

Abstract
Impressions of health are integral to social interactions, yet poorly understood. A review of the literature reveals multiple facial characteristics that potentially act as cues to health judgements. The cues vary in their stability across time: structural shape cues including symmetry and sexual dimorphism alter slowly across the lifespan and have been found to have weak links to actual health, but show inconsistent effects on perceived health. Facial adiposity changes over a medium time course and is associated with both perceived and actual health. Skin colour alters over a short time and has strong effects on perceived health, yet links to health outcomes have barely been evaluated. Reviewing suggested an additional influence of demeanour as a perceptual cue to health. We, therefore, investigated the association of health judgements with multiple facial cues measured objectively from two-dimensional and three-dimensional facial images. We found evidence for independent contributions of face shape and skin colour cues to perceived health. Our empirical findings: (i) reinforce the role of skin yellowness; (ii) demonstrate the utility of global face shape measures of adiposity; and (iii) emphasize the role of affect in facial images with nominally neutral expression in impressions of health.
Keywords: perceived health, cues, faces, adiposity, expression, skin colour
1. Introduction
Judgements of a person's health based on their facial appearance is a daily occurrence. Understanding how these judgements are informed is important because they feed into other social judgements such as attractiveness [1–3] or leadership ability [4], which is potentially consequential in terms of real-life outcomes, such as dating and or employment outcomes. Other social consequences may stem directly from judgements of health because maintaining a physical distance from those who are perceived to be unhealthy has clear evolutionary benefits through avoidance of contagious disease. Indeed, when cued with disease-relevant images, people tend to rate themselves as less extraverted and are quicker to make avoidance movements in response to faces [5]. Negative judgements of perceived health may, therefore, lead to a risk of social isolation and stigmatization [6,7]. This outcome is particularly disquieting in modern Western societies where disease is largely non-communicable, and social contact is known to provide health benefits [8]. A clearer understanding of how health attributions are informed and to what extent they are valid may reduce the negative social consequences which can follow.
To this end, a literature search was conducted in OVID, Web of Science and EBSCO (including PsychINFO) using the following search terms: ‘face’ (title) OR ‘facial’ (title) AND ‘health’ (title) OR ‘perceiv* health’ (keyword) AND ‘cue’ (keyword). The search returned 86 unique abstracts, 32 of which were retained after screening for relevance (i.e. papers reporting empirical results and testing for an association between at least one facial cue and either perceived health or actual health outcomes. The search was by no means exhaustive and additional papers were included from reference lists of identified papers. It should be noted that, although perceived attractiveness is often thought to be a proxy for apparent health, some studies have failed to find a relationship between attractiveness and health [9,10]. Therefore, for brevity and clarity, within this review perceptual studies were limited to those specifically investigating perceived health and not attractiveness. Results of the literature search have been grouped into the headings below, under which evidence of both cue use and cue validity is summarized. Cue use refers to information in a face (e.g. colour, shape, expression) which influences our perceptions or judgements of how healthy a person looks. Conversely, cue validity refers to whether the facial information is reliably related to the health of a person. For accurate assessment of health from faces, cues would have to be both valid and used.
(a). Men's facial masculinity
Male facial masculinity is thought to be a cue to good health and ‘good genes’ (i.e. genes promoting health). Based on the findings from the animal literature, the Immunocompetence Handicap Hypothesis (ICHH, [11]) proposes that male masculinity (including facial masculinity) acts as a handicap display that reliably conveys heritable aspects of good health to potential partners. Masculine facial features develop during puberty under the influence of androgenic steroid sex hormones (e.g. testosterone). As producing and metabolizing testosterone is costly (and might lead to higher oxidative stress [12]), the ICHH suggests that individuals with better innate immunity and health can afford to develop more pronounced (i.e. costly) masculine facial features than individuals of poorer health.
In line with this theoretical framework, several studies have found a relationship between male masculinity and perceived health: more masculine male faces are rated as looking healthier [1,13–15] although this is not a universal finding [16]. Studies investigating whether facial masculinity is indeed related to superior actual health are inconclusive [17]. For example, while both Thornhill & Gangestad [9] and Boothroyd et al. [1] found that facial masculinity was negatively related to male participants' reported number of prior colds and flu, mixed results were found regarding the relationship of male facial masculinity to length of infections and antibiotic use, and no association with ‘stomach flu’ was found. Rated facial masculinity has been associated with general health measured as a composite score from adolescent medical records [10] and to one aspect of immune function [18]. Rantala et al. [18] found that men with more masculine-looking faces were able to mount a stronger antibody response to a hepatitis B vaccination. Facial masculinity did not, however, mediate the relationship between immune response and facial attractiveness, suggesting that perceived masculinity was not being used as a cue to assess mate value.
(b). Facial symmetry
Facial symmetry is posited to be a cue to health during childhood and development because sources of environmental and genetic stress (e.g. pathogens or mutation rate) would test an individual's ability to maintain developmental stability, and resist asymmetric growth. Only two studies were identified which tested the effect of symmetry on judgements of health and both found a positive relationship [19,20].
Some support for the position that facial symmetry acts as an index to prior health has also been reported. Thornhill & Gangestad [9] found a positive relationship between facial asymmetry and number of bouts of colds and flu over the previous 3 years [9]. Facial asymmetry was found to be marginally related to total number of days ill with cold and flu infections, and also with antibiotic use, but was unrelated to stomach bugs. Also, Zebrowitz & Rhodes [14] found that facial symmetry was related to physicians' assessments of health, but this was true only among those who scored lower than average with regard to symmetry [14].
Contrary to the hypothesis that symmetry cues health, the largest study of facial asymmetry and health to date found no relationship between these variables [21]. Researchers used data from a British cohort study of 4732 individuals and found that facial symmetry at age 15 was unrelated to longitudinal measures of childhood health, including measures of the proportion of childhood years spent unwell, average number of illness symptoms per year, and total number of infections.
(c). Facial adiposity
Obesity is known to be related to a number of health risks, and is often indexed by weight, body mass index (BMI, weight scaled for height) or percentage body fat. Recent findings suggest that perceived weight as judged from the face alone, also referred to as facial adiposity, may also provide an important cue to health.
Perceptual studies have demonstrated that facial adiposity in adult faces is related negatively to judgements of health [2,22,23], but positively to health judgements in infant faces [24]. There is also growing evidence that perceived adiposity from facial images is related to actual health outcomes. For example, individuals that were judged to be heavier-looking reported more frequent and longer lasting colds and had higher blood pressure [22]. Similarly, perceived weight has been found to relate to a composite measure of general condition including items related to physical and psychological health [25]. Indeed, ratings of weight from faces not only predicted weight 36 years later but also predicted adulthood risk of obesity, illness symptoms (muscle aches, shortness of breath and chest pain), chronic conditions (arthritis, high blood pressure and diabetes) and all-cause mortality [26].
