

Abstract
As the segment of the population 65 years of age or older continues to grow, the number of individuals with dementia increases proportionally, highlighting the need to design therapies that meet the social and emotional needs of people with dementia. Information and communication technologies (ICT) are potential venues for supporting the delivery of such therapies, including reminiscence therapy (RT), which is a non-pharmacological intervention involving the prompting of past memories, often with artifacts such as old photographs or music for therapeutic benefits such as the facilitation of social interactions or the increase of self-esteem. This paper systematically examines the scientific literature on the use of ICT for facilitating RT to assess the current state of the evidence and identify future trends. We searched the PubMed (1966–2013), ACM (1954–2013), and PsycINFO (1908–2013) repositories using the keywords dementia and reminiscence. Three hundred eighty-six articles were retrieved, 44 of which met the inclusion and exclusion criteria. Findings of the systematic review include that there are benefits to using ICT for RT interventions. Some of these benefits are access to rich and engaging multimedia reminiscence materials, opportunities for people with dementia to participate in social interactions and take ownership of conversations, and a reduction of barriers due to motor deficits during interactions with media. Future studies should explore the types and content of media beneficial to individuals at different stages of dementia.
Keywords: aging and health, computer-mediated health promotion, dementia, media, public and consumer health informatics, reminiscence therapy
Dementia is a disease estimated to have affected 14.7% of Americans over the age of 70 in 2010 (Hurd, Martorell, Delavande, Mullen, & Langa, 2013). As the population of older adults grows worldwide, the number of individuals with dementia will increase proportionally. Dementia is most commonly marked by a loss of memory but also affects other cognitive skills, such as language, judgment, and problem solving (Bird & Miller, 2010) and the ability to independently carry out activities of daily living. While pharmacological treatments to address the biological dimensions of the disease have advanced, there is a need for non-pharmacological treatments to meet the social and emotional needs of people with dementia. Guidelines for dementia, such as the NICE clinical guidelines (National Institute for Health and Clinical Excellence, 2006), advise the use of non-pharmacological treatments for challenging behaviors in dementia prior to pharmacological treatments.
Standard non-pharmacological therapies for dementia include behavior therapy (addressing triggers of challenging behavior), validation therapy (empathizing with expressed emotions), and reminiscence therapy (RT; involving the “the act or process of recalling the past,” often using artifacts to unleash memories and prompt conversation for present benefit; Butler, 1963). One of the advantages of RT compared to the other therapies mentioned above is that it can be used with people with varying levels of cognition, including those who have lost ability to verbalize (Douglas, James, & Ballard, 2004).
RT has the potential to benefit individuals with dementia as well as family caregivers and to improve staff care. Therapeutic purposes of RT for people with dementia include reducing social isolation, offering an enjoyable and stimulating activity, promoting self-worth, and providing a way to sustain relationships with loved ones (Gibson, 2004). Although reminiscence often involves pleasant memories to promote enjoyment, it can also involve serious or sad memories for therapeutic or cathartic purposes (Parker, 2006). RT also offers benefits for family caregivers, including new ways of interacting with a relative (Gibson, 2004). Additionally, engaging in RT with residents with dementia provides an opportunity for staff to better understand the resident’s current behaviors and personality (Gibson, 1994). Several reviews have been published on randomized control trials of RT interventions, both for the general population of older adults (Y.-C. Lin, Dai, & Hwang, 1994) and for those with dementia (Cotelli, Manenti, & Zanetti, 2012; Subramaniam & Woods, 2012; Woods, Spector, Jones, Orrell, & Davies, 2009). These reviews identified problems with available evidence that include differing RT forms, limited number of studies, and small samples. Despite these problems, RT appears to be a promising intervention for individuals with dementia, with outcomes including improvements in mood, cognition, and behavior (Cotelli et al., 2012; Woods et al., 2009).
With advances in technology, there can be increased access to tools for health-related interventions, such as information and communication technology (ICT). Benefits of using ICT for people with dementia include the possibility of increasing the pool of study participants, the effectiveness of intervention, and the ability to assess outcomes. ICT has the potential to be a practical way to support the delivery of RT, whether through permitting individuals to stay in their local communities while communicating with others at a distance, using engaging multimedia, allowing for multiple users, or interacting through dynamic methods. One review addressed systems that used ICT to deliver RT and concluded that using ICT is feasible for RT in a population with dementia (Subramaniam & Woods, 2010); however, it did not address in depth how different forms of ICT have been used to benefit RT. Studying the different types of ICT used can lead to an understanding of how different technologies affect the delivery, quality, and effectiveness of an RT intervention. This understanding can aid future researchers and clinicians in designing or implementing a system. The aim of this study is to systematically examine the scientific literature on the use of ICT in conducting RT in order to assess current evidence, make recommendations regarding potential uses and challenges of using technology with persons with dementia, and identify areas requiring further study. The goal of the study is not to evaluate therapeutic benefits of RT but, rather, to examine the applications of ICT to RT.
The key questions explored in this review are as follows:
What kinds of technology have been used to facilitate RT?
What purpose did the technology serve?
Method
Sources
Three databases were searched: (a) ACM Guide to Computing Literature (1954 to September 2013), (b) PubMed (1966 to September 2013), and (c) PsycINFO (1908 to September 2013). All databases were searched with the text “dementia AND reminiscence.” Although the focus of this review was on technology use, no reference to technology or ICT was included in the search terms to ensure that interventions using technologies such as audio platforms for music that may not have been classified as “information technology” could still be considered for inclusion.
Ten percent of the retrieved articles were evaluated for inclusion by two investigators to determine reliability of article inclusion. One hundred percent agreement was obtained.
Inclusion and Exclusion Criteria
To be included in the review, studies had to (a) describe the design or evaluation of an RT intervention, (b) include ICT use in the intervention delivery, (c) be written in English, and (d) be targeted toward individuals with dementia (for example, a paper discussing how an intervention benefited a caregiver without discussing how it impacted individuals with dementia would not be included, nor would a study of a mixed population that did not include subgroup analysis for individuals with dementia). ICT was defined for this review as electronic technology used to present, access, or manipulate media (e.g., computer, cassette player, TV). The study did not need to specifically mention the words ICT or technology if the technology met the definition of ICT used by the researchers. Introductions, letters and comments, abstracts, theoretical/conceptual papers, books, and reviews were excluded.
