

Abstract
Autoimmune thyroid disease (AITD), including Graves disease (GD) and Hashimoto disease (HD), is an organ-specific autoimmune disease with a strong genetic component. Although the cytotoxic T-lymphocyte-associated protein 4 (CTLA4) polymorphism has been reported to be associated with AITD in adults, few studies have focused on children. The aim of our study was to investigate whether the CTLA4 polymorphisms, including -318C/T (rs5742909), +49A/G (rs231775), and CT60 (rs3087243), were associated with GD and HD in Han Chinese adults and children. We studied 289 adult GD, 265 pediatric GD, 229 pediatric HD patients, and 1058 healthy controls and then compared genotype, allele, carrier, and haplotype frequencies between patients and controls. We found that CTLA4 SNPs +49A/G and CT60 were associated with GD in adults and children. Allele G of +49A/G was significantly associated with GD in adults (odds ratio [OR], 1.50; 95% confidence interval [CI], 1.21–1.84; corrected P value [Pc] < 0.001) and children (OR, 1.42; 95% CI, 1.15–1.77; Pc = 0.002). Allele G of CT60 also significantly increased risk of GD in adults (OR, 1.63; 95% CI, 1.27–2.09; Pc < 0.001) and GD in children (OR, 1.58; 95% CI, 1.22–2.04; Pc < 0.001). Significant linkage disequilibrium was found between +49A/G and CT60 in GD and control subjects (D’ = 0.92). Our results showed that CTLA4 was associated with both GD and HD and played an equivalent role in both adult and pediatric GD in Han Chinese population.
Introduction
Autoimmune thyroid disease (AITD), including Graves disease (GD) and Hashimoto disease (HD), is an organ-specific autoimmune disease characterized by the presence of autoantibodies and T cell-mediated autoimmunity against self-antigens [1]. Both GD and HD involve similar genetic background and additional environmental and hormonal factors. Antibody-mediated thyroid stimulation prominently occurs in GD, whereas lymphocyte- and cytokine-mediated thyroid apoptosis predominates in HD, but overlap may occur [1]. They are the most prevalent autoimmune endocrinological diseases in children and adolescents [2], and are estimated to affect approximately 1% of the general population [3]. Although the exact etiology has not been fully clarified, the current hypothesis is that a complex interplay between genetic and environmental factors causes AITD [4–6].
AITD has been found to be clustered in families [7]. The risk ratio for a female sibling (λs) of a proband with GD is 15–20 [8]. The concordance rate of GD is 20–35% in monozygotic twins, but only 3–7% in dizygotic twins [9]. Twin studies also reveal that genetic factors contribute to about 75% of the development of AITD [10]. These observations strongly suggest that genetic factors are important in the pathogenesis of AITD.
The most important gene involved in AITD is the HLA-DR locus [4]. Other identified candidate genes that confer susceptibility to AITD can be classified into the following two groups: (1) immune regulatory genes: cytotoxic T-lymphocyte-associated protein 4 (CTLA4); protein tyrosine phosphatase, non-receptor 22 (PTPN22); interleukin 2 receptor (IL-2R); and (2) thyroid-specific genes: the thyroglobulin gene (TG) and the thyroid stimulating hormone receptor gene (TSHR) [4].
The CTLA4 gene encodes a transmembrane regulatory protein, cytotoxic T-lymphocyte-associated protein 4, which is expressed on activated T cells and negatively regulates their function [11]. CTLA4 competes with CD 28 binding with its ligand B7 on antigen presenting cells [12], raises the threshold of T cell activation [13], increases T cell motility and overrides T cell receptor induced stop signal required for stable conjugate formation between T cells and antigen presenting cells [14]. Several polymorphic sites in the gene, including C>T polymorphism in the promoter –318 (rs5742909) [15], A>G polymorphism in exon 1 +49A/G (rs231775) [16], microsatellite (AT)n repeat in the 3’-untranslated region (UTR) [17], and three single nucleotide polymorphisms (SNPs) in the 6.1-kb 3’ noncoding region, CT60 (rs3087243G>A), JO31 and JO30 [18, 19], are associated with organ-specific autoimmune disorders in several racial groups [18–25]. Among them, +49A/G and CT60 are the most widely investigated markers of autoimmune diseases [26]. These two polymorphisms are associated with thyroid antibody production [27, 28], GD relapse [25], Graves ophthalmopathy [29, 30], and susceptibility to GD [23, 31] and HD [32, 33]. Recently, many meta-analyses have also demonstrated the association between CTLA4 polymorphisms and AITD [34–38]. However, studies on GD in pediatric populations are limited and inconsistent [39–41]. Whether CTLA4 polymorphisms deliver different risks to adult and pediatric GD patients needs to be clarified [42, 43].
We hypothesized that the association between the CTLA4 gene and GD might be different between children and adults. Therefore we aimed to investigated CTLA4 polymorphisms (-318C/T, +49A/G, and CT60) in pediatric and adult GD patients and controls of Han Chinese ethnicity. In addition, we also analyzed these polymorphisms in HD children with the hope that the results on HD might provide more clues to help us solve the issue. The genotype, allele, carrier, and haplotype frequencies of each disease group were compared with those of ethnically matched controls.
Material and Methods
Patients
Graves disease
The subjects were 554 unrelated patients consisting of 289 adults from endocrine clinics and 265 children from pediatric clinics. An adult was defined as a person who was 18 years of age or older at diagnosis for patients or at blood sampling for controls. The adult patients were 47 men and 242 women. Their mean age at diagnosis was 33.6 years (SD = 10.2, range 18.2–66.7 years). The pediatric patients were 43 boys and 222 girls. Their mean age at diagnosis was 10.7 years (SD = 3.4, range 2.7–17.9 years). GD was diagnosed on the basis of clinical and laboratory evidence, including thyrotoxicosis, diffuse goiter, with or without ophthalmopathy, elevated free T4/total T4 levels, suppressed TSH levels, and presence of autoantibodies to TSH receptor and thyroglobulin, microsomes, or both [44, 45].
Hashimoto disease
The subjects were 229 unrelated patients from pediatric clinics, including 65 boys and 164 girls. Their mean age at diagnosis was 10.8 years (SD = 3.6, range 2.5–17.8 years). HD was diagnosed on the basis of clinical and laboratory evidence including hypothyroidism, diffuse goiter, depressed free T4/total T4 levels, elevated TSH levels, and presence of autoantibodies to thyroglobulin, microsomes or TSH receptor [46, 47].
Controls
The 1058 control subjects consisted of 478 males and 580 females. They included hospital personnel and individuals who underwent routine health examinations or minor surgery. None of them had a history of autoimmune disease. Ages were recorded for 575 subjects (mean ± SD = 15.6 ± 9.9, range 5.2–65.1 years), but the remaining 483 were only noted to be adults. All patients and controls were Han Chinese in Taiwan. The institutional review board of MacKay Memorial Hospital approved this study and all subjects and/or their guardians provided written informed consent.
