

Abstract
A 76-year-old male presented with angina and a large retrosternal goitre causing marked dyspnoea. Coronary angiography revealed triple vessel disease and moderately impaired left ventricular function. CT imaging demonstrated a substantial multinodular goitre extending into the posterior mediastinum to the level of the carina, with associated compression of the trachea and oesophagus. Preoperative thyroid function tests showed euthyroid state. The patient subsequently underwent off-pump coronary artery bypass grafting (OPCABG) ×2 with concomitant total thyroidectomy. A thyroid mass of dimensions 19 cm × 16 cm × 5.5 cm and weight 439 g was confirmed to be a multinodular goitre. Postoperative complications included bilateral recurrent laryngeal nerve damage, hypocalcaemia and ventilator-associated pneumonia. The patient was discharged 36 days postoperatively and remained asymptomatic at 1 year follow up. This case provides further evidence that concomitant OPCABG and thyroidectomy for the treatment of large retrosternal goitre can be safely and effectively performed, provided that perioperative levels of thyroid hormones are maintained at euthyroid or hypothyroid levels.
Keywords: Off-pump coronary artery bypass grafting (OPCABG), total thyroidectomy, retrosternal goitre, multinodular goitre
Introduction
Retrosternal goitre results when a proportion of at least 50% of the thyroid gland descends into the mediastinum. The documented incidence ranges from 0.02–0.5% in the general population and 2.6–21% in thyroidectomy patients, accounting for 3–12% of all mediastinal tumours (1,2). Clinical presentation may be associated with manifestations of thyroid dysfunction, as well as tracheal and oesophageal compression symptoms. Sternotomy is the indicated surgical approach if the retrosternal portion is large, thyroid tissue extends below the level of the aortic arch, invasive malignancy is likely or confirmed, or if there is existing adherence to surrounding mediastinal structures (3,4).
Thyroid disease affects cardiovascular physiology, presenting in up to 11% of patients with coronary artery or valvular heart disease (5). Whilst concomitant cardiac and thyroid procedures have been discussed in literature, no consensus exists regarding the optimal surgical management of such cases. Herein, we present a case of simultaneous off-pump coronary artery bypass grafting (OPCABG) and total thyroidectomy, followed by a review of the current literature on this subject. It is our view that in patients displaying severe cardiac ischaemia in conjunction with retrosternal goitre, concomitant CABG and thyroidectomy is the treatment of choice.
Case presentation
A 76-year-old male presented with sudden onset precordial pain. Relevant past medical history included angina pectoris (Canadian Cardiovascular Society Grade I) and dyspnoea (New York Heart Association Functional Class III). In addition, the patient suffered from stage III chronic kidney disease, type 2 diabetes mellitus, hyperlipidaemia and severe bilateral knee osteoarthritis. Previous procedures included transurethral resection of the prostate and bilateral inguinal hernia repair. With respect to social history, he was a lifelong non-smoker.
On admission, electrocardiogram showed new left bundle branch block, with troponin level within normal range. The patient underwent coronary angiography with the following findings: The left main stem (LMS) had no significant disease, but was calcified. The left anterior descending artery (LAD) was 80–90% proximally occluded, with a severe lesion in the large first diagonal branch and a less severe lesion located distally. The left circumflex artery had a severe proximal occlusive lesion just before the first obtuse marginal branch (Figure 1). The right coronary artery (RCA) was diffusely diseased with a 40–50% lesion in the mid-vessel and an 80–90% occlusion before the crux (Figure 2). A left ventricular angiography demonstrated anterior wall hypokinesis and moderately impaired left ventricular function.
Figure 1.
