

Abstract
Esophageal complications caused by gastroesophageal reflux disease (GERD) include reflux esophagitis and Barrett’s esophagus (BE). BE is a premalignant condition with an increased risk of developing esophageal adenocarcinoma (EAC). The carcinogenic sequence may progress through several steps, from normal esophageal mucosa through BE to EAC. A recent advent of functional esophageal testing (particularly multichannel intraluminal impedance and pH monitoring) has helped to improve our knowledge about GERD pathophysiology, including its complications. Those findings (when properly confirmed) might help to predict BE neoplastic progression. Over the last few decades, the incidence of EAC has continued to rise in Western populations. However, only a minority of BE patients develop EAC, opening the debate regarding the cost-effectiveness of current screening/surveillance strategies. Thus, major efforts in clinical and research practice are focused on new methods for optimal risk assessment that can stratify BE patients at low or high risk of developing EAC, which should improve the cost effectiveness of screening/surveillance programs and consequently significantly affect health-care costs. Furthermore, the area of BE therapeutic management is rapidly evolving. Endoscopic eradication therapies have been shown to be effective, and new therapeutic options for BE and EAC have emerged. The aim of the present review article is to highlight the status of screening/surveillance programs and the current progress of BE therapy. Moreover, we discuss the recent introduction of novel esophageal pathophysiological exams that have improved the knowledge of the mechanisms linking GERD to BE.
Keywords: Gastroesophageal reflux disease, Barrett’s esophagus, Esophageal adenocarcinoma, Impedance and pH monitoring, Endoscopy
Core tip: The review highlights the significant progress in the diagnostic and therapeutic management of Barrett’s esophagus (BE) thanks to the development of up-and-coming endoscopic technologies. Moreover, we discuss the recent introduction of novel esophageal pathophysiological exams that have improved the knowledge of the mechanisms implicated in the genesis of esophageal mucosal damage, paving the way to the future possibility of predicting BE neoplastic progression. The comparison of endoscopic surveillance and eradication therapy recommendations for BE in currently available guidelines are provided.
INTRODUCTION
Gastroesophageal reflux disease (GERD) is defined as a condition that develops when the reflux of stomach contents causes troublesome symptoms and/or complications[1]. Esophageal complications caused by GERD include reflux esophagitis and Barrett’s esophagus (BE), and the latter predisposes patients to esophageal adenocarcinoma (EAC)[1]. BE is a premalignant condition in which the normal stratified squamous epithelium of the distal esophagus is replaced by columnar mucosa with intestinal specialized metaplasia[2].
GERD is a worldwide disease, and evidence suggests an overall increase in its prevalence since 1995[3,4]. As a result, costs related to GERD diagnosis, treatment and surveillance represent a substantial commitment of economic resources[5]. In parallel, over the last few decades, the incidence of EAC has continued to rise in Western populations[6-8]. The totality of evidence supports the idea that the different racial, ethnic and gender distributions of BE may drive the risk of EAC, with incidence rates much higher among male, non-Hispanic whites[7,9]. However, fewer than 10% of GERD patients are likely to progress to a diagnosis of BE at 5 years[10], and only a minority of BE patients develop EAC; the previously estimated risk of 0.5% per year[11-13] was recently lowered to approximately 0.3% per year[14,15]. Furthermore, more than 90% of EAC patients are not known to have BE before diagnosis[16]. In line with these assumptions, the current strategies of BE screening and surveillance programs are debated and show moderate to absent cost-effectiveness[17,18].
The aim of the present review article is to highlight the status of screening/surveillance programs and the current progress of BE therapy. Moreover, we discuss the recent introduction of novel esophageal pathophysiological exams that have improved the knowledge of the mechanisms linking GERD to BE.
ESOPHAGEAL PATHOPHYSIOLOGICAL EXAMS
The overall characteristics and composition of the refluxate, together along with the dysfunction of the anti-reflux barrier, the impairment of mucosal defence, visceral motility and esophageal clearance, represent the complex set of mechanisms that determines GERD manifestation and its complications[19]. To date, it is well known that the refluxate may contain varying concentrations of acid, pepsin, or duodenal contents (i.e., bile acid, pancreatic enzymes) implicated in the development of esophageal mucosal damage[20-22]. In keeping with the spectrum model of GERD, several studies have demonstrated that severity of acid reflux increases from non-erosive reflux disease (NERD) through erosive reflux disease (ERD) up to short (i.e., esophageal intestinal metaplasia up to 3 cm in length, SSBE) and long segments (i.e., esophageal intestinal metaplasia more than 3 cm in length, LSBE) of BE[23-25]. Similarly, the presence of duodenogastroesophageal reflux (DGER), evaluated with a fibreoptic spectrophotometer (Bilitec), increases significantly across the spectrum of GERD from NERD to BE[26-29]. Of note, it has been established that acid and DGER occur simultaneously in the majority of the reflux episodes, and at best, bile reflux may have a synergistic role in producing esophageal damage[26,27].
Over the past decade, the introduction of new technologies with which to study the esophagus from a functional point of view has helped improve our knowledge of GERD pathophysiology. The combination of multichannel intraluminal impedance and pH monitoring (MII-pH) provides a comprehensive characterization of reflux episodes during a 24-h period, detecting both chemical (i.e., acid, weakly acidic or weakly alkaline) and physical properties (i.e., liquid, mixed, gas, proximal extension)[30]. Regarding SSBE, by means of monitoring only pH, the acid exposure time (AET) may be similar to that found in NERD and normal in several patients[31]. Therefore, Frazzoni et al[32] assessed reflux parameters via a combined MII-pH study in newly diagnosed SSBE, at baseline and during proton pump inhibitor (PPI) therapy. The authors found that MII-pH improved the overall diagnostic yield because the number of reflux episodes was altered in more than one half of patients with normal AET off PPI. Moreover, 69% of SSBE patients on PPI therapy showed an increased number of total reflux events, the vast majority of which were weakly acidic refluxes[32]. These findings are consistent with other studies in which the number of both acid and weakly acidic reflux episodes was increased in patients with BE[33,34]. In particular, Savarino et al[34] highlighted that the greater total exposure of esophageal mucosa to acid and weakly acidic reflux was due to intermittent reflux episodes. Indeed, the authors found a higher frequency of “re-reflux” episodes in BE than in ERD patients[34]. “Re-reflux” episodes (i.e., the occurrence of a further reflux when the basal esophageal pH is already below 4) represent a diagnostic advantage obtained through MII-pH because pH-only monitoring equipment has a lower sampling frequency[35,36]. Moreover, intermittent reflux episodes determining a brief exposure of acid or bile might be more important than continuous exposure concerning the genesis of the overall alterations promoting the progression of BE[37,38]. With regard to the role of weakly acidic refluxes, it is important to realize that in an environment at a pH between 4 and 5.5, pepsins and bile acids can still damage esophageal mucosa[39,40]. Given that the main consequence of PPI therapy is to convert acid refluxes into weakly acidic refluxes without significant changes in the number of total reflux events[41], a regression of intestinal metaplasia with long-term PPI therapy is somewhat doubtful. At last, Bredenoord et al[33] found that in patients with BE, only a few reflux episodes reached the proximal esophagus that seems to be more sensitive, likely explaining, at least in part, why these subjects often report fewer symptoms then NERD patients[42,43].
The recent introduction in the clinical and research practice of high-resolution manometry (HRM) has represented a major advance in characterizing esophageal motility abnormalities in GERD patients, with particular regard for dysfunction of the antireflux barrier and impaired esophageal clearance[44,45]. However, at present, the role of HRM in reflux remains restricted to preoperative testing, the identification of possible mechanisms and the exclusion of motility disorders[45]. Of note, several studies have shown that esophageal motility abnormalities are increasingly prevalent with increasing severity of GERD presentation[25,46-49]. In particular, Savarino et al[50] evaluated 755 GERD patients through conventional or impedance esophageal manometry and/or MII-pH testing, and they found that ineffective esophageal motility gradually increased from controls and functional heartburn to NERD and from ERD to BE. Likewise, the esophageal clearing function decreased as the severity of mucosal damage increased, with ERD and BE patients having the greatest prevalence of bolus transit abnormalities, which occurred also in cases of normal motility pattern[50].
Finally, a recent study by Frazzoni et al[51] assessed that neoplastic progression in SSBE was associated with an impairment of esophageal chemical clearance. Impedance can be used to measure the clearance of a swallowed bolus from the esophagus[52], and a parameter representing esophageal chemical clearance, named the post-reflux swallow-induced peristaltic wave (PSPW) index, can be obtained through MII-pH monitoring[53]. The impairment of chemical clearance represents a crucial mechanism in the pathophysiology of GERD and is not affected by medical or surgical therapy. In fact, the PSPW index has increased the diagnostic yield of MII-pH in GERD patients[54,55]. In this setting, Frazzoni et al[51] showed that the PSPW index was lower in SSBE patients with incident dysplasia than in those without it, and a PSPW index cut-off value of 26% was able to discriminate between these two groups of patients. Overall, the authors speculated that predicting neoplastic progression in SSBE based on a low PSPW index might be useful to select those patients deserving a close endoscopic follow-up, thus improving the cost-effectiveness of surveillance programs[51].
DIAGNOSTIC ROLE OF UPPER ENDOSCOPY
To date, the gold standard for the evaluation of BE is high-resolution white-light endoscopy with biopsy sampling performed according to the Seattle protocol[56-59]. The Prague classification represents a reliable and validated endoscopic classification of BE, which records the length of the esophagus involved circumferentially (C) in addition to the maximal length (M) involved at any point[60].
The development of EAC in BE seems to occur through the progression of intestinal metaplasia to low-grade dysplasia (LGD) and high-grade dysplasia (HGD). Thus, the presence of dysplasia represents the most widely used marker of neoplastic progression in BE[61]. High-resolution endoscopes, allowing for a fine definition of the mucosal layer, seem to have high sensitivity for detecting dysplasia and BE-related early neoplasia[62]. Furthermore, a longer inspection time during white-light endoscopy seems to be associated with a higher detection rate of HGD/EAC[63].
Some studies have investigated the detection of intestinal metaplasia with chromoendoscopy. Available data regarding the improvement of methylene blue-targeted biopsy samples, compared with random samples, are conflicting[64-67]. Moreover, methylene blue may damage DNA, so its use is not recommended[68]. The only randomized trial that has evaluated indigo carmine for the detection of dysplasia in BE has not found a higher rate of dysplasia than high-resolution white-light endoscopy[69]. Regarding virtual chromoendoscopy, narrow band imaging (NBI) is the most extensively studied in BE[70]. A meta-analysis of eight studies reported a NBI sensitivity and specificity of 95% and 65%, respectively, for the diagnosis of intestinal metaplasia and of 96% and 94%, respectively, for the diagnosis of HGD[71]. However, the interobserver agreement for the interpretation of NBI images is moderate, and on a per-patient basis, high-resolution endoscopy alone seems to be sufficient to maximize dysplasia detection[72,73].
Autofluorescence imaging alone has an excessively high false-positive rate of dysplasia detection[74]. Additionally, the use of endoscopic trimodal imaging (i.e., high-resolution endoscopy, autofluorescence imaging and NBI), compared with standard endoscopy with random biopsy sampling, has shown contradictory results[75,76]. Regarding spectroscopy and optical coherence tomography, further studies are warranted to define their usefulness in BE surveillance[77,78]. Randomized crossover studies on the diagnostic yield of acetic acid-enhanced magnification endoscopy for BE intestinal metaplasia have produced contradictory data[79,80]. Using this technique, promising results have been obtained in dysplasia detection[81,82], and it also seems to be more cost-effective than the Seattle protocol in a high-risk population[83]. However, further studies are necessary to ascertain the utility of this technique.
Recently, the use of probe-based confocal laser endomicroscopy combined with high-definition white-light endoscopy significantly improved the ability to detect neoplasia in BE patients compared with high-definition white-light endoscopy[84,85].
Finally, molecular imaging, exploiting fluorescently labelled molecules that bind with a different affinity to dysplastic and non-dysplastic cells, is a promising technique[86,87]. In a recent study, using a novel peptide that binds to areas of HGD and neoplasia, Sturm et al[88] reported 75% sensitivity and 97% specificity for neoplasia.
Screening
Because the proportion of EAC patients with a prior diagnosis of BE is low, and given the low incidence of EAC in BE[15,89], performing a screening program for BE with endoscopy in an unselected population is not cost-effective. Currently, most medical societies suggest endoscopic screening for BE in patients with chronic GERD symptoms and multiple risk factors (i.e., 50 years of age or older, white race, male gender, obesity, history of smoking, family history for BE or EAC)[58,59] or in men older than 60 years with reflux symptoms for 10 years[90].
New methods for BE screening are being evaluated with some promising results. Transnasal endoscopy is a well-tolerated method, and it seems to have good accuracy, but further validation is necessary[91]. Moreover, biopsy specimens taken with these endoscopes are small, which could increase sampling bias and hinder the interpretation[92].
Cytosponge is a non-endoscopic esophageal sampling device coupled with immunocytochemistry for trefoil factor 3, a marker of columnar epithelium with intestinal metaplasia[93,94]. In a study involving 504 patients, Kadri et al[93] reported a sensitivity and a specificity for the detection of BE of, respectively, 73% and 94%. This test also appears to be more cost-effective for screening than conventional endoscopy[95]. However, the Cytosponge needs further validation, particularly considering the lower sensitivity for SSBE detection.
