

Abstract
Background
Physical activity is of benefit for primary prevention of cardiovascular diseases, but it appears to increase the risk for atrial fibrillation. We aimed to study a cohort of patients following a first stroke in individuals with previous high physical activity, compare them to the general population with respect to recurrent stroke and death, and relate these to atrial fibrillation.
Methods and Results
From the participants of the Vasaloppet, the world's largest ski‐race, and matched individuals from the general population (n=708 604), we identified 5964 patients hospitalized with a first‐time stroke between 1994 and 2010. Individuals with severe diseases were excluded. One half percent of skiers and 1% of nonskiers were hospitalized due to stroke. The incidence rate was 8.3 per 100 person‐years among skiers and 11.1 among nonskiers. The hazard ratio (HR) for recurrent stroke or death between the 2 groups was 0.76 (95% CI 0.67 to 0.86). The result was consistent in subgroups. The HR for death was 0.66 (95% CI 0.56 to 0.78) and for recurrent stroke 0.82 (95% CI 0.70 to 0.96). After adjustment for smoking and socioeconomic factors, the HR for death was consistent at 0.70 (95% CI 0.56 to 0.87) while the HR for recurrent stroke was not statistically significant. Outcomes for skiers with atrial fibrillation tended to show a lower risk than for nonskiers.
Conclusions
This large cohort study supports the hypothesis that patients with a stroke and with prior regular physical activity have a lower risk of death, while their risk for recurrent stroke is similar to that of nonskiers. The skiers had a higher incidence of atrial fibrillation, but still no increased risk of recurring stroke.
Keywords: atrial fibrillation, cerebrovascular disease, cross‐country skiing, epidemiology, lifestyle, physical activity, prevention, recurrent stroke, sports medicine, Sweden, Vasaloppet
Introduction
Higher physical activity together with a healthy lifestyle have been shown to reduce the risk for cardiovascular diseases including stroke,1, 2 while recent studies report that long‐term endurance sports practice is associated with an increased risk of atrial fibrillation (AF).3, 4, 5 It is generally believed that embolic ischemic stroke associated with AF is more severe and more often fatal, and survivors are left more disabled than patients with other causes of stroke.6
The Vasaloppet is the largest cross‐county ski race in the world. The race recruits both elite and recreational skiers. Among these skiers, a faster finishing time and a high number of completed races are associated with a future higher incidence of AF5 that may theoretically increase the risk for embolic stroke. Yet, in contrast, the participants in the Vasaloppet have a substantially lower mortality rate compared with the general population.7 There is a seemingly contradictory relationship between a high level off physical activity and risk of cardiovascular disease. Physically active and fit individuals appear to be protected against atherosclerotic artery disease8 but at the same time have a higher risk of volume and pressure overload in their left atrium, leading to an increased risk for AF,3, 4 which may cause cardioembolic stroke.
We hypothesized that patients with a high level of physical activity prior to suffering stroke may have a lower risk of death, recurrent stroke, and myocardial infarction despite a higher incidence of AF. We also investigated whether these patients with a high level of physical activity suffer a less severe stroke with more favorable outcomes after stroke recurrence. Among patients with a high level of physical activity, we wanted to investigate whether there is a dose–response relationship between fitness and outcomes.
Methods
The Vasaloppet Register and the Swedish Stroke Register
The Vasaloppet is a long‐distance cross‐country ski race with various distances that takes place over 1 week annually in Sweden. From 1989 to 2010, 126 362 males (62%) and 77 447 females (38%) participated in at least 1 of the races. The majority (55%) of the skiers participated in the classic 90‐km race and the rest in the 30‐ or 45‐km races. The Vasaloppet Register has information about year and distance for each race, name, Swedish personal identification number, address, number of races, and finish time, which is also presented as a percentage of the winner's time.
Participants in the Vasaloppet over the age of 19 were included in our cohort and were denoted as skiers (n=203 809 unique individuals). Each skier frequently participated in several races (on average 2.5 races per skier). Men and women from the general population in Sweden were randomly selected from the Total Population Register and frequency‐matched to the skiers by age (5‐year categories), sex, county of residence, and year of the ski race. They were denoted as nonskiers. Individuals with prior history of stroke were excluded from the cohort. We additionally excluded skiers and nonskiers with a history of severe disease8 who therefore were unlikely to have been able to participate in the race. This exclusion list included chronic neurological, cardiovascular, psychiatric, and cancer diseases. The number of selected nonskiers was n=504 795. These nonskiers together with the skiers constitute the Vasaloppet cohort with a total number of 708 604 participants (Figure 1).
Figure 1.