In men, perceived facial adiposity has also been linked to the antibody response to a hepatitis C vaccination [18]. This relationship is in accord with findings that hepatitis vaccine reaction is stronger in individuals with lower weight and BMI [27]. In addition, facial adiposity was found to mediate the relationship between strength of hepatitis C antibody response and perceived attractiveness, suggesting that facial fatness is a valid and utilized cue to health [18].
Recently, a surprising finding has emerged: facial cues to body fat may be a better predictor of health outcomes than traditional indices of obesity such as BMI, percentage body fat or girth of waist. Neck adiposity (measured using a lipometer), for example, has been shown to be a better discriminatory factor in identifying type 2 diabetes than BMI, percentage fat and measurements of subcutaneous fat using the lipometer at 14 other body locations [28]. Similarly, neck circumference has been shown to be a significant predictor of hypertension, independent of BMI and waist circumference [29].
Fat distribution may be more informative than fat mass per se when it comes to health outcomes. If facial fatness provides key information to body fat distribution, this could explain the stronger relationship between perceived fatness from facial images relative to more common indices of body size such as BMI or percentage fat. Indeed, cheek fat is related to visceral abdominal fat [30], which is thought to be a particularly risky place to carry excess weight.
Three quantifiable aspects of face shape have also been identified as influencing judgements of weight and may provide targets for testing their relationship to health outcomes (width-to-height-ratio, perimeter-to-area ratio and cheek-to-jaw-width ratio) [31]. These three measures do not necessarily capture all aspects of face shape that relate to weight perceived from faces. It is also possible to use an empirical approach to derive more global measures of facial shape that characterize facial adiposity using principal component analysis (PCA) of landmarks capturing the structure of two-dimensional (2D) facial images [32] or the entire surface of three-dimensional (3D) faces [33]. It remains to be shown how such measures relate to perceived health and measured health.
(d). Skin condition (texture and colour)
Skin colour and texture are facial cues which are malleable and may change in response to illness in a short space of time. For this reason, it has been argued that such cues should provide more relevant information to current health than shape information such as facial masculinity or symmetry [34].
Studies showing correlations between perceived health in whole faces and isolated patches of skin from those same faces attest to the relevance of skin information in perceptual judgements of health [35,36]. Skin information can be further divided into more specific cues including surface topography (lumps, bumps and wrinkles), colour and colour distribution, each of which have been shown to influence judgements of health (although colour distribution may be more influential than surface topography [37]).
When the colour of faces is manipulated along three axes consistent with human colour perception, i.e. yellowness, redness or lightness, an increase in all three leads to more positive judgements of health [38]. The distribution of colour in the face is also important in judgements of health, with homogeneous colour distribution increasing judgements of health compared with patchy colour distribution [39–41]. Contrast in luminance and colour between the facial skin and features such as eyes and lips also contributes to health judgements [38,42].
In terms of cue validity, it has been demonstrated that judgements of health are more accurate when faces are presented containing relevant skin information alone (and face shape is held constant) compared with when face shape information alone are presented (and skin colour is held constant) [43]. This is consistent with the argument above that skin colour cues (including texture, colour and colour distribution) may provide more health information than face shape (although it should be noted that in [44], colour included shading cues to 3D face shape).
More detailed investigations of specific skin cues and their association with health outcomes are limited within the face perception literature. Several studies have suggested a causal relationship between diets rich in fruits and vegetables [44–48] and skin colour (specifically yellowness), yet there is limited evidence suggesting that this aspect of human skin coloration is related to health beyond diet. There were also no studies identified which tested relationships between measures of health and skin texture or colour distribution as measured from facial images. This is an area of research requiring future attention.
(e). Expression
There is clear lack of experimental studies investigating the role of expression or emotion upon perceived health. One study investigated smiles in photos and their link to health outcomes [49]. Researchers found from photographs of major league baseball players in the United States that those individuals who displayed a full Duchenne smile (with orbicularis muscle activity causing wrinkles around the eyes in addition to zygomatic activity raising mouth corners) were half as likely to die in any given subsequent year, relative to non-smiling individuals. The authors reasoned that individuals who are smiling in a photograph are likely to smile more often in general and that mood is related to physiology and general health. That mood and health are associated is widely accepted [50], and so the prospect that facial cues to mood will influence judgements of health follows logically.
The lack of more empirical studies in this area likely stems from the use of standardized passport style photographs in face perception studies. There is some work that has shown that even among standardized photos, in which participants are asked to hold a neutral expression, raters were able to judge images of sleep deprived individuals as more fatigued and sadder than images of the same participants after a normal sleep [51]. Sleep deprived images were also said to have ‘droopier mouths’ and ‘hanging eyelids’. Although this study did not investigate perceived health, it does highlight the possibility that variation in expression exists among standardized photos, and that raters are able to use this information to inform judgements. Indeed, the apparent mood of ‘neutral’ facial poses varies considerably and is the driving force behind many social attributions (e.g. trustworthiness) made to facial images [52]. Further work to explore the use of such cues and their validity in health judgements is necessary.
(f). Summary and future directions
Malleable face cues including facial adiposity, skin colour and texture may offer more current and relevant information with regard to health than relatively stable aspects of facial appearance such as masculinity and symmetry. Indeed, there is some evidence that skin information allows more accurate perceptions of health relative to shape information [43]. Links between actual health and specific skin condition cues (colour and texture) as measured from facial images is currently lacking, although a wealth of evidence attests to the fact that these cues are used in health judgements. Expression or mood-related information was also identified as a potentially important cue to health. To date, studies of facial cues and health outcomes have focused on stable structural aspects of the face such as averageness, symmetry and sexual dimorphism. Future research should therefore test the validity of health judgements made in response to malleable facial cues such as colour and resting demeanour.
The adiposity literature revealed the tantalizing possibility that facial cues to fatness may predict health outcomes more accurately than traditional measures of body fat or weight, although to date the only evidence supporting this notion comes from studies of neck diameter and neck adiposity measured by lipometer. Given that other facial cues are informing judgements and measures of facial fatness (e.g. chubby cheeks and jaw shape), an important step forward will be to test how measured or rated adiposity from whole faces compares with traditional measures of body weight and size in predicting health outcomes.
