

Highlights
-
•
Volar dislocation of the distal radioulnar joint is a rare injury and can be easily missed.
-
•
The stability of the DRUJ is enhanced by ligaments and muscles, and The triangular fibro cartilage complex (TFCC) is the most important stabilizer.
-
•
In cases of volar dislocation, there is a history of hyper supination and the patient is unable to pronate.
-
•
In cases of volar dislocation, there is a history of hyper supination and the patient is unable to pronate.
Keywords: DRUJ, Volar dislocation, TFCC, Pronator quadratus, Case report, Methods
Abstract
Introduction
Volar dislocation of the distal radioulnar joint is a rare injury which is commonly missed in the emergency departments. A thorough review of literature showed very few reported cases and the cause for irreducibility varied in different cases, Lack of suspicion and improper X-ray can delay the diagnosis.
Case presentation
Our article discusses a case 40 year old construction worker, who presented to the Emergency with work-related injury, complaining of left wrist pain, deformity and inability to rotate his forearm. X-rays revealed a volar dislocation of distal ulna which was reducible after manipulation under General Anesthesia (GA). The joint was stable after the reduction.
Discussion
Isolated dislocation of the distal radioulnar joint can be either volar or dorsal, although dorsal dislocation is more common. The distal radioulnar articulation plays an important role in the rotational movement of the forearm. It allows pronation and supination which are essential for the function of the upper limb. Pronator Quadratus muscle spasm is an important blockade to reduction and was preventing reduction in this case.
Methods
The work has been reported in line with the CARE criteria [9].
Conclusion
Volar locked dislocation of Distal Radio ulnar joint is a rare injury. High degree of clinical suspicion and proper X-ray is required for prompt detection.
The importance of this case is to raise the awareness among physicians in treating these kind of injuries by careful assessment of the patient and radiographs, and to consider pronator quadratus as an important cause for the blockade to reduction.
1. Introduction
Isolated dislocation of the distal radioulnar joint (DRUJ) can be easily missed in a busy emergency setting due to lack of obvious clinical deformity and incorrect evaluation of wrist radiographs. If not promptly recognized and treated, these injuries can lead to significant functional disability [1]. Dorsal dislocation is more common than volar dislocation. Our Case was readily recognized and treated in emergency as the joint was locked in supination. Literature review showed sporadic case reports of this rare injury. These cases had different causes for irreducibility and stability post reduction and hence were treated in different ways.
2. Case report
A 40-year-old male worker, Right hand dominant, presented to the Emergency department following a work-related injury. As he was using the electrical drill, the drill got stuck and his left forearm forcefully rotated in supination. He presented with left wrist pain and deformity and inability to rotate his forearm.
The patient had no previous medical or surgical history related to the injury, and had no previous injuries to the wrist, forearm or hand.
On examination, his left forearm was in supinated 10 ° position with absence of the ulnar head prominence on the dorsum of the forearm, with bulging of the ulnar side on the volar aspect of the left forearm. The patient was unable to further rotate the forearm. There were no sensory or motor deficit and distal pulses were intact, and the skin was intact (Fig. 1).
Fig. 1.

Clinical Photos of the patient on presentation.
Initial radiographs were made. The anteroposterior radiograph demonstrated an overlap of the radius and ulna at the distal radioulnar joint, and a true lateral radiograph demonstrated volar displacement of the ulna with respect to the radius. There is also ulnar styloid fracture associated with the injury (Fig. 2).
Fig. 2.
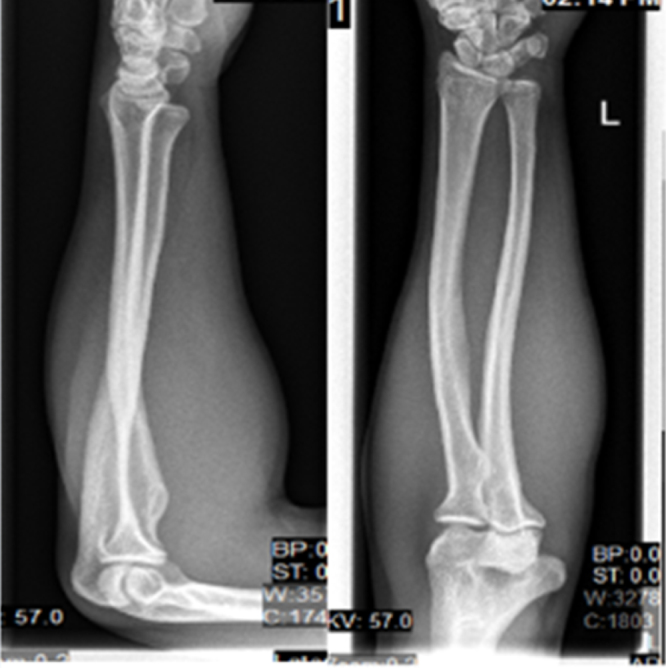
X-rays of the forearm at initial presentation.