Results
The initial search returned 386 papers, 115 from the ACM database, 107 from the PubMed database, and 164 from the PsycINFO database. Abstracts and titles were sufficient to rule out papers that did not meet inclusion criteria (a) or (c). One hundred full papers were reviewed when it was not clear whether they included ICT (criteria [b]). Twenty-four ACM papers, 13 PubMed papers, and 7 PsycINFO papers met the inclusion and exclusion criteria, resulting in a total of 44 papers (see Figure 1). Results are organized below by research question.
Figure 1.
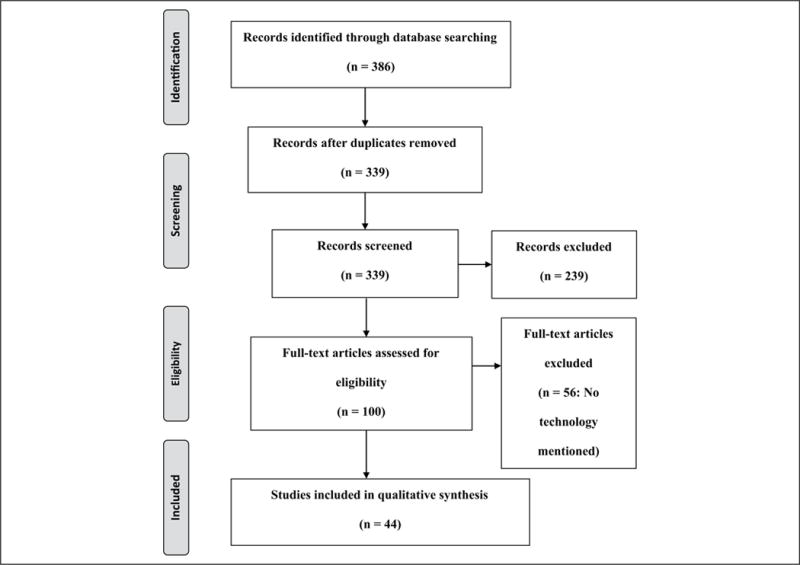
Study selection process.
What Kinds of Technology Have Been Used to Facilitate RT?
Supplemental Table 1 (available online at heb.sagepub.com/supplemental) summarizes the media types, content, and technologies used. Multiple papers describing evaluations of a single system are grouped together. Media content ranged from generic content to personal photographs; the predominant media type was music. Other content types were based on the era or region in which the individual with dementia grew up or were based on personal interest. The studies varied greatly in the degree of detail they reported, especially in regard to the specific technology used. Some were specific in reporting technology details (i.e., brands of monitors used), while others did not mention any details about what ICT was used. Diverse types of technology were used, from technology that monitored brainwaves to identify evocative media to technology that analyzed conversations through natural language processing. However, the predominant use was to play multimedia prompts.
Ten papers in this review reported the use of a technological component in a “reminiscence kit,” a portable selection of nontechnological triggers, such as old toys, smells, maps, and food, and technological triggers, such as slides or records. Some studies used kits available commercially (e.g., Bi Folkal kit; http://www.bifolkal.org/products.html), while others used reminiscence kits developed by the researchers. Audio was reported as a component of all identified reminiscence kits; 8 of the 10 identified reminiscence kits mentioned music. Namazi and Haynes (1994) used a tape recorder to play sounds to accompany paper photographs. The use of video (L.-J. Lin, Li, & Tabourne, 2011; Moss, Polignano, White, Minichiello, & Sunderland, 2002) and slides (Moss et al., 2002; Thorgrimsen, Schweitzer, & Orrell, 2002) were also reported. As it was impossible to evaluate the impact of technology components as opposed to the other kit components, the results of these papers are not discussed further in this review.
Eight papers, corresponding to five distinct projects, described systems that utilize ICT for RT but did not report any evaluation with the target population. These papers have been classified as “system architectures.” The projects used diverse types of technology: to deliver RT remotely (Hamada, Kuwahara, Morimoto, & Yasuda, 2009; Hattori, Kuwabara, Kuwahara, Abe, & Yasuda, 2007; Kuwahara, Yasuda, Abe, & Kuwabara, 2006), to capture and display daily activities (Kikhia, Bengtsson, Synnes, & Sani, 2010; Kikhia, Hallberg, Bengtsson, Sävenstedt, & Synnes, 2010), to play multimedia (Caprani, Dwyer, Harrison, & Brien, 2005), to monitor brainwaves of an individual during RT (Gary, 2012), and to present conversation facilitator prompts through the use of natural language processing (Green, Guinn, & Smith, 2012). These papers are not described in Table 1 as they do not report evaluation with the target population. However, they are discussed in the remainder of the paper as the novel uses of technology they propose are relevant to the study.
Table 1.
Study Details.