Of course, none of these facial cues exist in isolation and, while some studies have begun to investigate how cues are integrated to inform judgements of health [20,23,37,39], and the relative validity of cues [14,43], these are two areas of health perception which are still largely unexplored. The expectation may be that multiple cues of health are congruent (as has been argued for cues to mate quality [53–56]).
(g). The present study
Here we report results from two empirical studies that we feel are particularly timely in the quest to understand how we use facial cues to assess health. In both studies, we test the relative importance of malleable cues in judgements of perceived health. In 3D and 2D images, we have objectively measured variation in the upward or downward turn of the mouth as well as the extent to which eyes are opened (hereafter referred to as ‘mouth curvature’ and ‘eye openness’). These particular facial features were selected for investigation because they are related to perceptions of sadness and fatigue [51] and may therefore also influence judgements of health. In Study 1, the contribution of mouth curvature, eye openness and measured facial adiposity are tested in health judgements of 3D faces. Study 2 tests the relative contribution of these cues together with colour information in health attributions made to 2D facial images.
2. Material and methods
(a). Study 1: three-dimensional images
(i). Stimuli
Facial scans were taken using a 3D camera (http://www.3dMD.com). Participants were 68 Caucasian women (M ± s.d. = 20.9 ± 2.4 years, range 18–32) and 50 Caucasian men (M ± s.d. = 21.2 ± 2.5 years, range 18–32) who were photographed with a neutral facial expression, their hair pulled back and at a set distance and relative height to the camera [57]. Faces were delineated in MorphAnalyser 2.4.0 [58] with 49 landmarks. The landmark templates for all digitized head models were aligned in orientation, rotation and scale using Procrustes superimposition, and surface models were resampled in accordance with a standard head delineated with the same set of landmarks. This process establishes homology of each head model's tessellations across the entire sampled population. Thus, further analyses and averaging were conducted on the surfaces of the head models as a whole rather than on the template landmarks [33]. Height and weight were measured for all participants and used to calculate BMI. Basic demographic information (age, gender and ethnicity) was also recorded.
(ii). Objective measurements of facial stimuli
Facial BMI scores. All head models were subjected to a PCA. Each head model could then be described with a relatively small number of principal components (PCs). Next two groups were defined, one of 10 individuals low in BMI and one of 10 individuals high in BMI [57]. Owing to the sexual dimorphism in body composition and build, BMI scores were separately calculated for men and women. For men, the average BMI was 19.5 for the low group and 26.9 for the high group; for women, the average BMI was 17.9 for the low group and 28.7 for the high group (figure 1). For each of the 118 PCs, the average score of the low subsample was calculated (separately for male and female faces), defining a position in the 118-dimensional space. The average PC scores of the high subsample were similarly calculated. A ‘BMI axis’ in face space was then defined by the low and high BMI average face shapes. Each face in the sample was projected onto this axis, and the projection value defined the facial BMI score [57]. Average values for each PC were separately calculated for men and women with low and high BMI. Faces in the low and high groups were matched so that low and high BMI groups did not differ in height (t118 ≤ 0.78, all p ≥ 0.454). Facial BMI scores correlated with actual BMI (r118 = 0.59, p < 0.001), but not height (r117 = 0.05, p = 0.565) [57].1
Figure 1.

Female and male 3D face shapes associated with low (left of each pair) and high (right of each pair) BMI. For women, the face shapes correspond to BMIs of 18 and 31, respectively; for men, the face shapes correspond to BMIs of 17 and 29.
Eyelid openness. The degree of eyelid openness was examined by taking the vertical distance from the centre of the pupil to the top eyelid and dividing it by the width of the eye inner canthus to outer canthus. This measure was computed for left and right eyes separately and the two values averaged.
Mouth curvature. Measurements of mouth curvature were calculated by taking the average height of the right and left corners of the mouth (relative to the base of the image) and subtracting the height of the centre of the mouth (between the lips and directly under the philtrum). This value was then divided by the width of the mouth to standardize the measurement (see [59] for further details and validation of this measurement).
(iii). Perceptual ratings
To eliminate the influence of hairstyle, clothing and cues from the neck circumference on perceptual ratings, all 3D heads were masked to show faces only. Average male and female face texture images were created using PsychoMorph 4 [60]. All faces were rendered with this sex-specific standardized texture, so that only face shape differed between each of the 3D face models [33].
Participants residing in the USA and of mixed ethnicity were recruited via Amazon Mechanical Turk (46 women, M ± s.d. = 37.80 ± 10.71 years, and 70 men, M ± s.d. = 33.36 ± 9.09 years). Prior to the rating, participants were presented with static 2D frontal images of all face models to provide an overview of stimulus variability. The 3D face stimuli were then presented in randomized order, ‘bobbing’ in a sinusoidal manner from left to right and up and down. For each face, participants were asked ‘Compared to other men/women his/her age, how healthy is this person?’ Ratings were given on a 0–100 visual analogue scale. Stimuli were presented individually against a black background and remained visible until a rating was made. Female and male faces were presented in two separate blocks; the order of blocks was randomized. Ratings were averaged across participants for each face.
(b). Study 2: two-dimensional images
(i). Stimuli
Facial photographs of 67 Caucasian women (M ± s.d. = 20.85 ± 2.15 years, range 18–29) were taken using a camera in D65 lighting in a photographic booth painted with spectrally neutral grey and colour reference card (Gregtag Macbeth Mini ColorChecker Pantone). Clothing was covered with a grey-coloured board to prevent coloured reflection from clothing affecting facial illumination. Participants were photographed with a neutral facial expression, their hair pulled back and at a set distance and relative height to the camera. Faces were delineated in PsychoMorph with 187 landmarks. Face images were aligned on left and right pupils and were cropped to maximize the size of the face within the image frame.
(ii). Objective measurements of facial stimuli
Skin colour. Square image patches were cut from the left and right cheek areas and from the forehead. Average CIE L*, a*, b* colour in each cut patch was computed and the average colour was calculated by averaging across all three patches.
Eyes and mouth. Measurements of eyelid openness and mouth curvature were calculated in the same manner as described for Study 1.
Facial BMI scores. As detailed for the 3D faces, a data-driven approach was used to measure facial adiposity. A PCA of face shape determined by 117 delineation points (including the nose, mouth, eyes, and eyebrows, forehead, chin and neck) was used to define a BMI axis for female faces and to subsequently score individual faces along this axis.
(iii). Perceptual ratings
Participants were recruited and paid via Amazon Mechanical Turk to provide ratings of perceived health (11 females and 21 males, M ± s.d. = 40.16 ± 12.44 years). Analysis was restricted to participants who reported the same ethnicity as the images presented, i.e. ‘white Caucasian’, as sensitivity to skin colour cues may be weaker when raters are asked to make judgements from faces of other ethnicity [61].
