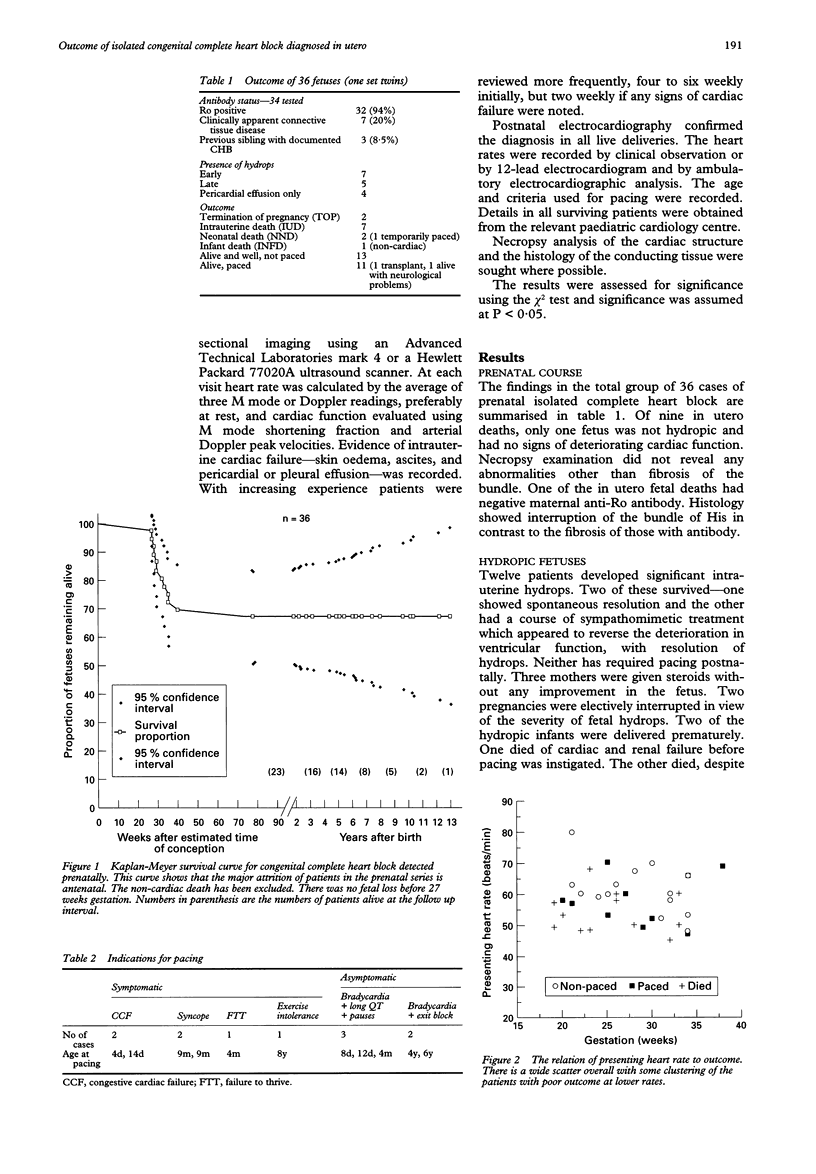
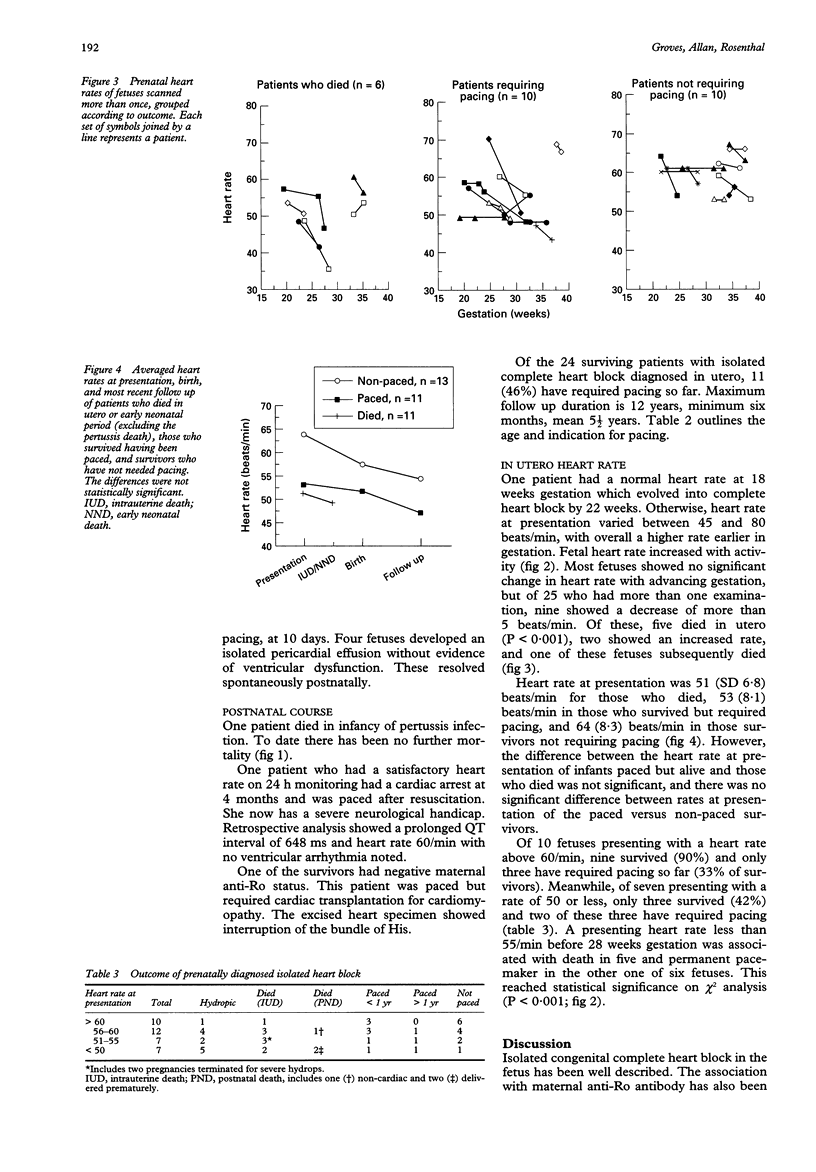
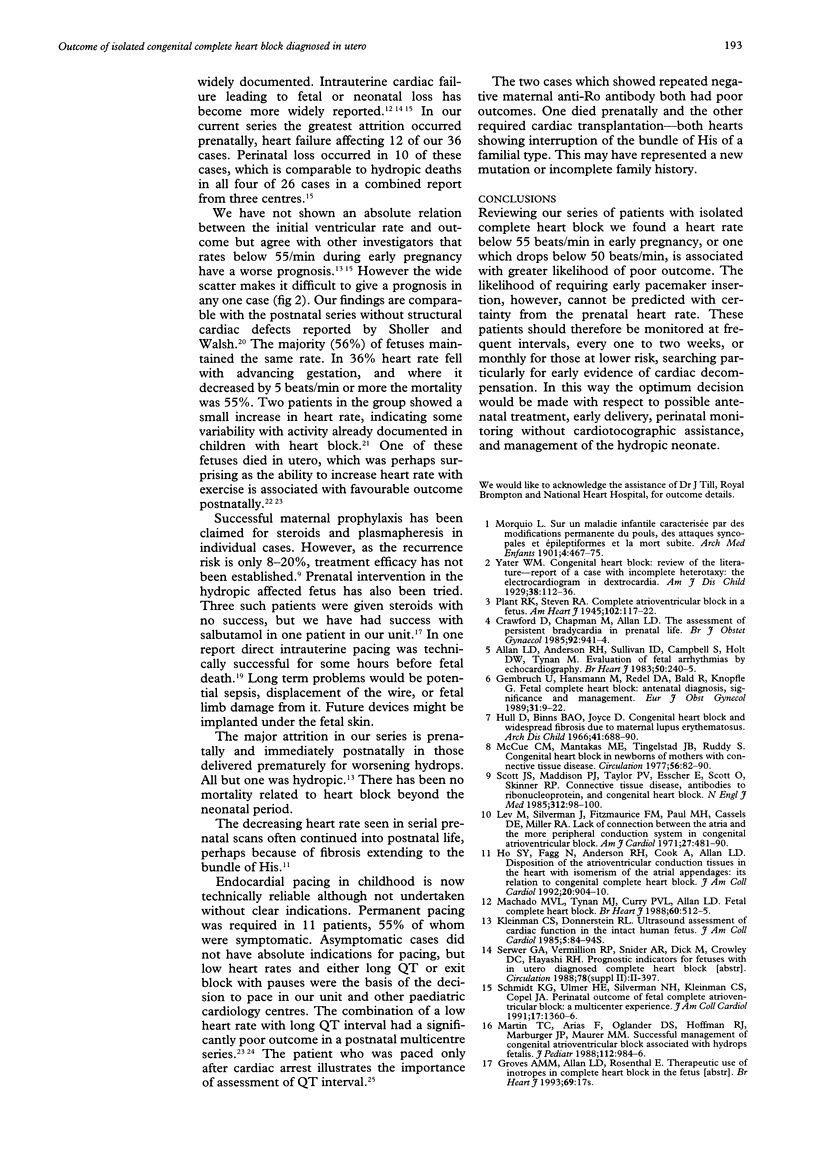
OBJECTIVE: To establish identifiable prenatal factors in fetal heart block which might predict death in utero, the need for intervention, or the probability of pacemaker requirement. SETTING: Tertiary referral unit for fetal echocardiography. SUBJECTS: 36 fetuses with congenital complete heart block and structurally normal hearts identified between 1980 and 1993. METHODS: Maternal anti-Ro antibody status was documented. Prenatal variables examined included absolute heart (ventricular) rate, change in rate, and development of hydrops fetalis. Postnatally, heart rate, need for pacing, and the indications for pacing were detailed. RESULTS: Of the total of 36 patients, there are 24 survivors; 11 are paced. Of those fetuses which died, two were electively aborted for severe hydrops, seven died in utero, two were immediate postnatal deaths, and one was an unrelated infant death. The trend was for the heart rate to decrease during fetal life and postnatally. Fetuses with deteriorating cardiac function did not always show the lowest heart rates. Bradycardia of less than 55 beats/min in early pregnancy or rapid decrease in heart rate prenatally were poor prognostic signs. Hydrops was also associated with bad outcome, 10 out of the 12 hydropic fetuses dying (83%). Of 10 fetuses presenting with a heart rate above 60/min, nine survived of whom three required pacing. Of seven presenting with heart rates of 50/min or less, only three survived and two of these required pacing. Of the two fetuses with negative maternal anti-Ro antibody status one died in utero and one required heart transplantation after pacemaker insertion. CONCLUSIONS: Isolated complete heart block