| Reference | Study design | N | Age (M) | Dementia severity | Country | Study aims | Technology-related findings |
|---|---|---|---|---|---|---|---|
| CIRCA (Alm et al., 2003, 2005) | Case control | 30 (18 PWDs, 12 CGs) | 81.9 | MMSE 2–23 (M = 15.4) | United Kingdom | Participation, engagement, and enjoyment; how the two compare, effectiveness of prototype | With CIRCA, improved enjoyment, participation (more equal footing), stronger and prolonged engagement |
| Alm, Astell, et al. (2004) | Case report | 12 (6 PWDs, 6 CGs) | 74.3 | MMSE 10–25 (M = 15.6) | United Kingdom | Assess reaction to system and identify usability issues | All participants enjoyed using system. Staff especially liked choice of material and system’s positive effect on how much PWDs spoke. FMs liked videos and system ease of use. Staff found system valuable for selves and PWDs but wished for more variety. |
| Alm, Astell, et al. (2004) | Case report | 18 (9 PWDs, 9 staff) | 83 | MMSE 8–22 (M = 16) | United Kingdom | How does system affect interest and involvement of PWDs and enjoyment of CGs? | All PWDs enjoyed using system. Participants wished there were personal materials. Touch screen easy to use. |
| Alm et al. (2007) | Case report | NS | NS | “People with dementia” | United Kingdom | Acceptability, reactions to different interfaces | Digital RT does not have to mimic scrapbook. Videos appreciated only when they triggered specific memories (photos and music appreciated regardless). System idea acceptable. |
| Astell, Ellis, Bernardi, et al. (2010) | Case report | 22 (11 PWDs, 11 staff) | 83.5 | MMSE 9–23 (M = 15.9) | United Kingdom | Effect on relationship between CGs and PWDs | Improved interactions when using CIRCA |
| Astell, Ellis, Alm, Dye, & Gowans (2010) | Case control | 20 (10 PWDs) | Group A, 82.8; Group B, 72 | Group A, MMSE 9–25 (M = 20.4); Group B, MMSE 12–24 (M = 16.8) | United Kingdom | How do what and how much PWDs say change based on whether they are viewing personal or generic photos? | Generic prompted more conversation, personal more labeling (which limited the amount of information PWDs produced) |
| Bass & Greger (1996) | Case report | 12 (6 PWDs) | 68.5 | 6 rated “confused” by nursing staff | United States | Does the addition of music as an additional stimulus during RT decrease depression? | No advantage in addition of music reported |
| Benveniste, Jouvelot, & Renaud (2010) | Case report | 9 | NS | MMSE 10–25 (M = NS) | France | Usability, what people liked and did not like about the system | Users felt empowered during use and enjoyed recollections spurred by music. Based on results, researchers focus on RT. |
| Boulay, Benveniste, Boespflug, Jouvelot, & Rigaud (2011) | Case report | 7 | 88.5 | MMSE 12–22 (M = 16.7) | France | Usability, whether PWDs were able to learn to use system, whether they found it satisfying to use | System usable and satisfying. Three participants showed significant learning. |
| Cohene (2005) | Case report | 1 PWD and family | NS | “Midstage AD” | Canada | To determine whether and how PWD reacts to life stories, to gather material to tell life story, to explore ways to support system interactions | PWD enjoyed using system and needed less prompting with time. |
| Glynn (1992) | Case report | 20 | 84 | All rated “severe” on GDS | United States | Interrater reliability of instrument, responses to different music genres (including nostalgic music to prompt reminiscence) | Acceptable interrater reliability. Low spontaneous (2.5%) or prompted (50%) reminiscing to nostalgic music. |
| Kuwahara, Abe, Yasuda, & Kuwabara (2006), Study 1 | Case control | 7 (5 PWDs) | 84.6 | Mean Hasegawa score = 8.8 (1 mild, 1 moderate, 3 severe) | Japan | Experience using system, usefulness, usability | All but one subject were able to concentrate during sessions. RT content improved remote reminiscence. |
| Kuwahara, Abe, et al. (2006), Study 2 | Case report | 9 | 77 | MMSE 10–25 (M = 19) | Japan | How does use of videophone compare with in-person RT in PWD’s time to respond and eagerness? | Videophone acceptable (no significant difference in terms of eagerness or time to respond) |
| NR (Kuwahara, Yasuda, Tetsutani, & Morimoto, 2010; Yasuda, Kuwahara, & Morimoto, 2009) | Case report | 4 | 79 | MMSE 16–27 (M = 22) | Japan | Effect on “psychological stability” (measures from GBS, such as anxiety and restlessness), caretaker observations | NR was effective for two PWDs, with persistent effects for one. CGs reported that system caused anxiety (n = 3) and enjoyment (n = 2) |
| Lee & Dey (2008) | Case report | 6 (3 PWDs, 3 CGs) | NS | Early stage of AD | United States | Usability, whether system supported interaction | CGs enjoyed using system but uncertain about selecting cues for PWDs. PWDs able to use system. More details recalled with system than with CGs using photos. |
| Piasek, Irving, & Smeaton (2012) | Case report | 2 (1 PWD, 1 CG) | 87 | Early stage of dementia | Ireland | Effect of viewing SenseCam photos on PWD’s sense of self, interactions with CG, and conversations | No change in psychosocial measures. Did not promote positive interactions between PWD and CG but led to richer conversation with therapist. Source of pictures confused PWD. |
| Sarne-Fleischmann, Tractinsky, Dwolatzky, & Rief (2011) | Case report | 3 | NS | AD diagnosis | Israel | Usability | Some visual components needed to be changed to reduce distraction and confusion. |
| Shik, Yue, & Tang (2009) | Case report | NS | NS | “Mild dementia” | Hong Kong | How to design and deliver a reminiscence intervention to Chinese older adults in Hong Kong | No results specific to technology |
| Smith, Crete-Nishihata, Damianakis, Baecker, & Marziali (2009) | Case report | 12 (6 PWDs) | 85 | Stage of (AD) dementia: early (2), mid (3), advanced (1) | Canada | Feasibility of producing personalized multimedia biography videos with people demonstrating cognitive impairments | Project was feasible, but time CGs must invest might be a barrier for some. Music highly appreciated. Videos for PWDs required FM involvement, so they may miss on benefits of seIf-reflection and self-esteem improvements that came with contributing to the project that occurred for other participants. |
| Tolson & Schofield (2012) | Cohort Study | NS | NS | “Men with dementia” | United Kingdom | What can be learned by analyzing four separate case studies using context, mechanism, and outcome? | No results specific to technology |
| Wallace, Thieme, Wood, Schofield, & Olivier (2012) | Case report | NS | NS | Clients with psychiatric disorders (predominantly dementia) | United Kingdom | Staffs experiences using piece are designed to evoke reminiscence with PWD | Piece used for several purposes, including individual reminiscence, relaxation, and to assess a PWD’s memory and life history |
| Wallace et al. (2013) | Case report | 2 (1 PWD, 1 CG) | “Early 60s” | “Early stage dementia” | United Kingdom | How to use design probes to empathically engage a PWD and CG in designing digital jewelry to support personhood | The design process helped the researchers understand how it was to live with dementia and codesign meaningful jewelry for the PWD. |
| Yamagami, Oosawa, Ito, & Yamaguchi (2007) | Case report | 22 (14 PWDs) | 82.2 | CDR = .5 (2), 1 (9), 2 (3) | Japan | To examine the effectiveness of activity reminiscence therapy | No results specific to technology |
| Yasuda, Kuwabara, Kuwahara, Abe, & Tetsutani (2009) | Case report | 15 | 77.3 | MMSE 0–23 (M = 14) | Whether personalized videos get more attention than generic TV shows | More concentration during personalized videos, especially for moderate and severe dementia | |
| Yasuda, Kuwahara, Kuwabara, Morimoto, & Tetsutani (2013) | Case report | 4 | 78.8 | MMSE 14–29 (M = 19.5) | Japan | Effect on “psychological stability” and caretaker observations | NR effective for 1 participant with effects persisting for 3 hr. Three CGs reported that that PWD enjoyed using system. |
Note. Multiple papers describing a single study are grouped. AD = Alzheimer’s disease; CDR= clinical dementia rating; CG = caregiver; CIRCA = Computer Interactive Reminiscence and Conversation Aid; FM = family member; GBS = Gottfried-Brane-Steen Scale; GDS = Global Deterioration Scale for Assessment of Primary Degenerative Dementia; MMSE = Mini-Mental State Examination; NR = networked reminiscence therapy; NS = not specified; PWD = person with dementia.