Evaluators first previewed all stimuli with each image displayed for 1 s. The stimuli were then re-presented in random order so that participants could rate each face for perceived health. A minimum viewing time of one second per image was set, but no maximum response time was enforced. Facial ratings were made on a 7-point scale with endpoints ‘not at all healthy’ to ‘very healthy’. Cronbach's alpha for health ratings was high (n = 32, α = 0.94).
(iv). Composite facial images
To illustrate the difference in appearance between faces rated high and low for perceived health, composite images were created. Each composite consisted of faces which on average received the 10 lowest or highest ratings of perceived health. Mean ratings were 3.5 and 5.7, respectively. In PsychoMorph, 184 facial landmarks were placed on each image before composites displaying the average shape, colour and texture were created [60].
3. Results
(a). Study 1: three-dimensional images
Figure 2 displays the relationship between facial BMI scores and perceived health. Curve fitting revealed a significant quadratic relationship (R2 = 0.25, F1,115 = 19.45, p < 0.001) but a non-significant linear relationship (R2 = 0.01, F1,116 = 0.95, p = 0.331). Mouth curvature was found to relate to perceived health (r118 = −0.20, p = 0.030) in that more downturned mouths were associated with lower ratings of perceived health. Eye openness was unrelated to perceived health (r118 = −0.02, p = 0.865).
Figure 2.
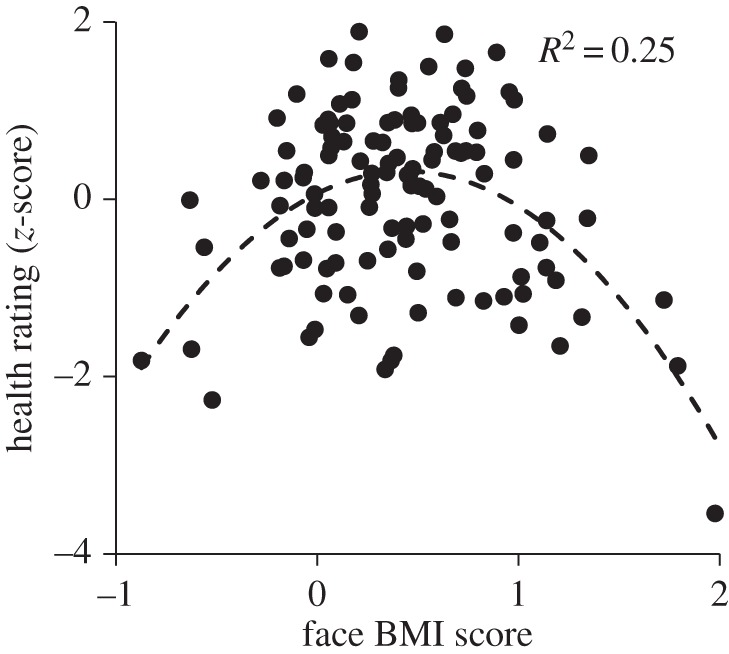
Relation of facial shape and perception of health for a set of 3D head models. The dashed line gives the best fit quadratic function relating perceived health to the face BMI score (variance explained R2 = 0.25). The quadratic relationship shows that face shapes associated with high and low BMI were perceived as less healthy than other faces.
When both mouth curvature and facial BMI score (squared) were included in the same model, only the curvilinear relationship between facial BMI score and perceived health remained significant (b = −0.35, t = −4.02, p < 0.001) while the predictive value of mouth curvature fell to a trend (b = −0.15, t = −1.71, p = 0.090). Downward mouth curvature showed a trend to relate to higher facial BMI score (r118 = 0.17, p = 0.072).2
Actual BMI was also found to predict perceived health through linear and squared terms, although the relationship was mediated by face BMI scores.3
(b). Study 2: two-dimensional images
(i). Composite images
Images displaying the average facial characteristics of the 10 faces rated highest and lowest in perceived health can be viewed in figure 3.
Figure 3.

Composite images illustrating the difference in facial characteristics of those rated low (left image, mean rating 3.5) and high (mean rating 5.7) in perceived health.
(ii). Skin colour
Perceived health correlated with skin yellowness (b*: r81 = 0.33, p = 0.003) but not skin redness (a*: r81 = 0.11, p = 0.344) or lightness (L*: r81 = −0.19, p = 0.096). The correlation between perceived health and skin yellowness persisted after controlling for skin lightness (r = 0.28, d.f. = 78, p = 0.013).
(iii). Face shape
Perceived health correlated with facial BMI score (r79 = −0.25, p = 0.023). As expected from the analysis of 3D face images, perceived health showed a stronger correlation with the square of the facial BMI score (r79 = −0.35, p = 0.002). Facial BMI scores were correlated with actual BMI (r79 = 0.55, p < 0.001) but did not mediate a relationship between actual BMI and perceived health.4 Perceived health correlated with upward mouth curvature (r81 = 0.51, p < 0.001) but not eyelid openness (r81 = 0.01, p = 0.953).
Entering skin yellowness, mouth curvature and facial adiposity into multiple regression with perceived health as the dependent variable revealed independent contributions to perceived health from skin yellowness (b = 0.22, t = 2.11, p = 0.038), and from upward mouth curvature (b = 0.39, t = 3.36, p = 0.001); (R2 = 0.28, overall model: F3,75 = 9.71, p < 0.001). This regression analysis failed to reveal an independent contribution of facial adiposity (b = −0.06, t = −0.46, p = 0.648), possibly because in this sample facial adiposity correlated with downward mouth curvature (r79 = 0.53, p < 0.001).
4. Discussion
The composite 2D images (figure 3) demonstrate multiple facial features associated with judgements of health. These include differences in skin colour, mouth curvature and shape related to weight. Analysis of objective image measurements confirmed that each of these cues was associated with impression of health. Mouth curvature was found to correlate with apparent health in both 2D and 3D images of faces; those with more downward turned mouths were rated as looking less healthy. We suggest that this relationship is driven by apparent sadness [51]. In line with this suggestion, the less healthy composite appears glum relative to the healthy composite. The extent to which one's eyes are open has previously been found to provide a cue to fatigue [51], but here we found no relation of eye openness to health judgements in either 2D or 3D facial images. The composite images do not appear to differ in fatigue.