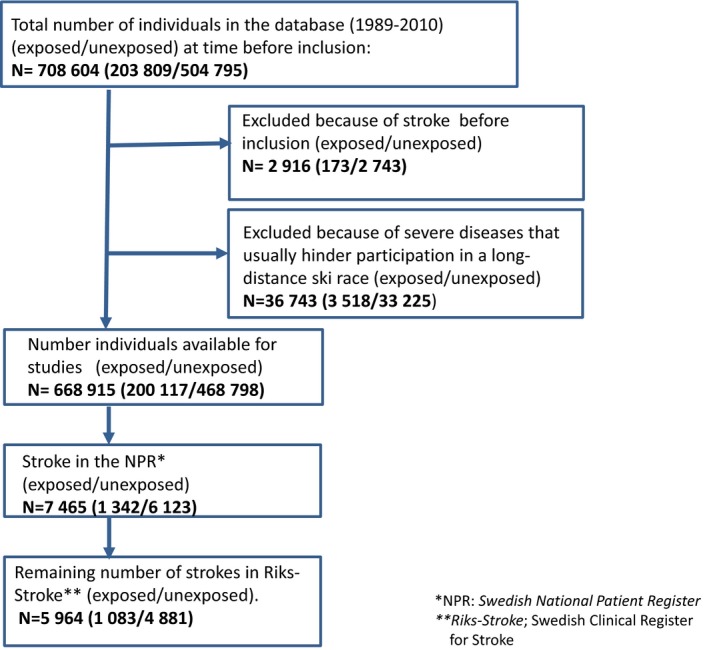
Flowchart describing the total number of individuals in Vasaloppet cohort before and after exclusions. From those avalible for studies the number of first stroke is shown.
The Swedish Stroke Register is a national clinical quality register for stroke care and was initiated in 1994. Since 1994, it has retrieved data from all Swedish hospitals admitting patients with acute stroke.9 The Swedish Stroke Register identifies the stroke hospitalizations and provides data on cardiovascular risk factors (such as AF, hypertension, diabetes, previous stroke, and smoking), level of consciousness on admission, living conditions, activities of daily living (ADL), and data on drug therapy both on admission and at discharge. The estimated coverage of acute stroke events in the Swedish Stroke Register varied during the study period between 80% and up to 96%.9
Study Population
We know from a published survey10 and other studies published about the Vasaloppet cohort5, 7, 8, 10, 11 that the long‐distance skiers as a group have a healthier lifestyle, including less smoking, a diet of more fruits and vegetables, less obesity, and a higher level of physical activity compared with the general population. For example, 60% of skiers practice physical training more than 4 hours per week, while 17% of the general population were exercising for up to 1.5 hours per week. Information about all skiers between 1989 and 2010 was available in the Vasaloppet Registry.
From the Vasaloppet cohort, we identified patients with an index of stroke and recurrent stroke events, both ischemic and hemorrhagic, in the Swedish Stroke Register from 1994 on. This resulted in a study population of 1083 skiers and 4881 nonskiers with a first‐time stroke.
Other Registers
By using the individual personal identification numbers provided to all Swedish citizens, we were able to link information from the Vasaloppet cohort with information retrieved from several different nationwide registers. Beginning in 1964, the Swedish National Patient Register (NPR) has included dates of admission and discharge, as well as primary and secondary diagnoses. The registry has been complete since 1987.12 The Causes of Death Register (CDR), established in 1961, contains the date and underlying cause of death as well as contributing causes. Statistics Sweden contains socioeconomic data for all Swedish citizens, including information about education, occupation, and civil status.
Variables and Outcome
Data on previous stroke, AF, hypertension, diabetes mellitus, and medications were retrieved from the National Patient Register and the Swedish Stroke Register. Information about activities of daily living (ADL), quality of life, and smoking were obtained from the Swedish Stroke Register, and all other comorbidities from the National Patient Register.
The Charlson comorbidity index was calculated to compare degree of comorbidity between the groups.13 The main outcome was death and recurrent stroke. The secondary outcome was myocardial infarction and combinations of the outcome events (Table 1).
Table 1.
Events (Incidence Rates) and Unadjusted and Adjusted HR With Corresponding 95% CI
| Nonskiers Events (%/pya) | Skiers Events (%/pya) | HR [95% CI] | Adj HRb [95% CI] | Adj HRc [95% CI] | |
|---|---|---|---|---|---|
| Death | 1089 (5.8) | 163 (3.8) | 0.66 [0.56, 0.78] | 0.71 [0.57, 0.88] | 0.70 [0.56, 0.87] |
| Death/re‐stroke | 1744 (11.1) | 303 (8.3) | 0.76 [0.67, 0.86] | 0.86 [0.74, 1.00] | 0.88 [0.75, 1.03] |
| Death/re‐stroke/MI | 1825 (11.9) | 323 (9.0) | 0.77 [0.69, 0.87] | 0.88 [0.76, 1.02] | 0.91 [0.78, 1.05] |
| Re‐stroke | 941 (6.0) | 177 (4.8) | 0.82 [0.70, 0.96] | 0.96 [0.79, 1.17] | 1.02 [0.84, 1.24] |
| MI | 261 (1.4) | 203 (1.0) | 0.69 [0.50, 0.96] | 0.74 [0.47, 1.15] | 0.85 [0.54, 1.33] |
| Re‐stroke/MI | 1086 (7.1) | 177 (5.6) | 0.81 [0.70, 0.94] | 0.95 [0.79, 1.14] | 1.02 [0.85, 1.23] |
Analysis is based on 4614 cases with nonmissing data. CI indicates confidence interval; HR, indicates hazard ratios; MI, myocardial infarction; nonskiers, population‐based controls with the same age, sex, and same county of residence; Re‐stroke, recurrent stroke; skiers, the participants in the Vasaloppet.
