

Abstract
Aneurysms of azygos anterior cerebral artery (ACA) are rare with very few cases reported in medical literature. We report here two cases of aneurysm of azygos ACA among 105 patients with subarachnoid hemorrhage. The two aneurysms were successfully clipped by using the bifrontal basal interhemispheric approach.
Keywords: Azygos anterior cerebral artery, azygos distal anterior cerebral artery, intracranial aneurysm
Introduction
The azygos anterior cerebral artery (ACA), with an incidence of <1%,[1] is a rare anatomical anomaly in the circle of Willis. In this vascular anomaly, the distal segments (A2) of both ACAs are represented by a single vessel from which all major vessels arise to supply the medial aspect of cerebral hemispheres and corpus callosum. Given the rare anatomical variant, aneurysms of the azygos ACA are even rare.[2] We reviewed 105 consecutive cases of aneurysmal subarachnoid hemorrhage (SAH) with 110 intracranial aneurysms treated by the first author between September 2006 and August 2012. There were 8 distal ACA (DACA) aneurysms in this series, of which 2 (1.9%) were azygos ACA aneurysms. Here, we have described these two cases, which were treated by surgical clipping.
Case Reports
Case 1
A 60-year-old female presented with two day history of headache and vomiting. There was no past history of hypertension. The patient was conscious, alert, and moving all her extremities (Hunt and Hess grade II SAH). Computed tomography (CT) scan of the brain showed anterior interhemispheric hemorrhage. Magnetic resonance angiography (MRA) showed an azygos ACA with aneurysm at the bifurcation [Figure 1a, b]. Surgery was performed using the basal bifrontal interhemispheric approach following bifrontal craniotomy. Aneurysm at the bifurcation of azygos ACA was identified [Figure 2]. Temporary clipping of the proximal azygos ACA was done for 8 min and aneurysm neck was dissected, followed by permanent clipping of the aneurysm. Postoperatively, CT scan of the patient's brain revealed bilateral ACA infarcts. The patient had bilateral lower limb weakness (paraparesis) and aphasia, which gradually improved in 6 months. The Glasgow Outcome Scale (GOS) at 1 year of follow-up was 4.
Figure 1.
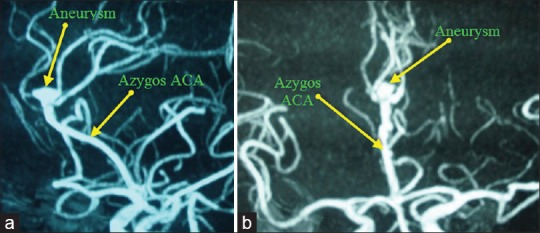
(a and b) 3D TOF MR Angio of circle of willis showing azygos ACA and aneurysm
Figure 2.
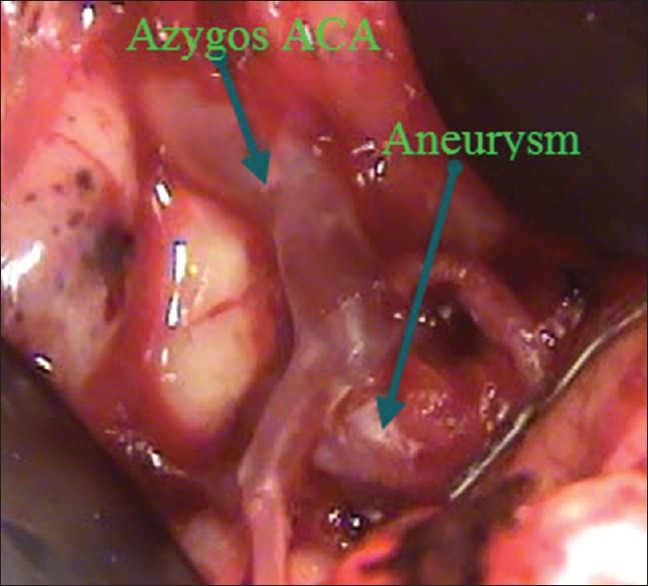
Intraoperative photograph showing azygos ACA and aneurysm at its bifurcation
Case 2
A 45-year-old female presented with a history of sudden onset of severe headache and transient loss of consciousness. She had no previous history of hypertension or diabetes. The patient was conscious and alert with no neurological deficit (Hunt and Hess grade II SAH). CT scan of the brain showed SAH in anterior interhemispheric fissure and a small hematoma in the frontal lobe. CT cerebral angiogram (CTA) revealed an aneurysm at the bifurcation of azygos ACA [Figure 3a, b]. The aneurysm was clipped using the basal bifrontal interhemispheric approach. This patient required temporary clipping of the proximal azygos ACA for 6 min before permanent clipping of the aneurysm. Postoperatively, the patient had no neurological deficits and was conscious, alert, and ambulatory at the time of discharge. GOS score at 6 months of follow-up was 5.
