

Abstract
Background:
Diabetic retinopathy (DR) is a leading cause of visual impairment in India. Available evidence shows that there are more than 60 million persons with diabetes in India and that the number will increase to more than a 100 million by 2030. There is a paucity of data on the perceptions and practices of persons with diabetes and the available infrastructure and uptake of services for DR in India.
Objectives:
Assess perception of care and challenges faced in availing eye care services among persons with diabetics and generate evidence on available human resources, infrastructure, and service utilization for DR in India.
Methods:
The cross-sectional, hospital-based survey was conducted in eleven cities across 9 States in India. In each city, public and private providers of eye-care were identified. Both multispecialty and standalone facilities were included. Specially designed semi-open ended questionnaires were administered to the clients. Semi-structured interviews were administered to the service providers (both diabetic care physicians and eye care teams) and observational checklists were used to record findings of the assessment of facilities conducted by a dedicated team of research staff.
Results:
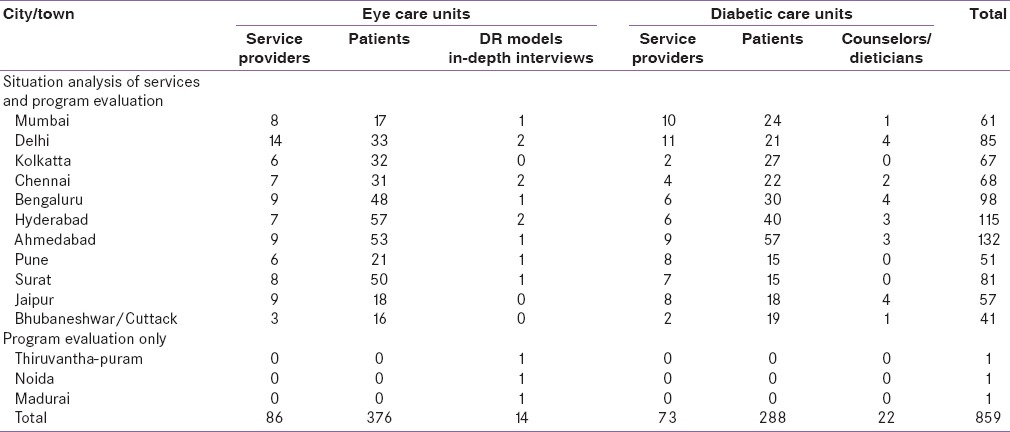
A total of 859 units were included in this study. This included 86 eye care and 73 diabetic care facilities, 376 persons with diabetes interviewed in the eye clinics and 288 persons with diabetes interviewed in the diabetic care facilities.
Conclusions:
The findings will have significant implications for the organization of services for persons with diabetes in India.
Keywords: Access to health care, diabetes, diabetic retinopathy, India, patient care
INTRODUCTION
Worldwide, an estimated 382 million people are living with diabetes, nearly a fifth of whom live in India.[1] The Indian Council of Medical Research recently conducted a study across four states in India (India Diabetes Study) and estimated that there were 62.4 million people with diabetes and 77.2 million people with prediabetes in 2011.[2] In some parts of India, the prevalence rate is as high as 20% among adults in urban areas and 10% in rural areas in those aged 20 years and above age?.[3] The number of people with diabetes in India is predicted to increase to 109 million by 2035 on account of population ageing and continuing socioeconomic status coupled with environmental and lifestyle changes. There is also evidence that Asian populations have a genetic predisposition to diabetes.[4]
Diabetic retinopathy (DR) is an important complication of diabetes. Globally there are an estimated 93 million people with DR, 38 million with the sight-threatening DR (STDR) forms, i.e., proliferative type (17 million) and cystoid/macular edema (21 million).[5] Studies in India have shown that between 18% and 34% of known diabetics have DR (of any severity).[6,7] There is a considerable body of evidence that the risk of blindness from DR can be reduced by better management of the known risk factors (i.e., hypertension,[8] blood glucose,[9] and lipids [10]) and by early detection and treatment of STDR.[11,12,13]
In India, the government has recently responded to the increase in noncommunicable diseases (NCDs) by establishing the National Programme on the Prevention and Control of Cancer, Diabetes, Cardiovascular diseases and Stroke. The program entails identification of those at risk at the community level, with referral to Primary and Community Health Centres for confirmatory diagnosis and treatment. However, the program does not currently emphasize control of the complications of diabetes, including DR. Lack of policies for control is compounded by the lack of knowledge of the risk of blindness among people living with diabetes as well as service providers in India.[14,15] A study from South India showed that only a fifth of the paramedical personnel and a tenth of the persons with diabetes were aware that poorly controlled blood glucose was an important risk factor for DR.[14] Many studies in India show that more than 50% persons with diabetes have poor glycemic control,[16,17] uncontrolled hypertension and dyslipidemia.[18] All these are potential risk factors for DR. Added to this is the finding that a significant proportion of persons with diabetes do not know that they have diabetes. For example, a recent study in 11 cities in India showed that 27.6% of newly detected middle-class diabetics did not know they were diabetic.[19] The situation is likely to be worse in economically and socially disadvantaged populations.