Recently, a risk-prediction model including multiple demographic and clinical variables (i.e., GERD frequency and duration, age, sex, race, waist-to-hip ratio, Helicobacter pylori status), serum levels of cytokines (IL12p70, IL6, IL8, IL10) and leptin obtained an area under the curve of 0.85, a better result than that achieved by other non-invasive methods[96].
Surveillance
Observational studies have shown that patients with BE receiving an EAC diagnosis during endoscopic surveillance have earlier-stage tumours and higher survival rates than those whose tumours are discovered because of symptoms[97,98]. However, such studies are susceptible to biases that could overestimate the benefits of surveillance. Furthermore, recent studies have reported a lower annual risk of progression from BE to EAC than previously observed (approximately 0.3% per year)[14,15]. The risk of progressing to EAC could also be lower in patients with a persistence of non-dysplastic BE after several surveillance endoscopies[99]. Despite the lack of high-quality evidence, most guidelines recommend surveillance endoscopy every 2-5 years for non-dysplastic BE, as shown in Table 1[57-59,90,100,101]. In cases of an indefinite diagnosis for dysplasia (IND), the risk of progression seems to be only in the first year[102], and it appears higher in patients with multifocal IND[103]. Current guidelines recommend a 6-12 mo interval to repeat, a biopsy (Table 1), and an increased acid suppression in cases of inflammatory infiltration and regenerative changes[57-59,90,100,101]. Because limited data are available, the natural history of LGD in BE is not yet clear. A recent meta-analysis found an annual rate of progression from LGD to EAC of 0.5% but a wide variability across studies[104]. The main issue for LGD diagnosis is a high degree of interobserver variability[105], in part due to the difficulty in differentiating it from reactive changes[106], therefore, a confirmation after an expert histological review is recommended[107]. Immunohistochemistry for p53 overexpression can be particularly useful to improve interobserver agreement for dysplasia detection[106], and it can be recommended as an adjunct to histopathology[58]. In patients with LGD on a single occasion, a repeat endoscopy in 2-12 mo (time interval depending on the society) is recommended, along with a more frequent surveillance if LGD is confirmed (Table 1). There is also evidence that LSBE patients with persistent and multifocal LGD are more likely to progress to EAC[108].
Table 1.
Comparison of endoscopic surveillance recommendations for Barrett’s esophagus in currently available guidelines
| Guidelines | NDBE | IND | LGD | HDG |
| BOB CAT[90] | Not recommended1 | ≤ 12 mo | 6-12 mo | Not recommended |
| ACPG[57] | < 3 cm 3-5 yr | ≤ 6 mo | 6 mo | Not recommended |
| ≥ 3 cm 2-3 yr | ||||
| BSG[58] | < 3 cm 3-5 yr | ≤ 6 mo | 6 mo | Not recommended |
| ≥ 3 cm 2-3 yr | ||||
| ASGE[100] | 3-5 yr | No specific time frame | 12 mo2 | 3 mo3 |
| ACP[101] | 3-5 yr | Not recommended | No specific time frame | No specific time frame |
| AGA[59] | 3-5 yr | Not recommended | 6-12 mo | 3 mo3 |
If undertaken, surveillance should be directed at high-risk groups (i.e., composite risk factors including but not limited to 50 years of age or older, white race, male sex, central obesity, the length of the segment, and the symptom duration, frequency and severity), unless the life expectancy ≤ 5 yr;
Six months to confirm LGD;
In the absence of eradication therapy. BOB CAT: Benign Barrett’s and Cancer Taskforce; ACPG: Australian Clinical Practice Guidelines; BSG: British Society for Gastroenterology; ASGE: American Society for Gastrointestinal Endoscopy; ACP: American College of Physicians; AGA: American Gastroenterological Association; NDBE: Non-dysplastic Barrett’s esophagus; IND: Indefinite for dysplasia; LGD: Low-grade dysplasia; HGD: High-grade dysplasia.
MEDICAL THERAPY
A large retrospective study highlighted how the control of reflux is important in the management of BE, showing a significantly lower rate of progression to LGD, HGD, or EAC in patients who had a history of antireflux surgery or PPI use[109]. Moreover, a recent meta-analysis of observational studies showed that PPI therapy was associated with a 71% risk reduction in BE progression with a trend towards a dose-response relationship, considering PPI use for > 2-3 years, protective against EAC or HGD[110]. However, a considerable heterogeneity was observed, and chemopreventive high-quality prospective trials of PPIs in patients with BE are warranted[110,111].
Complete, but not partial, acid suppression by PPIs over 6 mo, as measured by 24-h pH monitoring, decreases markers of epithelial proliferation and increases cell differentiation markers in patients with BE[112]. Similarly, a randomized clinical trial showed that a high-dose esomeprazole promoted a decrease in proliferative markers, concomitantly with a decrease in apoptotic cell death[113]. Overall, PPI therapy seems to be important not only because it reduces the acidity, and therefore the chemical damage, of the refluxate but also because PPIs have anti-inflammatory properties independent of their acid-suppressive effects[114].
A large case-control study by Nguyen et al[115] indicated that using PPI, nonsteroidal anti-inflammatory drugs (NSAID)/aspirin, or statin therapy in patients with BE might reduce the risk of developing EAC. Furthermore, an interesting study found that the incubation of isolated cells from mucosal biopsies of BE metaplasia with aspirin and omeprazole together induced a significantly greater reduction in proliferative activity than that induced separately by any of the two drugs, thus suggesting a synergistic effect of the two drugs[116]. To ascertain the efficacy of chemoprevention with PPIs and/or aspirin in BE metaplasia, a large clinical trial (Aspirin Esomeprazole Chemoprevention Trial - AspECT) was planned, the results of which are expected in 2016[117].
Although the exact dose of PPIs and the therapeutic efficacy endpoint are not known, high-dosage PPIs are commonly prescribed in clinical practice. However, the currently available international guidelines are not in a total agreement regarding recommendations for the maintenance treatment with PPIs in patients with BE. The recent international Benign Barrett’s and Cancer Taskforce (BOB CAT) consensus group hints at using medical over surgical therapies to prevent BE neoplastic progression[90]. The Australian Clinical Practice Guidelines suggests that only symptomatic patients with BE should be treated with PPI therapy, with the dose titrated to control symptoms[57]. According to the British Society of Gastroenterology, there is not yet sufficient evidence to recommend acid-suppression drugs as chemopreventive agents, even if PPIs have the best clinical profile for symptom management[58]. Moreover, the American Gastroenterological Association (AGA) highlighted that PPI therapy also has effects that, conceivably, might promote the development of cancer in BE (i.e., increasing the serum levels of gastrin, a hormone than can induce proliferation in BE epithelium)[59]. Because the evidence to support potent acid suppression with PPIs as a chemopreventive strategy in BE is largely indirect, the AGA asserts that insufficient data are available to advocate the prescription of PPIs in dosages higher than those necessary to eliminate the symptoms and endoscopic signs of GERD or, for patients without such symptoms and signs, in dosages higher than those suggested as conventional for GERD treatment. Likewise, there are not sufficient data to support the use of esophageal pH monitoring to titrate the PPI dosage to normalize AET in patients with BE[59].
ENDOSCOPIC THERAPY
Over the past decade, evidence has been accumulating on the effectiveness of the endoscopic management in BE treatment. There is generally high level of agreement across various guidelines regarding the management of non-dysplastic BE and BE with HGD or EAC. However, the therapy administered to patients with LGD is often a controversial topic. The changing guidelines for the BE endoscopic management are shown in Table 2.
Table 2.
Recommendations for endoscopic eradication therapy in Barrett’s esophagus
| Guidelines | NDBE | LGD | HGD/intramucosal EAC |
| ACG[118] | Not recommended | Not recommended | Endoscopic ablation or surgical esophagectomy |
| AGA[59] | RFA (± EMR) for select individuals at risk for progression | RFA is a therapeutic option | Endoscopic therapy with RFA, PDT or EMR EMR in BE dysplasia with a visible mucosal irregularity Before proceeding with esophagectomy, patients with HGD or intramucosal EAC should be referred for evaluation by surgical specialized centres |
| BAD CAT[120] | - | - | Endoscopic treatment should be preferred over endoscopic surveillance or surgery for the management of most patients with HGD/intramucosal EAC RFA is currently the best available ablation technique for the treatment of flat HGD and for the eradication of residual BE after focal EMR In the HGD endoscopic resection of all visible abnormalities, cap and snare and band ligation with resection are equally effective |
| ASGE (2012)[100] | Consider endoscopic ablation in select cases | Consider endoscopic resection or ablation | Consider endoscopic resection or RFA ablation. Consider EUS for local staging and lymphadenopathy Consider surgical consultation |
| BSG[58] | Not recommended | Not routinely recommended | Endoscopic therapy preferred over esophagectomy |
| ASGE (2013)[123] | - | - | EMR is indicated for nodular BE and T1a EAC and may be used for flat BE with HGD ESD can be used in similar situations but is preferred to EMR for large areas of dysplasia or T1b EAC (i.e., confined to the submucosa) Ablation techniques may be used alone or in combination with mucosal resection techniques |
| BOB CAT[90] | If the lesion is visible, endoscopic resection for diagnosis is then appropriate ablative therapy | - | |
| Not recommended | Lower risk: Intense surveillance. Higher risk: Ablative therapy with follow-up | ||
ACG: American College of Gastroenterology; AGA: American Gastroenterology Association; BAD CAT: Barrett’s Dysplasia and Cancer Taskforce; ASGE: American Society for Gastrointestinal Endoscopy; BSG: British Society for Gastroenterology; BOB CAT: Benign Barrett’s and Cancer Taskforce; RFA: Radiofrequency ablation; EMR: Endoscopic mucosal resection; PDT: Photodynamic therapy; EUS: Endoscopic ultrasound; ESD: Endoscopic submucosal dissection; BE: Barrett’s esophagus; NDBE: Non-dysplastic Barrett’s esophagus; LGD: Low-grade dysplasia; HGD: High-grade dysplasia; EAC: Esophageal adenocarcinoma.
Management of non-dysplastic and LGD BE
In 2011, AGA proposed using radiofrequency ablation (RFA; with or without endoscopic mucosal resection, EMR) for selected non-dysplastic BE individuals at risk for progression; however, the risk criteria were not fully defined. Then, it was also stated that RFA in LGD leads to reversion to normal-appearing squamous epithelium in > 90% of cases, and ablation should be the therapeutic option in those cases[59]. In the American Society for Gastrointestinal Endoscopy guidelines, endoscopic ablation therapy was suggested as the management option in selected patients with non-dysplastic BE. They also allowed the consideration of endoscopic resection or ablation in all LGD cases[100]. However, according to the British guidelines, the endoscopic treatment was not routinely recommended in non-dysplastic BE or in LGD[58].
Recent management strategies, established by the international BOB CAT consensus, include the following: (1) endoscopic resection/ablation is not recommended in benign BE; and (2) patients with LGD on a single occasion, without higher-risk features, should be managed with endoscopic surveillance continued for 6-12 mo (provided the patient is fit for endoscopy and is not already undergoing therapy)[90]. The absence of dysplasia in two subsequent upper endoscopies identifies a cohort of patients, previously diagnosed with LGD, who are at low risk of neoplastic progression and can keep on routine surveillance. Moreover, the BOB CAT consensus states that BE patients with multifocal LGD and/or with LGD that persists have an increased risk for neoplastic progression than those with focal LGD or with LGD detected on a single endoscopy[90]. The former group should be treated with ablative therapy rather than only followed up with[90].
Management of HGD and early-stage EAC
In HGD, there is a high rate of progression to EAC (6%-19% per year), and endoscopic therapy is a well-established therapy for these cases. All associations recommend endoscopic therapy (with a combination of EMR followed by the ablation of residual BE mucosa) for HGD and intramucosal EAC (Table 2)[58,59,118-120]. Previously, the standard of treatment was esophagectomy due to high cure rates, but it was also characterized by substantial mortality (2%-5%) and morbidity (30%-50%)[121].
In 2013, the European Society for Medical Oncology stated that surgery is the treatment of choice in early EAC (Tis-T1a, N0). However, endoscopic resection is an alternative treatment option for selected patients because similar cure rates in specialized centres have been reported[122]. Similarly to BE with dysplasia, endoscopic therapy for early-stage EAC includes resection and ablation techniques[123]. EMR successfully eradicates 91% to 98% of T1a EAC[123,124], with a cancer-free survival similar to and a lower morbidity than surgical resection[125]. The long-term survival of 742 patients with TisN0M0 and T1N0M0 EAC treated with either endoscopic modalities (most commonly EMR) and surgical resection was similar[126]. Zehetner et al[127] demonstrated similar survival in patients with HGD and intramucosal EAC treated with endoscopic resection and ablation than surgical resection, with a significantly lower morbidity associated with endoscopic treatment.
Categories of endoscopic BE eradication modalities
Multiple modalities may be employed for the endoscopic eradication of BE. There are two main types of endoscopic therapy: Tissue-acquiring techniques, which include EMR and endoscopic submucosal dissection (ESD), and ablative techniques, which include thermal techniques (RFA, multipolar electrocoagulation, argon plasma coagulation), cryotherapy and photochemical techniques (photodynamic therapy, PDT)[119]. Examples of ablative therapies are shown in Table 3.
Table 3.