Closed reduction was attempted by rotating the forearm but failed, with the patient under conscious sedation short GA, a closed reduction was attempted in the emergency department with use of a commonly accepted maneuver of distraction of the distal radioulnar joint, direct pressure on the ulnar head, and passive pronation.
The reduction was successful and the DRUJ was absolutely stable after reduction (Fig. 3).
Fig. 3.

X-rays of the forearm after reduction.
Above elbow back slab was applied in mid-pronation position and the patient came to the clinic after one week, where a long arm cast was applied for 3–4 weeks.
3. Discussion
Acute, isolated dislocation of the distal radioulnar joint was reported as early as in 1777 by Desault. The dislocation can be either volar or dorsal, although dorsal dislocation is more common [2].
The distal radioulnar articulation plays an important role in the rotational movement of the forearm and it is unstable by nature [7]. It allows pronation and supination which are essential for the function of the upper limb [3]. Due to the difference in the anatomy between the ulna and the radius in terms of radius of curvature, some degree of translocation also occurs during movement at the DRUJ [7]. During supination, the head of the ulna translates volarly and during pronation dorsally [3]. The radial notch is shallow and does not constrain the ulna during these movements.
The ligaments and muscles which enhance the stability of the DRUJ are the triangular fibro cartilage complex (TFCC), the ulnar carpal ligaments, the extensor retinaculum, the pronator quadratus muscle and the interosseous membrane [3]. Sectioning of all these soft tissues around the joint leads to significant instability as showed by cadaveric studies highlighting their importance [8].
The TFCC is the most important stabilizer. Up to fifty percent of all DRUJ dislocations are missed in the initial evaluation, especially if the injury is not associated with fracture. Secondary instability can develop following unrecognized DRUJ dislocation, which highlights the importance of careful history and physical examination in diagnosing these injuries.
A true lateral X-ray confirms the diagnosis [4]. Any rotation of the forearm during radiographic examination will change the relative position of the ulna making the diagnosis difficult [3].
In 1992, Bruckner et al. used the term “complex DRUJ dislocation” to describe dislocations of the distal radioulnar joint that met the following criteria: “obvious irreducibility, recurrent subluxation, or ‘mushy’ reduction caused by soft-tissue or bone interposition.” [5]. The fist hypothesis regarding the mechanism of injury was the interposition of extensor carpi ulnaris tendon in the distal radioulnar joint.
In DRUJ dislocations the Extensor carpi ulnaris tendon can be displaced either to the ulnar or radial border of the distal part of the ulna.
Factors that causes blocking of reduction in DRUJ dislocation are displacement of the ulnar styloid which causes extensor carpi ulnaris tendon dislocation,entrapment of the extensor digitorum communis to the ring and little finger, the extensor digiti minimi, the flexor pollicis longus, fragments of a torn triangular fibrocartilage complex, or even the median nerve [5].
The compressive pull of the pronator quadrates is another important cause of irreducibility in volar dislocations.
The severity of injury to TFCC ligaments is not clear in DRUJ dislocation. It was observed in many cases that the joint was stable after reduction suggesting that an incomplete TFCC injury may be sufficient for DRUJ dislocation.
Hagert, has described the mechanism of injury in volar vs dorsal dislocation. In dorsal dislocation the volar radioulnar ligament and dorsal joint capsule are disrupted while in volar dislocation the dorsal radioulnar ligament and volar joint capsule are disrupted. The interosseous membrane is the secondary constraint to palmar dislocation [6].
In cases of volar dislocation, there is a history of hyper supination and the patient is unable to pronate. The ulnar head is usually not visibly prominent on the volar wrist because of the overlying soft tissues. However, there can be a hollow dorsally where the ulnar head is usually visible. The wrist can appear narrow because of the compressive pull of the pronator quadratus muscle, resulting in a diminished transverse dimension.
In volar dislocation the X-ray shows an overlap of radius and ulna at the DRUJ. This is due to the pull of the pronator quadrates.
A standard Posteroanterior view of the wrist demonstrates DRUJ dislocation. This is done with the shoulder abducted 90 ° and the elbow at 90 ° flexion and neutral forearm rotation.