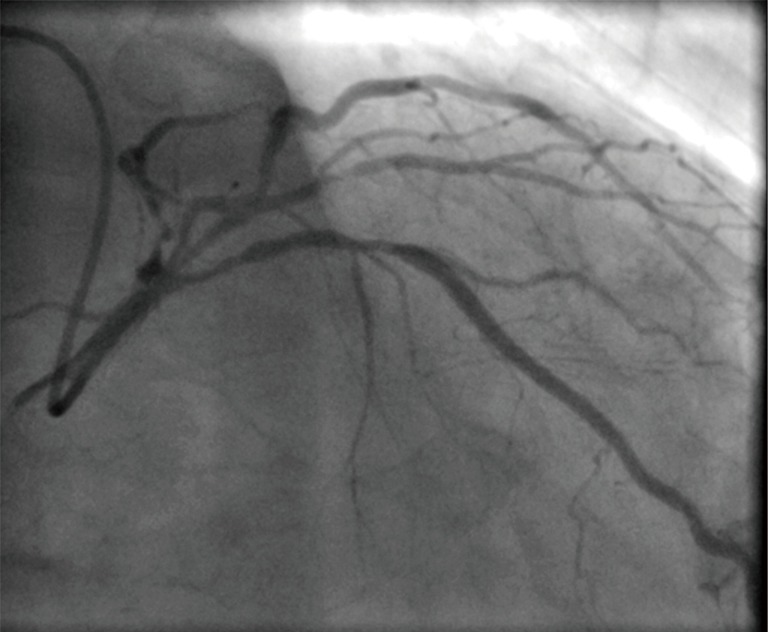
Coronary angiography demonstrating occlusive lesions of the left anterior descending artery, the first diagonal branch and the circumflex artery.
Figure 2.

Coronary angiography revealing diffuse disease of the right coronary artery.
Chest radiograph had revealed superior mediastinum enlargement (Figure 3) and a subsequent CT scan of neck, chest and abdomen showed a large, calcified, multinodular goitre descending into the posterior mediastinum to the level of the carina. It displaced the great vessels, trachea and oesophagus to the right, compressing both of the latter structures (Figure 4). Pulmonary function tests revealed forced expiratory volume in 1 second (FEV1) 117%, forced vital capacity (FVC) 122% and peak expiratory flow rate (PEFR) 79%.
Figure 3.
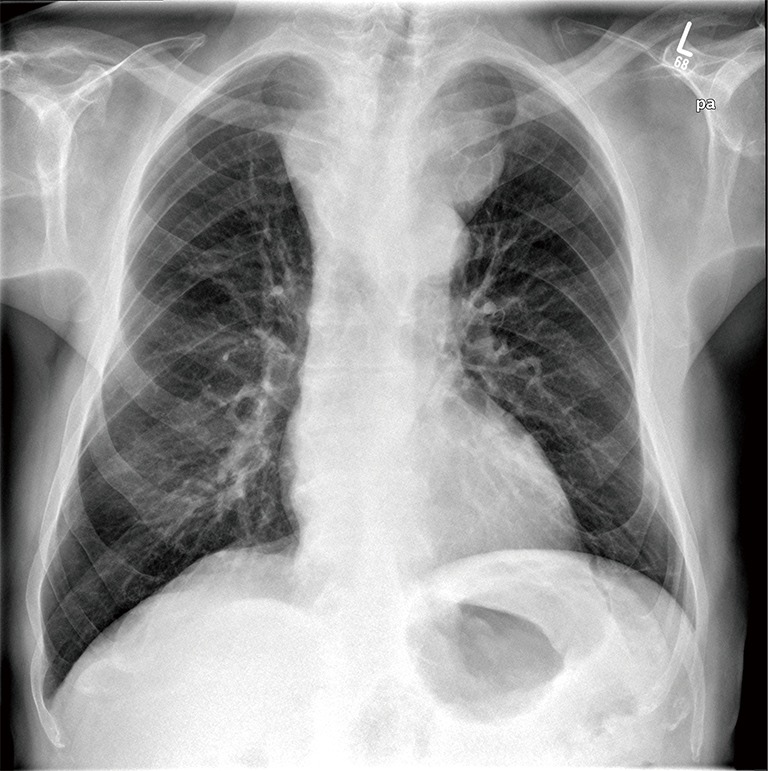
Chest radiograph showing significant superior mediastinal enlargement.
Figure 4.

Axial computed tomography of the chest displaying a huge, multinodular goitre extending into the posterior mediastinum. It displaces the trachea and oesophagus to the right, compressing both these structures, and contains several areas of calcification.
Due to the goitre location, a cardiac procedure with endocrine surgical input was planned. Preoperative assessment revealed left recurrent laryngeal nerve palsy and thyroid function tests showed euthyroid state. EuroSCORE values were an additive score of 9 and a logistic score of 13.71. A Parsonnet score of 19 (hard data) was determined.
The patient underwent concomitant OPCABG ×2 with total thyroidectomy, with the endocrine component of the operation performed first. A median sternotomy incision was made, to which a subsequent 6 cm transverse incision was joined to form a ‘T’ shape. Following division and lateral retraction of strap muscles, each thyroid lobe was approached separately and excised with division of the isthmus (Figures 5,6). After ligation and division of the superior thyroid vessels, the upper pole was mobilised. The superior parathyroid glands were identified and fully preserved. No middle thyroid vein was visualised. The lower pole was mobilised in a corresponding manner. Separation of the thyroid from the trachea, oesophagus and surrounding structures was then completed. Due to a difficult anatomical dissection, damage was incurred to both recurrent laryngeal nerves.
