

Abstract
Background: We conducted a rigorous review of videos related to multiple sclerosis (MS) and chronic cerebrospinal venous insufficiency (CCSVI) treatment posted by people with MS on one social media website (YouTube) that describe symptoms before and after the surgical procedure, as well as videos presented by health-care professionals (HCPs).
Methods: All relevant videos posted from December 2009 to July 2011 were downloaded, viewed, and systematically organized. Categorical data were classified, and dominant messages were gleaned.
Results: A total of 1789 videos were extracted. A total of 621 videos by people with MS and 238 by HCPs were included. Eighty-six percent of people with MS anecdotally reported experiencing some improvement in at least one symptom. The most common message was that “CCSVI is not a miracle but worth trying.” Most HCPs posting videos recommended the procedure but called for continued research.
Conclusions: Social media are conveying an anecdotal favorable message about CCSVI treatment for MS. The relative absence of videos offering a negative or more balanced perspective is a concern. Social persuasion through these videos creates a strong positive impression of CCSVI treatment, but the videos do not acknowledge the lack of supporting scientific evidence and the possible role of the placebo effect. Given the strong influence of social media on health-care decision making, researchers and clinicians should actively use social media to reach out to people with MS and describe the state of the evidence for MS treatments, both positive and negative.
Chronic cerebrospinal venous insufficiency (CCSVI) has been proposed as the cause of or a contributing factor to multiple sclerosis (MS) disease progress and is a hot topic among health-care professionals (HCPs) and people with MS. The initial research conducted by Zamboni et al.1 identified CCSVI in all patients with MS in the study and in none of the control patients. Despite an international research effort to explore the accuracy of this claim, to date, there remains little to no evidence to support a significant relationship between CCSVI and MS symptoms,2–4 and debate continues.5–8 Several randomized controlled trials and systematic reviews have shown no clear evidence for the presence of CCSVI or the effects of suggested surgery.9 Therefore, organizations such as the Multiple Sclerosis Society of Canada, the National Multiple Sclerosis Society, and the Consortium of Multiple Sclerosis Centers have advised people with MS to use caution and explore the evidence. Still, many people with MS seek and undergo the surgical procedure. In countries such as Canada, where medical care is embedded in the national social system, there are considerable lobbying efforts to have this surgical procedure funded by public dollars. However, the Canadian government is yet to be convinced that this procedure is of benefit and will cause no harm to the public.
Topics and opinions develop in a different way on the Internet than in traditional media. Social media is a contemporary method and platform that allows individuals to express their beliefs and shape the message to meet a political or ideological agenda that is not passively expressed but reflects social phenomena.10 Several publications relate that the information provided on the Internet is convincing people with MS that CCSVI is present and that treatment for it is an optimal method of managing their condition.11–13 A simple search in Google for CCSVI reveals more than 1 million results, primarily referring to the procedure as “liberation treatment.” This appealing name increases hope and introduces a challenge to explain why this treatment has not achieved a place in mainstream MS care. Content posted on the Internet is presenting CCSVI as “hope,”14 “truth of MS,”15 and “a miracle.”16
Several publications have addressed the emergence of medical tourism to meet the demand for liberation therapy17–19 and have highlighted the importance of the relationship with the HCP to moderate the influence of social media. Patients feel the need to be able to “trust” their HCP to provide them with unbiased and appropriate information about the possible risks and benefits of undergoing the procedure at home or abroad.18 Moreover, HCPs feel the need for support or guidelines for dealing with medical tourism and care after CCSVI treatment.17
It is essential that the health-care team and those working to understand the issues related to CCSVI and MS have a realistic view of social media, understand its dominant messages, and recognize its influence on people with MS. To date, there has been no systematic review of CCSVI and MS related to social media, yet the volume of messages and the ease of access cannot be ignored. The purpose of this study was to conduct a rigorous review of videos related to MS and CCSVI posted by people with MS on one social media website (YouTube) that describe symptoms before and after the surgical procedure, as well as videos presented by HCPs.
Methods
This study included a review of CCSVI-related videos posted on the YouTube website (http://www.youtube.com) between December 2009 and July 2011. All relevant videos were downloaded and viewed, and all the data presented in the videos were used, including visual, audio, and written information. Included in this study are videos posted by people with MS that describe their self-perceived function or symptoms before and after the surgical procedure for CCSVI and videos presented by HCPs. Excluded were non–English language videos, videos presented by other groups or individuals, and videos that did not address MS and CCSVI.
Data Collection and Analysis
All the videos were categorized by two lay reviewers with no expertise in MS and one HCP/researcher with 18 years' experience in MS. Having three reviewers controlled for rater variability and provided for an informed, nuanced interpretation of the video information.