Selection of single nucleotide polymorphisms (SNPs)
dbSNP -318C/T (rs5742909C>T) is at position -318 of the promoter region of the CTLA4 gene, +49A/G (rs231775A>G) is at position +49 in exon 1, and CT60 (rs3087243G>A) at position +6230 in the 3' untranslated region [18]. Individuals with the -318 T allele or +49 A/A genotype have higher CTLA4 expression [48]. The genotype G/G of CT60 is associated with a 50% decrease in the soluble CTLA4 isoform [18].
DNA extraction
Genomic DNA was extracted from fresh or frozen peripheral blood leukocytes by standard techniques.
Genotyping of the CTLA4 gene
The -318C/T, +49A/G, and CT60 polymorphisms were typed by using polymerase chain reaction–restriction fragment length polymorphism (PCR-RFLP) in 30% of the patients and 82% of controls. The procedure is detailed in our previous report [49]. The remaining patients and controls were typed using the Pre-Developed TaqMan Allelic Discrimination Assay (Applied Biosystems, Foster City, CA, USA). Briefly, polymerase chain reactions (PCR) were performed using TaqMan assay plates. Reactions contained 10 ng genomic DNA, 5 μl TaqMan Universal PCR Master Mix, 0.25 μl 40× Assay Mix, and ddH2O to a final volume of 10 μl. Thermal cycle conditions were as follows: denaturation at 95ºC for 10 min, followed by 40 cycles of denaturation at 92ºC for 15 sec, and annealing and extension at 60ºC for 1 min. Reactions were performed and read on a 7500 Fast Real-Time PCR System (Applied Biosystems). The allelic specific fluorescence data from each plate were analyzed by using the SDS v1.4.0 software (Applied Biosystems) to automatically determine the genotype of each sample.
Statistical power
We designed the study to have a power of >90% at a 5% significance level to determine a genotype relative risk of 1.61 for +49A/G (rs231775) G/G of CTLA4 in a recessive mode with a prevalence of 0.5% in GD [2] according to the Genetic Power Calculator [50]. We would need to study 223 cases and 1115 controls to be able to reject the null hypothesis.
Statistical analysis
We assessed the Hardy-Weinberg equilibrium for the SNPs, estimated the frequencies of haplotypes with an accelerated expectation-maximization algorithm, and tested pairwise linkage disequilibrium (LD) between the SNPs in both patients and controls using Haploview 4.2 [51].
Difference in genotype, allele, carrier, and haplotype distributions between patients and controls were assessed by using the χ2 test. Odds ratios (OR) and 95% confidence intervals (CI) were also calculated [52].
The Bonferroni correction, Pc = 1 –(1-P)n, was used for multiple comparisons where Pc is the corrected P value, P the uncorrected value, and n the number of comparisons [53]. In this study, n is 2 for each genotype, allele, or carrier (for simultaneously testing genotype, allele, and carrier frequencies [54]) but no correction for testing the three SNPs because of significant linkage between them and 4 for each of the four haplotypes [55]. A Pc value of less than 0.05 was considered statistically significant [56].
To test the influence of LD and detect a stronger association between alleles at two adjacent loci, we tested association with one locus in the presence or absence of the associated allele at the second locus [53].
Results
All patients and controls were successfully typed. We randomly selected and genotyped 30 specimens using both PCR-RFLP and TaqMan Allelic Discrimination Assay and found that the results were consistent. We detected no significant difference in the genotype, allele and carrier frequencies between pediatric and adult controls (data not shown). Therefore we pooled both control groups together for data presentation and analysis.
The genotype distributions of SNPs -318C/T, +49A/G, and CT60 in patients and controls were in Hardy-Weinberg equilibrium (P = 0.26–0.98) (Tables 1–3). The three SNPs were in LD with each other in the controls (D' ≥ 0.83) (Fig 1). The LD between them is strong (D' > 0.8) [57] and the three SNPs were in one block by solid spine of LD of Haploview 4.2 [51].
Table 1. Polymorphism of -318 C/T (rs5742909) of the CTLA4 gene in adult Graves disease, pediatric Graves disease, Hashimoto disease patients and controls.
| Adult Graves disease | Pediatric Graves disease | Pediatric Hashimoto disease | Controls | ||||
|---|---|---|---|---|---|---|---|
| N = 289 | N = 265 | N = 229 | N = 1058 | ||||
| Genotype | N (%) | OR (95%CI) | N (%) | OR (95%CI) | N (%) | OR (95%CI) | N(%) |
| C/C | 232(80.3) | 0.94(0.68–1.31) | 215(81.1) | 1.00(0.71–1.41) | 185(80.8) | 0.97(0.68–1.40) | 859(81.2) |
| C/T | 55(19.0) | 1.10(0.79–1.54) | 48(18.1) | 1.04(0.73–1.47) | 42(18.3) | 1.05(0.73–1.52) | 186(17.6) |
| T/T | 2(0.7) | 0.56(0.13–2.50) | 2(0.8) | 0.61(0.14–2.73) | 2(0.9) | 0.71(0.16–3.16) | 13(1.2) |
| Allele | |||||||
| C | 519(89.8) | 0.98(0.72–1.33) | 478(90.2) | 1.02(0.74–1.41) | 412(90.0) | 1.00(0.71–1.40) | 1904(90.0) |
| T | 59(10.2) | 1.02(0.75–1.38) | 52(9.8) | 0.98(0.71–1.34) | 46(10.0) | 1.00(0.72–1.40) | 212(10.0) |
| Carrier | |||||||
| C | 287(99.3) | 1.79(0.40–7.96) | 263(99.2) | 1.64(0.37–7.29) | 227(99.1) | 1.41(0.32–6.30) | 1045(98.8) |
| T | 57(19.7) | 1.06(0.76–1.47) | 50(18.9) | 1.00(0.71–1.42) | 44(19.2) | 1.03(0.71–1.48) | 199(18.8) |
Hardy-Weinberg test for adult GD: χ2 = 0.42, P = 0.81; pediatric GD: χ2 = 0.15, P = 0.93; pediatric HD: χ2 = 0.05, P = 0.97; controls: χ2 = 0.65
P = 0.72.