Incidence rate per 100 person‐years.
Adjusted for age, sex, education, family and occupation status, and smoking.
Adjusted for age, sex, education, family and occupation status, smoking, hypertension, and diabetes.
Statistical Analyses
The subjects were followed from the diagnosis of stroke either to the date of an event or end of follow‐up (December 31, 2010), maximum 10 years with median 2.3 years. Incidence rates were estimated as the number of events divided by the total follow‐up time. For the analysis of recurrent stroke, we also performed a competing risk analysis, with death as a competing risk, leading to materially unaltered results. We therefore decided to present the results from the simpler Cox‐regression model.
Cox regression models were used to compare the event‐free survival probability between those exposed to the Vasaloppet (skiers), and those not exposed (nonskiers). The proportional hazard assumptions were confirmed graphically. We used the directed acyclic graph approach14 to select suitable covariates for the multivariable model.
The model included age (continuous), race year (1994–2000, 2001–2005, 2006–2010), sex, smoking habits (never, ex‐smoker, current), education (primary school, high school, university), family (single), and occupational status (employed, unemployed, retired). Since hypertension and diabetes mellitus may be considered as confounding factors or in fact part of the lifestyle we are studying, we therefore reported the results in models with and without these factors (Table 1). We did not include type of discharge medication in the primary model as we regard these as a consequential part of the stroke. AF was registered on admission, which made it possible to perform stratified analyses by AF status. Finally, we included data on the ADL situation, health assessment, and discharge medication to attempt to estimate the severity of the stroke for skiers and nonskiers. All analyses were done using the R environment for statistical computing (version 3.0).15
The institutional Review Board (The Ethics Committees) at Uppsala University (Uppsala Dnr 2010/305, 2012/067 and Stockholm Dnr 2011/030) approved this Registry study under a waiver of informed consent. The approval included merging databases after anonymizing the data.
Results
Baseline data for the first stroke in the study population of 1083 skiers and 4881 nonskiers is shown for both groups in Table 2. Age and sex were similar by design. Eighty‐three percent were men and the median age at the time of the stroke was 64. Skiers had a higher educational level, reported less smoking, and had AF more often. Nonskiers had diabetes and hypertension more often. Drugs on admission to the hospital and at follow‐up are shown in Tables 2 and 3. The discharge and follow‐up frequencies are shown in Table 3. Nonskiers experienced worse health and more depression, had worse ADL functions, and were taking more pharmaceutical agents for the prevention of cardiovascular diseases. However, warfarin was prescribed more frequently to the skiers and this group also had more AF.
Table 2.
Baseline Characteristics
| Na | Nonskiers N=4881 | Skiers N=1083 | P Valueb | |
|---|---|---|---|---|
| Male | 5964 | 4062 (83.2) | 888 (82.0 | 0.331 |
| Age | 5964 | 64.0 (24.0 to 99.0) | 64.0 (25.0 to 96.0) | 0.202 |
| Smokers | 4689 | 1066 (27.8) | 61 (7.2) | <0.00111 |
| Education level | 5911 | <0.0011 | ||
| Primary school | 1962 (40.6) | 249 (23.0) | ||
| High school | 2019 (41.8) | 429 (39.7) | ||
| University | 849 (17.6) | 403 (37.3) | ||
| Occupation level | 5962 | <0.0011 | ||
| Unemployed | 1102 (22.6) | 102 (9.4) | ||
| Employed | 2209 (45.3) | 591 (54.6) | ||
| Retired | 1568 (32.1) | 390 (36.0) | ||
| Family status: single | 6964 | 2033 (41.7) | 325 (30.0) | <0.0011 |
| Living alone | 5912 | 1522 (31.4) | 228 (21.3) | <0.0011 |
| Mobility without assistance | 5930 | 4705 (97.0) | 1057 (98.1) | 0.0921 |
| Dressing: need help | 5922 | 125 (2.6) | 137 (2.3) | 0.0041 |
| Level of consciousness | 5903 | 0.211 | ||
| RLS 1 | 4218 (87.2) | 952 (89.3) | ||
| RLS 2 to 3 | 383 (7.9) | 68 (6.4) | ||
| RLS 4 to 8 | 150 (3.1) | 26 (2.4) | ||
| Charlson index: 1+ | 5964 | 1477 (30.3) | 267 (24.7) | <0.0011 |
| Atrial fibrillationc | 5658 | 679 (14.7) | 212 (20.4) | <0.00111 |
| Race time p% | ||||
| 100 to 150; m age 63 (33 to 92) | 22 (20.2) | |||
| 151 to 200; m age 65 (30 to 93) | 88 (24.9) | |||
| >200; m age 63 (25 to 96) | 65 (15.2) | |||
| Diabetesc | 5274 | 947 (21.9) | 63 (6.7) | <0.00111 |
| Hypertensionc | 5357 | 3633 (60.0) | 446 (45.9) | <0.00111 |
| Admission treatments | ||||
| Aspirin | 5117 | 1014 (24.2) | 203 (21.8) | 0.1111 |
| Clopidogrel | 4219 | 72 (2.1) | 12 (1.5) | 0.2811 |
| Aspirin+clopidogrel | 4222 | 31 (0.9) | 6 (0.8) | 0.6811 |
| Dipyridamole | 4221 | 35 (1.0) | 13 (1.6) | 0.1411 |
| Warfarin | 5113 | 171 (4.1) | 34 (3.7) | 0.5411 |
| Calcium antagonists | 4205 | 467 (13.7) | 68 (8.6) | <0.00111 |
| ACE‐inhibitors | 2844 | 427 (18.5) | 84 (18.8) | 0.1511 |
| Angiotensin II‐blockers | 2843 | 232 (10.0) | 37 (7.0) | 0.02811 |
| Diuretics | 4206 | 533 (15.6) | 72 (9.1) | <0.0011 |
| Statins | 4206 | 676 (19.8) | 119 (15.0) | 0.00211 |
Numbers represent frequencies with percentages in parentheses (age represents the median and range). Note that the denominator is different between variables due to partial missing of data. ACE indicates angiotensin‐converting enzyme; m age, median age and range in parentheses; Nonskiers, population‐based controls with the same age, sex, and same county of residence; Race time p%, race time as a percentage of the winner's time; RLS, reaction‐level scale; Skiers, the participants in the Vasaloppet.