Recent data from India show that DR is responsible for 3.5% of blindness and severe visual impairment among people aged 50+ years.[20] As the prevalence of diabetes increases and persons with diabetes live longer, the risk of STDR increases exponentially. India is sitting at the threshold of an impending “epidemic” of STDR unless proactive measures are taken to integrate control into the Government of India's program for NCDs. Having said this, there are a number of initiatives in India, mainly initiated and run by the nongovernment eye care providers, for the detection and treatment of STDR,[21,22] but these have not been evaluated for coverage, cost effectiveness or sustainability and their ability to be taken to scale.
The Queen Elizabeth Diamond Jubilee Trust (the Trust) has recently provided support to develop a program for the prevention, early detection and management of STDR at district level in India. As the first step in the process, it was decided that baseline information should be gathered on existing services for the care of persons with diabetes and for managing DR and on the perceptions of persons with diabetes regarding the eye complications. The information was presented at a national, multidisciplinary Summit in April 2014 when the main gaps in service provision were identified and strategies for control delineated. In this paper, the methods used in the study are presented. A number of companion articles highlight the findings of this situational analysis.
The study had two broad aims:First, to assess services for the management of persons with diabetes and DR in hospitals and clinics in the largest (most populated) cities in India, and second, to evaluate the approaches being used by eye care providers to detect and treat STDR and to identify best practices in relation to responsiveness, acceptability, efficiency, equity, and sustainability. The specific objectives were to review current government policies for NCDs, focusing on diabetes and control of the complications; to map large public and private sector institutions providing services for diabetics and for DR (physician and eye care facilities) in the largest cities in India; to ascertain the workload and strategies adopted for DR and referral pathways; to determine the proportion of diabetics who know about the eye complications of diabetes, and the proportion who have had a retinal/eye examination; to assess the capacities of eye hospitals (both private and public sector) to manage DR and whether they are proactive in detecting STDR; to undertake in-depth evaluation of at least eight different models for detecting STDR (e.g., telemedicine; eye camps for diabetics; mobile training and treatment); and to identify best practices for screening and management of DR.
METHODS
Ethical approval
Ethical approval was obtained from the Institutional Review Committees of London School of Hygiene and Tropical Medicine and the Indian Institute of Public Health (IIPH), Hyderabad.
Informed consent
Written informed consent was obtained separately from the head of the institution and from each of the interviewed clients of services.
Definitions used
For the purpose of this study the following operational definitions were used:
Public funded: Facilities which were financed by the national or state governments or statutory bodies financed and controlled by the national or state governments
Private-funded: Facilities which were financed by organizations or individuals on their own. These included both the not-for-profit as well as the for-profit agencies/individuals
More populated/larger metropolitan cities: Cities with a population ≥7 million
Less populated/smaller metropolitan cities: Cities with a population <7 million
Standalone facilities: Facilities which provide only diabetic care facilities, irrespective of the size of the facility. This could include single practitioner clinics or hospitals with a large team of human resources
Multispecialty facilities: Facilities which provided many specialty medical services including diabetic care facilities. These included polyclinics and large hospitals with both out-patient consultation and inpatient facilities
Teaching facilities: All facilities providing postgraduate residency programs recognized by Medical Council of India (MCI) and National Board of Examinations (NBE) (MD/MS/DNB) or postdoctoral specialty fellowships
Nonteaching facilities: Facilities without formal training programs approved by MCI or NBE for medical graduates.