All the studies except for reminiscence kits and system architectures are reported in Table 1. Almost all of the studies were case reports, signifying the early state of research in this area. Due to study heterogeneity, meta-analysis of results was not possible.
Outcomes were diverse and included usability, acceptability, interactions between people with dementia and caregivers or staff, and concentration and distraction while using the system. Few studies looked at health outcomes, such as impact on mood and cognition, or a comprehensive evaluation of wellness or engagement, also signifying the early state of the research.
What Purpose Did the Technology Serve?
Below are the purposes of using the various technologies identified through the systematic review.
Accommodating for Deficits: Using Technology to Ease Participation
Mitigate motor and sensory impairments
Aging is often accompanied by changes in psychomotor performance and dexterity due to slower response time, tremor, or arthritis. The presence of dementia, more often seen in older adults, further compounds these changes as motor impairments become an issue, particularly in later stages. In several studies, technology was used to accommodate motor impairments with the input devices users with dementia used to interact with the system. Technology was used to aid interaction through commercially available gaming devices, touch screens, and prototype devices.
The MINWii videogame (Benveniste, Jouvelot, & Renaud, 2010; Boulay, Benveniste, Boespflug, Jouvelot, & Rigaud, 2011) employed a Wii remote as an input device to accommodate motor impairments of users who might not otherwise be able to play the game. The research team also incorporated computational filtering to accommodate tremors or imprecision by filtering input from the Wii remote and adjusting the output to make their reminiscence game easier for users by “smoothing” their movements.
Several of the projects used a touch screen interface to allow people with dementia to manipulate the reminiscence materials. One example is the Computer Interactive Reminiscence and Conversation Aid (CIRCA) group (Alm et al., 2003, 2005, 2007; Astell, Ellis, Bernardi, et al., 2010; Gowans et al., 2004), who found that the touch screen interface encouraged users with dementia to use the system themselves with little prompting. Cohene, Baecker, and Marziali (2005) explored the design of several prototype input devices meant to be simple and familiar for the user with dementia, such as page turning and a single button control.
Various input devices have different trade-offs. A touch screen, as opposed to a Wii remote, combines navigation and content on one interface, which affects the distance the user must be from a screen and consequently the number of people who can gather around the system. Novel, custom-made devices, such as those discussed by Cohene et al. (2005), might be more suitable to the particular cognitive and motor needs of individuals with dementia but are not yet commercially available.
In addition to motor impairments, sensory impairments, such as vision and hearing loss, may accompany aging. Shik, Yue, and Tang (2009) used headphones and amplifiers to accommodate hearing impairments and projectors to magnify photographs to accommodate vision impairments. Using technology in this manner allowed participants who might otherwise be excluded to engage in RT with the rest of the group.
Compensate for memory deficits
As memory is both impaired by dementia and necessary for reminiscence, it is important for systems to support individuals with dementia in remembering. Many of the projects used materials from the past to prompt remembering and reminiscence. Two projects gathered materials from the users’ daily activities using technology, such as GPS, cameras, and audio recorders, to compensate for memory deficits during reminiscence (Kikhia, Bengtsson, et al., 2010; Kikhia, Hallberg, et al., 2010; Lee & Dey, 2008). The motivation for one design was to alleviate caregiver strain originating from repeatedly providing details to help someone with dementia recall facts about events during casual reminiscence (Lee & Dey, 2008). Yamagami, Oosawa, Ito, and Yamaguchi (2007) used a video at the beginning of the session to remind participants how to use tools from their past. The participants then showed staff how to use these tools, reversing the roles of staff as helper and resident as helper. By using a video instead of having staff instruct the residents, this role reversal was possible.
Taking Advantage of Continuing Abilities: Using Technology to Harness Strengths
The other side of accommodating impairments is taking advantage of abilities. Certain skills, such as sensory awareness, musical responsiveness, and emotional memory, have been labeled “continuing abilities” in dementia, as they are thought to persist after others have been compromised by the disease (Lawton & Rubinstein, 2000). Sensory awareness is the response to various forms of stimuli (e.g., visual, audio, tactile). Musical responsiveness refers to the strong responses people with dementia can have to music. Emotional memory refers to the ability of people to experience rich emotions. Below are detailed some of the systems that used technology to draw on these continuing abilities.
Sensory awareness and musical responsiveness
Technology is commonly used to display movies, photographs, and audio. Many of the projects, particularly those using reminiscence kits, used technology solely for this purpose. Media were used as triggers to prompt a positive response in the form of interactions or improved mood. Almost all of the studies in this review used technology to display or play media.
One consideration in creating multimedia reminiscence materials is the degree of stimulation desired. In general, it seemed that researchers shared the philosophy of “the more, the better.” For example, one group used photographs, background music, narration, panning, and zooming in its reminiscence video slideshows (Yasuda, Kuwabara, Kuwahara, Abe, & Tetsutani, 2009).
Emotional memory
Projects that focused on this ability mainly appealed to something personally relevant to the individual. This ranged from materials that were personal only in that they were from the general era in which one grew up to artifacts related to individual interests (e.g., football reminiscence groups; Tolson & Schofield, 2012). At the other end of the spectrum were projects that used materials that belonged to an individual, usually gathered from family members. One project personalized not only materials but also the reminiscence delivery platform, basing the design of interactive jewelry (e.g., digital photo-displaying locket) on the values and interests of a woman with dementia and her husband (Wallace et al., 2013).