Ablation therapy in Barrett’s esophagus
| Ablation modalities | Description of the technique | Outcome | Ref. |
| RFA | RFA uses a balloon-based circumferential array of closely spaced electrodes to deliver radiofrequency energy to the esophageal mucosa. With this technique, the mucosa is ablated to the submucosal level. A smaller, endoscope-mounted, radiofrequency catheter ablation device could be used for the focal ablation of metaplasia that could remain after treatment with the circumferential system. A follow-up endoscopy is at 3 mo when any remaining metaplasia is ablated, with a further follow-up endoscopy at 1 yr | A landmark large, multicentre, randomized trial showed that RFA can eliminate HGD, reducing the risk of EAC compared with a sham procedure. Overall, the eradication rates for HGD range from 79% to 90% and from 69% and 97% for NDBE/LGD patients RFA is safer and easier to administer, and it causes fewer major complications, particularly stricture formation, than PDT | [133,145] |
| APC | APC produces a flow of ionized argon plasma that generates a high-frequency monopolar current to the BE surface under direct vision | Different eradication rates for NDBE and LGD in the short term ranged from 36% to 100% for NDBE and rates of recurrence between 62% and 100% for LGD patients | [133] |
| PDT | PDT is based on the injection of a light sensitizing drug (e.g., porfimer sodium) into the patient and then the exposure of a portion of the esophagus to light of a specific wavelength, which would lead to dysplasia cell death. Once the photosensitizer is activated by the light, it generates oxygen free radicals that result in cytotoxicity to the mucosal cells | The eradication rates for HGD range from 77% to 100%, and those for NDBE/LGD range from 50%-100% of patients The limitations include the cost of the intravenous agent, the prolonged period (weeks) of photosensitivity following exposure, and an appreciable post-treatment stricture rate | [133] |
| CRY | CRY is a non-contact method of cryotherapy that involves an endoscopically directed spray of liquid nitrogen at -196 °C directly onto the Barrett’s mucosa The advantage is a lack of contact with mucosa and hence can be applied to irregularity, which would make the application of contact therapies such as RFA challenging | The rates of complete eradication are approximately 68%-97% for HGD and 57% for NDBE The current literature is inadequate to assess the ability of CRY to achieve sustained reversion of the metaplastic mucosa to normal-appearing squamous epithelium in subjects at any stage of BE. Further longitudinal studies are needed | [133,156] |
| MPEC | MPEC uses an endoscopic multipolar electrical probe, which is used to control gastrointestinal haemorrhage that applies electrical energy at 50 W so that all BE surfaces are treated | Complete eradication in 65%-100% of NDBE. This technique is very much operator dependent and causes dysphagia as the most common side effect | [133] |
RFA: Radiofrequency ablation; APC: Argon plasma coagulation; PDT: Photodynamic therapy; CRY: Cryoablation; MPEC: Multipolar electrocoagulation; EAC: Esophageal adenocarcinoma; BE: Barrett’s esophagus; IM: Intestinal metaplasia; NDBE: Non-dysplastic Barrett’s esophagus; LGD: Low-grade dysplasia; HGD: High-grade dysplasia.
The great advantage of both EMR and ESD, compared to ablative therapies, is that specimens for histopathological analysis at the time of treatment can be obtained. The diagnosis of dysplasia and neoplasia in EMR specimens is improved, particularly because of the upstaging of cases previously diagnosed as dysplasia and the assessment of the depth of invasion with the determination of margins of resection[119,128-130], which have crucial implications in the appropriate choice of treatment and outcomes[131]. However, ablation therapies can be applied to larger surface areas and to different resection locations[132].
The AGA guidelines recommended RFA, PDT, cryotherapy, thermal energy application, and EMR in BE eradication in 2011[59,133]. Currently, the most commonly used technologies are RFA and EMR used alone or in combination. In most cases, ablation techniques are used in combination with resection techniques (multimodal therapy), wherein ablation techniques are applied following EMR or ESD that are used to remove macroscopically visible lesions[119].
Endoscopic mucosal resection
EMR is an endoscopic technique useful in the resection of macroscopically visible BE lesions that are less than 2 cm in diameter. To lift the lesion from the muscularis propria, normal saline or dilute epinephrine is first injected into submucosa[119]. EMR can be performed with either EMR-cap or EMR-ligation techniques. The former uses suction to retract the target tissue into a plastic cap that is attached to the endoscope, and a snare is closed around the lesion, followed by electrocautery. The latter uses suction to aspirate the tissue, followed by band deployment, to create a pseudopolyp. Then, a hexagonal snare and electrocautery are used to resect the lesion[119]. These two techniques have shown similar diagnostic accuracy and safety[119,134]. However, with the ability to perform several resections with a single intubation and kit, EMR-ligation technique seems to be faster and less expensive[134].
Complete remission of dysplasia and intestinal metaplasia is achieved in > 80%-90% of patients undergoing EMR with or without concurrent ablative therapy[135,136]. Recently, a large group of patients with BE and T1a EAC treated with endoscopic therapy reported a 96.3% complete response rate. The overall survival rate was 91% at 5 years and 75% at 10 years[137].
Potential complications of EMR are bleeding, perforation, and stricture formation. Delayed bleeding is infrequent, but immediate post-resection bleeding can occur in 10% of patients[138]. Perforation rates are reported to be less than 3%. The extent of mucosa removed by EMR is the risk factor for stricture formations (37% of cases), the majority of which are successfully managed by endoscopic dilation[124,135,139].
ESD
ESD is more likely to achieve an en bloc resection, usually of lesions > 2 cm. First, a lesion is lifted off the muscularis propria with an injected solution; then, dissection in the submucosal plane, using a variety of dissection knives, is performed. ESD in the esophagus is technically more difficult, particularly due to narrow lumen, fibrosis caused by chronic reflux, and the thin wall of the esophagus. Furthermore, esophageal ESD showed frequent complications, such as bleeding, perforation (rates between 2% and 5%), and stricture formation (rates between 5% and 17.2%)[119,140-143]. Prophylactic steroid injection following esophageal ESD has been shown to decrease the risk of stricture formation[144].
Radiofrequency ablation
Radiofrequency ablation (RFA) delivers high-frequency energy to the esophageal mucosa to achieve tissue necrosis. The depth of ablation is between 500 and 1000 μm. There are two systems available: A 3-cm-long balloon ablation catheter (HALO 360) intended to treat circumferential LSBE (Figure 1) and an endoscope-mounted targeted device (HALO 90, HALO 60, HALO ULTRA) to treat SSBE and BE islands and tongues (Figure 1)[132]. The technique involves mucosal ablation under endoscopic guidance followed by the removal of the adhered white coagulum in the ablated area and then by repeat treatment of the same area, all within one endoscopic session (Figure 2). Multiple endoscopic treatments may be required depending on the length of the BE segment and the tissue response. Treatment is usually performed every 2-3 mo[132].
Figure 1.
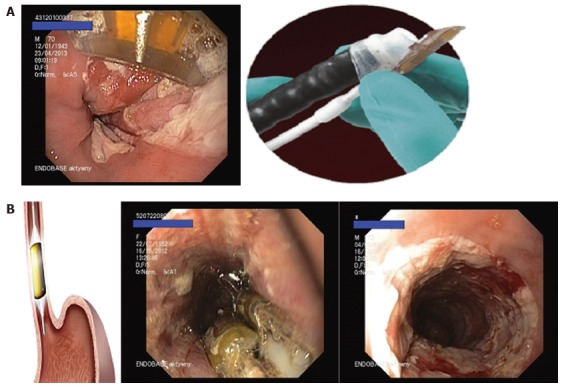
Radiofrequency ablation to treat Barrett’s esophagus. A: HALO 90 to treat short segments, islands and tongues of Barrett’s esophagus; B: Balloon ablation catheter (HALO 360) intended to treat long-segment circumferential Barrett’s esophagus. Material from Department of Digestive Tract Disease, Medical University of Lodz, Poland.
Figure 2.
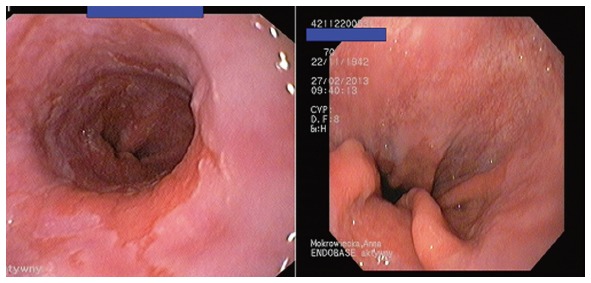
Improvement after radiofrequency ablation of Barrett’s esophagus. Material from Department of Digestive Tract Disease, Medical University of Lodz, Poland.
Among patients undergoing RFA, a complete eradication of dysplasia occurred in 90.5% and in 81% of LGD and HGD patients, respectively, at a 12-mo follow-up. Overall, 77.4% of patients in the ablation group had complete eradication of intestinal metaplasia[145]. Subsequently, RFA therapy provided an acceptable safety profile associated with a low rate of disease progression for up to 3 years[146]. RFA efficacy has been demonstrated in several other studies, with eradication rates of metaplasia and dysplasia ranging from approximately 81%-92.6% and 75%-88.2%, respectively[119,147,148]. Moreover, reductions in rates of progression from LGD and HGD to cancer have been demonstrated in randomized controlled trials with RFA[145,147].
RFA is safe and well tolerated. The most common complications reported include chest pain lasting less than one week, strictures requiring dilation (6%-8%), gastrointestinal haemorrhage (1%), and perforation (less than 1%)[132,145,149].
Incomplete response to ablation is possible, particularly in cases of a longer duration of dysplasia, longer BE segments, a loss of p16 locus or polysomy (detected by FISH) and poor reflux control[119,150-152]. The presence or persistence of intestinal metaplasia under new squamous epithelium is known as “buried metaplasia”. Because of its malignant potential, it is important to remember that it could be invisible in endoscopic surveillance and in superficial biopsies. The prevalence of buried metaplasia was 14% after PDT and 0.9% after RFA, but the results could be underestimated[119,153,154]. Similar rates of recurrence have been reported with all modalities of BE endotherapy (RFA, PDT and cryotherapy). Most recurrences can be treated endoscopically if detected early. Thus, post-treatment endoscopic surveillance is needed[119,155,156].
SURGICAL THERAPY
Surgical treatment is indicated particularly in patients who need long-term treatment of GERD (i.e., patients with persistent troublesome symptoms and/or a progression of disease despite adequate PPI therapy)[157,158]. To achieve an increase in the quality of life, proper diagnostic testing should be performed to adequately select patients before surgery[157-159].
Laparoscopic partial and total fundoplications are currently the best available surgical techniques to treat severe GERD[158]. The two major competing procedures are the laparoscopic Nissen fundoplication and the posterior partial Toupet hemifundoplication. Randomized studies have shown a similar outcome at 5 years but a higher rate of side effects (dysphagia, bloating, and flatulence) and a higher reoperation rate in the Nissen group than in the Toupet group[160,161]. In contrast, other studies have reported minor side effects and a lower reoperation rate for the Nissen procedure[162-164]. Because of these controversies, the choice of fundoplication technique should be left to the individual preferences of the surgeon.
Recently, the LOTUS trial showed a comparable rate of symptom control between surgery and escalating doses of PPIs[165]. Surgery should be considered for younger patients, particularly in cases with a high risk of progression with large hiatal hernias, severe reflux symptoms, and a long history of disease to prevent the progression to BE[166,167]. However, there is limited evidence of the effectiveness of antireflux surgery in reducing the extent of BE and the risk of progression to cancer, as well as the regression of BE. Thus, after antireflux surgery, endoscopic surveillance has to be maintained[168-171]. Of note, it has been shown that neoplastic progression after antireflux surgery is due primarily to the subsequent recurrence of reflux[172].
Surgery is still the treatment of choice in early EAC; however, in 2011, AGA stated that most patients with HGD BE (70%-80%) can be successfully treated with endoscopic eradication therapy. Esophagectomy in patients with HGD is an alternative; however, the current data suggest a lower morbidity with ablative therapy[59]. The important issue is the choice of surgical centres specializing in the treatment of foregut cancers and HGD. In 2012, the Barrett’s Dysplasia and Cancer Task Force (BAD CAT) consensus group stated that endoscopic treatment is preferred to surgery in most cases of HGD; however, esophagectomy results in a long-term cure. Moreover, there is no strong evidence that fundoplication reverses HGD[120].
For localized EAC without suspected lymph node involvement (T1-2 N0M0), surgery is regarded as a standard treatment. However, the long-term survival does not exceed 25% if regional lymph nodes are involved (pN1-3). Therefore, preoperative treatment can also be justified[122,173]. Preoperative chemoradiotherapy is preferred in EAC for selected patients, particularly in high-risk patients (i.e., those with locally more advanced stages). Even after a complete tumour response to preoperative chemoradiotherapy, operable patients with EAC should proceed to surgery[122].
CONCLUSION
BE is a premalignant condition that affects 1.3%-2% of the adult population[174-176]. Patients with BE have an increased risk of developing EAC through a gradual process, in which metaplastic epithelium without dysplasia evolves to LGD, HGD and eventually EAC. GERD is considered to play a major role in the development of these histologic changes[61,177]. Indeed, GERD symptoms, ERD, and BE have a number of common determinants (i.e., esophagogastric junction dysfunction, impaired esophageal clearance, gastric and duodenal contents of the refluxate), which are implicated in the genesis of esophageal mucosal damage[19]. In keeping with the spectrum model of GERD, the severity of acid reflux, DGER, and esophageal motility abnormalities are increasingly prevalent with the increasing severity of GERD presentation, from NERD, through ERD, and up to BE[25,28]. Over the past decade, the introduction of new technologies (particularly with regard to MII-pH) has increased the overall diagnostic yield of the pathophysiological mechanisms underlying GERD manifestation and its complications (including BE)[32-34,50,51]. In particular, a proper evaluation of impairment of esophageal chemical clearance might help predict BE neoplastic progression[51]. However, future studies are expected to substantiate this finding.