identified in fetal life does not always have a good prognosis. An individual heart rate does not accurately predict the outcome in utero or the need for postnatal pacing. Regular, careful monitoring during pregnancy is required in order to optimise care and timing of any interventions.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Allan L. D., Anderson R. H., Sullivan I. D., Campbell S., Holt D. W., Tynan M. Evaluation of fetal arrhythmias by echocardiography. Br Heart J. 1983 Sep;50(3):240–245. doi: 10.1136/hrt.50.3.240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barclay C. S., French M. A., Ross L. D., Sokol R. J. Successful pregnancy following steroid therapy and plasma exchange in a woman with anti-Ro (SS-A) antibodies. Case report. Br J Obstet Gynaecol. 1987 Apr;94(4):369–371. doi: 10.1111/j.1471-0528.1987.tb03107.x. [DOI] [PubMed] [Google Scholar]
- Carpenter R. J., Jr, Strasburger J. F., Garson A., Jr, Smith R. T., Deter R. L., Engelhardt H. T., Jr Fetal ventricular pacing for hydrops secondary to complete atrioventricular block. J Am Coll Cardiol. 1986 Dec;8(6):1434–1436. doi: 10.1016/s0735-1097(86)80319-9. [DOI] [PubMed] [Google Scholar]
- Crawford D., Chapman M., Allan L. The assessment of persistent bradycardia in prenatal life. Br J Obstet Gynaecol. 1985 Sep;92(9):941–944. doi: 10.1111/j.1471-0528.1985.tb03074.x. [DOI] [PubMed] [Google Scholar]
- Dewey R. C., Capeless M. A., Levy A. M. Use of ambulatory electrocardiographic monitoring to identify high-risk patients with congenital complete heart block. N Engl J Med. 1987 Apr 2;316(14):835–839. doi: 10.1056/NEJM198704023161403. [DOI] [PubMed] [Google Scholar]
- Esscher E., Michaëlsson M. Q-T interval in congenital complete heart block. Pediatr Cardiol. 1983 Apr-Jun;4(2):121–124. doi: 10.1007/BF02076336. [DOI] [PubMed] [Google Scholar]