Number of nonmissing observations.
Pearson χ2 test1 or Wilcoxon‐Mann–Whitney test2.
Information from the Swedish Stroke Register and from Swedish National Patient Register (NPR).
Table 3.
Discharge/Follow‐Up Characteristics
| Na | Nonskiers N=4881 | Skiers N=1083 | P Valueb | |
|---|---|---|---|---|
| Severity of stroke | ||||
| Mobility | 5231 | <0.001 | ||
| Deceased | 351 (8.3) | 73 (7.5) | ||
| No assistance | 3271 (76.9) | 819 (83.8) | ||
| With assistance indoors | 310 (7.3) | 44 (4.5) | ||
| With assistancec | 322 (7.6) | 41 (4.2) | ||
| Need assistance for toilet visits | 4812 | 385 (9.9) | 51 (5.6) | <0.001 |
| Dressing with assistance | 4809 | 470 (12.0) | 67 (7.4) | <0.001 |
| Dependent | 4066 | 0.001 | ||
| Partially | 1132 (34.3) | 229 (29.9) | ||
| Totally | 292 (8.9) | 49 (6.4) | ||
| Speaking problems | 2356 | 512 (27.1) | 111 (23.8) | 0.15 |
| Depressive mode | 4028 | <0.001 | ||
| Almost never | 1438 (44.1) | 418 (54.4) | ||
| Sometimes | 1477 (43.3) | 306 (39.8) | ||
| General health | 3983 | <0.001 | ||
| Poor | 67 (2.1) | 9 (1.2) | ||
| Bad | 427 (13.2) | 48 (6.3) | ||
| Good | 2181 (67.6) | 499 (65.8) | ||
| Very good | 550 (17.1) | 202 (26.6) | ||
| Smoking | 3474 | 398 (14.2) | 24 (3.5) | <0.001 |
| Discharge/follow‐up treatments | ||||
| Hypertension treatment | 3394 | 1989 (72.8) | 383 (57.9) | <0.001 |
| Warfarin | 5003 | 411 (10.0) | 132 (14.5) | <0.001 |
| Thrombolysis | 5137 | 192 (4.6) | 60 (6.4) | 0.017 |
| Calcium antagonists | 4127 | 467 (23.2) | 130 (16.8) | <0.001 |
| ACE‐inhibitors | 2767 | 931 (41.3) | 182 (35.4) | <0.014 |
| Angiotensin II‐blockers | 2766 | 263 (11.7) | 42 (8.2) | <0.022 |
| Diuretics | 4127 | 740 (22.1) | 118 (15.2) | <0.001 |
| Statins | 4127 | 1958 (58.4) | 438 (56.5) | 0.33 |
| Aspirin | 5015 | 2611 (63.6) | 554 (60.9) | 0.13 |
| Clopidogrel | 4128 | 213 (6.4) | 48 (6.2) | 0.87 |
| Aspirin+clopidogrel | 4131 | 136 (4.1) | 36 (4.6) | 0.46 |
| Dipyridamole | 4138 | 491 (14.6) | 103 (13.3) | 0.33 |
Numbers represent frequencies with percentages in parentheses. Note that the denominator is different between variables due to partial missing of data. ACE indicates angiotensin‐converting enzyme; Nonskiers, population‐based controls with the same age, sex, and same county of residence; Skiers, the participants in the Vasaloppet.
Number of nonmissing observations.
Pearson χ2 test.
From 2001.