Figure 3.
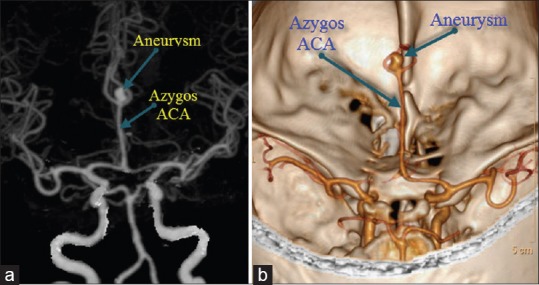
(a and b) CT Angio-MIP and 3D VR images showing azygos ACA and aneurysm at the bifurcation of ACA
Discussion
According to Yasargil, Wilder was the first to describe the fusion of both A2 segments of ACA to form a single artery and to introduce the term arteria termatica in 1885.[1] The presence of the unpaired, distal A2 segment of the ACA is named azygos ACA. This artery is also known as unpaired pericallosal artery or azygos pericallosal artery. Although the presence of unpaired ACA is common in lower mammals, it is uncommon in humans.[3] Baptista reviewed the literature and found that of the 2153 brains studied, 23 had azygos ACAs (1.06%).[4] In his own study of 381 brains, there was only one case of azygos ACA (0.26%). In contrast, Le May and Gooding reported four cases of azygos ACA in 107 consecutive carotid angiograms (3.73%).[3] In Huber et al.'s study of 7782 unselected angiographic cases, 17 had azygos ACA (0.21%).[5] Huh et al. reported three cases of azygos ACA aneurysms in a series of 781 consecutive patients of SAH (0.38%).[2] The incidence of azygos ACA in the general population can be assumed to be <1%, although the reported incidence varies from 0.21% to 3.73%.
Baptista defined three ACA variations.[4] In type I anomaly (true azygos ACA), there is only one azygos ACA from which all major branches spread to both the hemispheres. Type II anomaly is bihemispheric ACA, where both right and left ACA are present, but most of the major branches to the bilateral hemispheres arise from one ACA and the other one is rudimentary. In type III anomaly, a third artery (accessory ACA) arises from anterior communicating artery. Both cases in this report have type I anomaly. Digital substraction angiogram (DSA) was not performed in both these cases. In the first case, surgery was done on MRA findings and intraoperative findings confirmed the azygos nature of ACA [Figure 2]. In the second case, 3D CTA clearly demonstrated azygos ACA, which was confirmed during surgery.