Table 3. Polymorphism of CT60 (rs3087243) of the CTLA4 gene in adult Graves disease, pediatric Graves disease, Hashimoto disease patients and controls.
| Adult Graves disease | Pediatric Graves disease | Pediatric Hashimoto disease | Controls | ||||
|---|---|---|---|---|---|---|---|
| N = 289 | N = 265 | N = 229 | N = 1058 | ||||
| Genotype | N(%) | OR(95%CI) | N(%) | OR(95%CI) | N(%) | OR(95%CI) | N(%) |
| A/A | 3(1.0) | 0.23(0.07–0.75) | 7(2.6) | 0.60(0.27–1.34) | 7(3.1) | 0.69(0.31–1.56) | 46 (4.3) |
| A/G | 81(28.0) | 0.69(0.52–0.92) | 68(25.7) | 0.61*(0.45–0.83) | 67(29.3) | 0.76(0.56–1.05) | 382(36.1) |
| G/G | 205(70.9) | 1.66**(1.25–2.20) | 190(71.7) | 1.72**(1.28–2.31) | 155(67.7) | 1.42(1.05–1.93) | 630(59.5) |
| Allele | |||||||
| A | 87(15.1) | 0.61**(0.48–0.79) | 82(15.5) | 0.63**(0.49–0.82) | 81(17.7) | 0.74(0.57–0.97) | 474(22.4) |
| G | 49 (84.9) | 1.63**(1.27–2.09) | 448(84.5) | 1.58**(1.22–2.04) | 377(82.3) | 1.34(1.04–1.74) | 1642(77.6) |
| Carrier | |||||||
| A | 84(29.1) | 0.60**(0.45–0.80) | 75(28.3) | 0.58**(0.43–0.78) | 74(32.3) | 0.70(0.52–0.95) | 428(40.5) |
| G | 286(99.0) | 4.33(1.34–14.04) | 258(97.4) | 1.68(0.75–3.75) | 222(96.9) | 1.44(0.64–3.24) | 1012(95.7) |
Significant values are in bold (Pc <0.05).
* Pc <0.01.
**Pc <0.001.
Hardy-Weinberg test for adult GD: χ2 = 2.66, P = 0.26; pediatric GD: χ2 = 0.10, P = 0.95; pediatric HD: χ2 = 0.01, P = 1.0; controls: χ2 = 1.57, P = 0.46.
Fig 1. Linkage disequilibrium (LD) plot in 1058 controls.
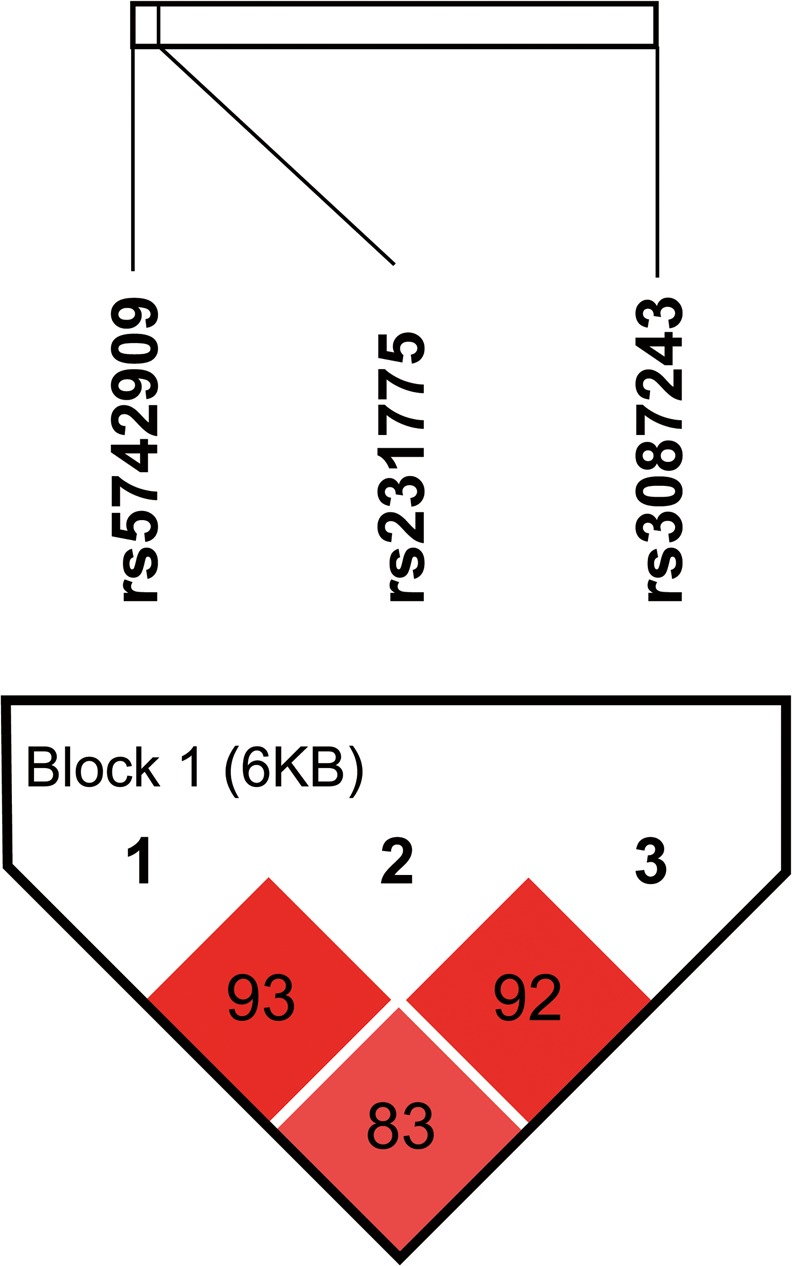
The ticks on the uppermost white bar denote the genotyped SNPs and their relative sites. The SNP pairwise information is plotted as boxes between these ticks. The number in the box denotes the D' value between each pair of SNPs. The intensity of the box color is proportional to the strength of the LD. The block is generated by solid spine of LD method in Haploview 4.2.
-318C/T (rs5742909C>T)
The distributions of genotype, allele, and carrier of -318C/T were not significantly different between adult GD, pediatric GD, HD patients and controls (Table 1).
+49A/G (rs231775A>G)
The SNP +49A/G was significantly associated with GD in adults and children, but only borderline significantly associated with HD in children (Table 2). Genotype G/G conferred a risk of 1.55 (95% CI, 1.20–2.02; Pc = 0.002) for GD in adults and of 1.56 (95% CI, 1.19–2.05; Pc = 0.002) in children. Allele G was significantly associated with GD in adults (OR, 1.50; 95% CI, 1.21–1.84; Pc < 0.001) and in children (OR, 1.42; 95% CI, 1.15–1.77; Pc = 0.002).