The benefits of using personalized versus generic materials were issues explored in two studies with differing conclusions. One study found that generic photographs prompted more storytelling from individuals with dementia (Astell, Ellis, Alm, Dye, & Gowans, 2010) and noted the potential for emotional distress when a person with dementia fails to recognize himself or herself or others in personal photographs (Gowans et al., 2004). Another study found that people showed more interest and less distraction while viewing personalized photo-videos than while viewing TV shows (Yasuda, Kuwabara, et al., 2009). One explanation for the disparity in findings is that the first group of researchers had people with dementia involved in conversation, possibly resulting in the person with dementia struggling to remember specific details about pictures from his or her past. The second study took place with a person with dementia alone in a room viewing photo-videos. By not requiring the participants to generate conversation with another party, the researchers might have enabled the participants to enjoy the personalized photo-videos. Another explanation is that the different findings are due to the higher score on the Mini-Mental State Examination (MMSE) of participants in the first study, possibly leading to more awareness of their difficulty in recalling information and subsequent discomfort.
A potential area of discomfort that may arise from RT is the reaction to disturbing photographs, such as wartime photographs or of deceased loved ones. Smith, Crete-Nishihata, Damianakis, Baecker, and Marziali (2009) recommend basing decisions of whether to include images or videos of relatives who had passed away on the wishes of participants and their families as well as their reactions to that type of media.
Easing the Burden of Therapy Delivery
RT can be time-intensive and costly in terms of preparation and delivery. One issue is gathering the materials for therapy, which may clearly be a barrier when personal materials are needed but also when desired materials may be hard to find due to their rarity. Technology can also bridge geographic distance and address transportation barriers. Listed below are systems that used technology to facilitate therapy delivery.
Gathering personal materials
A potential area for technology to aid in the delivery of RT is in allowing the digital transfer of materials for RT to the therapist. Sarne-Fleischmann, Tractinsky, Dwolatzky, and Rief (2011) built a back end into a website-hosted reminiscence intervention that allowed family members to upload personal material to be viewed by their relative with dementia. Piasek, Irving, and Smeaton (2012) had a person with early-stage dementia wear the Microsoft SenseCam, a device that takes photographs at intervals. A therapist then used the photographs during RT. The authors found that the individual was not able to remember that he had been wearing the SenseCam and was confused about where the pictures had come from but was able to engage in richer conversation than without the photographs as prompts.
Gathering generic materials
Digital archives can make a large body of uncommon materials available for session leaders in disparate locations. The football reminiscence project (Tolson & Schofield, 2012) consisted of four interventions in different locations that used digitized images from a historic football picture database for RT with older males with dementia. Giving therapists access to the archives allowed them to accommodate interests of participants.
Remote therapy
Like other therapies, a downside of RT is that either the individual with dementia or the therapist must travel to be in the same location. One approach that has become popular with telehealth is the use of technology to bridge geographic distance when delivering care. The set of papers dealing with networked reminiscence therapy describes a system focused on the delivery of therapy from afar. The system is designed to allow a caretaker or therapist to view videos and photos with an individual in another location. Both parties can indicate regions of interest, and the therapist or caretaker can control the visual effects that accompany the reminiscence videos. Evaluations of this system have found that most individuals find remote RT enjoyable, and some have had persisting benefits in terms of managing behavioral symptoms, such as anxiety, irritability, and restlessness (Kuwahara, Yasuda, Tetsutani, & Morimoto, 2010; Yasuda, Kuwahara, Kuwabara, Morimoto, & Tetsutani, 2013; Yasuda, Kuwahara, & Morimoto, 2009). While remote RT could reduce barriers due to transportation difficulties, they may create new barriers for individuals lacking technical expertise or necessary hardware. The researchers involved in networked reminiscence therapy addressed this concern by setting up the system in the participants’ homes and remotely starting applications (Yasuda et al., 2013).
Tailoring
Some of the systems used technology so that a single device or system could work for different people. One way systems did this was by providing individuals with their own log-in. Sarne-Fleischmann et al. (2011) accomplished this through selection on the touch screen. USB sticks were another method of tailoring, with the MINWii study recommending that each individual have a USB stick with his or her configurations and scores (Benveniste et al., 2010). Two other papers proposed using USB sticks to store personal reminiscence materials, such as photographs, for use with a shared television (Wallace, Thieme, Wood, Schofield, & Olivier, 2012) and a shared laptop (Caprani et al., 2005). USB sticks can prevent requiring someone to memorize a password. However, remembering to carry around the USB device could be an issue for cognitively impaired individuals or overwhelmed staff. In addition to separate log-ins, a second way the systems identified promoted tailoring to diverse interests was by having a large collection of materials organized in ways accessible to users with cognitive impairments. This arrangement might allow individuals with dementia to take more ownership over the topic of conversation than a physical set of materials brought in by a therapist. Gowans et al. (2004) reported surprise at the level of initiative taken by the individuals with dementia to operate their system and, as a result, made some ergonomic design modifications since the system had originally been designed for caregivers to operate. A third way material was tailored was through automatically detecting reactions of users to reminiscence content using commercially available brainwave sensors (Gary, 2012). This may be an effective method when people with dementia are unable to express their preferences.
Evaluating Progress and Use
Technology can be used to track and monitor progress and system use. Boulay et al. (2011) used logging to report on the speed with which people with dementia learned to use their game and mentioned the capability for therapists to log in and assess client progress as a favorable aspect of the system (Benveniste et al., 2010). The interactive wall display project kept track of the number of interactions through radio-frequency identification technology (Wallace et al., 2012). Information on progress and system use can be built into many ICT platforms and may be useful to health professionals to adjust interventions and also facility administrators to determine which interventions are being used. However, monitoring progress may require individual log-ins or accounts, which might not be feasible due to privacy issues involved in using shared machines.
Discussion
This review is limited in several ways. First, while three comprehensive and primarily nonoverlapping databases were used, papers may have been published in other databases not used in this review. Additionally, due to publication bias, only papers describing positive results may make up the majority of the published papers.
This paper systematically reviewed studies of the use of ICT for RT interventions. It answered questions such as the types of available studies, what technologies were used, and why they were used to facilitate RT. The answers to these questions can help guide facilities and therapists in deciding whether and how to incorporate ICT into RT and can aid researchers in deciding what elements to incorporate into future designs. The body of evidence for ICT RT interventions is limited by small sample sizes, limited description of the RT method used, and lack of details on how outcomes varied by level of dementia. These factors, as well as the high variability in technologies used and diverse aims, make a quantitative determination of how different aspects of technology contribute to the delivery of RT difficult. To move the field forward, larger studies are needed to determine whether these systems have a positive effect on people with dementia. Studies rarely described how RT was administered or whether therapists had any training. Future studies should be more descriptive in how RT is delivered. Another issue is that results were rarely separated by dementia severity, despite the differences in people across the spectrum of disease. If researchers include individuals at different stages of dementia, they should separate results by stage or specify if there is no difference.