To date, dysplasia is considered the most widely used marker of BE progression to cancer, and generally, its detection warrants intensified surveillance and/or treatment[59]. Considering the large increase in the incidence of EAC[8], effective screening/surveillance programs of BE, coupled with improved therapeutic approaches, represent the hope to reverse this incidence. However, only a minority of BE patients develop EAC, with a current estimated risk of 0.3% per year[14,15]. Moreover, given the large number of subjects with BE, endoscopic examinations represent a substantial commitment of resources[5]. Thus, current strategies of screening and surveillance programs of BE are debated, showing moderate to absent cost-effectiveness[18]. New methods for BE screening are being evaluated with some promising results; however, we still await conclusive data for the best screening approach (i.e., simple, minimally invasive), and additional studies are urgently needed. Clearly, the identification of subgroups of patients at reduced or increased risk for BE development and degeneration would lead to more cost-effective strategies for the prevention of EAC, helping select those patients deserving a close endoscopic follow-up. At present, the management of patients with LGD represents a main issue due to its unpredictable natural history, the lack of cost-effectiveness data regarding the surveillance of LGD and high disagreement between pathologists in LGD diagnosis[100].
The area of BE therapeutic management is rapidly evolving. Unequivocal data on the use of drugs such as PPIs, aspirin or statins in the chemoprevention of BE are lacking. At the moment, there is no doubt regarding the use of PPIs for symptom control[58,59]. Endoscopic eradication therapies have been shown to be effective in patients with BE/EAC, and new therapies have appeared. BE containing HGD and/or early-stage EAC can be treated endoscopically instead of with surgical esophagectomy. Moreover, recent management strategies, including a de-escalation strategy for lower-risk patients and escalation to intervention with follow-up for higher-risk patients, have been established[90,120]. The main objective of endoscopic therapy should be the elimination of all intestinal metaplasia because the recurrence of neoplasia appears to be higher in individuals who do not achieve a full eradication of BE[124].
Footnotes
Conflict-of-interest statement: The authors declare no potential conflicts of interest and no financial support.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Peer-review started: July 31, 2015
First decision: September 16, 2015
Article in press: March 18, 2016
P- Reviewer: Abdel-Salam O, Actis GC S- Editor: Kong JX L- Editor: A E- Editor: Wu HL
References
- 1.Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol. 2006;101:1900–1920; quiz 1943. doi: 10.1111/j.1572-0241.2006.00630.x. [DOI] [PubMed] [Google Scholar]
- 2.Spechler SJ. Barrett’s esophagus. Semin Oncol. 1994;21:431–437. [PubMed] [Google Scholar]
- 3.El-Serag HB, Sweet S, Winchester CC, Dent J. Update on the epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut. 2014;63:871–880. doi: 10.1136/gutjnl-2012-304269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ness-Jensen E, Lindam A, Lagergren J, Hveem K. Changes in prevalence, incidence and spontaneous loss of gastro-oesophageal reflux symptoms: a prospective population-based cohort study, the HUNT study. Gut. 2012;61:1390–1397. doi: 10.1136/gutjnl-2011-300715. [DOI] [PubMed] [Google Scholar]
- 5.Peery AF, Dellon ES, Lund J, Crockett SD, McGowan CE, Bulsiewicz WJ, Gangarosa LM, Thiny MT, Stizenberg K, Morgan DR, et al. Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterology. 2012;143:1179–1187.e1-3. doi: 10.1053/j.gastro.2012.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Chang CY, Cook MB, Lee YC, Lin JT, Ando T, Bhatia S, Chow WH, El-Omar EM, Goto H, Li YQ, et al. Current status of Barrett’s esophagus research in Asia. J Gastroenterol Hepatol. 2011;26:240–246. doi: 10.1111/j.1440-1746.2010.06529.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Cook MB, Chow WH, Devesa SS. Oesophageal cancer incidence in the United States by race, sex, and histologic type, 1977-2005. Br J Cancer. 2009;101:855–859. doi: 10.1038/sj.bjc.6605246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kroep S, Lansdorp-Vogelaar I, Rubenstein JH, Lemmens VE, van Heijningen EB, Aragonés N, van Ballegooijen M, Inadomi JM. Comparing trends in esophageal adenocarcinoma incidence and lifestyle factors between the United States, Spain, and the Netherlands. Am J Gastroenterol. 2014;109:336–343; quiz 335, 344. doi: 10.1038/ajg.2013.420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Corley DA, Kubo A, Levin TR, Block G, Habel L, Rumore G, Quesenberry C, Buffler P. Race, ethnicity, sex and temporal differences in Barrett’s oesophagus diagnosis: a large community-based study, 1994-2006. Gut. 2009;58:182–188. doi: 10.1136/gut.2008.163360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Malfertheiner P, Nocon M, Vieth M, Stolte M, Jaspersen D, Koelz HR, Labenz J, Leodolter A, Lind T, Richter K, et al. Evolution of gastro-oesophageal reflux disease over 5 years under routine medical care--the ProGERD study. Aliment Pharmacol Ther. 2012;35:154–164. doi: 10.1111/j.1365-2036.2011.04901.x. [DOI] [PubMed] [Google Scholar]
- 11.Jankowski JA, Provenzale D, Moayyedi P. Esophageal adenocarcinoma arising from Barrett’s metaplasia has regional variations in the west. Gastroenterology. 2002;122:588–590. doi: 10.1053/gast.2002.31599. [DOI] [PubMed] [Google Scholar]
- 12.Shaheen NJ, Crosby MA, Bozymski EM, Sandler RS. Is there publication bias in the reporting of cancer risk in Barrett’s esophagus. Gastroenterology. 2000;119:333–338. doi: 10.1053/gast.2000.9302. [DOI] [PubMed] [Google Scholar]
- 13.Murray L, Watson P, Johnston B, Sloan J, Mainie IM, Gavin A. Risk of adenocarcinoma in Barrett’s oesophagus: population based study. BMJ. 2003;327:534–535. doi: 10.1136/bmj.327.7414.534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hvid-Jensen F, Pedersen L, Drewes AM, Sørensen HT, Funch-Jensen P. Incidence of adenocarcinoma among patients with Barrett’s esophagus. N Engl J Med. 2011;365:1375–1383. doi: 10.1056/NEJMoa1103042. [DOI] [PubMed] [Google Scholar]
- 15.Bhat S, Coleman HG, Yousef F, Johnston BT, McManus DT, Gavin AT, Murray LJ. Risk of malignant progression in Barrett’s esophagus patients: results from a large population-based study. J Natl Cancer Inst. 2011;103:1049–1057. doi: 10.1093/jnci/djr203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Verbeek RE, Leenders M, Ten Kate FJ, van Hillegersberg R, Vleggaar FP, van Baal JW, van Oijen MG, Siersema PD. Surveillance of Barrett’s esophagus and mortality from esophageal adenocarcinoma: a population-based cohort study. Am J Gastroenterol. 2014;109:1215–1222. doi: 10.1038/ajg.2014.156. [DOI] [PubMed] [Google Scholar]
- 17.Corley DA, Mehtani K, Quesenberry C, Zhao W, de Boer J, Weiss NS. Impact of endoscopic surveillance on mortality from Barrett’s esophagus-associated esophageal adenocarcinomas. Gastroenterology. 2013;145:312–319.e1. doi: 10.1053/j.gastro.2013.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Gordon LG, Mayne GC. Cost-effectiveness of Barrett’s oesophagus screening and surveillance. Best Pract Res Clin Gastroenterol. 2013;27:893–903. doi: 10.1016/j.bpg.2013.08.019. [DOI] [PubMed] [Google Scholar]
- 19.Bredenoord AJ, Pandolfino JE, Smout AJ. Gastro-oesophageal reflux disease. Lancet. 2013;381:1933–1942. doi: 10.1016/S0140-6736(12)62171-0. [DOI] [PubMed] [Google Scholar]
- 20.Woodland P, Sifrim D. The refluxate: The impact of its magnitude, composition and distribution. Best Pract Res Clin Gastroenterol. 2010;24:861–871. doi: 10.1016/j.bpg.2010.09.002. [DOI] [PubMed] [Google Scholar]
- 21.Lagergren J, Bergström R, Lindgren A, Nyrén O. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med. 1999;340:825–831. doi: 10.1056/NEJM199903183401101. [DOI] [PubMed] [Google Scholar]
- 22.Koek GH, Tack J, Sifrim D, Lerut T, Janssens J. The role of acid and duodenal gastroesophageal reflux in symptomatic GERD. Am J Gastroenterol. 2001;96:2033–2040. doi: 10.1111/j.1572-0241.2001.03863.x. [DOI] [PubMed] [Google Scholar]
- 23.Loughney T, Maydonovitch CL, Wong RK. Esophageal manometry and ambulatory 24-hour pH monitoring in patients with short and long segment Barrett’s esophagus. Am J Gastroenterol. 1998;93:916–919. doi: 10.1111/j.1572-0241.1998.00276.x. [DOI] [PubMed] [Google Scholar]
- 24.Fass R, Hell RW, Garewal HS, Martinez P, Pulliam G, Wendel C, Sampliner RE. Correlation of oesophageal acid exposure with Barrett’s oesophagus length. Gut. 2001;48:310–313. doi: 10.1136/gut.48.3.310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Zentilin P, Conio M, Mele MR, Mansi C, Pandolfo N, Dulbecco P, Gambaro C, Tessieri L, Iiritano E, Bilardi C, et al. Comparison of the main oesophageal pathophysiological characteristics between short- and long-segment Barrett’s oesophagus. Aliment Pharmacol Ther. 2002;16:893–898. doi: 10.1046/j.1365-2036.2002.01237.x. [DOI] [PubMed] [Google Scholar]
- 26.Champion G, Richter JE, Vaezi MF, Singh S, Alexander R. Duodenogastroesophageal reflux: relationship to pH and importance in Barrett’s esophagus. Gastroenterology. 1994;107:747–754. doi: 10.1016/0016-5085(94)90123-6. [DOI] [PubMed] [Google Scholar]
- 27.Vaezi MF, Richter JE. Role of acid and duodenogastroesophageal reflux in gastroesophageal reflux disease. Gastroenterology. 1996;111:1192–1199. doi: 10.1053/gast.1996.v111.pm8898632. [DOI] [PubMed] [Google Scholar]
- 28.Koek GH, Sifrim D, Lerut T, Janssens J, Tack J. Multivariate analysis of the association of acid and duodeno-gastro-oesophageal reflux exposure with the presence of oesophagitis, the severity of oesophagitis and Barrett’s oesophagus. Gut. 2008;57:1056–1064. doi: 10.1136/gut.2006.119206. [DOI] [PubMed] [Google Scholar]
- 29.Zaninotto G, Portale G, Parenti A, Lanza C, Costantini M, Molena D, Ruol A, Battaglia G, Costantino M, Epifani M, et al. Role of acid and bile reflux in development of specialised intestinal metaplasia in distal oesophagus. Dig Liver Dis. 2002;34:251–257. doi: 10.1016/s1590-8658(02)80144-x. [DOI] [PubMed] [Google Scholar]
- 30.Zentilin P, Dulbecco P, Savarino E, Giannini E, Savarino V. Combined multichannel intraluminal impedance and pH-metry: a novel technique to improve detection of gastro-oesophageal reflux literature review. Dig Liver Dis. 2004;36:565–569. doi: 10.1016/j.dld.2004.03.019. [DOI] [PubMed] [Google Scholar]
- 31.Frazzoni M, Manno M, De Micheli E, Savarino V. Pathophysiological characteristics of the various forms of gastro-oesophageal reflux disease. Spectrum disease or distinct phenotypic presentations? Dig Liver Dis. 2006;38:643–648. doi: 10.1016/j.dld.2006.02.020. [DOI] [PubMed] [Google Scholar]
- 32.Frazzoni M, Savarino E, Manno M, Melotti G, Mirante VG, Mussetto A, Bertani H, Manta R, Conigliaro R. Reflux patterns in patients with short-segment Barrett’s oesophagus: a study using impedance-pH monitoring off and on proton pump inhibitor therapy. Aliment Pharmacol Ther. 2009;30:508–515. doi: 10.1111/j.1365-2036.2009.04063.x. [DOI] [PubMed] [Google Scholar]
