

Abstract
Introduction:
Periprosthetic fractures of the femur after total hip arthroplasty are increasing in frequency. In the polytraumatized patient with long-bone fracture, an ongoing debate exists regarding early definitive stabilization versus initial damage control orthopaedics, followed by delayed fixation. It remains to be seen whether this rationale applies to the polytraumatized patient with periprosthetic fracture.
Case presentation:
We present the case of a 73-years old Caucasian woman who sustained bilateral Gustillo-Anderson grade III open femur fractures; the fracture on the right was a Vancouver C open periprosthetic fracture after cemented total hip arthroplasty. After massive fluid resuscitation in the trauma bay she was taken to the intensive care unit in a hemodynamically unstable condition. She was subsequently operated and underwent early definitive fixation of both femurs with the rationale of potentially reducing pulmonary complications and promoting early mobilization.
Conclusion:
Early definitive stabilization versus delayed fixation in the polytraumatized patient with an open periprosthetic femur fracture is reviewed. Although several treatment algorithms based on fracture classification and implant stability exist, further study is required to delineate the preferred method and timeline of fixation for this growing cohort of patients.
Keywords: Periprosthetic fracture, open fracture, damage control orthopaedics
Introduction
Periprosthetic fracture of the femur after total hip arthroplasty is a relatively common and challenging complication. The incidence of these fractures is on the rise due to the increased use of total hip arthroplasty (THA), the aging population and complications such as osteolysis and aseptic loosening. Furthermore, with greater life expectancy, more number of people will have prosthetic implants for a longer period of time. Consequently, more patients are at risk for falls or high-energy trauma with subsequent periprosthetic fracture. In the polytraumatized patient with a longbone fracture, an ongoing debate exists in the literature regarding early definitive stabilization versus initial damage control orthopedics, followed by delayed fixatio. Although considerable attention has been placed on the management of the polytraumatized patient with femur fracture, we are not aware of any literature delineating the management of the polytraumatized patient with periprosthetic fracture.
We present the case of a 73-years old woman who sustained bilateral Gustillo-Anderson grade III open femur fractures. The fracture on the right was a Vancouver C open periprosthetic fracture after cemented THA done 8 years ago. After massive fluid resuscitation in the trauma bay for hypotension, anemia, and coagulopathy, she was taken to the intensive care unit in hemodynamically unstable condition. She was subsequently taken to the operating room and underwent early definitive fixation with a proximal femoral locking plate (Synthes) on the right, and a piriformis nail (Zimmer) on the left. Early definitive stabilization versus delayed fixation in the polytraumatized patient with a periprosthetic femur fracture is discussed.
Case Report
A 73-years old woman sustained bilateral open femur fractures after being run over by a commercial passenger bus. She had a previous well-functioning cemented total hip replacement on the right side performed 8 years ago. She had a past medical history of atrial fibrillation, polyarteritis nodosum, colostomy five years prior for small bowel obstruction, and chronic renal failure. The patient was intubated on scene and transferred to our Level 1 trauma centre for further stabilization. She sustained a PEA arrest on transfer and was resuscitated with epinephrine and atropine.
On arrival, she was hemodynamically unstable in the trauma bay; her injuries included bilateral lung contusions, multiple rib fractures, small left hemothorax, splenic laceration, stable pubic rami fractures, bilateral open femur fractures (Figs. 1&2), and massive degloving injuries with multiple open wounds throughout the lower extremity (Fig. 3). She was transfused 6 units of packed red blood cells (PRBCs) in the trauma bay and subsequently taken to the ICU for further stabilization.
Figure 1.

Radiograph of right periprosthetic femur fracture with large open wounds laterally, medially, and posterior
Figure 2.

Radiograph of left femoral shaft fracture with large open wounds laterally and posteriorly
Figure 3.