Table 2. Polymorphism of +49A/G (rs231775) of the CTLA4 gene in adult Graves disease, pediatric Graves disease, Hashimoto disease patients and controls.
| Adult Graves disease | Pediatric Graves disease | Pediatric Hashimoto disease | Controls | ||||
|---|---|---|---|---|---|---|---|
| N = 289 | N = 265 | N = 229 | N = 1058 | ||||
| Genotype | N(%) | OR(95%CI) | N(%) | OR(95%CI) | N(%) | OR(95%CI) | N(%) |
| A/A | 15(5.2) | 0.46(0.27–0.81) | 19(7.2) | 0.65(0.39–1.08) | 15(6.6) | 0.59(0.34–1.04) | 112(10.6) |
| A/G | 112(38.8) | 0.79(0.61–1.04) | 97(36.6) | 0.73(0.55–0.96) | 97(42.4) | 0.92(0.69–1.23) | 469(44.3) |
| G/G | 162(56.1) | 1.55*(1.20–2.02) | 149(56.2) | 1.56*(1.19–2.05) | 117(51.1) | 1.27(0.96–1.69) | 477(45.1) |
| Allele | |||||||
| A | 142(24.6) | 0.67**(0.54–0.83) | 135(25.5) | 0.70*(0.57–0.87) | 127(27.7) | 0.79(0.63–0.99) | 693(32.8) |
| G | 436(75.4) | 1.50**(1.21–1.84) | 395(74.5) | 1.42*(1.15–1.77) | 331(72.3) | 1.27(1.02–1.59) | 1423(67.2) |
| Carrier | |||||||
| A | 127(43.9) | 0.64*(0.50–0.84) | 116(43.8) | 0.64*(0.49–0.84) | 112(48.9) | 0.79(0.59–1.05) | 581(54.9) |
| G | 274(94.8) | 2.16(1.24–3.77) | 246(92.8) | 1.53(0.92–2.54) | 214(93.4) | 1.69(0.97–2.95) | 946(89.4) |
Significant values are in bold (Pc <0.05).
* Pc <0.01.
**Pc <0.001.
Hardy-Weinberg test for adult GD: χ2 = 0.60, P = 0.74; pediatric GD: χ2 = 0.34, P = 0.84; pediatric HD: χ2 = 0.74, P = 0.69; controls: χ2 = 0.04, P = 0.98.
CT60 (rs3087243G>A)
The SNP CT60 was also significantly associated with GD and HD (Table 3). Genotype G/G significantly increased the risk of GD in adults (OR, 1.66; 95% CI, 1.25–2.20; Pc < 0.001), GD in children (OR, 1.72; 95% CI, 1.28–2.31; Pc < 0.001) and HD in children (OR, 1.42; 95% CI, 1.05–1.93; Pc = 0.04). Allele G was significantly associated with GD in adults (OR, 1.63; 95% CI, 1.27–2.09; Pc < 0.001) and children (OR, 1.58; 95% CI, 1.22–2.04; Pc < 0.001).
Haplotypes of the CTLA gene and Graves disease
Seven haplotypes were detected with two major haplotypes (CGG and CAA), which accounted for >84% in combined frequency in both patients and controls (Table 4). Haplotypes CGG and CAA were significantly associated with GD in adults and children, but the association with HD was not statistically significant in children. Haplotype CGG conferred a significant risk of GD in adults (OR, 1.29; 95% CI, 1.06–1.58; Pc = 0.05) and in children (OR, 1.51; 95% CI, 1.22–1.87; Pc < 0.001) while haplotype CAA was less frequently observed in adults and pediatric GD patients than in controls. The OR for GD was 0.58 (95% CI, 0.44–0.75; Pc < 0.001) in adults and 0.67 (95% CI, 0.51–0.86; Pc = 0.008) in children.
Table 4. Frequency of haplotypes of the CTLA4 gene in adult Graves disease, pediatric Graves disease, Hashimoto disease patients and controls.
| Adult Graves disease | Pediatric Graves disease | Pediatric Hashimoto disease | Controls | ||||
|---|---|---|---|---|---|---|---|
| N = 578 | N = 530 | N = 458 | N = 2116 | ||||
| Haplotype | N(%) | OR(95%CI) | N(%) | OR (95%CI) | N(%) | OR(95%CI) | N(%) |
| CGG | 412(71.2) | 1.29(1.06–1.58) | 394(74.3) | 1.51**(1.22–1.87) | 326(71.2) | 1.28(1.03–1.60) | 1392(65.8) |
| CAA | 77(13.3) | 0.58**(0.44–0.75) | 80(15.1) | 0.67*(0.51–0.86) | 77(16.8) | 0.76(0.58–0.99) | 446(21.1) |
| TAG | 45(7.7) | 0.81(0.58–1.14) | 51(9.6) | 1.03(0.74–1.42) | 45 (9.8) | 1.05(0.75–1.48) | 199(9.4) |
| CAG | 21(3.6) | 1.86(1.09–3.17) | 3(0.6) | 0.28(0.09–0.91) | 5(1.1) | 0.55(0.21–1.39) | 42(2.0) |
| Others | 24(4.2) | 2(0.4) | 5(1.1) | 36(1.7) | |||
Significant values are in bold (Pc <0.05).
* Pc <0.01.
**Pc <0.001.
The order of SNPs in the haplotype is rs5742909-rs231775-rs3087243.
The haplotypes with a frequency of <2.0% in both patients and controls are grouped into "Others" and not compared.
Detection of independent or stronger associations
We investigated whether carrier +49G or CT60G had an independent or stronger association with AITD using 2 by 2 comparison on +49A/G and CT60 between patients and controls [53]. There was significant LD between +49A/G and CT60 in the three groups of AITD patients and controls (S1 Table). We did not detect a significant independent or stronger association between carrier +49G or CT60G and AITD. Thus, a combination of +49A/G and CT60 polymorphisms was needed to enhance the role of the CTLA4 gene in GD.
Comparisons between subgroups stratified by gender
We compared genotype, allele, and carrier frequencies of +49A/G, CT60 between disease groups and controls stratified by gender. Association was statistically significant only in females. All trends of genetic association and effect sizes were similar in males and females (data not shown).
Discussion
We demonstrated that SNPs +49A/G (rs231775) and CT60 (rs3087243) of the CTLA4 gene were significantly associated with GD in both adults and children. Genotype G/G and allele G of +49A/G as well as genotype G/G and allele G of CT60 were significantly more frequent in adult GD and pediatric GD patients than in controls. Haplotype CGG conferred a significant risk of GD in adults and children.
Our case-control study did not demonstrate any significant association between the -318C/T polymorphism and AITD. One study focusing on this polymorphism and CTLA4 protein expression showed that the -318T allele is associated with higher promoter activity and thus reduced autoimmunity [58]. However, most published studies do not show any association between -318 C/T and GD [59–62]. The homozygous T/T genotype is rare in our data set and in other populations [35, 61]. Therefore this SNP might not be important for susceptibility to AITD.
Our results suggested allele G of both +49A/G and CT60 were susceptibility factors for GD in adults and children. In addition, we found strong LD between +49A/G and CT60, but no stronger associations between +49A/G, CT60 polymorphisms and GD. This implied that the two SNPs were equally important genetic variants for GD in both children and adults. Likely, a single CTLA4 variant is not solely causative and a haplotype consisting of several variants is responsible for the association with GD [63].