Figure 5.
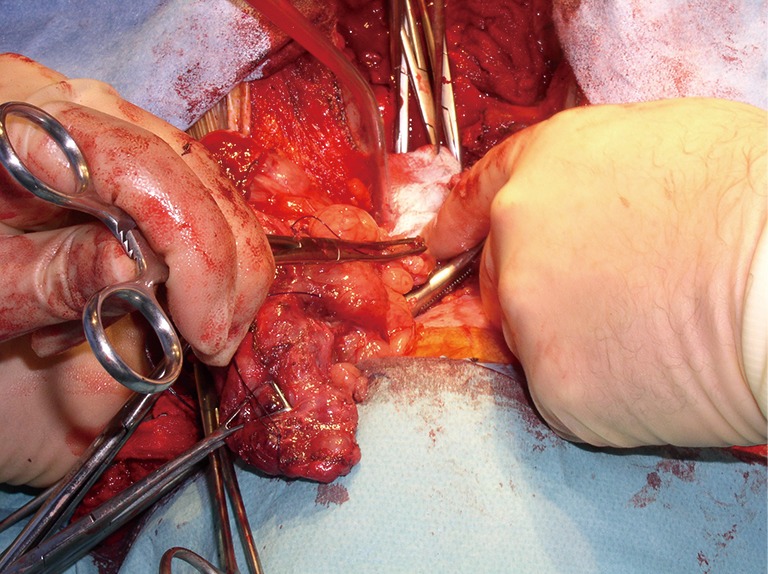
Mobilisation of the left thyroid lobe.
Figure 6.
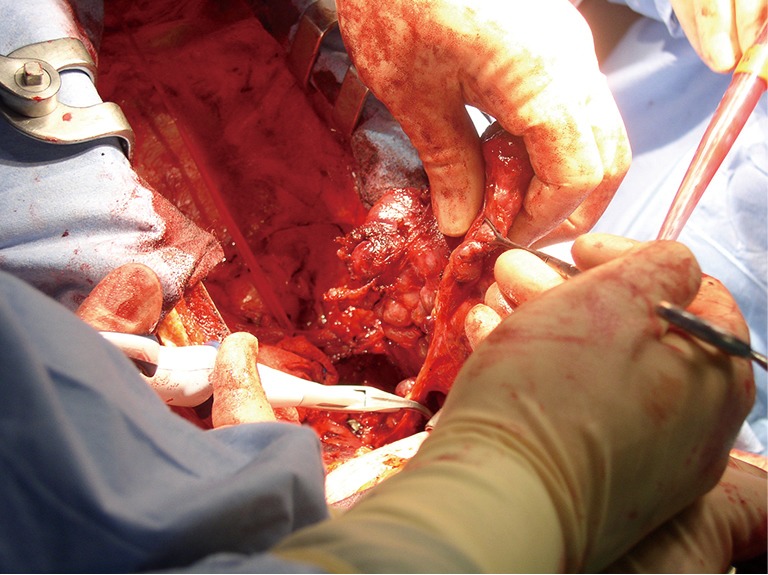
Mobilisation of the right thyroid lobe.
An intra-aortic balloon pump was inserted prior to the cardiac aspect of the operation. No cardiopulmonary bypass or cross-clamping of the aorta was implemented and the core temperature was sustained at 37 °C. Only 1 mg/kg body weight of heparin was administered intravenously, in order to minimise bleeding from the extensive raw mediastinal surfaces. Saphenous veins were not suitable for grafting. The patient underwent pedicled left internal mammary artery grafting to LAD and radial artery to distal RCA, with the proximal end of the radial artery anastomosed on the aorta. Ventricular pacing wires were placed and closure was carried out in layers, with the sternum approximated using three loop stainless steel wires.