A holistic measure of facial shape associated with adiposity was found to have a negative quadratic relationship to health judgements for both 2D and 3D face sets. That is, faces were judged to be less healthy as adiposity scores increased, but those with average adiposity scores were judged most healthy. For the 2D image set, skin yellowness but no other dimensions of skin colour (luminance and redness) was found to be positively associated with health judgements. Skin yellowness and face shape made independent contributions to judgements.
The quadratic relation between perceived health and measured facial adiposity in 2D and 3D found here was noted by Coetzee et al. [22] when facial adiposity was estimated as perceived weight. The curvilinear relationship may be due to two aspects of health understood by evaluators. One component of understanding may reflect awareness that body weight increasing above average (or the medically recommended BMI of 25) is associated with negative health consequences including risk of cardiovascular disease and diabetes. A second component may reflect awareness that severe chronic and acute illnesses are associated with weight loss. Indeed, unintended weight loss can be a symptom of a variety of diseases including type 1 diabetes, cancer and bacterial, viral or parasitic infection [62]. Health attributions triggered by low weight may reflect assumptions about a person's past or present condition. By contrast, attributions made to high weight could reflect the likelihood of current and future health problems (i.e. high weight may predispose to cancer and heart disease in later life).
Facial BMI scores were associated with perceived health in both 3D and 2D face image sets with the relationship being stronger in the 3D face set. In 3D images, the dominance of facial adiposity in influencing judgements of health could be because additional shape information allowed more accurate judgements (the correlation between shape score and BMI was largest in 3D) or because the moving 3D images and lack of colour fostered an expectancy effect whereby raters assumed that they should use shape cues to inform health judgements.
Mouth curvature was found to be a more powerful predictor compared with facial BMI score in health judgements of 2D faces. Faces with more downturned mouths, which presumably looked sadder, were rated as less healthy. For the 3D faces, mouth curvature was again correlated with apparent health, yet for this set of faces it did not improve the model relative to facial BMI scores alone. Mouth curvature may have been a more salient cue in front-facing 2D images relative to rotating 3D faces. Alternatively, mouth curvature may vary across samples and across time for the same individual; hence the importance of mouth curvature for health judgements could be capricious and reflect sampling [63].
For the 2D face set, facial BMI scores correlated with downturned mouth curvature, while for the 3D face set the same relationship showed a trend (p = 0.070). The association between mouth curvature and facial BMI scores we detected could arise because heavy jowls alter the real or apparent mouth shape. Alternatively, the link may arise because people with a heavier weight feel less comfortable in front of the camera. As facial BMI scores showed a curvilinear relationship to perceived health while mouth curvature showed a linear relationship, mouth curvature may have proportionally more importance for the faces of low weight individuals. By analogy, Fisher et al. [23] showed that skin colour was less important for health judgements for high weight faces [23]. Hence while BMI and mouth curvature are somewhat related in the face sets we studied, they are logically separable and should be investigated for independent contributions in future studies.
Finally, in 2D images, colour was found to be a significant predictor of health judgements, independent of facial adiposity and mouth curvature. Although the effect of colour was weaker than that of mouth curvature, faces with more yellow coloration were judged as looking healthier. This is consistent with prior work demonstrating a reliable preference for yellowness in faces [38,45,47,61], but additionally illustrates that yellowness acts independently of adiposity and mouth curvature as a cue to health in unaltered facial images.
Our findings in 2D faces highlight the influence of colour and mouth curvatures (which is likely to be perceived as subtle expression) in judgements of health in a sample of young Caucasian adults. Our samples are relatively leaner and presumably healthier than the population at large. A minority of our sample would be considered overweight, with reference to their BMI and WHO guidelines (19% of our 3D, and 16% of our 2D samples) while the majority (64.6%) of the Scottish population from which they were drawn are reported to be overweight. In a more representative population sample, face shape (indices of weight and expression) and skin colour cues may have a different relative importance. A further limitation of the current work is that our 2D sample of images is limited to female faces. There were no sex-specific effects of the relationship between mouth curvature and facial adiposity to perceived health in the 3D sample; we, therefore, have no reason to believe that there should be in 2D faces either. We also do not anticipate any sex-specific effects of the relationship between colour and perceived health because the preference for carotenoid coloration of skin is not specific to the sex of the face or the rater [45]. There are no obvious theoretical grounds to suggest that the relative importance of colour and shape cues would differ by sex of the face or rater; nevertheless, it is a question that could be addressed by future research.
While it will be important to extrapolate these findings by testing the relative contribution of cues in older, heavier or more varied populations, the current findings highlight two important implications for the study of perceptual judgements. The first is that cues may be used in a different manner depending upon the mode of stimulus presentation (e.g. 2D versus 3D), and this exposes the question of how cue utilization differs in judgements from static images compared with video and in real life with natural facial movements. The second implication is that, even in standardized images with apparently neutral expressions, there will be subtle variation in apparent expression. Here we have demonstrated that not only is this subtle variation measureable but it is also influencing social judgements. Given that variation in apparent affect is prevalent in collections of neutrally posed faces [52], it is advisable that expression-related features are measured and considered in perceptual studies.
Finally, a wider implication exists for anyone who uses a 2D image to represent themselves in any context whereby social assessments and interactions may follow. Health judgements have been shown to influence judgements of both attractiveness and leadership ability [3,4]; so if you have a picture on an online dating site or a professional network profile you may wish to update it in light of our findings. An image with a healthy skin tone and a positive expression could improve your chances of love and success.
Acknowledgement
We thank Dengke Xiao for assistance with facial feature measurements and PCA analysis of face shape, and Anne Perrett for proof reading.
Endnotes
We explored the ability of the process of deriving BMI scores to generalize. This was done by projecting the facial surfaces of the 118 faces used here into a PCA description of an independent set of 3D faces [34]. BMI scores were derived based on high and low BMI averages in this independent set of faces. The resulting independently derived BMI scores and the within set BMI scores correlated (r118 = 0.43, p < 0.001). We note that independently generated face BMI scores were not significantly correlated with actual BMI (r118 = 0.12, p = 0.210), potentially due to low power and also likely because BMI and facial BMI scores capture different information.
Entering sex of face into this analysis revealed no significant effects of sex of face or interactions between sex of face and facial parameters (all p > 0.127).
In a two-step linear regression, actual BMI explained 10.7% of variance in perceived health through linear (b = 2.34, p = 0.004) and squared terms (b = −2.57, p = 0.002). The addition of face BMI scores at step two significantly improved the model (R2 change = 0.16, p < 0.001). Actual BMI (both linear and squared) fell non-significant (p = 0.357 and p = 0.278), while face BMI score showed significant linear and squared terms (b = 0.57, p < 0.001 and b = −0.74, p < 0.001, respectively). This indicates that facial shape mediates the relationship between BMI and perceived health.
