

Abstract
We experienced a case of an elongated styloid process that was 8 cm in length. The patient was a 68-year-old Japanese man with frequent episodes of left-sided throat pain for 10 years. The elongated styloid process could be diagnosed by 3D-computed tomography (left and right length: 7.8 cm and 8.0 cm, respectively) and successfully treated with surgery, since the anatomic relationships could be fully visualized. Surgical methods for shortening an elongated styloid process involve an intraoral or external approach. The external approach to the styloid process involves a trans-cervical approach to the parapharyngeal space, which enables wider visualization in the operative field than an intraoral approach. In the present case, the styloid process reached the parapharyngal space. Therefore, we selected the external approach and shortened only the left-sided styloid process (the same side as the throat pain). The chief complaint disappeared immediately after the operation.
Key words: Elongated styloid process, transcervical approach, 3D-computed tomography, Eagle syndrome
Introduction
The normal length of styloid process is 17.4-18.8 mm in Japanese.1 Eagle2 reported an abnormal styloid process that was over 2.5 cm. Kaufman3 described that the mean length of the styloid process on the right and left sides was 30 mm and 29.49 mm, respectively in panographic radiographs of 484 hospitalized patients. He also reported that the mean length for elongated styloid processes was roughly 33 mm and 53 mm for left and right side. A styloid process more than 6 cm in length is considered giant.1 Therefore, a case of an elongated styloid process over 6 cm in length is very rare. We encountered a patient with an elongated styloid process 8 cm in length. Our case report presents the clinical findings, the diagnostic usefulness of 3D-computed tomography (3D-CT), and a comparison of treatment methods with reference to the existing literature, which could lead to better understanding of the pathophysiology and safer therapies for elongated styloid process.
Case Report
A 68-year-old Japanese man complained of repeated left-sided throat pain for 10 years and hard swallowing pain since 2 weeks before. Physical examination revealed no abnormal findings in the oral cavity, pharygolarynx or neck. 3D-CT showed bilateral elongated styloid processes (lengths of left and right: 7.8 cm and 8.0 cm). The right styloid process was longer and thicker than the left styloid process (Figure 1). We performed shortening of only the left-sided styloid process (the same side of throat pain) using by a transcervical approach (Figure 2). His chief compliant disappeared immediately after the operation (Figure 3). Stimulation of the pharynx or cervical nerves from an elongated styloid process is known to cause pharyngeal and swallowing pain.
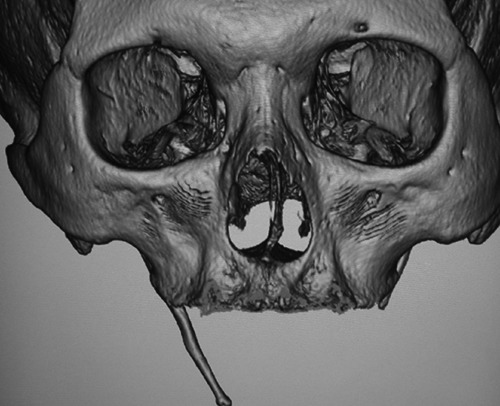
Figure 1.

Length of left and right styloid process (arrows) was 7.8 cm (empty arrow) and 8.0 cm (black arrow) in 3D-computed tomography, respectively.
Figure 2.
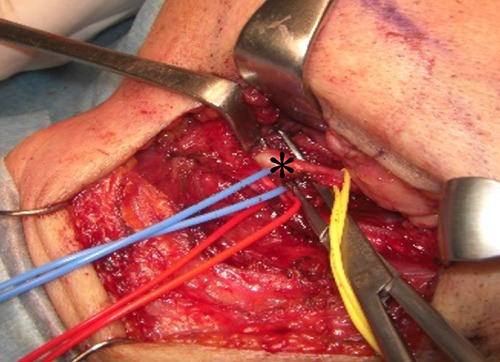
Left styloid process (asterisk) could be safely shortened by the external approach without injuring the hypoglossal nerve.
Figure 3.
This image was postoperative 3D-computed tomography. His throat pain was improved by shortening the left styloid process.
Discussion and Conclusions
Our patient was male and 68-year-old. Some institutions4,5 reported that no statistically significant correlation was found between the presence of elongated styloid process between the genders.
Ghosh and Corrella revealed that this disease was largest distribution of patients in age was seen in fifth decade of life. Vieira4 indicated that 36.28% of the elongated styloid process showed both right and left sides as our case. Kaufman,3 Vieira4 and Corrella6 demonstrated that there was no significant correlation of process elongation and calcification to age. Mendelsonhn7 and Yasmeenahamed8 reviewed only 4% of patients with elongated processes would be symptomatic. Chief complaints of our patient were repeated left-sided throat pain for 10 years and swallowing pain.
Some5,9 reported that pain in the throat was most frequently encountered as the presenting complaints, and majority of kind of complaints (e.g., pain in the throat, painful swallowing, foreign body sensation in the throat,) had more than one complaint as our case. Such a rare case, Maik10 introduced a patient as having glossopharyngeal neuralgia due to elongated styloid process could lead to syncope and seizures.
Ghosh5 in detail discussed the mechanism of elongation of the styloid process as follows.