Azygos ACA is also known to be associated with other midline malformations including agenesis of the corpus callosum, porencephalic cysts, holoprosencephaly, and saccular aneurysms.[6] Aneurysms of azygos ACA are rare, with only few cases reported in the literature. The mechanism of aneurysm formation in azygos ACA could be due to hemodynamic stress or because of a congenitally anomalous artery.[2] Although the incidence of azygos ACA anomaly is <1%, the incidence of aneurysms of pericallosal artery is higher in patients with azygos ACA, as postulated by Pool and Pots.[7] Katz et al. reviewed 36 cases of DACA aneurysms and found that 6 (17%) were associated with azygos ACA.[8] The incidence of aneurysm in azygos ACA varies from 13% to 71%.[2] In our series, 25% (2/8) cases of DACA aneurysms were associated with azygos ACA. Most of the reported cases of aneurysms of azygos ACA were described as saccular in nature.[9] Non-saccular aneurysms of azygos ACA have also been reported, which require complex clip application or multiple clips.[9]
Management of aneurysms of azygos ACA is by surgical clipping or by endovascular coiling. Most of the reported cases of azygos ACA aneurysms have been managed by surgical clipping. Endovascular coiling of azygos ACA aneurysm has been reported in few cases.[10] Both the cases in our report were clipped using the basal bifrontal interhemispheric approach and the aneurysm was seen at the bifurcation of the azygos ACA. Temporary clipping of the proximal A2 (ACA) is an essential adjunct for dissecting the aneurysm neck and final clip application.[9] Since this single vessel supplies to the bilateral medial cerebral hemispheres, temporary clipping of proximal azygos ACA can result in infarcts on both the sides. Temporary clipping of proximal azygos ACA was done in both the cases. Case 1 developed bilateral ACA infarcts and had delayed recovery, while case 2 had an uneventful recovery. It is difficult to ascertain the cause of this differential outcome in these two patients as both patients had grade II SAH and were operated by the same approach, although case 1 had temporary clipping of proximal A2 for longer duration than case 2. In view of the rarity of these aneurysms, need for temporary clipping, potential risk of developing bilateral infarcts, and the possibility of non-saccular aneurysms, surgeons should be prepared for judicious temporary clipping and for complex clip applications in cases of non-saccular aneurysms.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Ozkal E, Erongun U, Acar O, Kalkan E. Ruptured aneurysm of an azygous anterior cerebral artery. Turk Neurosurg. 1990;1:140–2. [Google Scholar]
- 2.Huh JS, Park SK, Shin JJ, Kim TH. Saccular aneurysm of the azygos anterior cerebral artery: Three case reports. J Korean Neurosurg Soc. 2007;42:342–5. doi: 10.3340/jkns.2007.42.4.342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.LeMay M, Gooding CA. The clinical significance of the azygous anterior cerebral artery (A.C.A) Am J Roentgenol Radium Ther Nucl Med. 1967;98:602–10. doi: 10.2214/ajr.98.3.602. [DOI] [PubMed] [Google Scholar]
- 4.Baptista AG. Studies on the arteries of the brain. II. The anterior cerebral artery: Some anatomic features and their clinical implications. Neurology. 1963;13:825–35. doi: 10.1212/wnl.13.10.825. [DOI] [PubMed] [Google Scholar]
- 5.Huber P, Braun J, Hirschmann D, Agyeman JF. Incidence of berry aneurysms of the unpaired pericallosal artery: Angiographic study. Neuroradiology. 1980;19:143–7. doi: 10.1007/BF00342389. [DOI] [PubMed] [Google Scholar]
- 6.Szdzuy D, Lehmann R, Nickel B. Common trunk of the anterior cerebral arteries. Neuroradiology. 1972;4:51–6. doi: 10.1007/BF00344810. [DOI] [PubMed] [Google Scholar]
- 7.Pool JL, Potts DG. New York: Harper and Row; 1965. Aneurysms and arteriovenous anomalies of the brain: Diagnosis and treatment; p. 463. [Google Scholar]
- 8.Katz RW, Horoupian DS, Zingesser L. Aneurysm of azygous anterior cerebral artery. A case report. J Neurosurg. 1978;48:804–8. doi: 10.3171/jns.1978.48.5.0804. [DOI] [PubMed] [Google Scholar]
- 9.Auguste KI, Ware ML, Lawton MT. Nonsaccular aneurysms of the azygos anterior cerebral artery. Neurosurg Focus. 2004;15-17:e12. doi: 10.3171/foc.2004.17.5.12. [DOI] [PubMed] [Google Scholar]
- 10.Sarikaya B, Oksuz E, Deniz FE, Firat MM. Endovascular treatment of a ruptured aneurysm at a very rare location. Distal azygos anterior cerebral artery. Interv Neuroradiol. 2008;14:457–60. doi: 10.1177/159101990801400413. [DOI] [PMC free article] [PubMed] [Google Scholar]