In a two-step linear regression, actual BMI explained 13.5% of variance in perceived health through linear (b = 1.11, p = 0.115) and squared terms (b = −1.42, p = 0.044). The addition of face BMI scores at step two did not significantly improve the model (R2 change = 0.01, p = 0.645). All predictors were non-significant, all ps > 0.264. The failure to find evidence for face BMI score mediating the relationship between actual BMI and perceived health may reflect a problem with multicollinearity because actual BMI and face BMI scores were highly correlated (r = 0.553, p < 0.001).
Ethics
All data collections were approved by UTREC and the School of Psychology and Neuroscience Ethics Committee, University of St Andrews. All participants provided informed written consent for their images and data to be used.
Data accessibility
Datasets supporting this article can be accessed at http://hdl.handle.net/10023/7924.
Software used to measure and manipulate facial images is freely accessible online:
PsychoMorph (http://users.aber.ac.uk/bpt/jpsychomorph/)
MorphAnalyser (http://cherry.dcs.aber.ac.uk:8080/wiki/MorphAnalyser)
Authors' contributions
Conception and design: All authors. Image and data collection: I.H. and S.T.; statistical analysis: D.P.; drafting the article: A.H.; revising critically for important intellectual content: A.H., I.H. and D.P.; final approval of the version to be published: all authors.
Competing interests
We have no competing interests.
Funding
A.H. is supported by a BBSRC studentship. D.P. was supported by a British Academy Wolfson Research Professorship.
References
- 1.Boothroyd LG, Scott I, Gray AW, Coombes CI, Pound N. 2013. Male facial masculinity as a cue to health outcomes. Evol. Psychol. 11, 1044–1058. ( 10.1177/147470491301100508) [DOI] [PubMed] [Google Scholar]
- 2.Coetzee V, Re D, Perrett DI, Tiddeman BP, Xiao D. 2011. Judging the health and attractiveness of female faces: is the most attractive level of facial adiposity also considered the healthiest? Body Image 8, 190–193. ( 10.1016/j.bodyim.2010.12.003) [DOI] [PubMed] [Google Scholar]
- 3.Rhodes G, Yoshikawa S, Palermo R, Simmons LW, Peters M, Lee K, Halberstadt J, Crawford JR. 2007. Perceived health contributes to the attractiveness of facial symmetry, averageness, and sexual dimorphism. Perception 36, 1244–1252. ( 10.1068/p5712) [DOI] [PubMed] [Google Scholar]
- 4.Spisak BR, Blaker NM, Lefevre CE, Moore FR, Krebbers KFB. 2014. A face for all seasons: searching for context-specific leadership traits and discovering a general preference for perceived health. Front. Hum. Neurosci. 8, 792 ( 10.3389/fnhum.2014.00792) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mortensen CR, Becker DV, Ackerman JM, Neuberg SL, Kenrick DT. 2010. Infection breeds reticence: the effects of disease salience on self-perceptions of personality and behavioral avoidance tendencies. Psychol. Sci. 21, 440–447. ( 10.1177/0956797610361706) [DOI] [PubMed] [Google Scholar]
- 6.Park JH, Schaller M, Crandall CS. 2007. Pathogen-avoidance mechanisms and the stigmatization of obese people. Evol. Hum. Behav. 28, 410–414. ( 10.1016/j.evolhumbehav.2007.05.008) [DOI] [Google Scholar]
- 7.Duncan LA, Schaller M. 2009. Prejudicial attitudes toward older adults may be exaggerated when people feel vulnerable to infectious disease: evidence and implications. Anal. Soc. Issues Public Policy 9, 97–115. ( 10.1111/j.1530-2415.2009.01188.x) [DOI] [Google Scholar]
- 8.Uchino BN. 2006. Social support and health: a review of physiological processes potentially underlying links to disease outcomes. J. Behav. Med. 29, 377–387. ( 10.1007/s10865-006-9056-5) [DOI] [PubMed] [Google Scholar]
- 9.Thornhill R, Gangestad SW. 2006. Facial sexual dimorphism, developmental stability, and susceptibility to disease in men and women. Evol. Hum. Behav. 27, 131–144. ( 10.1016/j.evolhumbehav.2005.06.001) [DOI] [Google Scholar]
- 10.Rhodes G, Chan J, Zebrowitz LA, Simmons LW. 2003. Does sexual dimorphism in human faces signal health? Proc. R. Soc. Lond. B 270, S93–S95. ( 10.1098/rsbl.2003.0023) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Folstad I, Karter AJ. 1992. Parasites, bright males, and the immunocompetence handicap. Am. Nat. 139, 603–622. ( 10.1086/285346) [DOI] [Google Scholar]
- 12.Alonso-Alvarez C, Bertrand S, Faivre B, Chastel O, Sorci G. 2007. Testosterone and oxidative stress: the oxidation handicap hypothesis. Proc. R. Soc. B 274, 819–825. ( 10.1098/rspb.2006.3764) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Smith FG, Jones BC, Debruine LM, Little AC. 2009. Interactions between masculinity-femininity and apparent health in face preferences. Behav. Ecol. 20, 441–445. ( 10.1093/beheco/arn141) [DOI] [Google Scholar]
- 14.Zebrowitz LA, Rhodes G. 2004. Sensitivity to ‘bad genes’ and the anomalous face overgeneralization effect: cue validity, cue utilization, and accuracy in judging intelligence and health. J. Nonverbal Behav. 28, 167–185. ( 10.1023/B:JONB.0000039648.30935.1b) [DOI] [Google Scholar]
- 15.Scott IML, Swami V, Josephson SC, Penton-Voak IS. 2008. Context-dependent preferences for facial dimorphism in a rural Malaysian population. Evol. Hum. Behav. 29, 289–296. ( 10.1016/j.evolhumbehav.2008.02.004) [DOI] [Google Scholar]
- 16.Boothroyd LG, Jones BC, Burt DM, Cornwell RE, Little AC, Tiddeman BP, Perrett DI. 2005. Facial masculinity is related to perceived age but not perceived health. Evol. Hum. Behav. 26, 417–431. ( 10.1016/j.evolhumbehav.2005.01.001) [DOI] [Google Scholar]