The total number of all‐cause deaths or recurrent stroke rate was 2047. The incidence rate was 8.3 per 100 person‐years among skiers and 11.1 among nonskiers. The unadjusted HR for recurrent stroke or death between skiers and nonskiers was 0.76 (95% CI: 0.67 to 0.86). The result was consistent in subgroups (Figure 2). After adjustment for smoking and socioeconomic factors, the HR for primary outcomes was 0.86 (95% CI: 0.74 to 1.00). The HR for death was 0.70 (95% CI: 0.56 to 0.87) while the HR for recurrent stroke was 0.96 (95% CI: 0.79 to 1.17) and not statistically significant (Table 1).
Figure 2.
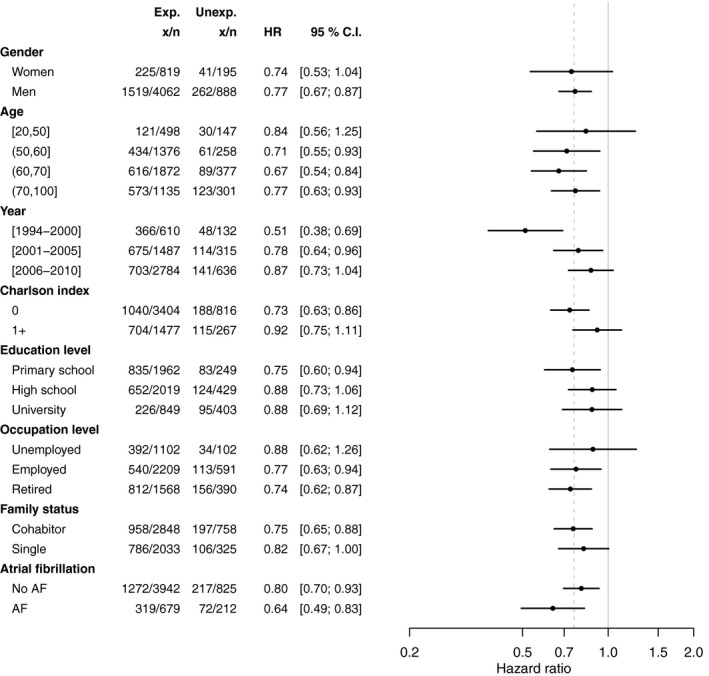
Relative hazard of stroke or all‐cause mortality with corresponding 95% CI for skiers compared with nonskiers in different subgroups. The vertical dashed line indicates the unadjusted HR (0.76). AF indicates atrial fibrillation; CI, confidence interval; Exp, Eexposed; HR, hazard ratio; Unexp, Unexposed; x/n actual number out of the cohort.
Atrial Fibrillation (AF)
AF at the first stroke was more common among skiers compared with nonskiers, 20.4% and 14.7%, respectively (Table 2). However, skiers still had a lower incidence rate of recurrent stroke compared with the age‐matched nonskiers, 4.8% and 6%, respectively (Table 1). The incidence rates for death or recurring stroke, as well as for a combination of these, were all higher for subjects with AF compared with those without AF. This was the case for both skiers and nonskiers (Figure 3).
Figure 3.
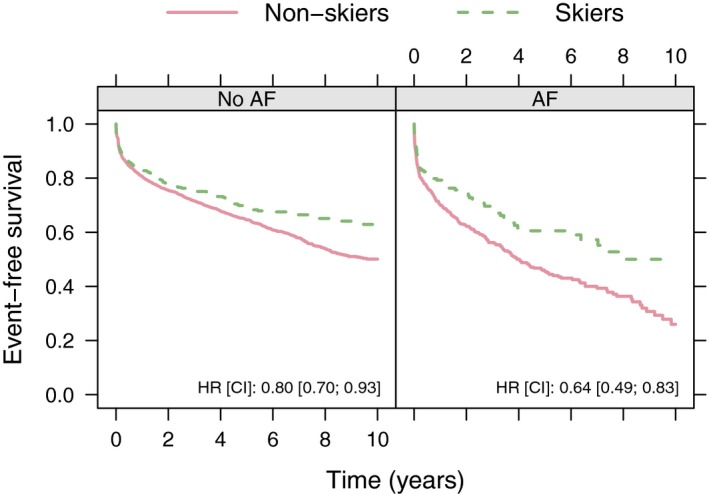
Stroke‐free survival with unadjusted hazard ratios (HR) and corresponding 95% CI for subjects (skiers and nonskiers) with and without atrial fibrillation (AF). Skiers: Participants in the Vasaloppet. Nonskiers: population‐based controls with the same age, sex, and same county of residence. CI indicate confidence interval.
Dose–Response
Among the skiers, we also studied the dose–response relationship with the finish time in relation to the winner's time, as a proxy measure of physical fitness and training intensity in a separate model shown in Figure 4. Overall there was an association showing a lower risk for death and recurrent stroke for skiers with better performance. However, there appeared to be a sex difference with a more obvious association between race time and outcome for women.
Figure 4.