Cardiac surgery ICU and HDU recovery period lasted 26 days. The patient was commenced on thyroid hormone replacement therapy and calcium and vitamin D supplements. Sequelae included a failed extubation on day two due to bilateral vocal cord palsy, and resultant prolonged endotracheal intubation, with a tracheostomy performed on day 8. An extended ventilator-weaning period necessitated the commencement of nasogastric feeding between days 13–25. Other postoperative complications included ventilator-associated pneumonia, initially treated with piperacillin/tazobactam and subsequently changed to meropenem following sensitivity results. Anaemia required transfusion of 2 units of packed red blood cells. As the patient also exhibited transient hypertension and frank haematuria, outpatient flexible cystoscopy was arranged as per urology review. On day 26 the patient was transferred to the care of the otolaryngology team. He remained in hospital for a further 10 days and was then discharged.
The thyroid was subject to pathological examination. The gland was of substantial size, weighing 439 g and measuring 19 cm × 16 cm × 5.5 cm. A multinodular appearance was noted with respect to both lobes (Figure 7). Histological examination showed considerable variation in follicular size and colloid content with small areas of fibrosis and dystrophic calcification. There was no evidence of malignancy.
Figure 7.

The excised multinodular goitre of dimensions 19 cm × 16 cm × 5.5 cm.
At 1-year follow up the patient remained asymptomatic. The right vocal cord function had improved and tracheostomy had since been reversed. The patient was confirmed to be euthyroid and was discharged from both cardiac and endocrine surgical care.
Discussion
In general, combined cardiac surgery and thyroidectomy is regarded as a safe and efficacious procedure with good clinical outcomes. A recent review of the existing literature determined 16 key papers (3 retrospective case series and 13 case reports) on this topic (6). However, of a total cohort of 32 patients, only four underwent concomitant OPCABG with total thyroidectomy for a retrosternal goitre. In the first report, Mehta et al. (7) documented the case of a 66-year-old female with unstable angina (LMS disease) and severely compromised airway secondary to a multinodular retrosternal goitre. Initially, a subtotal thyroidectomy was performed, followed by OPCABG with saphenous vein grafts to the LAD and the ramus intermedius, with the absence of intraoperative complications. Following a slow ventilator-weaning period, the patient was returned to theatre for extubation under general anaesthesia, due to development of post-intubation tracheomalacia. The patient was discharged on the 8th day postoperatively, with normal respiratory and cardiac function and euthyroid hormone levels. In the second case report, Mehra et al. (8) performed combined OPCABG and thyroidectomy on a 70-year-old woman with extensive coronary artery disease, involving the LMS, and tracheal compression as a consequence of a retrosternal goitre. They reported a successful procedure, with no resultant postoperative complications. As a consequence of this combined approach, normal cardiovascular function and upper airway patency were established, with the patient discharged on postoperative day 10. In the third case report, this same combined procedure was performed on a 57-year-old female with coronary artery disease, which included 95% in-stent restenosis of the LAD, accompanied by a large retrosternal goitre (9). The reported postoperative period was uneventful and the patient was discharged 5 days later. Finally, in one case from the retrospective series reported by Testini et al. (10), a total thyroidectomy followed by CABG was performed. All the cases from the aforementioned 16 key papers which involved a combined procedure of isolated CABG and thyroidectomy are presented in Table 1.
Table 1. Combined procedure of isolated coronary artery bypass grafting and thyroidectomy.
| Author, year, country | Age, gender: clinical presentation | Cardiac pathology | Thyroid pathology (thyroid function) | Operation | Outcomes |
|---|---|---|---|---|---|
| Cetin et al., 2014, Turkey (9) | 57-year-old female: cough | 95% in-stent restenosis of LAD | Retrosternal goitre (euthyroid) | Subtotal thyroidectomy followed by OPCABG ×1 | Successful operation. Nil postoperative complications. Patient discharged on day 5 with euthyroid hormone levels. Well at 6-month follow-up |
| Gürkan et al., 2012, Turkey (11) | 65-year-old male: asymptomatic | Sub-occlusive lesion of RCA and Cx, total proximal occlusion of LAD | Retrosternal multinodular goitre (euthyroid) | Subtotal thyroidectomy followed by CABG ×3 | Nil intra- or post-operative complications. Patient discharged on day 7 with euthyroid hormone levels |
| Koçak et al., 2007, Turkey (12) | 47-year-old male: angina, dyspnoea, limitation of cervical movements | Coronary artery disease (no further details documented) | Multinodular goitre (hyperthyroid) | Total thyroidectomy followed by CABG ×3 | Nil intra- or post-operative complications. Patient discharged on day 9 with euthyroid hormone levels. Well at 1-year follow-up |