Photograph demonstrating extent of open wounds of lower extremity
She was brought to the operating room urgently (within 3 hours from time of arrival) and underwent irrigation and debridement of all open wounds and definitive fixation of her femur fractures. A 4.5 mm 12-hole LCP plate was used for the right open periprosthetic fracture (Fig. 4), and a 12 mm Zimmer piriformis nail was used for the left femur (Fig. 5). Preoperatively, the cement mantle was examined via radiographs and appeared intact, and this was confirmed intraoperatively. An intraoperative plastic surgery consult was undertaken due to severe injury to the soft tissues. Where possible, the soft tissues were primarily closed with sutures or staples, and dressed with Jelonet and soft roll if primary closure was not possible. By the end of the case the patient had received in total 12 units of PRBCs, 4 units of fresh frozen plasma (FFP), 1 unit of platelets, and 1 unit of cryoprecipitate; she was started on dobutamine for pressure support. She was taken to the ICU for further hemodynamic stabilization.
Figure 4a & 4b.
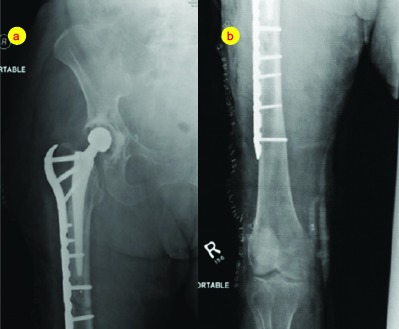
Immediate post-operative radiograph after open reduction internal fixation with proximal femoral locking plate of right periprosthetic fracture. Open wounds closed primarily with skin staples where possible
Figure 5a & 4b.
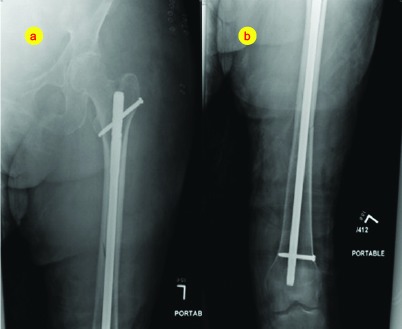
Immediate post-operative radiograph after piriformis nailing of left femur fracture.
She continued to remain unstable and a subsequent CT scan of her pelvis on post-operative day 1 showed active extravasation from her right obturator artery. She then underwent right obturator embolization via left femoral access by the interventional radiology service and was acutely stabilized. Over the ensuing few days in the ICU, she developed acute renal failure, acidemia, and disseminated intravascular coagulation (DIC). She was placed on continuous renal replacement therapy (CRRT). The patient continued to deteriorate in the ICU and eventually expired due to medical complications.
Discussion
Fractures of the femur are a morbid and potentially fatal injury, often occurring in the context of multiple traumatic injuries. The optimal timing of long-bone fracture fixation in the polytraumatized patient is controversial. Several studies have suggested that early stabilization of long-bone fractures, defined as fixation within 24 hours of admission is associated with reduced pulmonary complications, hospital stay and mortality. Other studies have suggested that early definitive fixation of longbone fractures, either with intramedullary nailing or plate osteosynthesis may have potentially deleterious effects in the acute setting, thereby increasing operative exposure and blood loss. The concept of damage control orthopedics (DCO) entails emergent temporary stabilization with an external fixator followed by definitive care with an intramedullary nail or plate when the patient is hemodynamically more stable. DCO is performed in coordination with acute resuscitation and hemodynamic stabilization, thus allowing fracture stabilization with minimal operative time and blood loss.
Although considerable attention has been placed on the management of the polytraumatized patient with a femur fracture, a notable lapse exists in the literature with regards to the polytraumatized patient with a periprosthetic fracture. The number of periprosthetic fractures is on the rise, with a reported incidence of approximately 1%. The 1-year mortality rate among those with a periprosthetic fracture is 11%, compared with 16.5% for a hip fracture and 2.9% in the primary arthroplasty group. Additionally, the treatment of periprosthetic femoral fractures requires particular care because secure fixation may be difficult and the instability of a femoral stem may affect the durability of the artificial joint. Such fractures often need definitive care by an arthroplasty surgeon where revision may be the treatment of choice. Although several classification systems for periprosthetic femoral fractures have been proposed, the Vancouver classification proposed by Duncan et al. (1995) has been universally accepted and shown to be valid and reliable. This classification subdivides periprosthetic femur fractures after hip arthroplasty into Type A (fracture of the greater or lesser trochanter), Type B (fracture around stem) and Type C (fracture below stem). Type B fractures are further divided into stable implant (Type B1), loose implant (Type B2) and loose implant and poor bone quality (Type B3). The majority of treatment algorithms advocate that conservative treatment is obsolete (exception is nondisplaced Type A fractures), revision arthroplasty should be performed in the case of a loose stem (Types B2 and B3), and open reduction internal fixation should be performed in case of a stable implant (Type B1 and Type C). The Vancouver classification system does not describe open periprosthetic injuries; due to the increasing numbers of these injuries, modification to include open or closed periprosthetic fractures may be warranted.
The patient described above presented in the polytrauma setting with a Vancouver C open periprosthetic fracture. We opted for early definitive fixation of her injuries to potentially reduce pulmonary complications, promote early mobilization and due to the fact that her open wounds allowed direct surgical access due to considerable soft tissue injury. The right femur was fractured distal to the cement plug and appeared to have an intact mantle surrounding the prosthesis. The wounds in the distal femur and tibia were so severe, skeletal traction was deemed to be an unacceptable option. Hence, a decision to place a proximal femoral locking plate directly through the wounds was made. This was applied rapidly with minimal additional dissection, and the soft tissues closed over the plate.
With two orthopaedic surgeons working at the same time, the left femur, also a Gustillo III C, was fixed definitively as well. The fracture was a simple transverse midshaft fracture, amenable to simple intramedullary nailing. The soft-tissue injuries in both lower extremities would have made skeletal traction in either case to be placed through open contaminated wounds. An external fixator from the iliac crest to the distal femur on the right leg was briefly discussed, but again deemed to be in the highly traumatized area of the femur.
Conclusions
The present case demonstrates the potential difficulty encountered in the decision-making algorithm of the polytraumatized patient with an open periprosthetic femur fracture. In this setting, we advocated for early definitive fixation. Although several treatment algorithms based on fracture classification and implant stability exist, further study is required to delineate the preferred method and timeline of fixation for this growing cohort of patients.
Clinical Message.
Periprosthetic fractures of the femur after total hip arthroplasty are increasing in frequency, and ongoing debate exists regarding early definitive stabilization versus initial damage control orthopaedics followed by delayed fixation. Early definitive stabilization versus delayed fixation in the polytraumatized patient with an open periprosthetic femur fracture is reviewed.
Biography