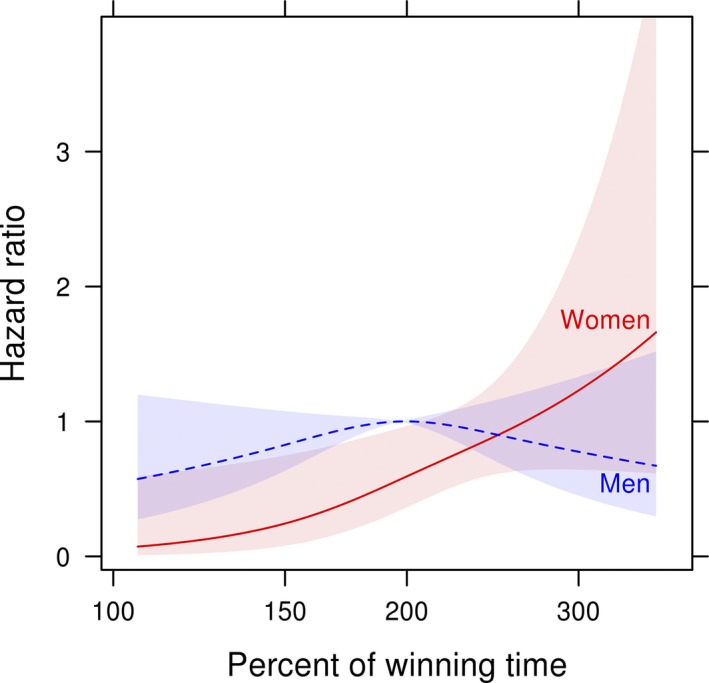
Estimated risk of death or stroke vs race time adjusted for age. The overall median relative race time (197%) and male sex is set as the reference. Comparison of skiers with different performance levels (finish times) is shown. Note the log scale.
Discussion
Principal Findings
The main finding is that stroke patients who had been physically active, as evidenced by their participation in a long‐distance cross‐country ski race, were associated after adjustment with a 29% relative risk reduction of all‐cause death and no significant risk difference for recurrent stroke compared with less physically active stroke patients (nonskiers) despite a higher prevalence of AF. Skiers poststroke had better ADL functions, were less depressed, less help dependent, rated their health higher, and used fewer medications (Table 3). Skiers had AF more often and consequently used more warfarin. The effectiveness of anti–vitamin K treatment and compliance is generally very high in Sweden. There is likely no difference between skiers and nonskiers.16 After adjustment for confounders such as socioeconomic data and smoking, the association remained essentially unchanged for death but the risk for recurrent stroke was similar for skiers and nonskiers. Interestingly, there appeared to be a dose–response relationship, suggesting that among individual skiers those with shorter race times had a lower risk for death and recurrent stroke compared with skiers with longer race times. This relationship was more pronounced in women (Figure 4).
Comparison With the Literature
This study supports the results of previous studies suggesting that physically fit or active people have a lower incidence of first stroke and all‐cause of death.2, 7 We found no prior reports regarding the benefits of physical activity prior to a stroke in relation to the risk of suffering a recurrent stroke, nor are we aware of studies reporting that individuals with a high level of physical activity suffer a less severe stroke than those less physically active. Our finding that 15% of stroke events are due to AF is similar to the estimates from a previous study.17
Potential Mechanisms
A healthy lifestyle including physical activity has recently been shown to reduce stroke.18 Thus, in the present study, it is difficult to discern the individual contribution of physical activity and physical fitness on these associations. It has previously been shown that physical fitness has a stronger relationship to a reduced risk for cerebrovascular disease than physical activity,19 but both physical fitness and physical activity are independent risk factors for cardiovascular disease. Regarding fitness, the maximum oxygen uptake (VO2‐max) for the skiing population is between 45 and 80 mL·kg−1·min−1 compared with the general population's VO2‐max of 35 mL·kg−1·min−1.20 Besides this higher fitness level, the Vasaloppet skiers are also physically more active than the general population. From questionnaires we know that a large part of them (60%) exercise for at least 4 hours weekly.10 This corresponds approximately to a mean value of about 20 MET‐h·week−1 (metabolic equivalent hours per week). The skiers have a healthy lifestyle in common; they have a higher education and are likely motivated to be physically active. The level of physical activity, for the majority at least 20 MET‐h weekly, may lead to a protective effect against developing atherosclerosis. It has been shown that cardiorespiratory fitness and physical activity have significantly different relationships to cardiovascular risk. The risks of coronary heart disease or cardiovascular disease decrease linearly in association with increasing physical activity but the risk reduction is significantly greater for fitness than physical activity.19 No such dose–response associations were seen for the risk of recurrent myocardial infarction in a previous report based on the Vasaloppet cohort.8 In this stroke study, however, individuals with better fitness had the lowest risk of recurrent stroke or death. We know that various cardiovascular risk factors have a different impact on the various cardiovascular outcomes, and it is likely that the benefits of physical activity are also different. The potential mediating mechanisms for physical activity and lower risk for cardiovascular events have been studied in a large cohort study.21 Inflammatory, hemostatic biomarkers made the largest contribution to lower risk followed by blood pressure, lipids, body mass index, and hemoglobin A1c in diabetes.
One alternative explanation for the results is that the Vasaloppet skiers may have a genetic predisposition (ie, an inherited lower risk for cerebrovascular diseases).22 Our study was not designed to investigate potential explanations for these relationships.