Layout
The methods will be described in two sections. First, the situation analysis of service providers, and secondly, evaluation of current initiatives for the detection and treatment of STDR will be described.
Situation analysis of service providers
Mixed-methods, i.e., qualitative and quantitative techniques were used to collect data from provider and clients' perspectives. Providers were teams in diabetic clinics (diabetologists, physicians, counselors, dieticians) and eye care teams providing clinical services for patients with DR (ophthalmologists, senior managers). Clients' perspectives were also sought by interviewing outpatients attending diabetic clinics and outpatients with DR attending eye departments/clinics.
Study location
A wide consultative process was adopted to decide where the study would take place and which cities to include. As the prevalence of diabetes is higher in urban than rural areas a decision was made to focus on services in urban areas, recognizing that these would probably represent the best available in India. Many services in urban areas are tertiary level referral centers for neighboring districts and smaller towns in the vicinity. If the services in these cities were sub-optimal, it is highly unlikely that services in smaller cities and towns would be better.
Selection of cities
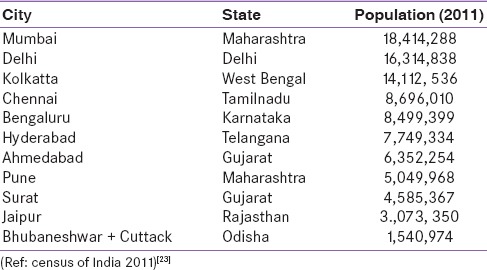
All cities in India were ranked in by population size (2011 census) and the 10 most populous cities were selected [Table 1].[23] As only one city (Kolkata) was in eastern India, the twin-cities of Bhubaneshwar and Cuttack were included to broaden geographical representation. Eleven cities were finally included in the study: Ahmedabad (Gujarat), Bengaluru (Karnataka), Bhubaneshwar (Odisha), Chennai (Tamil Nadu), Delhi, Hyderabad (Telangana), Jaipur (Rajasthan), Kolkata (West Bengal), Mumbai (Maharashtra), Pune (Maharashtra) and Surat (Gujarat). In addition, eye care models for screening for DR at the community level were assessed in three additional cities - Madurai (Tamil Nadu), Tiruvanthapuram (Kerala) and Noida (Uttar Pradesh).
Table 1.
Cities included in the study for assessing providers and clients, and their populations
Selection of health facilities
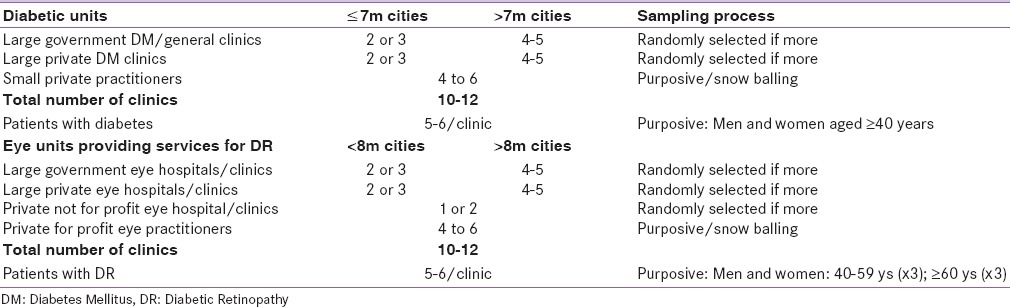
Two stage systematic, stratified random sampling was used to identify facilities to be included. In the first stage, cities were stratified based on their population (more than or less than 7 million) with a larger number of health facilities being included in bigger cities [Table 2]. In the second stage, a random sample was drawn from a list of hospitals/clinics meeting the inclusion criteria in each city.
Table 2.
Selection of units
The size of the health facility and provider (i.e., public funded; private-for-profit; private-not-for-profit) were used to identify facilities for inclusion. Diabetes care facilities were classified as (a) multi-specialty hospitals (i.e., 100 or more beds with three or more specialties), (b) polyclinics (smaller facilities providing a range of specialties) and (c) stand-alone diabetes clinics (physician/endocrinologist run facilities providing care for diabetes patients only). Eye care facilities were classified as (a) large dedicated eye hospitals (20 or more beds with sub-specialty services), (b) eye hospitals with satellites facilities (i.e., facilities in more than one location under joint management), (c) eye departments in general, multidisciplinary hospitals, and (d) eye practitioners (individual ophthalmologist practice).