Carrier G of +49A/G confers a higher risk of GD susceptibility in children than in adults [43]. The strength of the association between +49A/G and GD is similar in Japanese children and adults [42]. Allele G of CT60 is associated with a 1.61-fold risk to develop GD in children [39], and a 1.89-fold risk to develop GD in adults in Taiwanese population [31]. Our results suggested that both +49A/G and CT60 rendered an equivalent risk of GD in children and adults. Collectively, CTLA4 polymorphisms might play a similar role in conferring susceptibility to GD in both children and adults. Further large-scale studies are necessary to confirm this speculation.
The +49G allele encodes an alanine residue at codon 17 and is associated with inefficient glycosylation, decreased CTLA4 cell surface expression [64], and reduced control of T cell proliferation [65, 66]. The CT60 polymorphism correlates with soluble CTLA4 (sCTLA4, lacking exon 3) levels, with the disease-predisposing G allele rendering less sCTLA4 mRNA [18]. This suggests that a combination of +49G and CT60G might confer a lesser CTLA4 function, resulting in greater T-cell activity, stronger immune response, and a higher probability of autoimmunity. However, recently published data show a lack of correlation between the CT60 genotype and serum sCTLA4 levels [67] or even higher serum sCTLA4 levels in CT60G carriers [29]. GD patients have increased rather than decreased circulating sCTLA4 levels [29, 68, 69]. The sCTLA4 might inhibit T-cell activation by blocking the CD80/CD86-CD28 interaction in the earlier stage, but it might compete with membrane bound CTLA4 for CD80/CD86, and prevent down-regulation of T cell response in the later stage [68]. Further functional studies are required to clarify the complex relationship between CTLA4 polymorphisms, T-cell function and AITD.
In our study, only genotype G/G of CT60 was significantly associated with increased risk of pediatric HD. Although the remaining analyses on the allele and carrier distribution of CT60; on the genotype, allele, and carrier distribution of +49A/G; and on the haplotype distribution of CTLA4 showed no significant association with HD, the direction of the effect was in accord with that in GD and suggested a possible similar association as in GD. The inability to reach statistical significance is probably due to the small sample size of HD patients. Bicek at al. reported that +49G and CT60G positively correlated with GD but not with HD [70]. In an updated meta-analysis, consistent associations between +49A/G [36], CT60 [71] and GD are detected in various ethnic populations, whereas associations between +49A/G [72], CT60 [71] and HD are only found in Asians, but not in Caucasians. Effect size of genetic factors, genetic backgrounds, gene-environment interactions, and multiple mechanisms of autoimmune disease are confounding factors [34, 73]. Our results supported the notion that CTLA4 is important in the common pathogenic pathway leading to both GD and HD, but probably more involved in GD [70, 74].
Our study had several limitations. First, we did not include adult HD patients and were unable to compare the effects of CTLA4 polymorphisms between pediatric and adult HD patients. Second, we did not conduct subgroup analysis stratified by levels of antithyroid antibodies, which might confound the results. Third, we could not distinguish whether the associated alleles were causative factors or just markers linked with true disease loci.
Our study showed a significant association between CTLA4 polymorphism and GD in adults and children. The trend of the association between CTLA4 and HD was similar with less effect size and less significance. Further studies are required to elucidate the complex relationship between CTLA4 polymorphisms and AITD.
Conclusion
CTLA4 +49A/G and CT60 polymorphisms were associated GD in adults and children. Genotype G/G, allele G of +49A/G and genotype G/G, allele G of CT60 were found significantly more frequent in adults and children with GD than in controls. However, only genotype G/G of CT60 was significantly associated with HD. Our results showed that CTLA4 was associated with both GD and HD, and played an equivalent role in both adult and pediatric GD in Han Chinese population.
Supporting Information
(DOCX)
Acknowledgments
This study was supported by grants NSC 101-2314-B-715-002-MY3 from the Ministry of Science and Technology, Executive Yuan; MMH E-102-07 from MacKay Memorial Hospital, Taipei; and MMC RD1010045 from MacKay Medical College, New Taipei City; Taiwan.
Data Availability
All relevant data are within the paper and its Supporting Information files.
Funding Statement
This study was supported by grants NSC 101-2314-B-715-002-MY3 from the Ministry of Science and Technology, Executive Yuan; MMH E-102-07 from MacKay Memorial Hospital, Taipei; and MMC RD1010045 from MacKay Medical College, New Taipei City, Taiwan.
References
- 1.Brown RS. The Thyroid In: Charles G.D. Brook, Peter E. Clayton, Brown RS, editors. Brook's Clinical Pediatric Endocrinology 6th Edition Singapore: Wiley-Blackwell; 2009. p. 250–82. [Google Scholar]
- 2.Jaksic J, Dumic M, Filipovic B, Ille J, Cvijetic M, Gjuric G. Thyroid diseases in a school population with thyromegaly. Arch Dis Child 1994; 70: 103–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.McGrogan A, Seaman HE, Wright JW, de Vries CS. The incidence of autoimmune thyroid disease: a systematic review of the literature. Clin Endocrinol (Oxf) 2008; 69: 687–96. 10.1111/j.1365-2265.2008.03338.x [DOI] [PubMed] [Google Scholar]