- 33.Bredenoord AJ, Hemmink GJ, Smout AJ. Relationship between gastro-oesophageal reflux pattern and severity of mucosal damage. Neurogastroenterol Motil. 2009;21:807–812. doi: 10.1111/j.1365-2982.2009.01306.x. [DOI] [PubMed] [Google Scholar]
- 34.Savarino E, Zentilin P, Frazzoni M, Cuoco DL, Pohl D, Dulbecco P, Marabotto E, Sammito G, Gemignani L, Tutuian R, et al. Characteristics of gastro-esophageal reflux episodes in Barrett’s esophagus, erosive esophagitis and healthy volunteers. Neurogastroenterol Motil. 2010;22:1061–e280. doi: 10.1111/j.1365-2982.2010.01536.x. [DOI] [PubMed] [Google Scholar]
- 35.Sifrim D, Castell D, Dent J, Kahrilas PJ. Gastro-oesophageal reflux monitoring: review and consensus report on detection and definitions of acid, non-acid, and gas reflux. Gut. 2004;53:1024–1031. doi: 10.1136/gut.2003.033290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Shay SS, Johnson LF, Richter JE. Acid rereflux: a review, emphasizing detection by impedance, manometry, and scintigraphy, and the impact on acid clearing pathophysiology as well as interpreting the pH record. Dig Dis Sci. 2003;48:1–9. doi: 10.1023/a:1021762310433. [DOI] [PubMed] [Google Scholar]
- 37.Kaur BS, Ouatu-Lascar R, Omary MB, Triadafilopoulos G. Bile salts induce or blunt cell proliferation in Barrett’s esophagus in an acid-dependent fashion. Am J Physiol Gastrointest Liver Physiol. 2000;278:G1000–G1009. doi: 10.1152/ajpgi.2000.278.6.G1000. [DOI] [PubMed] [Google Scholar]
- 38.Tselepis C, Morris CD, Wakelin D, Hardy R, Perry I, Luong QT, Harper E, Harrison R, Attwood SE, Jankowski JA. Upregulation of the oncogene c-myc in Barrett’s adenocarcinoma: induction of c-myc by acidified bile acid in vitro. Gut. 2003;52:174–180. doi: 10.1136/gut.52.2.174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Roberts NB. Review article: human pepsins - their multiplicity, function and role in reflux disease. Aliment Pharmacol Ther. 2006;24 Suppl 2:2–9. doi: 10.1111/j.1365-2036.2006.03038.x. [DOI] [PubMed] [Google Scholar]
- 40.Farré R, van Malenstein H, De Vos R, Geboes K, Depoortere I, Vanden Berghe P, Fornari F, Blondeau K, Mertens V, Tack J, et al. Short exposure of oesophageal mucosa to bile acids, both in acidic and weakly acidic conditions, can impair mucosal integrity and provoke dilated intercellular spaces. Gut. 2008;57:1366–1374. doi: 10.1136/gut.2007.141804. [DOI] [PubMed] [Google Scholar]
- 41.Hemmink GJ, Bredenoord AJ, Weusten BL, Monkelbaan JF, Timmer R, Smout AJ. Esophageal pH-impedance monitoring in patients with therapy-resistant reflux symptoms: ‘on’ or ‘off’ proton pump inhibitor. Am J Gastroenterol. 2008;103:2446–2453. doi: 10.1111/j.1572-0241.2008.02033.x. [DOI] [PubMed] [Google Scholar]
- 42.Bredenoord AJ, Weusten BL, Timmer R, Smout AJ. Characteristics of gastroesophageal reflux in symptomatic patients with and without excessive esophageal acid exposure. Am J Gastroenterol. 2006;101:2470–2475. doi: 10.1111/j.1572-0241.2006.00945.x. [DOI] [PubMed] [Google Scholar]
- 43.Emerenziani S, Ribolsi M, Sifrim D, Blondeau K, Cicala M. Regional oesophageal sensitivity to acid and weakly acidic reflux in patients with non-erosive reflux disease. Neurogastroenterol Motil. 2009;21:253–258. doi: 10.1111/j.1365-2982.2008.01203.x. [DOI] [PubMed] [Google Scholar]
- 44.Martinucci I, de Bortoli N, Giacchino M, Bodini G, Marabotto E, Marchi S, Savarino V, Savarino E. Esophageal motility abnormalities in gastroesophageal reflux disease. World J Gastrointest Pharmacol Ther. 2014;5:86–96. doi: 10.4292/wjgpt.v5.i2.86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.DeVault K, McMahon BP, Celebi A, Costamagna G, Marchese M, Clarke JO, Hejazi RA, McCallum RW, Savarino V, Zentilin P, et al. Defining esophageal landmarks, gastroesophageal reflux disease, and Barrett’s esophagus. Ann N Y Acad Sci. 2013;1300:278–295. doi: 10.1111/nyas.12253. [DOI] [PubMed] [Google Scholar]
- 46.Kahrilas PJ, Dodds WJ, Hogan WJ, Kern M, Arndorfer RC, Reece A. Esophageal peristaltic dysfunction in peptic esophagitis. Gastroenterology. 1986;91:897–904. doi: 10.1016/0016-5085(86)90692-x. [DOI] [PubMed] [Google Scholar]
- 47.Ho KY, Kang JY. Reflux esophagitis patients in Singapore have motor and acid exposure abnormalities similar to patients in the Western hemisphere. Am J Gastroenterol. 1999;94:1186–1191. doi: 10.1111/j.1572-0241.1999.01063.x. [DOI] [PubMed] [Google Scholar]
- 48.Diener U, Patti MG, Molena D, Fisichella PM, Way LW. Esophageal dysmotility and gastroesophageal reflux disease. J Gastrointest Surg. 2001;5:260–265. doi: 10.1016/s1091-255x(01)80046-9. [DOI] [PubMed] [Google Scholar]
- 49.Wu JC, Cheung CM, Wong VW, Sung JJ. Distinct clinical characteristics between patients with nonerosive reflux disease and those with reflux esophagitis. Clin Gastroenterol Hepatol. 2007;5:690–695. doi: 10.1016/j.cgh.2007.02.023. [DOI] [PubMed] [Google Scholar]
- 50.Savarino E, Gemignani L, Pohl D, Zentilin P, Dulbecco P, Assandri L, Marabotto E, Bonfanti D, Inferrera S, Fazio V, et al. Oesophageal motility and bolus transit abnormalities increase in parallel with the severity of gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 2011;34:476–486. doi: 10.1111/j.1365-2036.2011.04742.x. [DOI] [PubMed] [Google Scholar]
- 51.Frazzoni M, Bertani H, Conigliaro R, Frazzoni L, Losi L, Melotti G. Neoplastic progression in short-segment Barrett’s oesophagus is associated with impairment of chemical clearance, but not inadequate acid suppression by proton pump inhibitor therapy. Aliment Pharmacol Ther. 2014;40:835–842. doi: 10.1111/apt.12895. [DOI] [PubMed] [Google Scholar]
- 52.Conchillo JM, Smout AJ. Review article: intra-oesophageal impedance monitoring for the assessment of bolus transit and gastro-oesophageal reflux. Aliment Pharmacol Ther. 2009;29:3–14. doi: 10.1111/j.1365-2036.2008.03863.x. [DOI] [PubMed] [Google Scholar]
- 53.Frazzoni M, Manta R, Mirante VG, Conigliaro R, Frazzoni L, Melotti G. Esophageal chemical clearance is impaired in gastro-esophageal reflux disease--a 24-h impedance-pH monitoring assessment. Neurogastroenterol Motil. 2013;25:399–406, e295. doi: 10.1111/nmo.12080. [DOI] [PubMed] [Google Scholar]
- 54.de Bortoli N, Martinucci I, Savarino E, Tutuian R, Frazzoni M, Piaggi P, Bertani L, Furnari M, Franchi R, Russo S, et al. Association between baseline impedance values and response proton pump inhibitors in patients with heartburn. Clin Gastroenterol Hepatol. 2015;13:1082–8.e1. doi: 10.1016/j.cgh.2014.11.035. [DOI] [PubMed] [Google Scholar]
- 55.Frazzoni M, Savarino E, de Bortoli N, Martinucci I, Furnari M, Frazzoni L, Mirante VG, Bertani H, Marchi S, Conigliaro R, et al. Analyses of the Post-reflux Swallow-induced Peristaltic Wave Index and Nocturnal Baseline Impedance Parameters Increase the Diagnostic Yield of Impedance-pH Monitoring of Patients With Reflux Disease. Clin Gastroenterol Hepatol. 2016;14:40–46. doi: 10.1016/j.cgh.2015.06.026. [DOI] [PubMed] [Google Scholar]
- 56.Levine DS, Haggitt RC, Blount PL, Rabinovitch PS, Rusch VW, Reid BJ. An endoscopic biopsy protocol can differentiate high-grade dysplasia from early adenocarcinoma in Barrett’s esophagus. Gastroenterology. 1993;105:40–50. doi: 10.1016/0016-5085(93)90008-z. [DOI] [PubMed] [Google Scholar]
- 57.Whiteman DC, Appleyard M, Bahin FF, Bobryshev YV, Bourke MJ, Brown I, Chung A, Clouston A, Dickins E, Emery J, et al. Australian clinical practice guidelines for the diagnosis and management of Barrett’s esophagus and early esophageal adenocarcinoma. J Gastroenterol Hepatol. 2015;30:804–820. doi: 10.1111/jgh.12913. [DOI] [PubMed] [Google Scholar]
- 58.Fitzgerald RC, di Pietro M, Ragunath K, Ang Y, Kang JY, Watson P, Trudgill N, Patel P, Kaye PV, Sanders S, et al. British Society of Gastroenterology guidelines on the diagnosis and management of Barrett’s oesophagus. Gut. 2014;63:7–42. doi: 10.1136/gutjnl-2013-305372. [DOI] [PubMed] [Google Scholar]
- 59.Spechler SJ, Sharma P, Souza RF, Inadomi JM, Shaheen NJ. American Gastroenterological Association medical position statement on the management of Barrett’s esophagus. Gastroenterology. 2011;140:1084–1091. doi: 10.1053/j.gastro.2011.01.030. [DOI] [PubMed] [Google Scholar]
- 60.Sharma P, Dent J, Armstrong D, Bergman JJ, Gossner L, Hoshihara Y, Jankowski JA, Junghard O, Lundell L, Tytgat GN, et al. The development and validation of an endoscopic grading system for Barrett’s esophagus: the Prague C & amp; M criteria. Gastroenterology. 2006;131:1392–1399. doi: 10.1053/j.gastro.2006.08.032. [DOI] [PubMed] [Google Scholar]
- 61.Hameeteman W, Tytgat GN, Houthoff HJ, van den Tweel JG. Barrett’s esophagus: development of dysplasia and adenocarcinoma. Gastroenterology. 1989;96:1249–1256. doi: 10.1016/s0016-5085(89)80011-3. [DOI] [PubMed] [Google Scholar]
- 62.Wolfsen HC, Crook JE, Krishna M, Achem SR, Devault KR, Bouras EP, Loeb DS, Stark ME, Woodward TA, Hemminger LL, et al. Prospective, controlled tandem endoscopy study of narrow band imaging for dysplasia detection in Barrett’s Esophagus. Gastroenterology. 2008;135:24–31. doi: 10.1053/j.gastro.2008.03.019. [DOI] [PubMed] [Google Scholar]
- 63.Gupta N, Gaddam S, Wani SB, Bansal A, Rastogi A, Sharma P. Longer inspection time is associated with increased detection of high-grade dysplasia and esophageal adenocarcinoma in Barrett’s esophagus. Gastrointest Endosc. 2012;76:531–538. doi: 10.1016/j.gie.2012.04.470. [DOI] [PubMed] [Google Scholar]
- 64.Sharma P, Topalovski M, Mayo MS, Weston AP. Methylene blue chromoendoscopy for detection of short-segment Barrett’s esophagus. Gastrointest Endosc. 2001;54:289–293. doi: 10.1067/mge.2001.115728. [DOI] [PubMed] [Google Scholar]
- 65.Canto MI, Setrakian S, Willis J, Chak A, Petras R, Powe NR, Sivak MV. Methylene blue-directed biopsies improve detection of intestinal metaplasia and dysplasia in Barrett’s esophagus. Gastrointest Endosc. 2000;51:560–568. doi: 10.1016/s0016-5107(00)70290-2. [DOI] [PubMed] [Google Scholar]
- 66.Gossner L, Pech O, May A, Vieth M, Stolte M, Ell C. Comparison of methylene blue-directed biopsies and four-quadrant biopsies in the detection of high-grade intraepithelial neoplasia and early cancer in Barrett’s oesophagus. Dig Liver Dis. 2006;38:724–729. doi: 10.1016/j.dld.2006.05.025. [DOI] [PubMed] [Google Scholar]
- 67.Ngamruengphong S, Sharma VK, Das A. Diagnostic yield of methylene blue chromoendoscopy for detecting specialized intestinal metaplasia and dysplasia in Barrett’s esophagus: a meta-analysis. Gastrointest Endosc. 2009;69:1021–1028. doi: 10.1016/j.gie.2008.06.056. [DOI] [PubMed] [Google Scholar]
- 68.Davies J, Burke D, Olliver JR, Hardie LJ, Wild CP, Routledge MN. Methylene blue but not indigo carmine causes DNA damage to colonocytes in vitro and in vivo at concentrations used in clinical chromoendoscopy. Gut. 2007;56:155–156. doi: 10.1136/gut.2006.107300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Kara MA, Peters FP, Rosmolen WD, Krishnadath KK, ten Kate FJ, Fockens P, Bergman JJ. High-resolution endoscopy plus chromoendoscopy or narrow-band imaging in Barrett’s esophagus: a prospective randomized crossover study. Endoscopy. 2005;37:929–936. doi: 10.1055/s-2005-870433. [DOI] [PubMed] [Google Scholar]