Footnotes
Conflict of Interest: Nil
Source of Support: None
References
- 1.Park SK, Kim YG, Kim SY. Treatment of periprosthetic femoral fractures in hip arthroplasty. Clin Orthop Surg. 2011;3(2):101–106. doi: 10.4055/cios.2011.3.2.101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Parvizi J, Vegari DN. Periprosthetic proximal femur fractures: current concepts. J Orthop Trauma. 2011;25(Suppl 2):77–81. doi: 10.1097/BOT.0b013e31821b8c3b. [DOI] [PubMed] [Google Scholar]
- 3.Pike J, Davidson D, Garbuz D, Duncan CP, O’Brien PJ, Masri BA. Principles of treatment for periprosthetic femoral shaft fractures around well-fixed total hip arthroplasty. J Am Acad Orthop Surg. 2009;17(11):677–688. doi: 10.5435/00124635-200911000-00002. [DOI] [PubMed] [Google Scholar]
- 4.Rayan F, Haddad F. Periprosthetic femoral fractures in total hip arthroplasty –a review. Hip Int. 2010;20(4):418–426. doi: 10.1177/112070001002000402. [DOI] [PubMed] [Google Scholar]
- 5.Bone LB, Johnson KD, Weigelt J, Scheinberg R. Early versus delayed stabilization of femoral fractures. A prospective randomized study. J Bone Joint Surg Am. 1989;71(3):336–340. [PubMed] [Google Scholar]
- 6.Bone LB, McNamara K, Shine B, Border J. Mortality in multiple trauma patients with fractures. J Trauma. 1994;37(2):262–264. doi: 10.1097/00005373-199408000-00019. discussion 264-265. [DOI] [PubMed] [Google Scholar]
- 7.Bosse MJ, MacKenzie EJ, Riemer BL, Brumback RJ, McCarthy ML, Burgess AR, Gens DR, Yasui Y. Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated either with intramedullary nailing with reaming or with a plate. A comparative study. J Bone Joint Surg Am. 1997;79(6):799–809. doi: 10.2106/00004623-199706000-00001. [DOI] [PubMed] [Google Scholar]
- 8.Brundage SI, McGhan R, Jurkovich GJ, Mack CD, Maier RV. Timing of femur fracture fixation: effect on outcome in patients with thoracic and head injuries. J Trauma. 2002;52(2):299–307. doi: 10.1097/00005373-200202000-00016. [DOI] [PubMed] [Google Scholar]
- 9.Morshed S, Miclau T, 3rd, Bembom O, Cohen M, Knudson MM, Colford JM., Jr Delayed internal fixation of femoral shaft fracture reduces mortality among patients with multisystem trauma. J Bone Joint Surg Am. 2009;91(1):3–13. doi: 10.2106/JBJS.H.00338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Nahm NJ, Como JJ, Wilber JH, Vallier HA. Early appropriate care: definitive stabilization of femoral fractures within 24 hours of injury is safe in most patients with multiple injuries. J Trauma. 2011;71(1):175–185. doi: 10.1097/TA.0b013e3181fc93a2. [DOI] [PubMed] [Google Scholar]
- 11.Renaldo N, Egol K. Damage-control orthopedics: evolution and practical applications. Am J Orthop (Belle Mead NJ) 2006;35(6):285–291. discussion 291. [PubMed] [Google Scholar]
- 12.Tuttle MS, Smith WR, Williams AE, Agudelo JF, Hartshorn CJ, Moore EE, et al. Safety and efficacy of damage control external fixation versus early definitive stabilization for femoral shaft fractures in the multiple-injured patient. J Trauma. 2009;67(3):602–605. doi: 10.1097/TA.0b013e3181aa21c0. [DOI] [PubMed] [Google Scholar]
- 13.Lindahl H. Epidemiology of periprosthetic femur fracture around a total hip arthroplasty. Injury. 2007;38(6):651–654. doi: 10.1016/j.injury.2007.02.048. [DOI] [PubMed] [Google Scholar]
- 14.Duncan CP, Masri BA. Fractures of the femur after hip replacement. Instr Course Lect. 1995;44:293–304. [PubMed] [Google Scholar]
- 15.Brady OH, Garbuz DS, Masri BA, Duncan CP. The reliability and validity of the Vancouver classification of femoral fractures after hip replacement. J Arthroplasty. 2000;15(1):59–62. doi: 10.1016/s0883-5403(00)91181-1. [DOI] [PubMed] [Google Scholar]