- 4.Tomer Y. Genetic susceptibility to autoimmune thyroid disease: past, present, and future. Thyroid 2010; 20: 715–25. 10.1089/thy.2010.1644 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tomer Y, Huber A. The etiology of autoimmune thyroid disease: a story of genes and environment. J Autoimmun 2009; 32: 231–9. 10.1016/j.jaut.2009.02.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Tanda ML, Piantanida E, Lai A, Lombardi V, Dalle Mule I, Liparulo L, et al. Thyroid autoimmunity and environment. Horm Metab Res 2009; 41: 436–42. 10.1055/s-0029-1215568 [DOI] [PubMed] [Google Scholar]
- 7.Antonelli A, Ferrari SM, Corrado A, Di Domenicantonio A, Fallahi P. Autoimmune thyroid disorders. Autoimmun Rev 2015; 14: 174–80. 10.1016/j.autrev.2014.10.016 [DOI] [PubMed] [Google Scholar]
- 8.Stenszky V, Kozma L, Balazs C, Rochlitz S, Bear JC, Farid NR. The genetics of Graves' disease: HLA and disease susceptibility. J Clin Endocrinol Metab 1985; 61: 735–40. [DOI] [PubMed] [Google Scholar]
- 9.Brix TH, Kyvik KO, Christensen K, Hegedus L. Evidence for a major role of heredity in Graves' disease: a population-based study of two Danish twin cohorts. J Clin Endocrinol Metab 2001; 86: 930–4. [DOI] [PubMed] [Google Scholar]
- 10.Brix TH, Hegedus L. Twins as a tool for evaluating the influence of genetic susceptibility in thyroid autoimmunity. Ann Endocrinol (Paris) 2011; 72: 103–7. 10.1016/j.ando.2011.03.013 [DOI] [PubMed] [Google Scholar]
- 11.Kolar P, Knieke K, Hegel JK, Quandt D, Burmester GR, Hoff H, et al. CTLA-4 (CD152) controls homeostasis and suppressive capacity of regulatory T cells in mice. Arthritis Rheum 2009; 60: 123–32. 10.1002/art.24181 [DOI] [PubMed] [Google Scholar]
- 12.Fife BT, Bluestone JA. Control of peripheral T-cell tolerance and autoimmunity via the CTLA-4 and PD-1 pathways. Immunol Rev 2008; 224: 166–82. 10.1111/j.1600-065X.2008.00662.x [DOI] [PubMed] [Google Scholar]
- 13.Rudd CE. The reverse stop-signal model for CTLA4 function. Nat Rev Immunol 2008; 8: 153–60. 10.1038/nri2253 [DOI] [PubMed] [Google Scholar]
- 14.Schneider H, Downey J, Smith A, Zinselmeyer BH, Rush C, Brewer JM, et al. Reversal of the TCR stop signal by CTLA-4. Science 2006; 313: 1972–5. 1131078 [DOI] [PubMed] [Google Scholar]
- 15.Deichmann K, Heinzmann A, Bruggenolte E, Forster J, Kuehr J. An Mse I RFLP in the human CTLA4 promotor. Biochem Biophys Res Commun 1996; 225: 817–8. 10.1006/bbrc.1996.1256 [DOI] [PubMed] [Google Scholar]
- 16.Harper K, Balzano C, Rouvier E, Mattei MG, Luciani MF, Golstein P. CTLA-4 and CD28 activated lymphocyte molecules are closely related in both mouse and human as to sequence, message expression, gene structure, and chromosomal location. J Immunol 1991; 147: 1037–44. [PubMed] [Google Scholar]
- 17.Dariavach P, Mattei MG, Golstein P, Lefranc MP. Human Ig superfamily CTLA-4 gene: chromosomal localization and identity of protein sequence between murine and human CTLA-4 cytoplasmic domains. Eur J Immunol 1988; 18: 1901–5. 10.1002/eji.1830181206 [DOI] [PubMed] [Google Scholar]
- 18.Ueda H, Howson JM, Esposito L, Heward J, Snook H, Chamberlain G, et al. Association of the T-cell regulatory gene CTLA4 with susceptibility to autoimmune disease. Nature 2003; 423: 506–11. 10.1038/nature01621 [DOI] [PubMed] [Google Scholar]
- 19.Furugaki K, Shirasawa S, Ishikawa N, Ito K, Kubota S, Kuma K, et al. Association of the T-cell regulatory gene CTLA4 with Graves' disease and autoimmune thyroid disease in the Japanese. J Hum Genet 2004; 49: 166–8. 10.1007/s10038-003-0120-5 [DOI] [PubMed] [Google Scholar]
- 20.Heward JM, Allahabadia A, Armitage M, Hattersley A, Dodson PM, Macleod K, et al. The development of Graves' disease and the CTLA-4 gene on chromosome 2q33. J Clin Endocrinol Metab 1999; 84: 2398–401. [DOI] [PubMed] [Google Scholar]
- 21.Nistico L, Buzzetti R, Pritchard LE, Van der Auwera B, Giovannini C, Bosi E, et al. The CTLA-4 gene region of chromosome 2q33 is linked to, and associated with, type 1 diabetes. Belgian Diabetes Registry. Hum Mol Genet 1996; 5: 1075–80. [DOI] [PubMed] [Google Scholar]
- 22.Orozco G, Torres B, Nunez-Roldan A, Gonzalez-Escribano MF, Martin J. Cytotoxic T-lymphocyte antigen-4-CT60 polymorphism in rheumatoid arthritis. Tissue Antigens 2004; 64: 667–70. 10.1111/j.1399-0039.2004.00318.x [DOI] [PubMed] [Google Scholar]
- 23.Ban Y, Concepcion ES, Villanueva R, Greenberg DA, Davies TF, Tomer Y. Analysis of immune regulatory genes in familial and sporadic Graves' disease. J Clin Endocrinol Metab 2004; 89: 4562–8. 10.1210/jc.2003-031693 [DOI] [PubMed] [Google Scholar]
- 24.Torres B, Aguilar F, Franco E, Sanchez E, Sanchez-Roman J, Jimenez Alonso J, et al. Association of the CT60 marker of the CTLA4 gene with systemic lupus erythematosus. Arthritis Rheum 2004; 50: 2211–5. 10.1002/art.20347 [DOI] [PubMed] [Google Scholar]
- 25.Wang PW, Liu RT, Juo SH, Wang ST, Hu YH, Hsieh CJ, et al. Cytotoxic T lymphocyte-associated molecule-4 polymorphism and relapse of Graves' hyperthyroidism after antithyroid withdrawal. J Clin Endocrinol Metab 2004; 89: 169–73. [DOI] [PubMed] [Google Scholar]
- 26.Vaidya B, Pearce S. The emerging role of the CTLA-4 gene in autoimmune endocrinopathies. Eur J Endocrinol 2004; 150: 619–26. [DOI] [PubMed] [Google Scholar]
- 27.Tomer Y, Greenberg DA, Barbesino G, Concepcion E, Davies TF. CTLA-4 and not CD28 is a susceptibility gene for thyroid autoantibody production. J Clin Endocrinol Metab 2001; 86: 1687–93. [DOI] [PubMed] [Google Scholar]
- 28.Kucharska AM, Wisniewska A, Popko K, Demkow U. Association between the polymorphism A/G at position 49 of exon 1 of the CTLA-4 gene and antithyroid antibody production in children with Hashimoto's thyroiditis. Horm Res Paediatr 2012; 78: 67–72. 10.1159/000338997 [DOI] [PubMed] [Google Scholar]
- 29.Daroszewski J, Pawlak E, Karabon L, Frydecka I, Jonkisz A, Slowik M, et al. Soluble CTLA-4 receptor an immunological marker of Graves' disease and severity of ophthalmopathy is associated with CTLA-4 Jo31 and CT60 gene polymorphisms. Eur J Endocrinol 2009; 161: 787–93. 10.1530/EJE-09-0600 [DOI] [PubMed] [Google Scholar]