- Gembruch U., Hansmann M., Redel D. A., Bald R., Knöpfle G. Fetal complete heart block: antenatal diagnosis, significance and management. Eur J Obstet Gynecol Reprod Biol. 1989 Apr;31(1):9–22. doi: 10.1016/0028-2243(89)90022-1. [DOI] [PubMed] [Google Scholar]
- Ho S. Y., Fagg N., Anderson R. H., Cook A., Allan L. Disposition of the atrioventricular conduction tissues in the heart with isomerism of the atrial appendages: its relation to congenital complete heart block. J Am Coll Cardiol. 1992 Oct;20(4):904–910. doi: 10.1016/0735-1097(92)90191-o. [DOI] [PubMed] [Google Scholar]
- Hull D., Binns B. A., Joyce D. Congenital heart block and widespread fibrosis due to maternal lupus erythematosus. Arch Dis Child. 1966 Dec;41(220):688–690. doi: 10.1136/adc.41.220.688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karpawich P. P., Gillette P. C., Garson A., Jr, Hesslein P. S., Porter C. B., McNamara D. G. Congenital complete atrioventricular block: clinical and electrophysiologic predictors of need for pacemaker insertion. Am J Cardiol. 1981 Dec;48(6):1098–1102. doi: 10.1016/0002-9149(81)90326-x. [DOI] [PubMed] [Google Scholar]
- Kleinman C. S., Donnerstein R. L. Ultrasonic assessment of cardiac function in the intact human fetus. J Am Coll Cardiol. 1985 Jan;5(1 Suppl):84S–94S. doi: 10.1016/s0735-1097(85)80149-2. [DOI] [PubMed] [Google Scholar]
- Lev M., Silverman J., Fitzmaurice F. M., Paul M. H., Cassels D. E., Miller R. A. Lack of connection between the atria and the more peripheral conduction system in congenital atrioventricular block. Am J Cardiol. 1971 May;27(5):481–490. doi: 10.1016/0002-9149(71)90410-3. [DOI] [PubMed] [Google Scholar]