- 70.Sharma P, Bansal A, Mathur S, Wani S, Cherian R, McGregor D, Higbee A, Hall S, Weston A. The utility of a novel narrow band imaging endoscopy system in patients with Barrett’s esophagus. Gastrointest Endosc. 2006;64:167–175. doi: 10.1016/j.gie.2005.10.044. [DOI] [PubMed] [Google Scholar]
- 71.Mannath J, Subramanian V, Hawkey CJ, Ragunath K. Narrow band imaging for characterization of high grade dysplasia and specialized intestinal metaplasia in Barrett’s esophagus: a meta-analysis. Endoscopy. 2010;42:351–359. doi: 10.1055/s-0029-1243949. [DOI] [PubMed] [Google Scholar]
- 72.Sharma P, Hawes RH, Bansal A, Gupta N, Curvers W, Rastogi A, Singh M, Hall M, Mathur SC, Wani SB, et al. Standard endoscopy with random biopsies versus narrow band imaging targeted biopsies in Barrett’s oesophagus: a prospective, international, randomised controlled trial. Gut. 2013;62:15–21. doi: 10.1136/gutjnl-2011-300962. [DOI] [PubMed] [Google Scholar]
- 73.Curvers WL, Bohmer CJ, Mallant-Hent RC, Naber AH, Ponsioen CI, Ragunath K, Singh R, Wallace MB, Wolfsen HC, Song LM, et al. Mucosal morphology in Barrett’s esophagus: interobserver agreement and role of narrow band imaging. Endoscopy. 2008;40:799–805. doi: 10.1055/s-2008-1077596. [DOI] [PubMed] [Google Scholar]
- 74.Kara MA, Peters FP, Fockens P, ten Kate FJ, Bergman JJ. Endoscopic video-autofluorescence imaging followed by narrow band imaging for detecting early neoplasia in Barrett’s esophagus. Gastrointest Endosc. 2006;64:176–185. doi: 10.1016/j.gie.2005.11.050. [DOI] [PubMed] [Google Scholar]
- 75.Curvers WL, Alvarez Herrero L, Wallace MB, Wong Kee Song LM, Ragunath K, Wolfsen HC, Prasad GA, Wang KK, Subramanian V, Weusten BL, et al. Endoscopic tri-modal imaging is more effective than standard endoscopy in identifying early-stage neoplasia in Barrett’s esophagus. Gastroenterology. 2010;139:1106–1114. doi: 10.1053/j.gastro.2010.06.045. [DOI] [PubMed] [Google Scholar]
- 76.Curvers WL, van Vilsteren FG, Baak LC, Böhmer C, Mallant-Hent RC, Naber AH, van Oijen A, Ponsioen CY, Scholten P, Schenk E, et al. Endoscopic trimodal imaging versus standard video endoscopy for detection of early Barrett’s neoplasia: a multicenter, randomized, crossover study in general practice. Gastrointest Endosc. 2011;73:195–203. doi: 10.1016/j.gie.2010.10.014. [DOI] [PubMed] [Google Scholar]
- 77.Wallace MB, Perelman LT, Backman V, Crawford JM, Fitzmaurice M, Seiler M, Badizadegan K, Shields SJ, Itzkan I, Dasari RR, et al. Endoscopic detection of dysplasia in patients with Barrett’s esophagus using light-scattering spectroscopy. Gastroenterology. 2000;119:677–682. doi: 10.1053/gast.2000.16511. [DOI] [PubMed] [Google Scholar]
- 78.Evans JA, Poneros JM, Bouma BE, Bressner J, Halpern EF, Shishkov M, Lauwers GY, Mino-Kenudson M, Nishioka NS, Tearney GJ. Optical coherence tomography to identify intramucosal carcinoma and high-grade dysplasia in Barrett’s esophagus. Clin Gastroenterol Hepatol. 2006;4:38–43. doi: 10.1053/S1542-3565(05)00746-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Hoffman A, Kiesslich R, Bender A, Neurath MF, Nafe B, Herrmann G, Jung M. Acetic acid-guided biopsies after magnifying endoscopy compared with random biopsies in the detection of Barrett’s esophagus: a prospective randomized trial with crossover design. Gastrointest Endosc. 2006;64:1–8. doi: 10.1016/j.gie.2005.09.031. [DOI] [PubMed] [Google Scholar]
- 80.Ferguson DD, DeVault KR, Krishna M, Loeb DS, Wolfsen HC, Wallace MB. Enhanced magnification-directed biopsies do not increase the detection of intestinal metaplasia in patients with GERD. Am J Gastroenterol. 2006;101:1611–1616. doi: 10.1111/j.1572-0241.2006.00622.x. [DOI] [PubMed] [Google Scholar]
- 81.Longcroft-Wheaton G, Duku M, Mead R, Poller D, Bhandari P. Acetic acid spray is an effective tool for the endoscopic detection of neoplasia in patients with Barrett’s esophagus. Clin Gastroenterol Hepatol. 2010;8:843–847. doi: 10.1016/j.cgh.2010.06.016. [DOI] [PubMed] [Google Scholar]
- 82.Pohl J, Pech O, May A, Manner H, Fissler-Eckhoff A, Ell C. Incidence of macroscopically occult neoplasias in Barrett’s esophagus: are random biopsies dispensable in the era of advanced endoscopic imaging? Am J Gastroenterol. 2010;105:2350–2356. doi: 10.1038/ajg.2010.280. [DOI] [PubMed] [Google Scholar]
- 83.Bhandari P, Kandaswamy P, Cowlishaw D, Longcroft-Wheaton G. Acetic acid-enhanced chromoendoscopy is more cost-effective than protocol-guided biopsies in a high-risk Barrett’s population. Dis Esophagus. 2012;25:386–392. doi: 10.1111/j.1442-2050.2011.01267.x. [DOI] [PubMed] [Google Scholar]
- 84.Sharma P, Meining AR, Coron E, Lightdale CJ, Wolfsen HC, Bansal A, Bajbouj M, Galmiche JP, Abrams JA, Rastogi A, et al. Real-time increased detection of neoplastic tissue in Barrett’s esophagus with probe-based confocal laser endomicroscopy: final results of an international multicenter, prospective, randomized, controlled trial. Gastrointest Endosc. 2011;74:465–472. doi: 10.1016/j.gie.2011.04.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Canto MI, Anandasabapathy S, Brugge W, Falk GW, Dunbar KB, Zhang Z, Woods K, Almario JA, Schell U, Goldblum J, et al. In vivo endomicroscopy improves detection of Barrett’s esophagus-related neoplasia: a multicenter international randomized controlled trial (with video) Gastrointest Endosc. 2014;79:211–221. doi: 10.1016/j.gie.2013.09.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Bird-Lieberman EL, Neves AA, Lao-Sirieix P, O’Donovan M, Novelli M, Lovat LB, Eng WS, Mahal LK, Brindle KM, Fitzgerald RC. Molecular imaging using fluorescent lectins permits rapid endoscopic identification of dysplasia in Barrett’s esophagus. Nat Med. 2012;18:315–321. doi: 10.1038/nm.2616. [DOI] [PubMed] [Google Scholar]
- 87.Li M, Anastassiades CP, Joshi B, Komarck CM, Piraka C, Elmunzer BJ, Turgeon DK, Johnson TD, Appelman H, Beer DG, et al. Affinity peptide for targeted detection of dysplasia in Barrett’s esophagus. Gastroenterology. 2010;139:1472–1480. doi: 10.1053/j.gastro.2010.07.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Sturm MB, Joshi BP, Lu S, Piraka C, Khondee S, Elmunzer BJ, Kwon RS, Beer DG, Appelman HD, Turgeon DK, et al. Targeted imaging of esophageal neoplasia with a fluorescently labeled peptide: first-in-human results. Sci Transl Med. 2013;5:184ra61. doi: 10.1126/scitranslmed.3004733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Bhat SK, McManus DT, Coleman HG, Johnston BT, Cardwell CR, McMenamin U, Bannon F, Hicks B, Kennedy G, Gavin AT, et al. Oesophageal adenocarcinoma and prior diagnosis of Barrett’s oesophagus: a population-based study. Gut. 2015;64:20–25. doi: 10.1136/gutjnl-2013-305506. [DOI] [PubMed] [Google Scholar]
- 90.Bennett C, Moayyedi P, Corley DA, DeCaestecker J, Falck-Ytter Y, Falk G, Vakil N, Sanders S, Vieth M, Inadomi J, et al. BOB CAT: A Large-Scale Review and Delphi Consensus for Management of Barrett’s Esophagus With No Dysplasia, Indefinite for, or Low-Grade Dysplasia. Am J Gastroenterol. 2015;110:662–682; quiz 683. doi: 10.1038/ajg.2015.55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Alashkar B, Faulx AL, Hepner A, Pulice R, Vemana S, Greer KB, Isenberg GA, Falck-Ytter Y, Chak A. Development of a program to train physician extenders to perform transnasal esophagoscopy and screen for Barrett’s esophagus. Clin Gastroenterol Hepatol. 2014;12:785–792. doi: 10.1016/j.cgh.2013.10.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Shariff MK, Bird-Lieberman EL, O’Donovan M, Abdullahi Z, Liu X, Blazeby J, Fitzgerald R. Randomized crossover study comparing efficacy of transnasal endoscopy with that of standard endoscopy to detect Barrett’s esophagus. Gastrointest Endosc. 2012;75:954–961. doi: 10.1016/j.gie.2012.01.029. [DOI] [PubMed] [Google Scholar]
- 93.Kadri SR, Lao-Sirieix P, O’Donovan M, Debiram I, Das M, Blazeby JM, Emery J, Boussioutas A, Morris H, Walter FM, et al. Acceptability and accuracy of a non-endoscopic screening test for Barrett’s oesophagus in primary care: cohort study. BMJ. 2010;341:c4372. doi: 10.1136/bmj.c4372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Lao-Sirieix P, Boussioutas A, Kadri SR, O’Donovan M, Debiram I, Das M, Harihar L, Fitzgerald RC. Non-endoscopic screening biomarkers for Barrett’s oesophagus: from microarray analysis to the clinic. Gut. 2009;58:1451–1459. doi: 10.1136/gut.2009.180281. [DOI] [PubMed] [Google Scholar]
- 95.Benaglia T, Sharples LD, Fitzgerald RC, Lyratzopoulos G. Health benefits and cost effectiveness of endoscopic and nonendoscopic cytosponge screening for Barrett’s esophagus. Gastroenterology. 2013;144:62–73.e6. doi: 10.1053/j.gastro.2012.09.060. [DOI] [PubMed] [Google Scholar]
- 96.Thrift AP, Garcia JM, El-Serag HB. A multibiomarker risk score helps predict risk for Barrett’s esophagus. Clin Gastroenterol Hepatol. 2014;12:1267–1271. doi: 10.1016/j.cgh.2013.12.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Corley DA, Levin TR, Habel LA, Weiss NS, Buffler PA. Surveillance and survival in Barrett’s adenocarcinomas: a population-based study. Gastroenterology. 2002;122:633–640. doi: 10.1053/gast.2002.31879. [DOI] [PubMed] [Google Scholar]
- 98.Aldulaimi DM, Cox M, Nwokolo CU, Loft DE. Barrett’s surveillance is worthwhile and detects curable cancers. A prospective cohort study addressing cancer incidence, treatment outcome and survival. Eur J Gastroenterol Hepatol. 2005;17:943–950. doi: 10.1097/00042737-200509000-00010. [DOI] [PubMed] [Google Scholar]
- 99.Gaddam S, Singh M, Balasubramanian G, Thota P, Gupta N, Wani S, Higbee AD, Mathur SC, Horwhat JD, Rastogi A, et al. Persistence of nondysplastic Barrett’s esophagus identifies patients at lower risk for esophageal adenocarcinoma: results from a large multicenter cohort. Gastroenterology. 2013;145:548–553.e1. doi: 10.1053/j.gastro.2013.05.040. [DOI] [PubMed] [Google Scholar]
- 100.Evans JA, Early DS, Fukami N, Ben-Menachem T, Chandrasekhara V, Chathadi KV, Decker GA, Fanelli RD, Fisher DA, Foley KQ, et al. The role of endoscopy in Barrett’s esophagus and other premalignant conditions of the esophagus. Gastrointest Endosc. 2012;76:1087–1094. doi: 10.1016/j.gie.2012.08.004. [DOI] [PubMed] [Google Scholar]
- 101.Shaheen NJ, Weinberg DS, Denberg TD, Chou R, Qaseem A, Shekelle P. Upper endoscopy for gastroesophageal reflux disease: best practice advice from the clinical guidelines committee of the American College of Physicians. Ann Intern Med. 2012;157:808–816. doi: 10.7326/0003-4819-157-11-201212040-00008. [DOI] [PubMed] [Google Scholar]
- 102.Horvath B, Singh P, Xie H, Thota PN, Allende DS, Pai RK, Patil DT, Plesec TP, Goldblum JR, Liu X. Risk for esophageal neoplasia in Barrett’s esophagus patients with mucosal changes indefinite for dysplasia. J Gastroenterol Hepatol. 2015;30:262–267. doi: 10.1111/jgh.12696. [DOI] [PubMed] [Google Scholar]
- 103.Younes M, Lauwers GY, Ertan A, Ergun G, Verm R, Bridges M, Woods K, Meriano F, Schmulen C, Johnson C, et al. The significance of “indefinite for dysplasia” grading in Barrett metaplasia. Arch Pathol Lab Med. 2011;135:430–432. doi: 10.5858/2010-0097-OA.1. [DOI] [PubMed] [Google Scholar]
- 104.Singh S, Manickam P, Amin AV, Samala N, Schouten LJ, Iyer PG, Desai TK. Incidence of esophageal adenocarcinoma in Barrett’s esophagus with low-grade dysplasia: a systematic review and meta-analysis. Gastrointest Endosc. 2014;79:897–909.e4; quiz 983.e1, 983.e3. doi: 10.1016/j.gie.2014.01.009. [DOI] [PubMed] [Google Scholar]