In our cohort, the nonskiers had a 15% incidence of AF. The prevalence of AF as a risk factor for stroke has been highlighted in a study in which AF increased the risk of stroke 5‐fold and caused 15% of all strokes.23 There was a strong relationship between age and AF in stroke as shown in the Swedish Stroke Register, ranging from 10% in stroke patients below the age of 65 to 40% in those above 80 years of age.24
There is evidence from other publications that people who practice strenuous sports25 have a higher proportion of AF, just like our cohort. Thus, physically active people appear to suffer fewer strokes despite more AF. The explanation for this finding can only be speculated. There might be a lower incidence of concomitant diseases or structural cardiac changes, factors that reduce their risk for thromboembolic stroke. People with a high level of physical activity are likely to have a low CHADS2 (Congestive heart failure, Hypertension, age ≥75 years, Diabetes, previous Stroke)/CHA2DS2‐VASc (Vascular disease, age 65 to 74 years, sex category) score, with a low stroke risk. CHA2DS2‐VASc grade 0 in AF is associated with <1% annual risk for stroke.26 This background, in addition to a generally lower risk of cardiovascular events, may explain the trend in our study (Figure 3), namely, that skiers have fewer strokes than nonskiers, even if they have a higher frequency of AF.
Strengths and Limitations
Our study included a larger population of physically active people than most previous studies and a matched population not exposed to the long‐distance ski race, the Vasaloppet. This study was possible thanks to the individual personal identification number of each participant and the unique national registers in Sweden.
When comparing 2 different cohorts, there is an inherent risk of selection bias. To avoid this we excluded all patients in the cohort with known severe diseases. We thereby tried to compare the skiers with a “healthy” population.
We have defined stroke as 1 group: ischemic, hemorrhagic, and nonspecific stroke. The consequences for ischemic strokes may therefore be diluted.
We are unaware of the physical activity of each study participant among the skiers and nonskiers. Previous studies of the Vasaloppet skiers show that in addition to being active, cross‐country skiers are physically active and have a generally healthy lifestyle.10 We therefore cannot isolate the physical activity factor and sedentary time from factors related to a healthy lifestyle.
Conclusions
Among patients with a history of stroke, those with high physical activity and a healthy lifestyle have a lower incidence of all‐cause death but a similar incidence of recurrent stroke. The skiers had a higher frequency of atrial fibrillation, but despite this they seemed to suffer less severe stroke and had no increased risk of recurrent stroke. Our data suggest that a lifestyle with a higher level of physical activity may work as a protection against recurrent cardiovascular events and death, and may reduce the severity of such events. The underlying mechanisms of these observations remain to be established.
Sources of Funding
The Folksam Research Foundation, the Center for Clinical Research in Falun, the Uppsala‐Örebro Regional Research Foundation, the Uppsala County Association Against Heart and Vessel Diseases, and the Erik, Karin and Gösta Selanders Foundation, Uppsala.
Disclosures
None.
Acknowledgments
The authors thank the Vasaloppet organization and the staff handling the register: Benny Skog and Jompa Cervin. Thanks also to Elisabeth Ärnström for managing the register at Uppsala Clinical Researach Center and the steering committee of the Swedish Stroke Registry.
(J Am Heart Assoc. 2015;4:e002469 doi: 10.1161/JAHA.115.002469)
References
- 1. Jefferis BJ, Whincup PH, Papacosta O, Wannamethee SG. Protective effect of time spent walking on risk of stroke in older men. Stroke. 2014;45:194–199. [DOI] [PubMed] [Google Scholar]
- 2. Chiuve SE, Rexrode KM, Spiegelman D, Logroscino G, Manson JE, Rimm EB. Primary prevention of stroke by healthy lifestyle. Circulation. 2008;118:947–954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Mascia G, Perrotta L, Galanti G, Padeletti L. Atrial fibrillation in athletes. Int J Sports Med. 2013;34:379–384. [DOI] [PubMed] [Google Scholar]
- 4. Grimsmo J, Grundvold I, Maehlum S, Arnesen H. High prevalence of atrial fibrillation in long‐term endurance cross‐country skiers: echocardiographic findings and possible predictors—a 28‐30 years follow‐up study. Eur J Cardiovasc Prev Rehabil. 2010;17:100–105. [DOI] [PubMed] [Google Scholar]
- 5. Andersen K, Farahmand B, Ahlbom A, Held C, Ljunghall S, Michaëlsson K, Sundström J. Risk of arrhythmias in 52 755 long‐distance cross‐country skiers: a cohort study. Eur Heart J. 2013;34:3624–3631. [DOI] [PubMed] [Google Scholar]