Ten random videos by people with MS were viewed to ascertain the type of content in the videos and to gain a sense of dominant messages. The research team then developed a list of possible categories (such as country of origin, MS symptoms, and degree of symptom change). After this, all the reviewers saw 20 additional videos to ensure consistent interpretation across categories, to structure category titles, and to make category modifications, including adding categories or, for categories that were too broad, dividing into subcategories. A codebook was then developed, and the remaining videos were categorized. For example, 1) symptoms before the surgical procedure were coded as “present” or “not present” and 2) for postprocedure video data, symptoms were categorized as “not reported,” “fluctuations or no change reported,” or “improved.” The coding for mobility resulted in several subcategories, such as “walking without a cane,” “walking with a cane,” “using a walker,” “using a wheelchair,” and “not reported.” For people who reported more than one method of mobility (eg, walking without a cane indoors and with a cane outdoors), the lower mobility level was used (in this example, walking with a cane). “Significant improvement/regression” for mobility was defined as moving from one mobility level to another (eg, from “with a cane” to “without a cane”), and maintaining the same mobility level was “no change.” When the lay reviewers were uncertain about category inclusion, the HCP was consulted, the issues were discussed, and a consensus on categorization was reached.
Categorization of videos was sequenced. First, a lay reviewer screened out all the non-CCSVI videos and categorized videos by the individual(s) giving the message and the topic discussed. Next, the HCP, using discourse analysis, gleaned the messages from the videos posted by people with MS related to MS symptoms and developed thematic groupings for overarching messages. Finally, a lay reviewer extracted categorical data from the videos by HCPs related to the presentation (ie, type, audience, and continent) and presenter characteristics (eg, sex, continent of practice, and specialty) and then, using discourse analysis, identified overarching messages.
The discourse analysis approach was used in this study because it recognizes that no discourse is a closed entity; all discourse is informed and transformed by other discourses.20 This is the situation with social media because it allows individuals and collectives to take part in public discourse and thereby shape and change the processes and structures. The discourse analysis approach is concerned with the use of language; the way in which individuals achieve personal, social, and political goals through language; and the influence of groups participating in the discourse.16 In the discourse approach, interpretative analysis is undertaken, as it is an iterative process in which categories and codes are organized and textual data are distilled around overarching themes and relationships drawn across all the cases/videos.21 When bringing the discourse analysis approach to studies of media representation, it is beneficial to use macrotextual approaches that attend to the meanings embedded in text as well as the language.10
Data related to video length, date of upload, and number of views were collected from the YouTube website. This and all other categorical data were entered into a statistical software program (IBM SPSS Statistics for Windows, Version 20.0; IBM Corp, Armonk, NY) for frequency and descriptive analysis.
Results
As shown in Figure 1, 1789 YouTube files that provided 194 hours of footage were extracted. Of these, 509 did not meet the inclusion criteria, and 1042 videos were presented by people with MS. Of the 1042 videos, 421 (40%) were not included in this analysis because they covered a range of topics, such as the doctor appointment related to undergoing the surgery, summarizing a paper about CCSVI, lobbying for CCSVI, and expressing views about health policy related to CCSVI. The remaining 621 videos (60%) reported anecdotal or self-perceived results before and after the liberation surgery and are the data reported herein. This study also includes the messages depicted in the 238 videos presented by HCPs.
Figure 1.
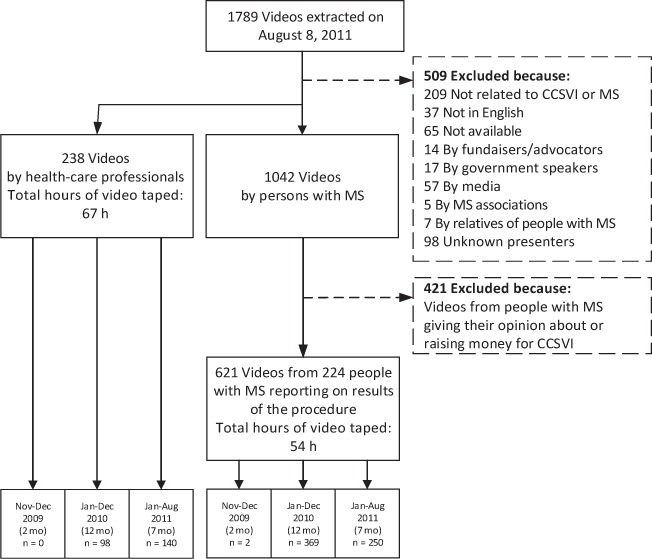
Flow diagram
CCSVI, chronic cerebrospinal venous insufficiency; MS, multiple sclerosis.
Videos by People with MS
The 621 videos were presented by 224 people with MS, with a range of 1 to 20 videos posted per person.