- 105.Wani S, Falk GW, Post J, Yerian L, Hall M, Wang A, Gupta N, Gaddam S, Singh M, Singh V, et al. Risk factors for progression of low-grade dysplasia in patients with Barrett’s esophagus. Gastroenterology. 2011;141:1179–1186, 1186.e1. doi: 10.1053/j.gastro.2011.06.055. [DOI] [PubMed] [Google Scholar]
- 106.Kaye PV, Haider SA, Ilyas M, James PD, Soomro I, Faisal W, Catton J, Parsons SL, Ragunath K. Barrett’s dysplasia and the Vienna classification: reproducibility, prediction of progression and impact of consensus reporting and p53 immunohistochemistry. Histopathology. 2009;54:699–712. doi: 10.1111/j.1365-2559.2009.03288.x. [DOI] [PubMed] [Google Scholar]
- 107.Duits LC, Phoa KN, Curvers WL, Ten Kate FJ, Meijer GA, Seldenrijk CA, Offerhaus GJ, Visser M, Meijer SL, Krishnadath KK, et al. Barrett’s oesophagus patients with low-grade dysplasia can be accurately risk-stratified after histological review by an expert pathology panel. Gut. 2015;64:700–706. doi: 10.1136/gutjnl-2014-307278. [DOI] [PubMed] [Google Scholar]
- 108.Abdalla M, Dhanekula R, Greenspan M, Mobarhan S, Patil A, Jakate S, Giusto D, Silva R, Li H, Melson J. Dysplasia detection rate of confirmatory EGD in nondysplastic Barrett’s esophagus. Dis Esophagus. 2014;27:505–510. doi: 10.1111/j.1442-2050.2012.01431.x. [DOI] [PubMed] [Google Scholar]
- 109.Brown CS, Lapin B, Wang C, Goldstein JL, Linn JG, Denham W, Haggerty SP, Talamonti MS, Howington JA, Carbray J, et al. Reflux control is important in the management of Barrett’s Esophagus: results from a retrospective 1,830 patient cohort. Surg Endosc. 2015;29:3528–3534. doi: 10.1007/s00464-015-4103-3. [DOI] [PubMed] [Google Scholar]
- 110.Singh S, Garg SK, Singh PP, Iyer PG, El-Serag HB. Acid-suppressive medications and risk of oesophageal adenocarcinoma in patients with Barrett’s oesophagus: a systematic review and meta-analysis. Gut. 2014;63:1229–1237. doi: 10.1136/gutjnl-2013-305997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Islami F, Kamangar F, Boffetta P. Use of proton pump inhibitors and risk of progression of Barrett’s esophagus to neoplastic lesions. Am J Gastroenterol. 2009;104:2646–2648. doi: 10.1038/ajg.2009.369. [DOI] [PubMed] [Google Scholar]
- 112.Ouatu-Lascar R, Fitzgerald RC, Triadafilopoulos G. Differentiation and proliferation in Barrett’s esophagus and the effects of acid suppression. Gastroenterology. 1999;117:327–335. doi: 10.1053/gast.1999.0029900327. [DOI] [PubMed] [Google Scholar]
- 113.de Bortoli N, Martinucci I, Piaggi P, Maltinti S, Bianchi G, Ciancia E, Gambaccini D, Lenzi F, Costa F, Leonardi G, et al. Randomised clinical trial: twice daily esomeprazole 40 mg vs. pantoprazole 40 mg in Barrett’s oesophagus for 1 year. Aliment Pharmacol Ther. 2011;33:1019–1027. doi: 10.1111/j.1365-2036.2011.04616.x. [DOI] [PubMed] [Google Scholar]
- 114.Kedika RR, Souza RF, Spechler SJ. Potential anti-inflammatory effects of proton pump inhibitors: a review and discussion of the clinical implications. Dig Dis Sci. 2009;54:2312–2317. doi: 10.1007/s10620-009-0951-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Nguyen DM, Richardson P, El-Serag HB. Medications (NSAIDs, statins, proton pump inhibitors) and the risk of esophageal adenocarcinoma in patients with Barrett’s esophagus. Gastroenterology. 2010;138:2260–2266. doi: 10.1053/j.gastro.2010.02.045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Richter JE, Penagini R, Tenca A, Pohl D, Dvorak K, Goldman A, Savarino E, Zentilin P, Savarino V, Watson JT, et al. Barrett’s esophagus: proton pump inhibitors and chemoprevention II. Ann N Y Acad Sci. 2011;1232:114–139. doi: 10.1111/j.1749-6632.2011.06048.x. [DOI] [PubMed] [Google Scholar]
- 117.Das D, Chilton AP, Jankowski JA. Chemoprevention of oesophageal cancer and the AspECT trial. Recent Results Cancer Res. 2009;181:161–169. doi: 10.1007/978-3-540-69297-3_15. [DOI] [PubMed] [Google Scholar]
- 118.Wang KK, Sampliner RE. Updated guidelines 2008 for the diagnosis, surveillance and therapy of Barrett’s esophagus. Am J Gastroenterol. 2008;103:788–797. doi: 10.1111/j.1572-0241.2008.01835.x. [DOI] [PubMed] [Google Scholar]
- 119.Blevins CH, Iyer PG. Endoscopic therapy for Barrett’s oesophagus. Best Pract Res Clin Gastroenterol. 2015;29:167–177. doi: 10.1016/j.bpg.2014.11.007. [DOI] [PubMed] [Google Scholar]
- 120.Bennett C, Vakil N, Bergman J, Harrison R, Odze R, Vieth M, Sanders S, Gay L, Pech O, Longcroft-Wheaton G, et al. Consensus statements for management of Barrett’s dysplasia and early-stage esophageal adenocarcinoma, based on a Delphi process. Gastroenterology. 2012;143:336–346. doi: 10.1053/j.gastro.2012.04.032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Perry KA, Enestvedt CK, Pham T, Welker M, Jobe BA, Hunter JG, Sheppard BC. Comparison of laparoscopic inversion esophagectomy and open transhiatal esophagectomy for high-grade dysplasia and stage I esophageal adenocarcinoma. Arch Surg. 2009;144:679–684. doi: 10.1001/archsurg.2009.113. [DOI] [PubMed] [Google Scholar]
- 122.Stahl M, Mariette C, Haustermans K, Cervantes A, Arnold D. Oesophageal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24 Suppl 6:vi51–vi56. doi: 10.1093/annonc/mdt342. [DOI] [PubMed] [Google Scholar]
- 123.Evans JA, Early DS, Chandraskhara V, Chathadi KV, Fanelli RD, Fisher DA, Foley KQ, Hwang JH, Jue TL, Pasha SF, et al. The role of endoscopy in the assessment and treatment of esophageal cancer. Gastrointest Endosc. 2013;77:328–334. doi: 10.1016/j.gie.2012.10.001. [DOI] [PubMed] [Google Scholar]
- 124.Pech O, Behrens A, May A, Nachbar L, Gossner L, Rabenstein T, Manner H, Guenter E, Huijsmans J, Vieth M, et al. Long-term results and risk factor analysis for recurrence after curative endoscopic therapy in 349 patients with high-grade intraepithelial neoplasia and mucosal adenocarcinoma in Barrett’s oesophagus. Gut. 2008;57:1200–1206. doi: 10.1136/gut.2007.142539. [DOI] [PubMed] [Google Scholar]
- 125.Prasad GA, Wu TT, Wigle DA, Buttar NS, Wongkeesong LM, Dunagan KT, Lutzke LS, Borkenhagen LS, Wang KK. Endoscopic and surgical treatment of mucosal (T1a) esophageal adenocarcinoma in Barrett’s esophagus. Gastroenterology. 2009;137:815–823. doi: 10.1053/j.gastro.2009.05.059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Das A, Singh V, Fleischer DE, Sharma VK. A comparison of endoscopic treatment and surgery in early esophageal cancer: an analysis of surveillance epidemiology and end results data. Am J Gastroenterol. 2008;103:1340–1345. doi: 10.1111/j.1572-0241.2008.01889.x. [DOI] [PubMed] [Google Scholar]
- 127.Zehetner J, DeMeester SR, Hagen JA, Ayazi S, Augustin F, Lipham JC, DeMeester TR. Endoscopic resection and ablation versus esophagectomy for high-grade dysplasia and intramucosal adenocarcinoma. J Thorac Cardiovasc Surg. 2011;141:39–47. doi: 10.1016/j.jtcvs.2010.08.058. [DOI] [PubMed] [Google Scholar]
- 128.Wani S, Mathur SC, Curvers WL, Singh V, Alvarez Herrero L, Hall SB, Ulusarac O, Cherian R, McGregor DH, Bansal A, et al. Greater interobserver agreement by endoscopic mucosal resection than biopsy samples in Barrett’s dysplasia. Clin Gastroenterol Hepatol. 2010;8:783–788. doi: 10.1016/j.cgh.2010.04.028. [DOI] [PubMed] [Google Scholar]
- 129.Wani S, Abrams J, Edmundowicz SA, Gaddam S, Hovis CE, Green D, Gupta N, Higbee A, Bansal A, Rastogi A, et al. Endoscopic mucosal resection results in change of histologic diagnosis in Barrett’s esophagus patients with visible and flat neoplasia: a multicenter cohort study. Dig Dis Sci. 2013;58:1703–1709. doi: 10.1007/s10620-013-2689-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Mino-Kenudson M, Hull MJ, Brown I, Muzikansky A, Srivastava A, Glickman J, Park DY, Zuckerberg L, Misdraji J, Odze RD, et al. EMR for Barrett’s esophagus-related superficial neoplasms offers better diagnostic reproducibility than mucosal biopsy. Gastrointest Endosc. 2007;66:660–666; quiz 767, 769. doi: 10.1016/j.gie.2007.02.063. [DOI] [PubMed] [Google Scholar]
- 131.Leggett CL, Lewis JT, Wu TT, Schleck CD, Zinsmeister AR, Dunagan KT, Lutzke LS, Wang KK, Iyer PG. Clinical and histologic determinants of mortality for patients with Barrett’s esophagus-related T1 esophageal adenocarcinoma. Clin Gastroenterol Hepatol. 2015;13:658–664.e1-3. doi: 10.1016/j.cgh.2014.08.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Davila ML, Hofstetter WL. Endoscopic management of Barrett’s esophagus with high-grade dysplasia and early-stage esophageal adenocarcinoma. Thorac Surg Clin. 2013;23:479–489. doi: 10.1016/j.thorsurg.2013.07.010. [DOI] [PubMed] [Google Scholar]
- 133.Spechler SJ, Sharma P, Souza RF, Inadomi JM, Shaheen NJ. American Gastroenterological Association technical review on the management of Barrett’s esophagus. Gastroenterology. 2011;140:e18–52; quiz e13. doi: 10.1053/j.gastro.2011.01.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Pouw RE, van Vilsteren FG, Peters FP, Alvarez Herrero L, Ten Kate FJ, Visser M, Schenk BE, Schoon EJ, Peters FT, Houben M, et al. Randomized trial on endoscopic resection-cap versus multiband mucosectomy for piecemeal endoscopic resection of early Barrett’s neoplasia. Gastrointest Endosc. 2011;74:35–43. doi: 10.1016/j.gie.2011.03.1243. [DOI] [PubMed] [Google Scholar]
- 135.Ell C, May A, Pech O, Gossner L, Guenter E, Behrens A, Nachbar L, Huijsmans J, Vieth M, Stolte M. Curative endoscopic resection of early esophageal adenocarcinomas (Barrett’s cancer) Gastrointest Endosc. 2007;65:3–10. doi: 10.1016/j.gie.2006.04.033. [DOI] [PubMed] [Google Scholar]
- 136.May A, Gossner L, Pech O, Fritz A, Günter E, Mayer G, Müller H, Seitz G, Vieth M, Stolte M, et al. Local endoscopic therapy for intraepithelial high-grade neoplasia and early adenocarcinoma in Barrett’s oesophagus: acute-phase and intermediate results of a new treatment approach. Eur J Gastroenterol Hepatol. 2002;14:1085–1091. doi: 10.1097/00042737-200210000-00009. [DOI] [PubMed] [Google Scholar]
- 137.Pech O, May A, Manner H, Behrens A, Pohl J, Weferling M, Hartmann U, Manner N, Huijsmans J, Gossner L, et al. Long-term efficacy and safety of endoscopic resection for patients with mucosal adenocarcinoma of the esophagus. Gastroenterology. 2014;146:652–660.e1. doi: 10.1053/j.gastro.2013.11.006. [DOI] [PubMed] [Google Scholar]
- 138.Moss A, Bourke MJ, Hourigan LF, Gupta S, Williams SJ, Tran K, Swan MP, Hopper AD, Kwan V, Bailey AA. Endoscopic resection for Barrett’s high-grade dysplasia and early esophageal adenocarcinoma: an essential staging procedure with long-term therapeutic benefit. Am J Gastroenterol. 2010;105:1276–1283. doi: 10.1038/ajg.2010.1. [DOI] [PubMed] [Google Scholar]
- 139.Gerke H, Siddiqui J, Nasr I, Van Handel DM, Jensen CS. Efficacy and safety of EMR to completely remove Barrett’s esophagus: experience in 41 patients. Gastrointest Endosc. 2011;74:761–771. doi: 10.1016/j.gie.2011.06.009. [DOI] [PubMed] [Google Scholar]
- 140.Yoshinaga S, Gotoda T, Kusano C, Oda I, Nakamura K, Takayanagi R. Clinical impact of endoscopic submucosal dissection for superficial adenocarcinoma located at the esophagogastric junction. Gastrointest Endosc. 2008;67:202–209. doi: 10.1016/j.gie.2007.09.054. [DOI] [PubMed] [Google Scholar]