- 17.Roberts ML, Buchanan KL, Evans MR. 2004. Testing the immunocompetence handicap hypothesis: a review of the evidence. Anim. Behav. 68, 227–239. ( 10.1016/j.anbehav.2004.05.001) [DOI] [Google Scholar]
- 18.Rantala MJ, Coetzee V, Moore FR, Skrinda I, Kecko S, Krama T, Kivleniece I, Krams I. 2013. Adiposity, compared with masculinity, serves as a more valid cue to immunocompetence in human mate choice. Proc. R. Soc. B 280, 20122495 ( 10.1098/rspb.2012.2495) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Fink B, Neave N, Manning JT, Grammer K. 2006. Facial symmetry and judgements of attractiveness, health and personality. Pers. Individ. Differ. 41, 491–499. ( 10.1016/j.paid.2006.01.017) [DOI] [Google Scholar]
- 20.Jones BC, Little AC, Feinberg DR, Penton-Voak IS, Tiddeman BP, Perrett DI. 2004. The relationship between shape symmetry and perceived skin condition in male facial attractiveness. Evol. Hum. Behav. 25, 24–30. ( 10.1016/S1090-5138(03)00080-1) [DOI] [Google Scholar]
- 21.Pound N, Lawson DW, Toma AM, Richmond S, Zhurov AI, Ian S, Penton-Voak IS. 2014. Facial fluctuating asymmetry is not associated with childhood ill-health in a large British cohort study. Proc. R. Soc. B 281, 20141639 ( 10.1098/rspb.2014.1639) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Coetzee V, Perrett DI, Stephen ID. 2009. Facial adiposity: a cue to health? Perception 38, 1700–1711. ( 10.1068/p6423) [DOI] [PubMed] [Google Scholar]
- 23.Fisher CI, Hahn AC, Debruine LM, Jones BC. 2014. Integrating shape cues of adiposity and color information when judging facial health and attractiveness. Perception 43, 499–508. ( 10.1068/p7728) [DOI] [PubMed] [Google Scholar]
- 24.Volk AA, Lukjanczuk JM, Quinsey VL. 2005. Influence of infant and child facial cues of low body weight on adults’ ratings of adoption preference, cuteness, and health. Infant Ment. Health J. 26, 459–469. ( 10.1002/imhj.20064) [DOI] [PubMed] [Google Scholar]
- 25.Tinlin RM, Watkins CD, Welling LLM, Debruine LM, Al-Dujaili EAS, Jones BC. 2013. Perceived facial adiposity conveys information about women's health. Br. J. Psychol. 104, 235–248. ( 10.1111/j.2044-8295.2012.02117.x) [DOI] [PubMed] [Google Scholar]
- 26.Reither EN, Hauser RM, Swallen KC.. 2009. Predicting adult health and mortality from adolescent facial characteristics in yearbook photographs. Demography 46, 27–41. ( 10.1353/dem.0.0037) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Reuman PD, Kubilis P, Hurni W, Brown L, Nalin D. 1997. The effect of age and weight on the response to formalin inactivated, alum-adjuvanted hepatitis A vaccine in healthy adults. Vaccine 15, 1157–1161. ( 10.1016/S0264-410X(96)00310-6) [DOI] [PubMed] [Google Scholar]
- 28.Tafeit E, Möller R, Pieber TR, Sudi K, Reibnegger G. 2000. Differences of subcutaneous adipose tissue topography in type-2 diabetic (NIDDM) women and healthy controls. Am. J. Phys. Anthropol. 113, 381–388. ( 10.1002/1096-8644(200011)113:3<381::AID-AJPA8>3.0.CO;2-T) [DOI] [PubMed] [Google Scholar]
- 29.Laakso M, Matilainen V, Keinanen-Kiukaanniemi S. 2002. Association of neck circumference with insulin resistance-related factors. Int. J. Obes. 26, 873–875. ( 10.1038/sj.ijo.0802002) [DOI] [PubMed] [Google Scholar]
- 30.Levine J, Ray M, Jensen M. 1998. Relation between chubby cheeks and visceral fat. N. Engl. J. Med. 339, 1946–1947. ( 10.1056/NEJM199812243392614) [DOI] [PubMed] [Google Scholar]
- 31.Coetzee V, Chen J, Perrett DI, Stephen ID. 2010. Deciphering faces: quantifiable visual cues to weight. Perception 39, 51–61. ( 10.1068/p6560) [DOI] [PubMed] [Google Scholar]
- 32.Wolffhechel K, Hahn AC, Jarmer H, Fisher CI, Jones BC, DeBruine LM. 2015. Testing the utility of a data-driven approach for assessing BMI from face images. PLoS ONE 10, e0140347 ( 10.1371/journal.pone.0140347) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Holzleitner IJ, Hunter DW, Tiddeman BP, Seck A, Re DE, Perrett DI. 2014. Men's facial masculinity: when (body) size matters. Perception 43, 1191–1202. ( 10.1068/p7673) [DOI] [PubMed] [Google Scholar]
- 34.Scott IML, Pound N, Stephen ID, Clark AP, Penton-Voak IS. 2010. Does masculinity matter? The contribution of masculine face shape to male attractiveness in humans. PLoS ONE 5, e13585 ( 10.1371/journal.pone.0013585) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Fink B, Bunse L, Matts PJ, D'Emiliano D. 2012. Visible skin colouration predicts perception of male facial age, health and attractiveness. Int. J. Cosmet. Sci. 34, 307–310. ( 10.1111/j.1468-2494.2012.00724.x) [DOI] [PubMed] [Google Scholar]
- 36.Jones BC, Little AC, Burt DM, Perrett DI. 2004. When facial attractiveness is only skin deep. Perception 33, 569–577. ( 10.1068/p3463) [DOI] [PubMed] [Google Scholar]
- 37.Samson N, Fink B, Matts P. 2011. Interaction of skin color distribution and skin surface topography cues in the perception of female facial age and health. J. Cosmet. Dermatol. 10, 78–84. ( 10.1111/j.1473-2165.2010.00538.x) [DOI] [PubMed] [Google Scholar]
- 38.Stephen ID, Law Smith MJ, Stirrat MR, Perrett DI. 2009. Facial skin coloration affects perceived health of human faces. Int. J. Primatol. 30, 845–857. ( 10.1007/s10764-009-9380-z) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Fink B, Matts P. 2008. The effects of skin colour distribution and topography cues on the perception of female facial age and health. J. Eur. Acad. Dermatol. Venereol. 22, 493–498. ( 10.1111/j.1468-3083.2007.02512.x) [DOI] [PubMed] [Google Scholar]