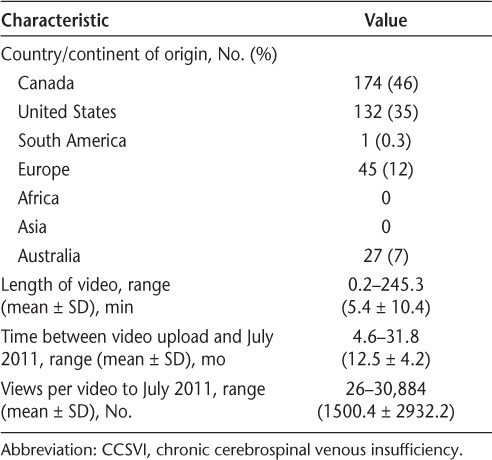
Characteristics of the Videos
The global distribution of the origin was reported for 379 videos (61%) (Table 1). Of note, 81% were North American, with a disproportionate representation from Canada, with 174 videos (vs. 132 videos from the United States). The mean number of views per video was 1500.4 (Table 1). The video with the highest number of views (30,884), titled “3 Days Later He Is Walking,” was from a person with MS who was a wheelchair user for several years. In the video, he reports, “30 minutes later, I had no double vision and within 3 days after the procedure I was capable of walking independently with no assistive device.” He stated, “it [the result of surgery] is a miracle.” Unlike most other videos, this video was not prepared by the person but by the Reformed MS Society, which is a consumer-based organization focusing on CCSVI and its treatment.22
Table 1.
Characteristics of the 621 videos on the CCSVI procedure
Characteristics of People with MS Who Uploaded Videos
Of the 224 people who presented the CCSVI-related videos, 143 (64%) were women. Time since MS diagnosis was reported by 69 people (31%) and was a mean ± SD of 11.0 ± 8.2 years (range, 1–40 years). Type of MS was reported by 30 of the participants (13%), with the following results: 6 (3%) with primary progressive, 9 (4%) with relapsing-remitting, and 15 (7%) with secondary progressive MS.
Endovascular Procedure Experienced
A total of 170 individuals (76%) did not report the location of their angioplasty. Of the remaining 54 people (24%), 39 (17%) reported that the left jugular was used, 48 (21%) the right jugular, and 13 (6%) the azygos vein. Some people reported that more than one vein was used. A stent was used for 12 individuals (5%). Two hundred five participants (92%) reported on their first angioplasty, 14 (6%) on the second, and 4 (2%) on the third. One person (0.4%) had undergone four procedures.
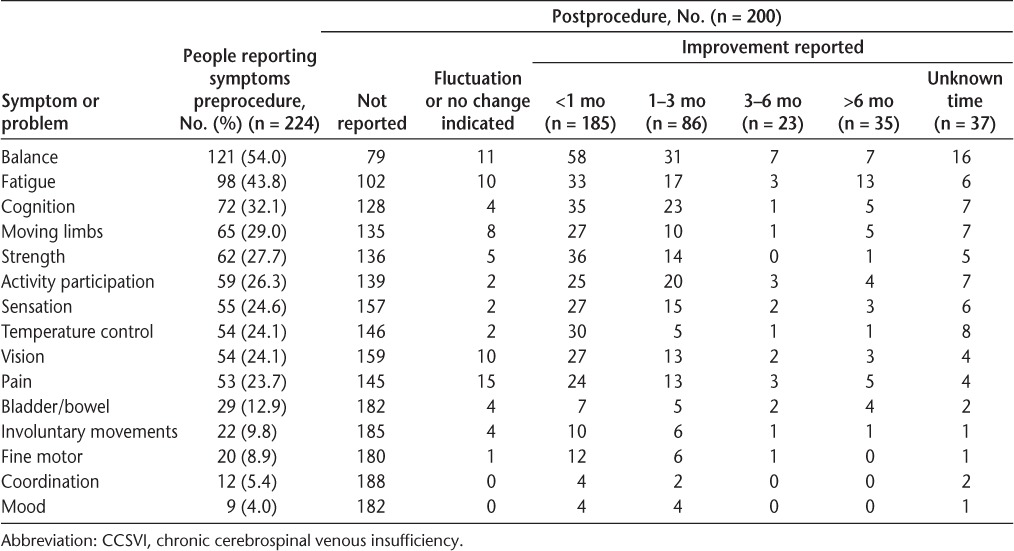
Results Attributed to the Endovascular Procedure Reported in the Videos
Table 2 presents the self-assessed results of the surgical procedure as reported in videos by people with MS. Thirty-one individuals (14%) reported no change with their message, emphasizing that “it did not work for them” because “MS is specific for each person” but suggested “it is worth a try.” The remaining 193 individuals (86%) reported 1 to 11 areas of improvement (mean ± SD, 3.4 ± 2.1), with balance, fatigue, cognition, moving limbs, and strength being the most frequently reported. The greatest improvements were reported in the first 3 months after the procedure.
Table 2.