- 141.Teoh AY, Chiu PW, Yu Ngo DK, Wong SK, Lau JY, Ng EK. Outcomes of endoscopic submucosal dissection versus endoscopic mucosal resection in management of superficial squamous esophageal neoplasms outside Japan. J Clin Gastroenterol. 2010;44:e190–e194. doi: 10.1097/MCG.0b013e3181ce52fb. [DOI] [PubMed] [Google Scholar]
- 142.Repici A, Hassan C, Carlino A, Pagano N, Zullo A, Rando G, Strangio G, Romeo F, Nicita R, Rosati R, et al. Endoscopic submucosal dissection in patients with early esophageal squamous cell carcinoma: results from a prospective Western series. Gastrointest Endosc. 2010;71:715–721. doi: 10.1016/j.gie.2009.11.020. [DOI] [PubMed] [Google Scholar]
- 143.Chennat J, Konda VJ, Ross AS, de Tejada AH, Noffsinger A, Hart J, Lin S, Ferguson MK, Posner MC, Waxman I. Complete Barrett’s eradication endoscopic mucosal resection: an effective treatment modality for high-grade dysplasia and intramucosal carcinoma--an American single-center experience. Am J Gastroenterol. 2009;104:2684–2692. doi: 10.1038/ajg.2009.465. [DOI] [PubMed] [Google Scholar]
- 144.Hashimoto S, Kobayashi M, Takeuchi M, Sato Y, Narisawa R, Aoyagi Y. The efficacy of endoscopic triamcinolone injection for the prevention of esophageal stricture after endoscopic submucosal dissection. Gastrointest Endosc. 2011;74:1389–1393. doi: 10.1016/j.gie.2011.07.070. [DOI] [PubMed] [Google Scholar]
- 145.Shaheen NJ, Sharma P, Overholt BF, Wolfsen HC, Sampliner RE, Wang KK, Galanko JA, Bronner MP, Goldblum JR, Bennett AE, et al. Radiofrequency ablation in Barrett’s esophagus with dysplasia. N Engl J Med. 2009;360:2277–2288. doi: 10.1056/NEJMoa0808145. [DOI] [PubMed] [Google Scholar]
- 146.Shaheen NJ, Overholt BF, Sampliner RE, Wolfsen HC, Wang KK, Fleischer DE, Sharma VK, Eisen GM, Fennerty MB, Hunter JG, et al. Durability of radiofrequency ablation in Barrett’s esophagus with dysplasia. Gastroenterology. 2011;141:460–468. doi: 10.1053/j.gastro.2011.04.061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147.Phoa KN, van Vilsteren FG, Weusten BL, Bisschops R, Schoon EJ, Ragunath K, Fullarton G, Di Pietro M, Ravi N, Visser M, et al. Radiofrequency ablation vs endoscopic surveillance for patients with Barrett esophagus and low-grade dysplasia: a randomized clinical trial. JAMA. 2014;311:1209–1217. doi: 10.1001/jama.2014.2511. [DOI] [PubMed] [Google Scholar]
- 148.Orman ES, Li N, Shaheen NJ. Efficacy and durability of radiofrequency ablation for Barrett’s Esophagus: systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2013;11:1245–1255. doi: 10.1016/j.cgh.2013.03.039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149.Bulsiewicz WJ, Kim HP, Dellon ES, Cotton CC, Pasricha S, Madanick RD, Spacek MB, Bream SE, Chen X, Orlando RC, et al. Safety and efficacy of endoscopic mucosal therapy with radiofrequency ablation for patients with neoplastic Barrett’s esophagus. Clin Gastroenterol Hepatol. 2013;11:636–642. doi: 10.1016/j.cgh.2012.10.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.Prasad GA, Wang KK, Halling KC, Buttar NS, Wongkeesong LM, Zinsmeister AR, Brankley SM, Fritcher EG, Westra WM, Krishnadath KK, et al. Utility of biomarkers in prediction of response to ablative therapy in Barrett’s esophagus. Gastroenterology. 2008;135:370–379. doi: 10.1053/j.gastro.2008.04.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.Krishnan K, Pandolfino JE, Kahrilas PJ, Keefer L, Boris L, Komanduri S. Increased risk for persistent intestinal metaplasia in patients with Barrett’s esophagus and uncontrolled reflux exposure before radiofrequency ablation. Gastroenterology. 2012;143:576–581. doi: 10.1053/j.gastro.2012.05.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 152.Timmer MR, Brankley SM, Gorospe EC, Sun G, Lutzke LS, Iyer PG, Halling KC, Krishnadath KK, Wang KK. Prediction of response to endoscopic therapy of Barrett’s dysplasia by using genetic biomarkers. Gastrointest Endosc. 2014;80:984–991. doi: 10.1016/j.gie.2014.06.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Gray NA, Odze RD, Spechler SJ. Buried metaplasia after endoscopic ablation of Barrett’s esophagus: a systematic review. Am J Gastroenterol. 2011;106:1899–1908; quiz 1909. doi: 10.1038/ajg.2011.255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 154.Gupta N, Mathur SC, Dumot JA, Singh V, Gaddam S, Wani SB, Bansal A, Rastogi A, Goldblum JR, Sharma P. Adequacy of esophageal squamous mucosa specimens obtained during endoscopy: are standard biopsies sufficient for postablation surveillance in Barrett’s esophagus? Gastrointest Endosc. 2012;75:11–18. doi: 10.1016/j.gie.2011.06.040. [DOI] [PubMed] [Google Scholar]
- 155.Dulai PS, Pohl H, Levenick JM, Gordon SR, MacKenzie TA, Rothstein RI. Radiofrequency ablation for long- and ultralong-segment Barrett’s esophagus: a comparative long-term follow-up study. Gastrointest Endosc. 2013;77:534–541. doi: 10.1016/j.gie.2012.10.021. [DOI] [PubMed] [Google Scholar]
- 156.Gosain S, Mercer K, Twaddell WS, Uradomo L, Greenwald BD. Liquid nitrogen spray cryotherapy in Barrett’s esophagus with high-grade dysplasia: long-term results. Gastrointest Endosc. 2013;78:260–265. doi: 10.1016/j.gie.2013.03.002. [DOI] [PubMed] [Google Scholar]
- 157.Fuchs KH, Babic B, Breithaupt W, Dallemagne B, Fingerhut A, Furnee E, Granderath F, Horvath P, Kardos P, Pointner R, et al. EAES recommendations for the management of gastroesophageal reflux disease. Surg Endosc. 2014;28:1753–1773. doi: 10.1007/s00464-014-3431-z. [DOI] [PubMed] [Google Scholar]
- 158.Galmiche JP, Hatlebakk J, Attwood S, Ell C, Fiocca R, Eklund S, Långström G, Lind T, Lundell L. Laparoscopic antireflux surgery vs esomeprazole treatment for chronic GERD: the LOTUS randomized clinical trial. JAMA. 2011;305:1969–1977. doi: 10.1001/jama.2011.626. [DOI] [PubMed] [Google Scholar]
- 159.Faria R, Bojke L, Epstein D, Corbacho B, Sculpher M. Cost-effectiveness of laparoscopic fundoplication versus continued medical management for the treatment of gastro-oesophageal reflux disease based on long-term follow-up of the REFLUX trial. Br J Surg. 2013;100:1205–1213. doi: 10.1002/bjs.9190. [DOI] [PubMed] [Google Scholar]
- 160.Strate U, Emmermann A, Fibbe C, Layer P, Zornig C. Laparoscopic fundoplication: Nissen versus Toupet two-year outcome of a prospective randomized study of 200 patients regarding preoperative esophageal motility. Surg Endosc. 2008;22:21–30. doi: 10.1007/s00464-007-9546-8. [DOI] [PubMed] [Google Scholar]
- 161.Zornig C, Strate U, Fibbe C, Emmermann A, Layer P. Nissen vs Toupet laparoscopic fundoplication. Surg Endosc. 2002;16:758–766. doi: 10.1007/s00464-001-9092-8. [DOI] [PubMed] [Google Scholar]
- 162.Patti MG, Robinson T, Galvani C, Gorodner MV, Fisichella PM, Way LW. Total fundoplication is superior to partial fundoplication even when esophageal peristalsis is weak. J Am Coll Surg. 2004;198:863–869; discussion 869-870. doi: 10.1016/j.jamcollsurg.2004.01.029. [DOI] [PubMed] [Google Scholar]
- 163.Dallemagne B, Weerts J, Markiewicz S, Dewandre JM, Wahlen C, Monami B, Jehaes C. Clinical results of laparoscopic fundoplication at ten years after surgery. Surg Endosc. 2006;20:159–165. doi: 10.1007/s00464-005-0174-x. [DOI] [PubMed] [Google Scholar]
- 164.Fein M, Bueter M, Thalheimer A, Pachmayr V, Heimbucher J, Freys SM, Fuchs KH. Less reflux recurrence following Nissen fundoplication : results of laparoscopic antireflux surgery after 10 years. Chirurg. 2008;79:759–764. doi: 10.1007/s00104-008-1532-8. [DOI] [PubMed] [Google Scholar]
- 165.Attwood SE, Lundell L, Hatlebakk JG, Eklund S, Junghard O, Galmiche JP, Ell C, Fiocca R, Lind T. Medical or surgical management of GERD patients with Barrett’s esophagus: the LOTUS trial 3-year experience. J Gastrointest Surg. 2008;12:1646–1654; discussion 1654-1655. doi: 10.1007/s11605-008-0645-1. [DOI] [PubMed] [Google Scholar]
- 166.Caygill CP, Watson A, Lao-Sirieix P, Fitzgerald RC. Barrett’s oesophagus and adenocarcinoma. World J Surg Oncol. 2004;2:12. doi: 10.1186/1477-7819-2-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 167.Avidan B, Sonnenberg A, Schnell TG, Chejfec G, Metz A, Sontag SJ. Hiatal hernia size, Barrett’s length, and severity of acid reflux are all risk factors for esophageal adenocarcinoma. Am J Gastroenterol. 2002;97:1930–1936. doi: 10.1111/j.1572-0241.2002.05902.x. [DOI] [PubMed] [Google Scholar]
- 168.Rossi M, Barreca M, de Bortoli N, Renzi C, Santi S, Gennai A, Bellini M, Costa F, Conio M, Marchi S. Efficacy of Nissen fundoplication versus medical therapy in the regression of low-grade dysplasia in patients with Barrett esophagus: a prospective study. Ann Surg. 2006;243:58–63. doi: 10.1097/01.sla.0000194085.56699.db. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 169.Zaninotto G, Parente P, Salvador R, Farinati F, Tieppo C, Passuello N, Zanatta L, Fassan M, Cavallin F, Costantini M, et al. Long-term follow-up of Barrett’s epithelium: medical versus antireflux surgical therapy. J Gastrointest Surg. 2012;16:7–14; discussion 14-15. doi: 10.1007/s11605-011-1739-8. [DOI] [PubMed] [Google Scholar]
- 170.Chang EY, Morris CD, Seltman AK, O’Rourke RW, Chan BK, Hunter JG, Jobe BA. The effect of antireflux surgery on esophageal carcinogenesis in patients with barrett esophagus: a systematic review. Ann Surg. 2007;246:11–21. doi: 10.1097/01.sla.0000261459.10565.e9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 171.Corey KE, Schmitz SM, Shaheen NJ. Does a surgical antireflux procedure decrease the incidence of esophageal adenocarcinoma in Barrett’s esophagus? A meta-analysis. Am J Gastroenterol. 2003;98:2390–2394. doi: 10.1111/j.1572-0241.2003.08702.x. [DOI] [PubMed] [Google Scholar]
- 172.Löfdahl HE, Lu Y, Lagergren P, Lagergren J. Risk factors for esophageal adenocarcinoma after antireflux surgery. Ann Surg. 2013;257:579–582. doi: 10.1097/SLA.0b013e3182888384. [DOI] [PubMed] [Google Scholar]
- 173.Sjoquist KM, Burmeister BH, Smithers BM, Zalcberg JR, Simes RJ, Barbour A, Gebski V. Survival after neoadjuvant chemotherapy or chemoradiotherapy for resectable oesophageal carcinoma: an updated meta-analysis. Lancet Oncol. 2011;12:681–692. doi: 10.1016/S1470-2045(11)70142-5. [DOI] [PubMed] [Google Scholar]
- 174.Ford AC, Forman D, Reynolds PD, Cooper BT, Moayyedi P. Ethnicity, gender, and socioeconomic status as risk factors for esophagitis and Barrett’s esophagus. Am J Epidemiol. 2005;162:454–460. doi: 10.1093/aje/kwi218. [DOI] [PubMed] [Google Scholar]
- 175.Conio M, Filiberti R, Blanchi S, Ferraris R, Marchi S, Ravelli P, Lapertosa G, Iaquinto G, Sablich R, Gusmaroli R, et al. Risk factors for Barrett’s esophagus: a case-control study. Int J Cancer. 2002;97:225–229. doi: 10.1002/ijc.1583. [DOI] [PubMed] [Google Scholar]
- 176.Zagari RM, Fuccio L, Wallander MA, Johansson S, Fiocca R, Casanova S, Farahmand BY, Winchester CC, Roda E, Bazzoli F. Gastro-oesophageal reflux symptoms, oesophagitis and Barrett’s oesophagus in the general population: the Loiano-Monghidoro study. Gut. 2008;57:1354–1359. doi: 10.1136/gut.2007.145177. [DOI] [PubMed] [Google Scholar]
- 177.Conio M, Blanchi S, Lapertosa G, Ferraris R, Sablich R, Marchi S, D’Onofrio V, Lacchin T, Iaquinto G, Missale G, et al. Long-term endoscopic surveillance of patients with Barrett’s esophagus. Incidence of dysplasia and adenocarcinoma: a prospective study. Am J Gastroenterol. 2003;98:1931–1939. doi: 10.1111/j.1572-0241.2003.07666.x. [DOI] [PubMed] [Google Scholar]