Assessment of infrastructure in eye care and diabetic care facilities
Semi-structured interviews were conducted with physicians/diabetologists and eye care providers. In both types of service, the six elements of the World Health Organization's framework for health systems were evaluated i.e., number of staff and their skills; availability of infrastructure, equipment, laboratories, and medication; whether clinical guidelines and protocols were available as well as information for patients. All interviews were audio-recorded after obtaining permission respondents. All interviews are transcribed and translated into English for analysis.
Selection of patients for interview
Patients were randomly sampled at diabetes hospital/clinics and eye care hospital/clinics [Table 2] after obtaining permission from hospital administrators. At each diabetic care facility, 4–6 patients with diabetes were identified among those waiting for doctor's consultation, selecting equal numbers of males and females. Two patients in each of the following age strata (<50 years and >50 years) were interviewed. Similar procedures were followed in eye care facilities, but patients were only recruited after they were identified as having DR by the ophthalmologist. Since it was very difficult to identify younger patients with DR, in some cities only three age groups (<50 years and >50 years) were recruited. Interviews were conducted by trained interviewers using structured questionnaires.
In both types of clinics, patients were interviewed to assess their knowledge of diabetes and DR, to assess their health seeking behavior and the challenges they face in controlling their diabetes and/or in accessing services.
Data collection instruments
Personnel managing the programs were interviewed and data recorded using pretested data collection instruments. A consultation of key stakeholders was organized to finalize the methodological questions, instruments, and scope of the study. The following protocol was used for data collection.
Diabetic care providers: The following instruments were used: Semi-structured questionnaires were administered to the Senior Administrator or Head of Endocrinology Department on diabetes services; in-depth interviews were conducted with Senior Physician/Heads of Endocrinology/Internal Medicine Units using interview guides; structured questionnaires were administered to counselors, dieticians and patients, and an observation checklist was used to assess available equipment and services.
Eye care providers: The following instruments were used: Structured questionnaires were administered to the Senior Administrator or Head of Department; in-depth interviews were conducted with the Senior Physician or Heads Departments in the eye clinics or retina unit; structured questionnaires were administered to DR patients attending eye hospitals, and an observation checklist was used to assess available equipment and services.
All data collection instruments for patients, and the information sheets and consent forms, were translated into the local language and back-translated into English. The instruments were translated into eight Indian languages - Hindi, Telugu, Tamil, Oriya, Bengali, Gujarati, Marathi and Kannada. The data collection instruments were pretested in an eye hospital and a general hospital in Medak district, Telangana. Some questions were subsequently dropped or modified.
Data collection teams
Five dedicated teams each comprising a public health specialist/senior researcher from IIPH, a trained interviewer and two research assistants were constituted for data collection. The teams were first trained at the IIPH, Hyderabad for 3 days. Mock interviews were conducted by team members followed by a pilot in two locations in Medak district, Telangana state.
Data management and analysis
Databases for all the structured questionnaires and observation checklists were created in MS Access 2010. The following features were included to reduce data entry error, i.e., validation, skip pattern, drop down menu, auto calculation, etc. Data was entered by trained data entry operators. For the purpose of data protection, a login and password were created, and copies of the database were stored in three different systems. Data were then cleaned using appropriate steps and transferred into Stata and R (Stata Corp, Texas, US and R Foundation, Vienna, Austria) software for analysis. Numerous cross-tabulations were performed, focusing on the counts/frequencies of different types of facilities of DR.
Evaluation of initiatives for the detection and management of diabetic retinopathy
The purpose of the evaluation was to describe and evaluate the different approaches being used across the country for the detection and management of DR and more specifically treatment of STDR. The evaluation assessed each approach from the perspectives of collaboration and partnerships, effectiveness and efficiency, sustainability, integration, comprehensiveness and responsiveness and cost effectiveness with a view to identifying approaches that could be adopted or modified and taken to scale with support from the Trust. A range of different models was identified through prior knowledge of the authors, and by identifying additional providers during the situation analysis and snowballing. Some providers used more than one approach. Criteria for selecting the models were that they used different approaches (e.g., telemedicine; eye camps for diabetics; mobile screening with or without training and treatment; screening in clinics for diabetics), and hospitals providing large community-based screening programs for DR, by the government and private facilities.