- 30.Han S, Zhang S, Zhang W, Li R, Li Y, Wang Z, et al. CTLA4 Polymorphisms and Ophthalmopathy in Graves’ Disease Patients: Association Study and Meta-Analysis. Hum Immunol 2006; 67: 618–26. 10.1016/j.humimm.2006.05.003 [DOI] [PubMed] [Google Scholar]
- 31.Weng YC, Wu MJ, Lin WS. CT60 single nucleotide polymorphism of the CTLA-4 gene is associated with susceptibility to Graves' disease in the Taiwanese population. Ann Clin Lab Sci 2005; 35: 259–64. [PubMed] [Google Scholar]
- 32.Terauchi M, Yanagawa T, Ishikawa N, Ito K, Fukazawa T, Maruyama H, et al. Interactions of HLA-DRB4 and CTLA-4 genes influence thyroid function in Hashimoto's thyroiditis in Japanese population. J Endocrinol Invest 2003; 26: 1208–12. 10.1007/BF03349159 [DOI] [PubMed] [Google Scholar]
- 33.Tomoyose T, Komiya I, Takara M, Yabiku K, Kinjo Y, Shimajiri Y, et al. Cytotoxic T-lymphocyte antigen-4 gene polymorphisms and human T-cell lymphotrophic virus-1 infection: their associations with Hashimoto's thyroiditis in Japanese patients. Thyroid 2002; 12: 673–7. 10.1089/105072502760258640 [DOI] [PubMed] [Google Scholar]
- 34.Qiu H, Tang W, Yin P, Cheng F, Wang L. Cytotoxic T-lymphocyte associated antigen 4 polymorphism and Hashimoto’s thyroiditis susceptibility: a meta-analysis. Endocrine 2013. 10.1007/s12020-013-9985-z [DOI] [PubMed] [Google Scholar]
- 35.Du L, Yang J, Huang J, Ma Y, Wang H, Xiong T, et al. The associations between the polymorphisms in the CTLA-4 gene and the risk of Graves' disease in the Chinese population. BMC Med Genet 2013; 14: 46 10.1186/1471-2350-14-46 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Si X, Zhang X, Tang W, Luo Y. Association between the CTLA-4 +49A/G polymorphism and Graves' disease: A meta-analysis. Exp Ther Med 2012; 4: 538–44. 10.3892/etm.2012.618 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Brandstaetter A, Zhao S- X, Pan C- M, Cao H- M, Han B, Shi J- Y, et al. Association of the CTLA4 Gene with Graves' Disease in the Chinese Han Population. PLoS One 2010; 5: e9821 10.1371/journal.pone.0009821 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Kavvoura FK, Akamizu T, Awata T, Ban Y, Chistiakov DA, Frydecka I, et al. Cytotoxic T-Lymphocyte Associated Antigen 4 Gene Polymorphisms and Autoimmune Thyroid Disease: A Meta-Analysis. Journal of Clinical Endocrinology & Metabolism 2007; 92: 3162–70. 10.1210/jc.2007-0147 [DOI] [PubMed] [Google Scholar]
- 39.Tsai ST, Huang CY, Lo FS, Chang YT, Tanizawa T, Chen CK, et al. Association of CT60 polymorphism of the CTLA4 gene with Graves' disease in Taiwanese children. J Pediatr Endocrinol Metab 2008; 21: 665–72. [DOI] [PubMed] [Google Scholar]
- 40.Yesilkaya E, Koc A, Bideci A, Camurdan O, Boyraz M, Erkal O, et al. CTLA4 gene polymorphisms in children and adolescents with autoimmune thyroid diseases. Genet Test 2008; 12: 461–4. 10.1089/gte.2008.0053 [DOI] [PubMed] [Google Scholar]
- 41.Namo Cury A, Longui CA, Kochi C, Calliari LE, Scalissi N, Salles JE, et al. Graves' disease in Brazilian children and adults: lack of genetic association with CTLA-4 +49A>G polymorphism. Horm Res 2008; 70: 36–41. 10.1159/000129676 [DOI] [PubMed] [Google Scholar]
- 42.Iwama S, Ikezaki A, Kikuoka N, Kim HS, Matsuoka H, Yanagawa T, et al. Association of HLA-DR, -DQ genotype and CTLA-4 gene polymorphism with Graves' disease in Japanese children. Horm Res 2005; 63: 55–60. 83137 [DOI] [PubMed] [Google Scholar]
- 43.Yung E, Cheng PS, Fok TF, Wong GW. CTLA-4 gene A-G polymorphism and childhood Graves' disease. Clin Endocrinol (Oxf) 2002; 56: 649–53. [DOI] [PubMed] [Google Scholar]
- 44.Barlow AB, Wheatcroft N, Watson P, Weetman AP. Association of HLA-DQA1*0501 with Graves' disease in English Caucasian men and women. Clin Endocrinol (Oxf) 1996; 44: 73–7. [DOI] [PubMed] [Google Scholar]
- 45.Susan J. Mandel, P. Reed Larsen, Davies TF. Thyrotoxicosis. In: Shlomo Melmed M, Kenneth S. Polonsky M, P. Reed Larsen M, FACP, FRCP, Henry M. Kronenberg M, editors. Williams Textbook of Endocrinology, 12th Edition. Philadelphia: Elsevier; 2011. p. 362–405.
- 46.LeFranchi S. Hypothyroidism. In: Robert M. Kliegman, Bonita F. Stanton, Joseph W. St. Geme, Nina F. Schor, Behrman RE, editors. NELSON TEXTBOOK OF PEDIATRICS, NINETEENTH EDITION. Philadelphia: Elsevier; 2011. p. 1895–903.
- 47.Donner H, Braun J, Seidl C, Rau H, Finke R, Ventz M, et al. Codon 17 polymorphism of the cytotoxic T lymphocyte antigen 4 gene in Hashimoto's thyroiditis and Addison's disease. J Clin Endocrinol Metab 1997; 82: 4130–2. [DOI] [PubMed] [Google Scholar]
- 48.Ligers A, Teleshova N, Masterman T, Huang WX, Hillert J. CTLA-4 gene expression is influenced by promoter and exon 1 polymorphisms. Genes Immun 2001; 2: 145–52. 10.1038/sj.gene.6363752 [DOI] [PubMed] [Google Scholar]
- 49.Su TH, Chang TY, Lee YJ, Chen CK, Liu HF, Chu CC, et al. CTLA-4 gene and susceptibility to human papillomavirus-16-associated cervical squamous cell carcinoma in Taiwanese women. Carcinogenesis 2007; 28: 1237–40. 10.1093/carcin/bgm043 [DOI] [PubMed] [Google Scholar]
- 50.Purcell S, Cherny SS, Sham PC. Genetic Power Calculator: design of linkage and association genetic mapping studies of complex traits. Bioinformatics 2003; 19: 149–50. [DOI] [PubMed] [Google Scholar]
- 51.Barrett JC, Fry B, Maller J, Daly MJ. Haploview: analysis and visualization of LD and haplotype maps. Bioinformatics 2005; 21: 263–5. 10.1093/bioinformatics/bth457 [DOI] [PubMed] [Google Scholar]
- 52.Lee YJ, Chen MR, Chang WC, Lo FS, Huang FY. A freely available statistical program for testing associations. MD Comput 1998; 15: 327–30. [PubMed] [Google Scholar]