Despite their limitations, the papers included in this review yield some rich insights on benefits and challenges of using ICT during RT. Challenges include that many of the systems described in the study require technical expertise for setup or operation and may not be ready for independent use by family caregivers. Benefits include the enjoyment derived by people with dementia from viewing reminiscing materials through various forms of multimedia, such as video and audio, and that these individuals can benefit from ICT-supported RT by having increased opportunities for interactions and greater ability to take ownership of the conversation. Additionally, ICT can aid reminiscence and activity therapists by reducing session preparation time, making available materials possible for a therapist to find on his or her own, and providing opportunities for remote sessions to reach distant clients.
Supplementary Material
Acknowledgments
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Science Foundation Graduate Research Fellowship [Grant DGE-1256082] and the National Library of Medicine Biomedical and Health Informatics Training Grant Program [Grant 2T15LM007442].
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Additional supporting information is available at heb.sagepub.com/supplemental.
Supplement Issue Note
This article is part of an open access supplement “Fostering Engagement and Independence: Opportunities and Challenges for an Aging Society,” published in SOPHE’s Health Education & Behavior. This supplement was supported by funding provided by the Centers for Disease Control and Prevention’s (CDC) National Center for Chronic Disease Prevention and Health Promotion, Healthy Aging Program (Cooperative Agreement #U38HM000454) via the Association of State and Territorial Health Officials, and from a grant provided by the Retirement Research Foundation. Views presented herein do not represent the official views of the CDC.
References
- Alm N, Astell A, Ellis M, Dye R, Gowans G, Campbell J. A cognitive prosthesis and communication support for people with dementia. Neuropsychological Rehabilitation. 2004;14(1/2):117–134. doi: 10.1080/09602010343000147. [DOI] [Google Scholar]
- Alm N, Dye R, Astell A, Ellis M, Gowans G, Campbell J. Making software accessible to people with severe memory deficits. In: Gibson L, Gregor P, Sloan D, editors. Proceedings of the 2005 International Conference on Accessible Design in the Digital World (Accessible Design ‘05) Swinton, UK: British Computer Society; 2005. p. 16. [Google Scholar]
- Alm N, Dye R, Gowans G, Campbell J, Astell A, Ellis M. Proceedings of the 2003 Conference on Universal Usability (CUU ‘03) New York, NY: ACM Press; 2003. Designing an interface usable by people with dementia; pp. 156–157. [DOI] [Google Scholar]
- Alm N, Dye R, Gowans G, Campbell J, Astell A, Ellis M. A communication support system for older people with dementia. Computer. 2007;40(5):35–41. doi: 10.1109/MC.2007.153. [DOI] [Google Scholar]
- Astell AJ, Ellis MP, Alm N, Dye R, Gowans G. Stimulating people with dementia to reminisce using personal and generic photographs. International Journal of Computers in Healthcare. 2010;1(2):177–198. [Google Scholar]
- Astell AJ, Ellis MP, Bernardi L, Alm N, Dye R, Gowans G, Campbell J. Using a touch screen computer to support relationships between people with dementia and caregivers. Interacting With Computers. 2010;22(4):267–275. doi: 10.1016/j.intcom.2010.03.003. [DOI] [Google Scholar]
- Azcurra DJLS. A reminiscence program intervention to improve the quality of life of long-term care residents with Alzheimer’s disease: A randomized controlled trial. Revista Brasileira de Psiquiatria. 2012;34(4):422–433. doi: 10.1016/j.rbp.2012.05.008. [DOI] [PubMed] [Google Scholar]
- Bass BA, Greger LM. Stimulus complexity in reminiscence therapy and scores on the beck depression inventory of a small group of nursing-home residents. Perceptual and Motor Skills. 1996;82(3, Pt. 1):973–974. doi: 10.2466/pms.1996.82.3.973. [DOI] [PubMed] [Google Scholar]
- Benveniste S, Jouvelot P, Renaud P. The MINWii Project: Renarcissization of patients suffering from Alzheimer’s disease through video game-based music therapy. In: Yang HS, Malaka R, Hoshino J, Han JH, editors. Proceedings on the 9th International Conference on Entertainment Computing (ICEC ‘10) Berlin, Germany: Springer-Verlag; 2010. pp. 79–90. [Google Scholar]
- Bird TD, Miller BL. Alzheimer’s disease and other dementias. In: Hauser S, Josephson S, editors. Harrison’s neurology in clinical medicine. 2nd. New York, NY: McGraw-Hill Professional; 2010. pp. 298–319. [Google Scholar]
- Boulay M, Benveniste S, Boespflug S, Jouvelot P, Rigaud A-S. A pilot usability study of MINWii, a music therapy game for demented patients. Technology and Health Care: Official Journal of the European Society for Engineering and Medicine. 2011;19(4):233–246. doi: 10.3233/THC-2011-0628. [DOI] [PubMed] [Google Scholar]
- Butler R. The life review: An interpretation of reminiscence in the aged. Psychiatry. 1963;26:65–76. doi: 10.1080/00332747.1963.11023339. [DOI] [PubMed] [Google Scholar]
- Caprani N, Dwyer N, Harrison K, Brien KO. CHI ’05 extended abstracts on human factors in computing systems (CHI EA ’05) New York, NY: ACM Press; 2005. Remember when: Development of an Interactive reminiscence device; pp. 2070–2073. [DOI] [Google Scholar]
- Cohene T, Baecker R, Marziali E. CHI ’05 extended abstracts on human factors in computing systems (CHI EA ’05) New York, NY: ACM Press; 2005. Designing interactive life story multimedia for a family affected by Alzheimer’s disease; pp. 1300–1303. [DOI] [Google Scholar]