A team of senior community eye care physicians developed a framework and protocol for mapping and analyzing services in terms of human resources, protocols, methods used and validity of screening procedures, monitoring follow-up of those who failed screening and those referred for treatment, and initiatives to improve uptake. Site visits and interviews, as well as reviewing information presented, were undertaken for this question. Information was collected on the processes used in all steps of the program, from how diabetics were identified for screening through to policies about follow-up after treatment. Multiple approaches were used to assess the parameters outlined above. First, a range of closed-ended questions were administered, drawing on the published literature whenever possible, followed by a detailed observation checklist on service provision, manpower, infrastructure, governance structure, community outreach program, etc., was used to collect information. Finally, service providers were asked to rank their service on a scale of 1 (low) to 100 (high) for each parameter included in the assessment. Data were managed as above. The methods used for this component of the study are described in more detail in a separate paper.
Coverage
A total of 859 units were included in the study [Table 3], including 14 eye care providers managing programs for the detection and treatment of STDR, which was more than initially planned.
Table 3.
Distribution of units included in the study
DISCUSSION
In this study, a range of different types of facilities caring for diabetics and those with DR were assessed, and the perceptions of patients regarding diabetes and DR were gathered in 11 cities across India. Three further cities were included in the program evaluation component. This is the largest and most comprehensive study of its kind in India. Findings are being used to inform elements of a comprehensive integrated district model of screening and management of DR embedded in the Government health system. The Queen's Trust working in partnership with the Public Health Foundation of India is supporting some of these initiatives for DR in India, including models for the detection and treatment of STDR which are integrated into the government of India's program for the control of noncommunicable diseases.
CONCLSUIONS
The findings of the study will be used to plan for need-based services for diabetic retinopathy in India.
Financial support and sponsorship
The study was supported by a grant from the Queen Elizabeth Diamond Jubilee Trust, London, UK
Conflicts of interest
There are no conflicts of interest
REFERENCES
- 1.International Diabetes Federation, Diabetes Atlas. 6th ed. 2013. [Last accessed on 2014 Feb 25]. Available from: http://www.idf.org/diabetesatlas .
- 2.Anjana RM, Pradeepa R, Deepa M, Datta M, Sudha V, Unnikrishnan R, et al. Prevalence of diabetes and prediabetes (impaired fasting glucose and/or impaired glucose tolerance) in urban and rural India: Phase I results of the Indian council of medical research-India DIABetes (ICMR-INDIAB) study. Diabetologia. 2011;54:3022–7. doi: 10.1007/s00125-011-2291-5. [DOI] [PubMed] [Google Scholar]
- 3.Unnikrishnan R, Anjana RM, Mohan V. Diabetes in South Asians: Is the phenotype different? Diabetes. 2014;63:53–5. doi: 10.2337/db13-1592. [DOI] [PubMed] [Google Scholar]
- 4.Yajnik CS. Early life origins of insulin resistance and type 2 diabetes in India and other Asian countries. J Nutr. 2004;134:205–10. doi: 10.1093/jn/134.1.205. [DOI] [PubMed] [Google Scholar]
- 5.Yau JW, Rogers SL, Kawasaki R, Lamoureux EL, Kowalski JW, Bek T, et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care. 2012;35:556–64. doi: 10.2337/dc11-1909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Raman R, Rani PK, Reddi Rachepalle S, Gnanamoorthy P, Uthra S, Kumaramanickavel G, et al. Prevalence of diabetic retinopathy in India: Sankara Nethralaya diabetic retinopathy epidemiology and molecular genetics study report 2. Ophthalmology. 2009;116:311–8. doi: 10.1016/j.ophtha.2008.09.010. [DOI] [PubMed] [Google Scholar]
- 7.Gupta S, Ambade A. Prevalence of diabetic retinopathy and influencing factors amongst type 2 diabetics from central India. Int J Diabetes Dev Ctries. 2004;24:75–8. [Google Scholar]