- 6. Lin HJ, Wolf PA, Kelly‐Hayes M, Beiser AS, Kase CS, Benjamin EJ, D'Agostino RB. Stroke severity in atrial fibrillation. The Framingham Study. Stroke. 1996;27:1760–1764. [DOI] [PubMed] [Google Scholar]
- 7. Farahmand BY, Ahlbom A, Ekblom O, Ekblom B, Hållmarker U, Aronson D, Brobert GP. Mortality amongst participants in the Vasaloppet: a classical long‐distance ski race in Sweden. J Intern Med. 2003;253:276–283. [DOI] [PubMed] [Google Scholar]
- 8. Hållmarker U, Michaelsson K, Arnlov J, Hellberg D, Lagerqvist B, Lindback J, James S. Risk of recurrent ischaemic events after myocardial infarction in long‐distance ski race participants. Eur J Prev Cardiol. 2015; pii: 2047487315578664. doi: 10.1177/2047487315578664 [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- 9. Asplund K, Hulter Asberg K, Appelros P, Bjarne D, Eriksson M, Johansson A, Jonsson F, Norrving B, Stegmayr B, Terent A, Wallin S, Wester PO. The Riks‐Stroke story: building a sustainable national register for quality assessment of stroke care. Int J Stroke. 2011;6:99–108. [DOI] [PubMed] [Google Scholar]
- 10. Carlsson S, Olsson L, Farahmand BY, Hallmarker U, Ahlbom A. Skiers in the long‐distance ski race invest in their health. Läkartidningen. 2007;104:670–671. [PubMed] [Google Scholar]
- 11. Farahmand B, Hållmarker U, Brobert GP, Ahlbom A. Acute mortality during long‐distance ski races (Vasaloppet). Scand J Med Sci Sports. 2007;17:356–361. [DOI] [PubMed] [Google Scholar]
- 12. Ludvigsson JF, Andersson E, Ekbom A, Feychting M, Kim JL, Reuterwall C, Heurgren M, Olausson PO. External review and validation of the Swedish national inpatient register. BMC Public Health. 2011;11:450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–383. [DOI] [PubMed] [Google Scholar]
- 14. VanderWeele TJ, Hernan MA, Robins JM. Causal directed acyclic graphs and the direction of unmeasured confounding bias. Epidemiology. 2008;19:720–728. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Team RC . A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2013. Available at: http://www.R-project.Org/. Accessed April 30, 2015. [Google Scholar]
- 16. Sjögren V, Grzymala‐Lubanski B, Renlund H, Friberg L, Lip GYH, Svensson PJ, Själander A. Safety and efficacy of well managed warfarin. A report from the Swedish quality register Auricula. Thromb Haemost. 2015;113:1370–1377. [DOI] [PubMed] [Google Scholar]
- 17. Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, Singer DE. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the anticoagulation and risk factors in atrial fibrillation (ATRIA) study. JAMA. 2001;285:2370–2375. [DOI] [PubMed] [Google Scholar]
- 18. Larsson SC, Akesson A, Wolk A. Primary prevention of stroke by a healthy lifestyle in a high‐risk group. Neurology. 2015;84:2224–2228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Williams PT. Physical fitness and activity as separate heart disease risk factors: a meta‐analysis. Med Sci Sports Exerc. 2001;33:754–761. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Berg U, Forberg A. Cross‐country Ski Racing. Endurance in Sport. 2nd ed Haboken, NJ: John Wiley & Sons, Inc.; 2008:844–856. doi: 10.1002/9780470694930.ch57 [Google Scholar]
- 21. Mora S, Cook N, Buring JE, Ridker PM, Lee IM. Physical activity and reduced risk of cardiovascular events: potential mediating mechanisms. Circulation. 2007;116:2110–2118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Stubbe JH, Boomsma DI, Vink JM, Cornes BK, Martin NG, Skytthe A, Kyvik KO, Rose RJ, Kujala UM, Kaprio J, Harris JR, Pedersen NL, Hunkin J, Spector TD, de Geus EJ. Genetic influences on exercise participation in 37,051 twin pairs from seven countries. PLoS One. 2006;1:e22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Diep L, Kwagyan J, Kurantsin‐Mills J, Weir R, Jayam‐Trouth A. Association of physical activity level and stroke outcomes in men and women: a meta‐analysis. J Womens Health (Larchmt). 2010;19:1815–1822. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Åsberg S, Henriksson KM, Farahmand B, Asplund K, Norrving B, Appelros P, Stegmayr B, Asberg KH, Terent A. Ischemic stroke and secondary prevention in clinical practice: a cohort study of 14,529 patients in the Swedish Stroke Register. Stroke. 2010;41:1338–1342. [DOI] [PubMed] [Google Scholar]
- 25. Grimsmo J, Maehlum S, Moelstad P, Arnesen H. Mortality and cardiovascular morbidity among male long‐term endurance cross country skiers followed for 28–30 years. Scand J Med Sci Sports. 2011;21:e351–e358. [DOI] [PubMed] [Google Scholar]
- 26. Olesen JB, Lip GY, Hansen ML, Hansen PR, Tolstrup JS, Lindhardsen J, Selmer C, Ahlehoff O, Olsen AM, Gislason GH, Torp‐Pedersen C. Validation of risk stratification schemes for predicting stroke and thromboembolism in patients with atrial fibrillation: nationwide cohort study. Br Med J (Clin Res Ed). 2011;342:d124. [DOI] [PMC free article] [PubMed] [Google Scholar]