- Cotelli M, Manenti R, Zanetti O. Reminiscence therapy in dementia: A review. Maturitas. 2012;72(3):203–205. doi: 10.1016/j.maturitas.2012.04.008. [DOI] [PubMed] [Google Scholar]
- Crispi EL, Heitner G. An activity-based intervention for caregivers and residents with dementia in nursing homes. Activities, Adaptation and Aging. 2002;26(4):61–72. [Google Scholar]
- Douglas S, James I, Ballard C. Non-pharmacological interventions in dementia. Advances in Psychiatric Treatment. 2004;10:171–177. doi: 10.1192/apt.10.3.171. [DOI] [Google Scholar]
- Gary L. Proceedings of the 6th International Conference on Rehabilitation Engineering and Assistive Technology (i-Create ‘12) Singapore: Singapore Therapeutic, Assistive and Rehabilitative Technologies (START) Centre; 2012. Improving reminiscence therapy through active brainwave analysis; pp. 1–3. Article No. 27. [Google Scholar]
- Gibson F. What can reminiscence contribute to people with dementia? In: Bornat J, editor. Reminiscence reviewed: Persceptives, evaluations, achievements. Milton Keynes, UK: Open University Press; 1994. pp. 46–60. [Google Scholar]
- Gibson F. The past in the present: Using reminiscence in health and social care. Baltimore, Baltimore, MD: Health Professions Press; 2004. [Google Scholar]
- Glynn NJ. The music therapy assessment tool in Alzheimer’s patients. Journal of Gerontological Nursing. 1992;18(1):3–9. doi: 10.3928/0098-9134-19920101-03. [DOI] [PubMed] [Google Scholar]
- Gowans G, Campbell J, Alm N, Dye R, Astell A, Ellis M. CHI ’04 extended abstracts on human factors in computing systems (CHI EA ’04) New York, NY: ACM Press; 2004. Designing a multimedia conversation aid for reminiscence therapy in dementia care environments; pp. 825–836. [DOI] [Google Scholar]
- Green NL, Guinn C, Smith RW. Proceedings of the Third Workshop on Speech and Language Processing for Assistive Technologies (SLPAT ’12) Stroudsburg, PA: Association for Computational Linguistics; 2012. Assisting social conversation between persons with Alzheimer’s disease and their conversational partners; pp. 37–46. [Google Scholar]
- Hamada T, Kuwahara N, Morimoto K, Yasuda K. Preliminary study on remote assistance for people with dementia at home by using multi-media contents. In: Stephanidis C, editor. Proceedings of the 5th International Conference on Universal Access in Human-Computer Interaction: Addressing Diversity Part I: Held as Part of HCI International 2009 (UAHCI ‘09) Berlin, Germany: Springer-Verlag; 2009. pp. 236–244. [DOI] [Google Scholar]
- Hattori F, Kuwabara K, Kuwahara N, Abe S, Yasuda K. Proceedings of the 6th IEEE International Conference on Cognitive Informatics (COGINF ‘07) Washington, DC: IEEE Computer Society; 2007. Socialware for people with disabilities; pp. 321–326. [DOI] [Google Scholar]
- Hurd MD, Martorell P, Delavande A, Mullen KJ, Langa KM. Monetary costs of dementia in the United States. New England Journal of Medicine. 2013;368(14):1326–1334. doi: 10.1056/NEJMsa1204629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kikhia B, Bengtsson JE, Synnes K, Sani H. Creating digital life stories through activity recognition with image filtering. In: Lee Y, Bien ZZ, Mokhtari M, Kim JT, Park M, Kim J, Khalil I, editors. Proceedings of the Aging Friendly Technology for Health and Independence, and 8th International Conference on Smart Homes and Health Telematics (ICOST ’10) Berlin, Germany: Springer-Verlag; 2010. pp. 203–210. [Google Scholar]
- Kikhia B, Hallberg J, Bengtsson JE, Sävenstedt S, Synnes K. Building digital life stories for memory support. International Journal of Computers in Healthcare. 2010;1(2):161–176. [Google Scholar]
- Kuwahara N, Abe S, Yasuda K, Kuwabara K. Proceedings of the 8th International ACM SIGACCESS Conference on Computers and Accessibility (Assets ‘06) New York, NY: ACM Press; 2006. Networked reminiscence therapy for individuals with dementia by using photo and video sharing; p. 125. [DOI] [Google Scholar]
- Kuwahara N, Yasuda K, Abe S, Kuwabara K. Networked interactive photo annotation and reminiscence content delivery. In: Mizoguchi R, Shi Z, Giunchiglia F, editors. Proceedings of the First Asian Conference on the Semantic Web (ASWC ‘06) Berlin, Germany: Springer-Verlag; 2006. pp. 762–767. [DOI] [Google Scholar]
- Kuwahara N, Yasuda K, Tetsutani N, Morimoto K. Remote assistance for people with dementia at home using reminiscence systems and a schedule prompter. International Journal of Computers in Healthcare. 2010;1(2):126–143. [Google Scholar]
- Lawton MP, Rubinstein RL, editors. Interventions in dementia care: Towards improving quality of life. New York, NY: Springer; 2000. [Google Scholar]
- Lee ML, Dey AK. Proceedings of the 2nd International Workshop on Systems and Networking Support for Health Care and Assisted Living Environments (HealthNet ’08) New York, NY: ACM Press; 2008. Using lifelogging to support recollection for people with episodic memory impairment and their caregivers. [DOI] [Google Scholar]
- Lin L-J, Li K-Y, Tabourne CES. Impact of the life review program on elders with dementia: a preliminary study at a day care center in southern Taiwan. Journal of Nursing Research. 2011;19(3):199–209. doi: 10.1097/JNR.0b013e318228ced3. [DOI] [PubMed] [Google Scholar]
- Lin Y-C, Dai Y-T, Hwang S-L. The effect of reminiscence on the elderly population: A systematic review. Public Health Nursing. 1994;20(4):297–306. doi: 10.1046/j.1525-1446.2003.20407.x. [DOI] [PubMed] [Google Scholar]
- Moss SE, Polignano E, White C, Minichiello M, Sunderland T. Reminiscence group activities and discourse interaction in Alzheimer’s disease. Journal of Gerontological Nursing. 2002;8:36–44. doi: 10.3928/0098-9134-20020801-09. [DOI] [PubMed] [Google Scholar]
- Namazi K, Haynes S. Sensory stimuli reminiscence for patients with Alzheimer’s disease: Relevance and implications. Clinical Gerontologist. 1994;14(4):29–46. [Google Scholar]