- 53.Svejgaard A, Ryder LP. HLA and disease associations: detecting the strongest association. Tissue Antigens 1994; 43: 18–27. [DOI] [PubMed] [Google Scholar]
- 54.Ohashi J, Yamamoto S, Tsuchiya N, Hatta Y, Komata T, Matsushita M, et al. Comparison of statistical power between 2 * 2 allele frequency and allele positivity tables in case-control studies of complex disease genes. Ann Hum Genet 2001; 65: 197–206. [DOI] [PubMed] [Google Scholar]
- 55.Nyholt DR. Genetic case-control association studies—correcting for multiple testing. Hum Genet 2001; 109: 564–7. 10.1007/s00439-001-0611-4 [DOI] [PubMed] [Google Scholar]
- 56.Huang CY, Ting WH, Lo FS, Wu YL, Chang TY, Chan HW, et al. The IL18 gene and Hashimoto thyroiditis in children. Hum Immunol 2013; 74: 120–4. 10.1016/j.humimm.2012.10.005 [DOI] [PubMed] [Google Scholar]
- 57.Gabriel SB, Schaffner SF, Nguyen H, Moore JM, Roy J, Blumenstiel B, et al. The structure of haplotype blocks in the human genome. Science 2002; 296: 2225–9. 10.1126/science.1069424 [DOI] [PubMed] [Google Scholar]
- 58.Wang XB, Zhao X, Giscombe R, Lefvert AK. A CTLA-4 gene polymorphism at position -318 in the promoter region affects the expression of protein. Genes Immun 2002; 3: 233–4. 10.1038/sj.gene.6363869 [DOI] [PubMed] [Google Scholar]
- 59.Chong KK, Chiang SW, Wong GW, Tam PO, Ng TK, Hu YJ, et al. Association of CTLA-4 and IL-13 gene polymorphisms with Graves' disease and ophthalmopathy in Chinese children. Invest Ophthalmol Vis Sci 2008; 49: 2409–15. 10.1167/iovs.07-1433 [DOI] [PubMed] [Google Scholar]
- 60.Vaidya B, Oakes EJ, Imrie H, Dickinson AJ, Perros P, Kendall-Taylor P, et al. CTLA4 gene and Graves' disease: association of Graves' disease with the CTLA4 exon 1 and intron 1 polymorphisms, but not with the promoter polymorphism. Clin Endocrinol (Oxf) 2003; 58: 732–5. [DOI] [PubMed] [Google Scholar]
- 61.Braun J, Donner H, Siegmund T, Walfish PG, Usadel KH, Badenhoop K. CTLA-4 promoter variants in patients with Graves' disease and Hashimoto's thyroiditis. Tissue Antigens 1998; 51: 563–6. [DOI] [PubMed] [Google Scholar]
- 62.Zhang Q, Yang YM, Lv XY. Association of Graves' disease and Graves' ophthalmopathy with the polymorphisms in promoter and exon 1 of cytotoxic T lymphocyte associated antigen-4 gene. J Zhejiang Univ Sci B 2006; 7: 887–91. 10.1631/jzus.2006.B0887 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Butty V, Roy M, Sabeti P, Besse W, Benoist C, Mathis D. Signatures of strong population differentiation shape extended haplotypes across the human CD28, CTLA4, and ICOS costimulatory genes. Proc Natl Acad Sci U S A 2007; 104: 570–5. 10.1073/pnas.0610124104 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Anjos S, Nguyen A, Ounissi-Benkalha H, Tessier MC, Polychronakos C. A common autoimmunity predisposing signal peptide variant of the cytotoxic T-lymphocyte antigen 4 results in inefficient glycosylation of the susceptibility allele. J Biol Chem 2002; 277: 46478–86. 10.1074/jbc.M206894200 [DOI] [PubMed] [Google Scholar]
- 65.Kouki T, Sawai Y, Gardine CA, Fisfalen ME, Alegre ML, DeGroot LJ. CTLA-4 gene polymorphism at position 49 in exon 1 reduces the inhibitory function of CTLA-4 and contributes to the pathogenesis of Graves' disease. J Immunol 2000; 165: 6606–11. [DOI] [PubMed] [Google Scholar]
- 66.Ban Y, Davies TF, Greenberg DA, Kissin A, Marder B, Murphy B, et al. Analysis of the CTLA-4, CD28, and inducible costimulator (ICOS) genes in autoimmune thyroid disease. Genes Immun 2003; 4: 586–93. 10.1038/sj.gene.6364018 [DOI] [PubMed] [Google Scholar]
- 67.Purohit S, Podolsky R, Collins C, Zheng W, Schatz D, Muir A, et al. Lack of correlation between the levels of soluble cytotoxic T-lymphocyte associated antigen-4 (CTLA-4) and the CT-60 genotypes. J Autoimmune Dis 2005; 2: 8 10.1186/1740-2557-2-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Saverino D, Brizzolara R, Simone R, Chiappori A, Milintenda-Floriani F, Pesce G, et al. Soluble CTLA-4 in autoimmune thyroid diseases: relationship with clinical status and possible role in the immune response dysregulation. Clin Immunol 2007; 123: 190–8. 10.1016/j.clim.2007.01.003 [DOI] [PubMed] [Google Scholar]
- 69.Oaks MK, Hallett KM. Cutting edge: a soluble form of CTLA-4 in patients with autoimmune thyroid disease. J Immunol 2000; 164: 5015–8. [DOI] [PubMed] [Google Scholar]
- 70.Bicek A, Zaletel K, Gaberscek S, Pirnat E, Krhin B, Stopar TG, et al. 49A/G and CT60 polymorphisms of the cytotoxic T-lymphocyte-associated antigen 4 gene associated with autoimmune thyroid disease. Hum Immunol 2009; 70: 820–4. 10.1016/j.humimm.2009.06.016 [DOI] [PubMed] [Google Scholar]
- 71.Ni J, Qiu LJ, Zhang M, Wen PF, Ye XR, Liang Y, et al. CTLA-4 CT60 (rs3087243) polymorphism and autoimmune thyroid diseases susceptibility: a comprehensive meta-analysis. Endocr Res 2014. 10.3109/07435800.2013.879167 [DOI] [PubMed] [Google Scholar]
- 72.Feng M, Zhang FB, Deng HR. The CTLA4 +49A/G polymorphism is associated with an increased risk of Hashimoto's thyroiditis in Asian but not Caucasian populations: an updated meta-analysis. Endocrine 2013; 44: 350–8. 10.1007/s12020-013-0014-z [DOI] [PubMed] [Google Scholar]
- 73.Lee HJ, Li CW, Hammerstad SS, Stefan M, Tomer Y. Immunogenetics of autoimmune thyroid diseases: A comprehensive review. J Autoimmun 2015; 64: 82–90. 10.1016/j.jaut.2015.07.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Pastuszak-Lewandoska D, Sewerynek E, Domanska D, Gladys A, Skrzypczak R, Brzezianska E. CTLA-4 gene polymorphisms and their influence on predisposition to autoimmune thyroid diseases (Graves' disease and Hashimoto's thyroiditis). Arch Med Sci 2012; 8: 415–21. 10.5114/aoms.2012.28593 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(DOCX)
Data Availability Statement
All relevant data are within the paper and its Supporting Information files.