Results of the CCSVI procedure for 224 people with MS
More than one-third of the people with MS were not using an assistive device for walking before the procedure. Preprocedure and postprocedure mobility function was described by 96 people. “Significant improvement” for mobility was reported by 17 individuals (18%), 78 (81%) reported no change (remained at the same level), and 1 (1%) had significant regression.
Messages by People with MS Who Uploaded Videos
On thematically analyzing the overarching messages, there was a sentiment of hope coupled with a conservative tone about results. The following six central overarching messages emerged from these videos:
CCSVI “is not a miracle but worth trying” as “I have nothing to lose.”
An implicit understanding about the differential results across individuals, with beliefs that suggest that the surgery “is more effective at earlier stages of MS” and “is not very effective for progressive MS.” This gives rise to the overall message that the “CCSVI procedure does not work for everybody.”
The results of the surgery are time limited, with some suggesting that “the results seem to be temporary” and others warning “not to have high expectations.”
The impact of the surgery is felt to “change quality of life” and to “just be hopeful.”
The procedure was viewed as being “noninvasive” and “a safe and easy procedure to undergo.”
“Stents should be used carefully.”
Videos Presented by HCPs
Characteristics of the Videos
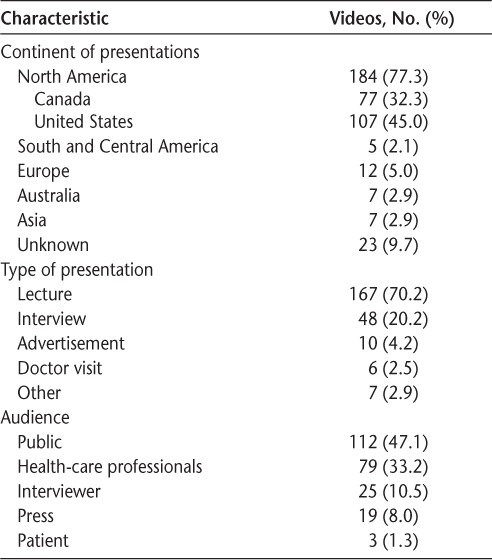
The 238 videos posted on YouTube were completed by 68 HCPs. Longer presentations were uploaded as more than one video, resulting in 210 unique presentations. The mean ± SD length of these videos was 16.8 ± 21.1 minutes (range, 0.55–124.1 minutes). Similar to videos by people with MS, most presenters were from North America (Table 3). Most videos, 167 (70%), were formal presentations in seminars, conferences, or forums. The target audience for 112 of the presentations (47%) was the public.
Table 3.
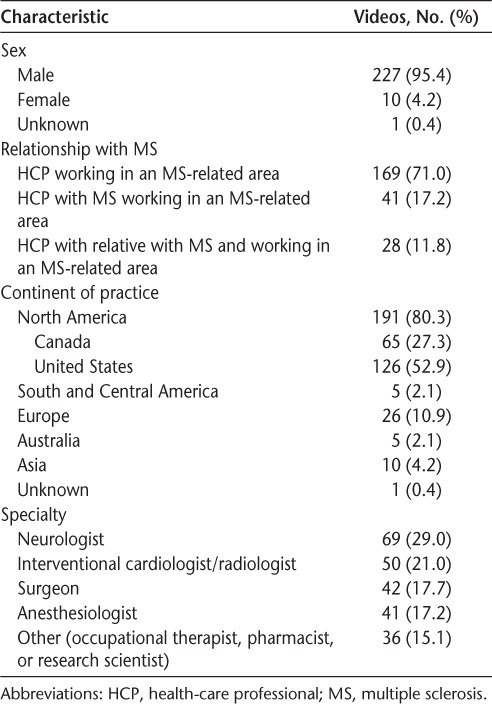
Characteristics of the 238 videos presented by health-care professionals
Characteristics of Presenters
A total of 227 video presentations (95%) were delivered by men, 69 (29%) by HCPs who had MS or a relative with MS, 69 (29%) by neurologists, and 50 (21%) by interventional cardiologists/radiologists (Table 4). Of the 68 HCPs giving presentations posted on YouTube, there was a range of 1 to 39 videos per HCP, with 48 HCPs posting 1 or 2 videos, 12 posting 3 to 9 videos, and 8 posting 10 or more videos. None of these videos were selling a product but rather attempted to present scientific results or personal or professional experience.
Table 4.