The styloid process is derived from the second branchial bar of cartilage of Reichert. This cartilage consists of four highly variable parts (tympanohyale, stylohyale, ceratohyale, hypohyale). Long process results from the ossification of the tympanohyale and the styohyle portions during the first 8 years of life, and short process encountered from the ossification for the tympanohyale segment only while stylo- and ceratohyale portions degenerate. Conventionally, postnatal growth of the styloid has been advanced as a possible mechanism for the elongated styloid process. But a correlation between an increase in styloid process length and age has not been substantiated.
Recently developed histologic and microradiographic techniques had not identified process.
Beder11 recommended that 3D-CT was the radiologic investigation of choice for elongated styloid process because of the most advanced technique available for definitively measuring the length of the styloid process. Also, our elongated styloid process could be easily diagnosed by 3D-CT (left and right lengths: 7.8 cm and 8.0 cm, respectively) and safety treated with surgery, since it can fully visualize the anatomic relationships.
The management of this disease process has been known to be non-surgical or surgical treatment.12,13 The nonsurgical treatment generally involves pharmacotherapy with anticonvulsants or antidepressants, but the results are short-lived.12,14 Therefore, many hospitals1,5,6,8,12,15 stated that the first choice for treatment of elongated styloid process was surgery because of the severity of symptoms. Ghosh5 insisted that surgical shortening of the elongated process was the only to give symptomatic relief to the patient. This surgical shortening of an elongated styloid process is often performed using an intraoral or external approach.7,15,16 It can often enable an intraoral approach requiring shorter surgical time and less surgical trauma without leaving visible scars on the neck. The external approach to the styloid process involves a transcervical approach to the parapharyngeal space,6 and wider visualization in the operative field than an intraoral approach.7,15,16 In our cases, the styloid process reached the parapharyngeal space. Therefore, we selected the external approach. Recently, it reported that endoscopic-assisted styliodectomy for this disease could safety resect stylohyoid ligament with a smaller portion remaining at the skull base.13 In our case, the right styloid process was longer and thicker than the left styloid process. However, since the throat symptoms at swallowing were on the left side, appeared that the longer and thicker right styloid process would work as the pivot of a door and that the left styloid process had an abnormal orbit that stimulated the pharynx muscles and cervical nerves.
References
- 1.Sakaguchi H, Asano J, Sado F, et al. An elongated styloid process shortened with external approach. Pract Otol 2000;93:971-7. [Google Scholar]
- 2.Eagle WW. Symptomatic elongated styloid process; report of two cases of styloid process-carotid artery syndrome with operation. Arch Otolaryngol 1949;49:490-503. [DOI] [PubMed] [Google Scholar]
- 3.Kauffman SM, Elzay RP, Irish E F. Styloid process variation; radiological and clinical study. Arch Otolaryngol 1970;91:460-3. [DOI] [PubMed] [Google Scholar]
- 4.Vieira EM, Guedes OA, Morais SD, et al. Prevalence of elongated styloid process in Central Brazilian. J Clin Diagn Res 2015:9:ZC90-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ghosh LM, Dubey SP. The syndrome of elongated styloid process. Auris Nassus Larynx 1999:26;169-75. [DOI] [PubMed] [Google Scholar]
- 6.Corrella RW, Jensen JL, Taylor JB, et al. Mineralization of the stylohyoid-stylomandibular ligament complex. Oral Surg 1974:48:286-91. [DOI] [PubMed] [Google Scholar]
- 7.Mendelsonhn AH, Berke GS, Chhetri DK. Heterogeneity in the clinical presentation of Eagle’s syndrome. Otolaryngol Head Neck Surg 2006;134:389-93. [DOI] [PubMed] [Google Scholar]
- 8.Yasmeenahamed S, Laliytha BK, Sivaraman S, et al. Eagle’s syndrome-masquerading as ear pain: review of literature. J Pharm Bioallied Sci 2015:7:S372-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Tanaka K, Ozawa H, Kitajima K. Four cases of elongation of the styloid process. Pract Otol 1997;90:1255-61. [Google Scholar]
- 10.Malik Y, Dar JA, Almeadani AA. Seizures with an atypical aetiology in an elderly patient: Eagle’s syndrome-how dose one treat it?. BMJ Case Rep 2015. [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Beder E, Ozgursoy OB, Ozgursoy SK, Anadolu Y. Three-dimensional computed tomography and surgical treatment for Eagle’s syndrome. Ear Nose Throat J 2006;85:443-45. [PubMed] [Google Scholar]
- 12.Kim E, Hansen K, Frizzi J. Eagle syndrome: case report and review of the literature. Ear Nose Throat J 2008;87:631-3. [PubMed] [Google Scholar]
- 13.Weteid AS, Miloro M. Transoral endoscopic-assisted styloidectomy: how should Eagle syndrome be managed surgically?. Int J Oral Maxillfac Surg 2015;44:1181-7. [DOI] [PubMed] [Google Scholar]
- 14.Prasad KC, Kamath MP, Reddy KI, et al. Elongated styloid process (Eagle’s syndrome): a clinical study. J Oral Maxilofac Surg 2002;60:171-5. [DOI] [PubMed] [Google Scholar]
- 15.Strauss M, Zohar Y, Laurian N. Elongated styloid process syndrome: intraoral versus external approach for styloid surgery. Laryngoscope 1985;95:976-9. [PubMed] [Google Scholar]
- 16.Miyata R, Kondo A, Seki N, et al. Elongated styloid process. Pract Otol 2012;105:814-5. [Google Scholar]