Even a 10 ° oblique malalignment can lead to false negative results.
If the diagnosis is uncertain, it can be confirmed by further imaging like CT scan or Magnetic resonance imaging (MRI), which demonstrates any joint incongruence.
Associated lesions can also be detected by these imaging procedures.
Treatment is usually closed reduction under Local anesthesia with or without Sedation.
In our Case, reduction was possible only after full muscle relaxation under GA. Post reduction the joint was absolutely stable. This suggests that the spasm of pronator quadrates was the chief blockade to reduction in this case.
The forearm was immobilized in above elbow slab in neutral rotation and later converted to cast after 1 week follow up in clinic. (Although the new recommendation is to immobilize the forearm in pronation).
In the Follow up in clinic after 3 months patient had no complaints. Full range of supination, pronation and flexion and extension.
The work has been reported in line with the CARE criteria [9].
4. Conclusion
Volar locked dislocation of Distal Radio ulnar joint is a rare injury. High degree of clinical suspicion and proper X-ray is required for prompt detection. Spasm of Pronator Quadratus muscle is an important blockade to reduction in volar DRUJ dislocations and will require relaxation of this muscle for reduction. Post reduction the joint can be very stable negating any need for internal fixation.
Conflict of interest
All authors in the paper have no conflict of interest.
Funding
No source of funding. No sponsors.
Consent
Informed consent was taken from the patient for publication of the case and related data.
Author’s contribution
Dr. Fadi Bouri: Resident Orthopedics, First Author, involved in Writing the discussion, design Dr. Mazhar Fuad: Specialist Orthopedics, Co-Author, contributed in writing the discussion Dr. Ayman Elsayed Abolenour: Consultant Orthopedics, Primary physician of the patient and data collection, Co-Author.
Contributor Information
Fadi Bouri, Email: Fadi.bouri@gmail.com, faboray@hotmail.com.
Mazhar Fuad, Email: Drfuad14@gmail.com.
Ayman Elsayed Abdolenour, Email: Ayman2882@hotmail.com.
References
- 1.Mittal R., Kulkarni R., Subsposh S.Y., Giannoudis P.V. Isolated volar dislocation of distal radioulnar joint: how easy to miss! Eur. J. Emerg. Med. 2004;11(April (2)):113–116. doi: 10.1097/00063110-200404000-00012. [DOI] [PubMed] [Google Scholar]
- 2.Dameron T.B., Jr. Traumatic dislocation of the distal radio-ulnar joint. Clin. Orthop. Relat. Res. 1972;83:55–63. doi: 10.1097/00003086-197203000-00010. [DOI] [PubMed] [Google Scholar]
- 3.Szabo R.M. Distal radioulnar joint instability. Instr. Course Lect. 2007;56:79–89. [PubMed] [Google Scholar]
- 4.Nicolaidis S.C., Hildreth D.H., Lichtman D.M. Acute injuries of the distal radioulnar joint. Hand Clin. 2000;16:449–459. [PubMed] [Google Scholar]
- 5.Bruckner J.D., Lichtman D.M., Alexander A.H. Complex dislocations of the distal radioulnar joint: recognition and management. Clin. Orthop. Relat. Res. 1992;275:90–103. [PubMed] [Google Scholar]
- 6.Hagert C.G. Distal radius fracture and the distal radioulnar joint—anatomical considerations. Handchir. Mikrochir. Plast. Chir. 1994;26(1):22–26. [PubMed] [Google Scholar]
- 7.Robert M., Szabo M.P.H. Distal radioulnar joint instability. J. Bone Joint Surg. Am. 2006;88(April 4):884–894. doi: 10.2106/00004623-200604000-00027. [DOI] [PubMed] [Google Scholar]
- 8.Wade Gofton T., Karen Gordon D., Cynthia Dunning E., James Johnson A., Graham King J.W. Soft-tissue stabilizers of the distal radioulnar joint: an in vitro kinematic study. J. Hand Surg. 2016 doi: 10.1016/j.jhsa.2004.01.020. http://www.jhandsurg.org/article/S0363-5023(04)00199-6/abstract [DOI] [PubMed] [Google Scholar]
- 9.Joel Gagnier J., Kienle Gunver, Douglas Altman G., David Moher, Sox Harold, Riley David, The CARE Group The CARE guidelines: consensus-based clinical case reporting guideline development. BMJ Case Rep. 2013 doi: 10.1186/1752-1947-7-223. [DOI] [PMC free article] [PubMed] [Google Scholar]