Characteristics of HCPs presented in 238 videos
Topics
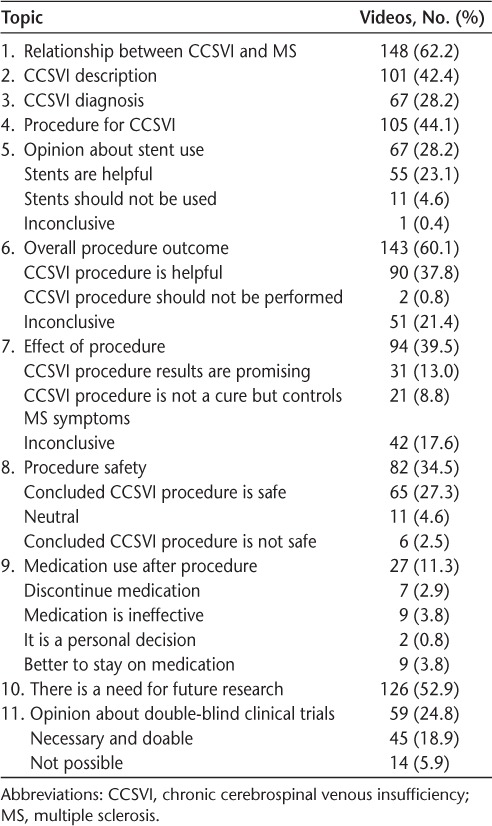
Table 5 summarizes the 11 topics discussed by HCPs, of which 148 videos (62%) were about the relationship between CCSVI and MS. A total of 143 videos (60%) gave their opinion about the overall outcome of the surgery, of which 90 (38%) regarded the surgical procedure as helpful.
Table 5.
CCSVI-related topics discussed in the 238 videos by health-care professionals
In addition, the overall stance or view about the CCSVI treatment was thematically organized. Of these, 175 videos (74%) referred to CCSVI or related topics with a positive view, and 7 (3%) presented a negative view. From the point of view of a lay reviewer, 17 of the presentations (7%) offered a positive perspective and gave convincing reasons, as did the 94 video presentations (39%) that were neutral.
Symptom Improvements and Complications
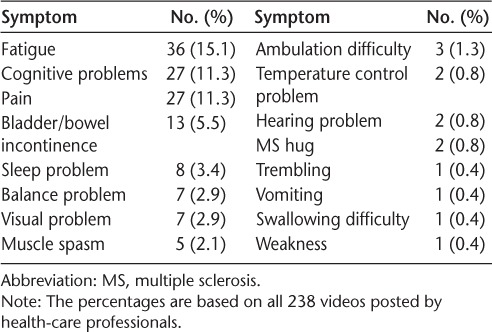
Sixty-one videos (26%) commented on symptoms (Table 6). More than one area/symptom of improvement was mentioned by some presenters. Improvements in fatigue, cognition, pain, and bowel/bladder control were the most commonly reported benefits of the CCSVI-related procedure. Presenters noted that there had not yet been any systematic evaluation of the impact of the procedure on symptoms.
Table 6.
Symptoms considered to improve after the procedure in 61 videos by health-care professionals
Most presentations were silent on funding and health-care policy issues, as only 20 (8%) addressed these topics. Presenters in 15 videos (6%) believed that the angioplasty procedure should be allowed for any person who is suspected of having blockage of veins and that limiting access to this procedure in people with MS in Canada is discrimination. Presenters in 16 videos (7%) went further, claiming that MS societies and neurologists are in denial because of self-serving motives.
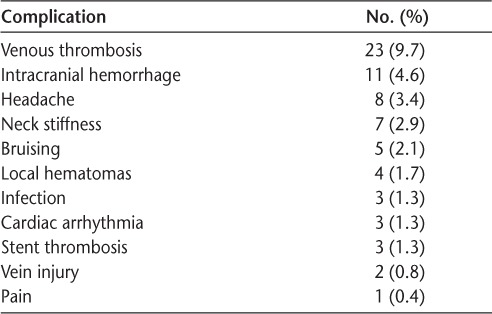
Forty-seven videos (20%) mentioned restenosis as a possible failure of the procedure. Fifty-seven videos (24%) commented on complications of the procedure, with venous thrombosis being the most frequently cited (Table 7).
Table 7.