- 8.Do DV, Wang X, Vedula SS, Marrone M, Sleilati G, Hawkins BS, et al. Blood pressure control for diabetic retinopathy. Cochrane Database Syst Rev. 2015;1:CD006127. doi: 10.1002/14651858.CD006127.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hemmingsen B, Lund SS, Gluud C, Vaag A, Almdal TP, Hemmingsen C, et al. Targeting intensive glycaemic control versus targeting conventional glycaemic control for type 2 diabetes mellitus. Cochrane Database Syst Rev. 2013;11:CD008143. doi: 10.1002/14651858.CD008143.pub3. [DOI] [PubMed] [Google Scholar]
- 10.Keech AC, Mitchell P, Summanen PA, O'Day J, Davis TM, Moffitt MS, et al. Effect of fenofibrate on the need for laser treatment for diabetic retinopathy (FIELD study): A randomised controlled trial. Lancet. 2007;370:1687–97. doi: 10.1016/S0140-6736(07)61607-9. [DOI] [PubMed] [Google Scholar]
- 11.Evans JR, Michelessi M, Virgili G. Laser photocoagulation for proliferative diabetic retinopathy. Cochrane Database Syst Rev. 2014;11:CD011234. doi: 10.1002/14651858.CD011234.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Virgili G, Parravano M, Menchini F, Evans JR. Anti-vascular endothelial growth factor for diabetic macular oedema. Cochrane Database Syst Rev. 2014;10:CD007419. doi: 10.1002/14651858.CD007419.pub4. [DOI] [PubMed] [Google Scholar]
- 13.Han L, Zhang L, Xing W, Zhuo R, Lin X, Hao Y, et al. The associations between VEGF gene polymorphisms and diabetic retinopathy susceptibility: A meta-analysis of 11 case-control studies. J Diabetes Res. 2014;2014:805801. doi: 10.1155/2014/805801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Namperumalsamy P, Kim R, Kaliaperumal K, Sekar A, Karthika A, Nirmalan PK. A pilot study on awareness of diabetic retinopathy among non-medical persons in South India. The challenge for eye care programmes in the region. Indian J Ophthalmol. 2004;52:247–51. [PubMed] [Google Scholar]
- 15.Rani PK, Raman R, Subramani S, Perumal G, Kumaramanickavel G, Sharma T. Knowledge of diabetes and diabetic retinopathy among rural populations in India, and the influence of knowledge of diabetic retinopathy on attitude and practice. Rural Remote Health. 2008;8:838. [PubMed] [Google Scholar]
- 16.Raheja BS, Kapur A, Bhoraskar A, Sathe SR, Jorgensen LN, Moorthi SR, et al. DiabCare Asia – India study: Diabetes care in India – Current status. J Assoc Physicians India. 2001;49:717–22. [PubMed] [Google Scholar]
- 17.Nagpal J, Bhartia A. Quality of diabetes care in the middle- and high-income group populace: The Delhi diabetes community (DEDICOM) survey. Diabetes Care. 2006;29:2341–8. doi: 10.2337/dc06-0783. [DOI] [PubMed] [Google Scholar]
- 18.Ramachandran A, Mary S, Sathish CK, Selvam S, Catherin Seeli A, Muruganandam M, et al. Population based study of quality of diabetes care in Southern India. J Assoc Physicians India. 2008;56:513–6. [PubMed] [Google Scholar]
- 19.Gupta A, Gupta R, Sharma KK, Lodha S, Achari V, Asirvatham AJ, et al. Prevalence of diabetes and cardiovascular risk factors in middle-class urban participants in India. BMJ Open Diabetes Res Care. 2014;2:e000048. doi: 10.1136/bmjdrc-2014-000048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Patil S, Gogate P, Vora S, Ainapure S, Hingane RN, Kulkarni AN, et al. Prevalence, causes of blindness, visual impairment and cataract surgical services in Sindhudurg district on the western coastal strip of India. Indian J Ophthalmol. 2014;62:240–5. doi: 10.4103/0301-4738.128633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Rani PK, Raman R, Sharma V, Mahuli SV, Tarigopala A, Sudhir RR, et al. Analysis of a comprehensive diabetic retinopathy screening model for rural and urban diabetics in developing countries. Br J Ophthalmol. 2007;91:1425–9. doi: 10.1136/bjo.2007.120659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Rani PK, Raman R, Agarwal S, Paul PG, Uthra S, Margabandhu G, et al. Diabetic retinopathy screening model for rural population: Awareness and screening methodology. Rural Remote Health. 2005;5:350. [PubMed] [Google Scholar]
- 23.Census of India. City Census 2011. [Last accessed on 2014 Feb 25]. Available from: http://www.census2011.co.in/city.php .