- Litsey S. E., Noonan J. A., O'Connor W. N., Cottrill C. M., Mitchell B. Maternal connective tissue disease and congenital heart block. Demonstration of immunoglobulin in cardiac tissue. N Engl J Med. 1985 Jan 10;312(2):98–100. doi: 10.1056/NEJM198501103120206. [DOI] [PubMed] [Google Scholar]
- Machado M. V., Tynan M. J., Curry P. V., Allan L. D. Fetal complete heart block. Br Heart J. 1988 Dec;60(6):512–515. doi: 10.1136/hrt.60.6.512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martin T. C., Arias F., Olander D. S., Hoffman R. J., Marbarger J. P., Maurer M. M. Successful management of congenital atrioventricular block associated with hydrops fetalis. J Pediatr. 1988 Jun;112(6):984–986. doi: 10.1016/s0022-3476(88)80231-2. [DOI] [PubMed] [Google Scholar]
- McCue C. M., Mantakas M. E., Tingelstad J. B., Ruddy S. Congenital heart block in newborns of mothers with connective tissue disease. Circulation. 1977 Jul;56(1):82–90. doi: 10.1161/01.cir.56.1.82. [DOI] [PubMed] [Google Scholar]
- Michaëlsson M., Engle M. A. Congenital complete heart block: an international study of the natural history. Cardiovasc Clin. 1972;4(3):85–101. [PubMed] [Google Scholar]
- Pinsky W. W., Gillette P. C., Garson A., Jr, McNamara D. G. Diagnosis, management, and long-term results of patients with congenital complete atrioventricular block. Pediatrics. 1982 Jun;69(6):728–733. [PubMed] [Google Scholar]
- Schmidt K. G., Ulmer H. E., Silverman N. H., Kleinman C. S., Copel J. A. Perinatal outcome of fetal complete atrioventricular block: a multicenter experience. J Am Coll Cardiol. 1991 May;17(6):1360–1366. doi: 10.1016/s0735-1097(10)80148-2. [DOI] [PubMed] [Google Scholar]
- Sholler G. F., Walsh E. P. Congenital complete heart block in patients without anatomic cardiac defects. Am Heart J. 1989 Dec;118(6):1193–1198. doi: 10.1016/0002-8703(89)90009-4. [DOI] [PubMed] [Google Scholar]