Complications that might occur during or after the procedure in 238 videos by health-care professionals
Discussion
The purpose of this study was to systematically review the videos uploaded to YouTube in relation to MS and CCSVI. The results of the analysis of the videos presented by people with MS and HCPs suggested that the overall perceived message about the impact of the liberation procedure is positive. This is different from the current research findings. A recent Cochrane systematic review shows that despite the international effort to evaluate the efficacy of CCSVI-related angioplasty and completion of several randomized controlled trials, the evidence does not support or refute the efficacy or safety of the CCSVI-related angioplasty.4
In this study, 86% of people with MS who uploaded videos reported improvements in at least one area of their functional symptoms. Fatigue and cognition were reported to improve after the CCSVI-related procedure by both people with MS and HCPs. Two other symptoms reported to improve by people with MS were balance and their ability to move their limbs, and HCPs reported symptom relief for pain and bladder/bowel control. None of these reports were based on standard tests by blinded raters. Of note, positive results for fatigue, mobility, and sensation problems were also seen in open-label, nonrandomized studies of CCSVI.23,24 These reports need to be viewed with great caution given the lack of a randomized controlled research design and the absence of rater blinding. Without controlled studies, conclusions related to effectiveness are tentative.4,25
The overarching message in videos by people with MS was that “CCSVI is not a miracle but worth trying,” suggesting that despite anecdotal reports of success, there remains doubt about CCSVI and related treatment for MS. This sentiment has shifted from the original hypothesis posed by Zamboni et al. that CCSVI was the cause of MS and that the procedure was a cure.18,26 The results of this study suggest that “hope” has been the significant motivation for engaging in medical tourism to access the angioplasty procedure. This overwhelming hope for complete cure gradually diminished and gave way to messages such as “not to have high expectations” and “just be hopeful,” as the “CCSVI procedure does not work for everybody.” This may be because only 18% of the videos reported significant change in mobility. The likelihood of existence of the placebo effect driven by the possible hope highlights the importance and critical need for blinded studies for testing the efficacy of the procedure. The importance of blinded studies was also highlighted in 19% of presentations by HCPs.
The results of this study are similar to those of other studies on decision making related to CCSVI. A study of 100 selected videos from YouTube found overwhelmingly positive messages about CCSVI.18 The authors highlighted that “skepticism of big pharma and a sense of dissatisfaction of the available treatment”18(p423) was a strong theme in their study. Another study27 interviewed people with MS who traveled abroad after undergoing the angioplasty surgery and found that the CCSVI treatment created hope among participants, despite their limited expectations about the results.
Unlike the videos posted by people with MS, the HCP videos reported several adverse effects. To date, there have been few published studies systematically describing the complications of the procedure.28,29 Further research is required to develop guidelines and strategies to monitor and manage these postsurgical complications.
The global distribution of videos shows the degree of the controversy between people with MS and HCPs in North America.30 Initially, the CCSVI-related procedure was available only through randomized controlled trials in Canada, whereas in countries such as India, the United States, and Germany, the procedure is available with no restrictions. More than 80% of videos that were included in the study were from people in North America. This suggests that North Americans and certainly Canadians (with a socialized health-care system) feel the necessity to advocate for the procedure, believing it to be unnecessarily restricted by governments. This may also reflect a consumer behavior in North America.
Whether HCPs agree with patients pursuing such treatment, the results of this study confirm that providing patients with adequate and accurate information is essential. This study also clearly demonstrates the skewed messaging in social media, in this case on YouTube. The Internet is providing people with a wide range of information and misinformation related to treatment for MS, and it is challenging to decide what information is accurate and evidence based.12 The overwhelming number of videos related to CCSVI with positive results does not seem to be unreliable to most people but presents real-world examples of people talking sincerely about their perspectives and experiences. Although the goal of people with MS posting videos may simply be to share their experience, the disproportionate representation of positive messages may lead to social persuasion. This social persuasion by peers, known to be the most compelling and quickest way to gain confidence,30 is magnified when more than 200 videos by HCPs report that CCSVI-related procedures help improve MS-related symptoms. The recommendations for caution regarding expectations, expression of a need for scientific evidence, and mention of possible adverse effects and complications may be overlooked by reviewers. At the same time, Internet content provides us with valuable insight on perceptions and experience from individuals with MS, which may not be spontaneously shared during medical appointments. Therefore, we might not want or be able to change the way the Internet is used. However, the impact of Internet-based information can be moderated by HCPs if a trusting relationship with their patients is reinforced and enough information is provided to describe the state of the research in an open, nonconfrontational manner. This includes physicians and other HCPs assisting patients to evaluate advertisements by providers offering the angioplasty, to understand the benefits as well as the risks of the procedure, and to make informed decisions about undergoing the procedure.18,27 In addition, providing education and guidelines for HCPs to manage issues of medical tourism and handle the postsurgical results and potential adverse effects is essential for optimal care.
The importance of providing relevant information to patients was demonstrated in the videos in this study. After two stent-related deaths in Canada, patients were warned about the risk of stent use and considered this information when undergoing the procedure. As a result, only a few patients in this study have actually agreed or needed to use a stent during the procedure.
To our knowledge, this is the only study published on CCSVI and social media that includes an extensive list of the possible MS symptoms and considers change in mobility from a functional perspective, that is, by use of assistive devices. Also, this is the only study to look at the perspective of the HCP as uploaded to social media, through their presentations about CCSVI treatment, its effectiveness, and its adverse effects.
This study has both strengths and limitations. A methodological strength is that three reviewers participated in categorizing patient videos. This augmented the trustworthiness of the data owing to the consensus and verification process embedded in the study. A second strength of this study is the use of social media as the source of data. This enables a higher level of transparency in research because the data are publicly available in original form.