- 40.Matts PJ, Fink B, Grammer K, Burquest M. 2007. Color homogeneity and visual perception of age, health, and attractiveness of female facial skin. J. Am. Acad. Dermatol. 57, 977–984. ( 10.1016/j.jaad.2007.07.040) [DOI] [PubMed] [Google Scholar]
- 41.Fink B, Matts PJ, D'Emiliano D, Bunse L, Weege B, Röder S. 2012. Colour homogeneity and visual perception of age, health and attractiveness of male facial skin. J. Eur. Acad. Dermatol. Venereol. 26, 1486–1492. ( 10.1111/j.1468-3083.2011.04316.x) [DOI] [PubMed] [Google Scholar]
- 42.Russell R, Sweda J, Porcheron A, Mauger E. 2014. Sclera color changes with age and is a cue for perceiveing age, health, and beauty. Psychol. Aging 29, 626–635. ( 10.1007/1-4020-0613-6_16551) [DOI] [PubMed] [Google Scholar]
- 43.Jones AL, Kramer RSS, Ward R. 2012. Signals of personality and health: the contributions of facial shape, skin texture, and viewing angle. J. Exp. Psychol. Hum. Percept. Perform. 38, 1353–1361. ( 10.1037/a0027078) [DOI] [PubMed] [Google Scholar]
- 44.Alaluf S, Heinrich U, Stahl W, Tronnier H, Wiseman S. 2002. Dietary carotenoids contribute to normal human skin color and UV photosensitivity. Hum. Nutr. Metab. 132, 399–403. [DOI] [PubMed] [Google Scholar]
- 45.Stephen ID, Coetzee V, Perrett DI. 2011. Carotenoid and melanin pigment coloration affect perceived human health. Evol. Hum. Behav. 32, 216–227. ( 10.1016/j.evolhumbehav.2010.09.003) [DOI] [Google Scholar]
- 46.Tan KW, Graf BA, Mitra SR, Stephen ID. 2015. Daily consumption of a fruit and vegetable smoothie alters facial skin color. PLoS ONE 10, e0133445 ( 10.1371/journal.pone.0133445) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Whitehead RD, Re D, Xiao D, Ozakinci G, Perrett DI. 2012. You are what you eat: within-subject increases in fruit and vegetable consumption confer beneficial skin-color changes. PLoS ONE 7, e32988 ( 10.1371/journal.pone.0032988) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Whitehead RD, Ozakinci G, Perrett DI. 2013. A randomized controlled trial of an appearance-based dietary intervention. Health Psychol. 33, 99–102. ( 10.1037/a0032322) [DOI] [PubMed] [Google Scholar]
- 49.Abel EL, Kruger ML. 2010. Smile intensity in photographs predicts longevity. Psychol. Sci. 21, 542–544. ( 10.1177/0956797610363775) [DOI] [PubMed] [Google Scholar]
- 50.Pressman SD, Cohen S. 2005. Does positive affect influence health? Psychol. Bull. 131, 925–971. ( 10.1037/0033-2909.131.6.925) [DOI] [PubMed] [Google Scholar]
- 51.Sundelin T, Lekander M, Kecklund G, Van Someren EJW, Olsson A, Axelsson J. 2013. Cues of fatigue: effects of sleep deprivation on facial appearance. Sleep 36, 1355–1360. ( 10.5665/sleep.2964) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Oosterhof NN, Todorov A. 2009. Shared perceptual basis of emotional expressions and trustworthiness impressions from faces. Emotion 9, 128–133. ( 10.1037/a0014520) [DOI] [PubMed] [Google Scholar]
- 53.Loyau A, Saint Jalme M, Cagniant C, Sorci G. 2005. Multiple sexual advertisements honestly reflect health status in peacocks (Pavo cristatus). Behav. Ecol. Sociobiol. 58, 552–557. ( 10.1007/s00265-005-0958-y) [DOI] [Google Scholar]
- 54.Feinberg DR, Jones BC, DeBruine LM, Moore FR, Law Smith MJ, Cornwell RE, Tiddeman BP, Boothroyd LG, Perrett DI. 2005. The voice and face of woman: one ornament that signals quality? Evol. Hum. Behav. 26, 398–408. ( 10.1016/j.evolhumbehav.2005.04.001) [DOI] [Google Scholar]
- 55.Thornhill R, Grammer K. 1999. The body and face of woman. Evol. Hum. Behav. 20, 105–120. ( 10.1016/S1090-5138(98)00044-0) [DOI] [Google Scholar]
- 56.Candolin U. 2003. The use of multiple cues in mate choice. Biol. Rev. Camb. Philos. Soc. 78, 575–595. ( 10.1017/S1464793103006158) [DOI] [PubMed] [Google Scholar]
- 57.Holzleitner IJ, Perrett DI. In press. Perception of strength from 3D faces is linked to facial cues of physique. Evol. Hum. Behav. ( 10.1016/j.evolhumbehav.2015.11.004) [DOI] [Google Scholar]
- 58.Tiddeman BP, Duffy N, Rabey G. 2000. Construction and visualisation of three-dimensional facial statistics. Comput. Methods Programs Biomed. 63, 9–20. ( 10.1016/S0169-2607(00)00072-9) [DOI] [PubMed] [Google Scholar]
- 59.Talamas SN, Mavor KI, Axelsson J, Sundelin T, Perrett DI. In press Eyelid-openness and mouth curvature influence perceived intelligence beyond attractiveness. J. Exp. Psychol. ( 10.1037/xge0000152) [DOI] [PubMed] [Google Scholar]
- 60.Tiddeman B, Burt M, Perrett DI. 2001. Prototyping and transforming facial textures for perception research. IEEE Comput. Graph. Appl. 21, 42–50. ( 10.1109/38.946630) [DOI] [Google Scholar]
- 61.Stephen ID, Scott IML, Coetzee V, Pound N, Perrett DI, Africa S. 2012. Cross-cultural effects of color, but not morphological masculinity, on perceived attractiveness of men’s faces. Evol. Hum. Behav. 33, 260–267. ( 10.1016/j.evolhumbehav.2011.10.003) [DOI] [Google Scholar]
- 62.NHS Choices. 2015. Unintentional weight loss. See http://www.nhs.uk/Conditions/unexpected-weight-loss/Pages/Introduction.aspx .
- 63.Todorov A, Porter JM. 2014. Misleading first impressions: different for different facial images of the same person. Psychol. Sci. 25, 1404–1417. ( 10.1177/0956797614532474) [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Datasets supporting this article can be accessed at http://hdl.handle.net/10023/7924.
Software used to measure and manipulate facial images is freely accessible online:
PsychoMorph (http://users.aber.ac.uk/bpt/jpsychomorph/)
MorphAnalyser (http://cherry.dcs.aber.ac.uk:8080/wiki/MorphAnalyser)