| Litmathe et al., 2004, Germany (13) | 67-year-old male: angina, dyspnoea | Coronary artery disease (no further details documented) | Multinodular goitre (euthyroid) | Goitre resection and CABG with LIMA (no further details documented) | No symptoms of cardiac ischaemia at follow-up (no further details documented) |
| 65-year-old male: angina, dyspnoea | Coronary artery disease (no further details documented) | Retrosternal multinodular goitre (euthyroid) | Goitre resection and CABG with LIMA (no further details documented) | Intraoperative death | |
| Mehra et al., 2009, India (8) | 70-year-old female: myocardial infarction, dyspnoea, cachexia, anaemia | 80% occlusion of LMS, 70% proximal stenosis of LAD, 30–40% ostial narrowing of Cx, 80% occlusion of RCA | Retrosternal multinodular goitre causing tracheal compression (euthyroid) | OPCABG ×3 followed by total thyroidectomy | Nil intra- or post-operative complications. Patient discharged on day 10 with euthyroid hormone levels. Well at 6-month follow-up |
| Mehta et al., 2005, India (7) | 66-year-old female: angina | Double vessel disease with 60% stenosis of LMS | Retrosternal multinodular goitre causing significant tracheal stenosis (hypothyroid) | Subtotal thyroidectomy followed by OPCABG ×2 | Nil intraoperative complications. Patient returned to theatre for extubation under general anaesthesia, following post-intubation tracheomalacia; discharged on postoperative day 8 with euthyroid hormone levels |
| Testini et al., 2010, Italy (10) | 51-year-old female: dysphagia | Coronary artery disease (no further details documented) | Goitre (euthyroid) | Total thyroidectomy followed by CABG | All five operations were successful. Transient recurrent laryngeal nerve palsy in one case. Nil complications over 2- to 14-month follow-up |
| 65-year-old male: asymptomatic | Coronary artery disease (no further details documented) | Retrosternal goitre (euthyroid) | Total thyroidectomy followed by CABG | ||
| 69-year-old male: thyrotoxicosis | Coronary artery disease (no further details documented) | Retrosternal goitre (hyperthyroid) | Total thyroidectomy followed by CABG | ||
| 70-year-old female: dysphagia | Coronary artery disease (no further details documented) | Toxic retrosternal goitre (hyperthyroid) | Total thyroidectomy followed by CABG | ||
| 59-year-old male: asymptomatic | Coronary artery disease (no further details documented) | Goitre (euthyroid) | Total thyroidectomy followed by CABG | ||
| Wexler et al., 2011, USA (14) | 76-year-old female: myocardial infarction, dyspnoea | Severe proximal stenosis of LAD, bifurcating lesion of diagonal artery | Retrosternal multinodular goitre causing tracheal compression (euthyroid) | Total thyroidectomy followed by CABG ×2 | Nil intra- or post-operative complications. Patient discharged on day 9. No cardiac or thyroid complications present at 6-week follow-up |
CABG, coronary artery bypass grafting; Cx, circmflex artery; LAD, left anterior descending artery; LMS, left main stem; OPCABG, off-pump coronary artery bypass grafting; RCA, right coronary artery.
This paper has presented a case involving the single-procedure treatment of two significant diseases of differing pathology, namely severe myocardial ischaemia and retrosternal goitre causing displacement and compression of adjacent structures. Both for our patient and in a wider context, the combined approach exhibits various advantages. Firstly, the anatomical proximity of the thyroid facilitates its excision in conjunction with CABG, making this a feasible surgical option (5). Furthermore, the cumulative risk of a combined operation seems to be less than the individual risks associated with each separate procedure and also avoids the need for resternotomy (15). A stand-alone thyroidectomy preceding CABG subjects a patient with coexisting coronary artery disease to significant risk associated with the use of general anesthesia. Conversely, an independently performed CABG prior to thyroidectomy cannot address goitre-related respiratory dysfunction and may result in a problematic and prolonged ventilator-weaning period. Moreover, CABG as an initial stand-alone procedure in cases of hyperthyroidism could lead to undesirable arrhythmias complicating the postoperative recovery period (5). In our case, an off-pump approach was preferable due to the patient’s increased age and impairment of left ventricular function. A significant advantage of OPCABG is the use of lower heparin doses relative to on-pump procedures, which reduces the risk of bleeding, especially from the highly vascularised thyroid (16).
In conclusion, it is our view that a simultaneous, dual discipline approach combining OPCABG and thyroidectomy for a retrosternal goitre can be safely and effectively performed to achieve good clinical outcomes, provided that perioperative levels of thyroid hormones are maintained at euthyroid or hypothyroid levels.