This study also has limitations. As with all social media, data could not be substantiated for accuracy beyond the opinion of the presenters, and there were a large number of missing data. It is also important to note that the data used in this study can be skewed because only 14% of the videos reported no change or worsened symptoms. It is likely that mostly those who experienced positive results were motivated to upload videos to share their experience, whereas those who experienced no or poor results may have been disappointed about spending money with no gain or were reluctant to reduce hope for others for whom the treatment might be successful. Another limitation comes from the fact that we did not have the opportunity to ask people with MS or HCPs what motivated them to post the videos; therefore, the intent of the posting is open to interpretation. This study suggests that the underlying themes of hope and control over treatment decisions motivated at least some patients.
Social media content conveys overall positive messages about the results of angioplasty to treat CCSVI for MS. This observation raises concern about the role played by social persuasion in CCSVI-related decision making. At the same time, social media content provides valuable insight into the feelings, beliefs, and experiences of people with MS, which they may not always fully express to their HCPs. The results of this study show the need for researchers and clinicians to be actively engaged with the public so that people are adequately informed of the scientific findings and possible complications related to CCSVI treatment for MS.
PracticePoints.
Social media are routinely used by people with MS as a source of medical information.
Social media are conveying strong positive messages about the results of angioplasty for MS, and social persuasion seems to strongly influence decision making related to chronic cerebrospinal venous insufficiency treatment.
The results of this study show the need for researchers and clinicians to be actively engaged with the public.
Footnotes
Financial Disclosures: The authors have no conflicts of interest to disclose.
Funding/Support: This study was supported by a National Multiple Sclerosis Society Mentor-Based Rehabilitation Fellowship (award No. MB 0016).
References
- 1.Zamboni P, Galeotti R, Menegatti E et al. Chronic cerebrospinal venous insufficiency in patients with multiple sclerosis. J Neurol Neurosurg Psychiatry. 2009;80:392–399. doi: 10.1136/jnnp.2008.157164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kuehn BM. FDA warns about the risks of unproven surgical therapy for multiple sclerosis. JAMA. 2012;307:2575–2576. doi: 10.1001/jama.2012.6399. [DOI] [PubMed] [Google Scholar]
- 3.Traboulsee AL, Knox KB, Machan L et al. Prevalence of extracranial venous narrowing on catheter venography in people with multiple sclerosis, their siblings, and unrelated healthy controls: a blinded, case-control study. Lancet. 2014;383:138–145. doi: 10.1016/S0140-6736(13)61747-X. [DOI] [PubMed] [Google Scholar]
- 4.van Zuuren EJ, Fedorowicz Z, Pucci E, Jagannath V, Robak EW. Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency in people with multiple sclerosis: a summary of a Cochrane systematic review. J Neurol Neurosurg Psychiatry. 2014;85:405–410. doi: 10.1136/jnnp-2013-305481. [DOI] [PubMed] [Google Scholar]
- 5.Bourdette DN, Cohen JA. Venous angioplasty for “CCSVI” in multiple sclerosis: ending a therapeutic misadventure. Neurology. 2014;83:388–389. doi: 10.1212/WNL.0000000000000651. [DOI] [PubMed] [Google Scholar]
- 6.Hutchinson M. Funding CCSVI research is/was a waste of valuable time, money and intellectual energy: commentary. Mult Scler J. 2013;19:861–862. doi: 10.1177/1352458513490817. [DOI] [PubMed] [Google Scholar]
- 7.Zivadinov R, Weinstock-Guttman B. Funding CCSVI research is/was a waste of valuable time, money and intellectual energy: no. Mult Scler J. 2013;19:858–860. doi: 10.1177/1352458513480252. [DOI] [PubMed] [Google Scholar]
- 8.Ghezzi A. Funding CCSVI research is/was a waste of valuable time, money and intellectual energy: yes. Mult Scler J. 2013;19:855–857. doi: 10.1177/1352458513479825. [DOI] [PubMed] [Google Scholar]
- 9.Laupacis A, Lillie E, Dueck A, Aviv R, Straus S, Perrier L. Systematic reviews of the evidence regarding chronic cerebral spinal venous insufficiency (CCSVI) and multiple sclerosis: an update for the CIHR Expert Panel. Sep 23, 2011. http://www.cihr-irsc.gc.ca/e/44356.html. Accessed September 2012.