- National Institute for Health and Clinical Excellence. NICE clinical guideline 42: Dementia. Supporting people with dementia and their carers in health and social care. London, UK: Author; 2006. [Google Scholar]
- Parker J. “I remember that …”: Reminiscence groups with people with dementia. A valuable site for practice learning. Groupwork. 2006;16(1):7–28. [Google Scholar]
- Piasek P, Irving K, Smeaton AF. Case study in SenseCam use as an intervention technology for early-stage dementia. International Journal of Computers in Healthcare. 2012;1(4):304–319. [Google Scholar]
- Politis AM, Vozzella S, Mayer LS, Onyike CU, Baker AS, Lyketsos CG. A randomized, controlled, clinical trial of activity therapy for apathy in patients with dementia residing in long-term care. International Journal of Geriatric Psychiatry. 2004;19(11):1087–1094. doi: 10.1002/gps.1215. [DOI] [PubMed] [Google Scholar]
- Sarne-Fleischmann V, Tractinsky N. Development and evaluation of a personalised multimedia system for reminiscence therapy in Alzheimer’s patients. International Journal of Social and Humanistic Computing. 2008;1(1):81–96. doi: 10.1504/IJSHC.2008.020482. [DOI] [Google Scholar]
- Sarne-Fleischmann V, Tractinsky N, Dwolatzky T, Rief I. Proceedings of the 4th International Conference on Pervasive Technologies Related to Assistive Environments (PETRA ’11) New York, NY: ACM Press; 2011. Personalized reminiscence therapy for patients with Alzheimer’s disease using a computerized system. [DOI] [Google Scholar]
- Shik AW, Yue JS-C, Tang K. Life is beautiful: Using reminiscence groups to promote well-being among Chinese older people with mild dementia. Groupwork. 2009;19(2):8–27. [Google Scholar]
- Smith KL, Crete-Nishihata M, Damianakis T, Baecker RM, Marziali E. Multimedia biographies: A Reminiscence and social stimulus tool for persons with cognitive impairment. Journal of Technology in Human Services. 2009;27(4):287–306. doi: 10.1080/15228830903329831. [DOI] [Google Scholar]
- Su T-W, Wu L-L, Lin C-P. The prevalence of dementia and depression in Taiwanese institutionalized leprosy patients, and the effectiveness evaluation of reminiscence therapy: A longitudinal, single-blind, randomized control study. International Journal of Geriatric Psychiatry. 2012;27(2):187–196. doi: 10.1002/gps.2707. [DOI] [PubMed] [Google Scholar]
- Subramaniam P, Woods B. Towards the therapeutic use of information and communication technology in reminiscence work for people with dementia: A systematic review. International Journal of Computers in Healthcare. 2010;1(2):106–125. [Google Scholar]
- Subramaniam P, Woods B. The impact of individual reminiscence therapy for people with dementia: systematic review. Expert Review of Neurotherapeutics. 2012;12(5):545–555. doi: 10.1586/ern.12.35. [DOI] [PubMed] [Google Scholar]
- Thorgrimsen L, Schweitzer P, Orrell M. Evaluating reminiscence for people with dementia: A pilot study. The Arts in Psychotherapy. 2002;29:93–97. [Google Scholar]
- Tolson D, Schofield I. Football reminiscence for men with dementia: Lessons from a realistic evaluation. Nursing Inquiry. 2012;19(1):63–70. doi: 10.1111/j.1440-1800.2011.00581.x. [DOI] [PubMed] [Google Scholar]
- Wallace J, Thieme A, Wood G, Schofield G, Olivier P. Proceedings of the 2012 ACM Annual Conference on Human Factors in Computing Systems (CHI ’12) New York, NY: ACM Press.; 2012. Enabling self, intimacy and a sense of home in dementia: An enquiry into design in a hospital setting; pp. 2629–2638. [DOI] [Google Scholar]
- Wallace J, Wright PC, McCarthy J, Green DP, Thomas J, Olivier P. Proceedings of the SIGCHI Conference on Human Factors in Computing Systems (CHI ’13) New York, NY: ACM Press; 2013. A design-led inquiry into personhood in dementia; pp. 2617–2626. [DOI] [Google Scholar]
- Wang J-J. Group reminiscence therapy for cognitive and affective function of demented elderly in Taiwan. International Journal of Geriatric Psychiatry. 2007;22:1235–1240. doi: 10.1002/gps.1821. [DOI] [PubMed] [Google Scholar]
- Wang JJ-, Yen M, OuYang W-C. Group reminiscence intervention in Taiwanese elders with dementia. Archives of Gerontology and Geriatrics. 2009;49:227–232. doi: 10.1016/j.archger.2008.08.007. [DOI] [PubMed] [Google Scholar]
- Woods B, Spector AE, Jones CA, Orrell M, Davies SP. Reminiscence therapy for dementia. Cochrane Database of Systematic Reviews, 1. 2009 doi: 10.1002/14651858.CD001120.pub2. [DOI] [PubMed] [Google Scholar]
- Yamagami T, Oosawa M, Ito S, Yamaguchi H. Effect of activity reminiscence therapy as brain-activating rehabilitation for elderly people with and without dementia. Psychogeriatrics. 2007;7(2):69–75. doi: 10.1111/j.1479-8301.2007.00189.x. [DOI] [Google Scholar]
- Yasuda K, Kuwabara K, Kuwahara N, Abe S, Tetsutani N. Effectiveness of personalised reminiscence photo videos for individuals with dementia. Neuropsychological Rehabilitation. 2009;19(4):603–619. doi: 10.1080/09602010802586216. [DOI] [PubMed] [Google Scholar]
- Yasuda K, Kuwahara N, Kuwabara K, Morimoto K, Tetsutani N. Daily assistance for individuals with dementia via videophone. American Journal of Alzheimer’s Disease and Other Dementias. 2013;28(5):508–516. doi: 10.1177/1533317513494440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yasuda K, Kuwahara N, Morimoto K. Proceedings of the 5th International Conference on Universal Access in Human-Computer Interaction: Addressing Diversity Part I: Held as Part of HCI International 2009 (UAHCI ‘09) San Diego, CA: Springer-Verlag; 2009. Remote reminiscence talking and scheduling prompter for individuals with dementia using video phone; pp. 429–438. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.