Acknowledgements
None.
Informed Consent: Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Footnotes
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- 1.Hedayati N, McHenry CR. The clinical presentation and operative management of nodular and diffuse substernal thyroid disease. Am Surg 2002;68:245-51; discussion 251-2. [PubMed] [Google Scholar]
- 2.Raffaelli M, De Crea C, Ronti S, et al. Substernal goiters: incidence, surgical approach, and complications in a tertiary care referral center. Head Neck 2011;33:1420-5. 10.1002/hed.21617 [DOI] [PubMed] [Google Scholar]
- 3.Ahmed ME, Ahmed EO, Mahadi SI. Retrosternal goiter: the need for median sternotomy. World J Surg 2006;30:1945-8; discussion 1949. [DOI] [PubMed]
- 4.Rugiu MG, Piemonte M. Surgical approach to retrosternal goitre: do we still need sternotomy? Acta Otorhinolaryngol Ital 2009;29:331-8. [PMC free article] [PubMed] [Google Scholar]
- 5.Abboud B, Sleilaty G, Asmar B, et al. Interventions in heart and thyroid surgery: can they be safely combined? Eur J Cardiothorac Surg 2003;24:712-5. 10.1016/S1010-7940(03)00411-1 [DOI] [PubMed] [Google Scholar]
- 6.De Silva RP, Dignan RJ. Does a combined procedure for cardiac surgery and thyroidectomy offer acceptable outcomes? Interact Cardiovasc Thorac Surg 2015;21:787-91. 10.1093/icvts/ivv241 [DOI] [PubMed] [Google Scholar]
- 7.Mehta Y, P S, Juneja R, et al. OPCAB and thyroidectomy in a patient with a severely compromised airway. J Cardiothorac Vasc Anesth 2005;19:79-82. 10.1053/j.jvca.2004.11.015 [DOI] [PubMed] [Google Scholar]
- 8.Mehra AP, Shah KS, Jain PC, et al. Combined off-pump coronary artery bypass grafting and thyroidectomy. Ann Thorac Surg 2009;88:661-3. 10.1016/j.athoracsur.2009.01.072 [DOI] [PubMed] [Google Scholar]
- 9.Cetin E, Ozyuksel A, Dalbasi E. Single stage substernal thyroidectomy and off-pump coronary artery bypass grafting: is it worth using cardiopulmonary bypass unless absolutely necessary? BMJ Case Rep 2014;2014. [DOI] [PMC free article] [PubMed]
- 10.Testini M, Poli E, Lardo D, et al. Combined cardiac surgery and total thyroidectomy: our experience and review of the literature. Thorac Cardiovasc Surg 2010;58:450-4. 10.1055/s-0030-1249867 [DOI] [PubMed] [Google Scholar]
- 11.Gürkan S, Hüseyin S, Saraç A, et al. Combined cardiac surgery and substernal thyroidectomy. Türk Göğüs Kalp Damar Cerrahisi Dergisi 2012;20:629-31. [Google Scholar]
- 12.Koçak H, Becit N, Erkut B, et al. Combined coronary arterial bypass graft and thyroidectomy in a patient with giant goiter: how reliable is it? Thorac Cardiovasc Surg 2007;55:56-8. 10.1055/s-2006-924105 [DOI] [PubMed] [Google Scholar]
- 13.Litmathe J, Kurt M, Boeken U, et al. Combined cardiothoracic surgery and interventions of the para/thyroid gland. A rare clinical cooperation. Z Kardiol 2005;94:28-32. 10.1007/s00392-005-0177-6 [DOI] [PubMed] [Google Scholar]
- 14.Wexler S, Yamane K, Fisher KW, et al. Single-stage operation for giant substernal goiter with severe coronary artery disease. Ann Thorac Cardiovasc Surg 2011;17:524-7. 10.5761/atcs.cr.10.01628 [DOI] [PubMed] [Google Scholar]
- 15.Wolfhard U, Krause U, Walz MK, et al. Combined interventions in heart and thyroid surgery--an example of interdisciplinary cooperation. Chirurg 1994;65:1107-10. [PubMed] [Google Scholar]
- 16.Englberger L, Streich M, Tevaearai H, et al. Different anticoagulation strategies in off-pump coronary artery bypass operations: a European survey. Interact Cardiovasc Thorac Surg 2008;7:378-82. 10.1510/icvts.2007.169086 [DOI] [PubMed] [Google Scholar]