- 10.Carpentier N, De Cleen B. Bringing discourse theory into media studies: the applicability of discourse theoretical analysis (DTA) for the study of media practices and discourses. J Lang Polit. 2007;6:265–293. [Google Scholar]
- 11.Fragoso YD. The internet racing ahead of the scientific evidence: the case of “liberation treatment” for multiple sclerosis. Arq Neuropsiquiatr. 2011;69:525–527. doi: 10.1590/s0004-282x2011000400022. [DOI] [PubMed] [Google Scholar]
- 12.Oger J, Alkhawajah M. CCSVI: hope, hype of snake oil? Can J Neurol Sci. 2010;37:716. [PubMed] [Google Scholar]
- 13.Chafe R, Born KB, Slutsky AS, Laupacis A. The rise of people power. Nature. 2011;472:410–411. doi: 10.1038/472410a. [DOI] [PubMed] [Google Scholar]
- 14. Angelusa73 CCSVI—meeting the face of hope YouTube website. https://www.youtube.com/all_comments?v=TO7cw7NLIKE&lc=wjyw80onPME9Kzr2JeBwTY68BWsl_JagqIBJCDcv_qs. Published February 9, 2010. Accessed December 10, 2011.
- 15.LiberateMichelle. The naked truth of MS and CCSVI. YouTube website. https://www.youtube.com/watch?v=x6vZxVyTL7U. Published April 7, 2011. Accessed December 10, 2011.
- 16.Munkres B. Pitch for funding—living through a miracle—a documentary about CCSVI. YouTube website. https://www.youtube.com/watch?v=gMCzmP3y7Zg. Updated July 11, 2011. Accessed December 10, 2011.
- 17.Johnston R, Crooks V, Snyder J. “I didn't even know what I was looking for”: a qualitative study of the decision-making processes of Canadian medical tourists. Globalization Health. 2012;8:23. doi: 10.1186/1744-8603-8-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mazanderani F, O'Neill B, Powell J. “People power” or “pester power”? YouTube as a forum for the generation of evidence and patient advocacy. Patient Educ Counsel. 2013;93:420–425. doi: 10.1016/j.pec.2013.06.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Pullman D, Zarzeczny A, Picard A. Media, politics and science policy: MS and evidence from the CCSVI trenches. BMC Med Ethics. 2013;14:6. doi: 10.1186/1472-6939-14-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Jorgensen M, Phillips L. Discourse Analysis as Theory and Method. London, England: Sage Publications; 2002. [Google Scholar]
- 21.Starks H, Trinidad SB. Choose your method: a comparison of phenomenology, discourse analysis, and grounded theory. Qual Health Res. 2007;17:1372–1380. doi: 10.1177/1049732307307031. [DOI] [PubMed] [Google Scholar]
- 22.The Reformed Multiple Sclerosis Society website. 2011. http://www.reformedms.org/. Accessed January 20, 2012.
- 23.Malagoni AM, Galeotti R, Menegatti E et al. Is chronic fatigue the symptom of venous insufficiency associated with multiple sclerosis? a longitudinal pilot study. Int Angiol. 2010;29:176–182. [PubMed] [Google Scholar]
- 24.Spagnolo S, Scalise F, Barbato L, Grasso MA, Tesler UF. Bilateral surgical reconstruction for internal jugular veins disease in patients with chronic cerebrospinal venous insufficiency and associated multiple sclerosis. Ann Vasc Surg. 2014;28:1793.e1–1793.e4. doi: 10.1016/j.avsg.2014.03.012. [DOI] [PubMed] [Google Scholar]
- 25.Zwischenberger BA, Beasley MM, Davenport DL, Xenos ES. Meta-analysis of the correlation between chronic cerebrospinal venous insufficiency and multiple sclerosis. Vasc Endovasc Surg. 2013;47:620–624. doi: 10.1177/1538574413503562. [DOI] [PubMed] [Google Scholar]
- 26.Johnston R. Examining the Role of Family Physicians in the Decision-making Processes of Canadian Medical Tourists. Burnaby, BC, Canada: Simon Fraser University; 2010. [Google Scholar]
- 27.Snyder J, Adams K, Crooks V, Whitehurst D, Vallee J. “I knew what was going to happen if I did nothing and so I was going to do something”: faith, hope, and trust in the decisions of Canadians with multiple sclerosis to seek unproven interventions abroad. BMC Health Serv Res. 2014;14:445. doi: 10.1186/1472-6963-14-445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Burton JM, Alikhani K, Goyal M et al. Complications in MS patients after CCSVI procedures abroad (Calgary, AB) Can J Neurol Sci. 2011;38:741–746. doi: 10.1017/s0317167100054123. [DOI] [PubMed] [Google Scholar]
- 29.Mandato KD, Hegener PF, Siskin GP et al. Safety of endovascular treatment of chronic cerebrospinal venous insufficiency: a report of 240 patients with multiple sclerosis. J Vasc Interven Radiol. 2012;23:55–59. doi: 10.1016/j.jvir.2011.09.019. [DOI] [PubMed] [Google Scholar]
- 30.Bandura A. Self-efficacy. In: Ramachaudran VS, editor. Encyclopedia of Human Behavior. Vol. 4. New York, NY: Academic Press; 1994. pp. 71–81. [Google Scholar]