

Abstract
Endoscopic ultrasonography (EUS)-guided walled-off necrosis drainage using a double flanged metal stent was reported for satisfactory drainage and endoscopic necrosectomy. High complication rates related to stent migration are reported. This is the first report of the removal of a displaced, double flanged metal stent in walled-off necrosis by EUS. The patient was a 62-year-old male who was suffering from mild midepigastric abdominal pain. A double flanged metal stent had been placed in our endoscopy center 8 weeks before presentation. Computed tomography demonstrated complete resolution of the walled-off necrosis; however, the stent migrated into the cyst. We dislodged the stent using forceps with real-time endosonography.
In conclusion, Follow-up is important for patients with a double flanged metal stent, specifically with regards to postprocedural stent migration.
Keywords: displaced, double flanged metal stent, endoscopic ultrasonography
INTRODUCTION
Endoscopic ultrasonography (EUS)-guided walled-off necrosis drainage using a fully covered double flanged metal stent as a novel technique has been reported for satisfactory drainage and endoscopic necrosectomy.[1,2,3] However, managing a displaced double flanged metal stent and when to remove the stent remains controversial.
CASE REPORT
The patient was a 62-year-old male with a history of acute necrotizing pancreatitis, who was found to have a peripancreatic fluid collection for approximately 6 months. He had developed a fever and abdominal pain for one week, and was diagnosed with infected walled-off necrosis of the pancreatic tail (62 mm × 74 mm on EUS). Mass lesions were excluded and a puncture site was determined within the gastric body. A fully covered double flanged metal stent (Micro-Tech, Nanjing, China) was placed into the pancreatic cyst using real-time EUS guidance; there was an abundance of cystic debris.
Postprocedure, the body temperature of the patient returned to normal. Computed tomography (CT) was performed 7 days later, then monthly.
Eight weeks after drainage, the patient began to experience midepigastric abdominal pain and underwent repeat CT imaging, which demonstrated complete resolution of the cyst, but with the stent having migrated into the cyst. Endoscopic imaging demonstrated one ulcer in the body of the stomach. However, using EUS, the metallic stent was found to be outside of the stomach. We dislodged the stent using a forceps under EUS guidance [Figure 1]. After the procedure, EUS was used to monitor the site. To ensure no bleeding, we withdrew the echo-endoscope. The patient's abdominal pain resolved after the procedure. After a 6-month follow-up period, no pseudocyst recurrence was noted.
Figure 1.
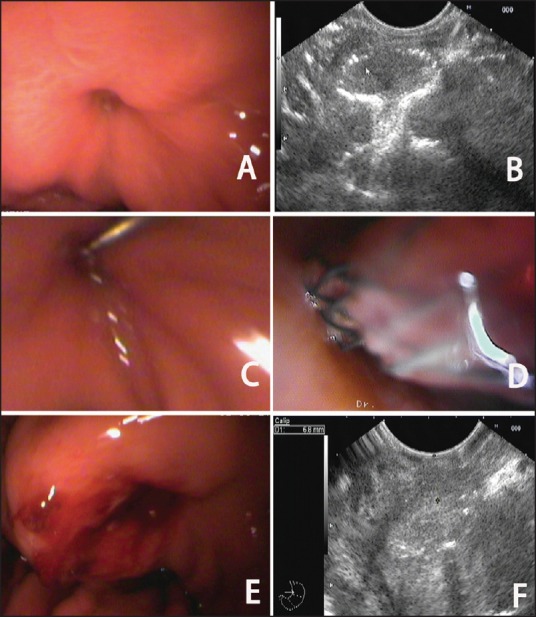
(a) Using endoscopic imaging, only one ulcer was seen in the body of the stomach. (b) Using endoscopic ultrasonography (EUS), the metal stent was seen outside of the stomach. c) and d) We dislodged the stent using a forceps under EUS guidance. (e) The endoscopic image of the site after procedure. (f) Post-procedure EUS
DISCUSSION
The use of a conventional, fully covered double flanged metal stent for pancreatic pseudocyst drainage has been previously reported.[1,2] High complication rates related to migration have also been documented.[2] When the stent should be removed remains controversial. Long-term stent patency and safety is unknown and requires further investigation. According to Itoi et al.,[3] metal stent removal was successful even after an implant time of 11.7 weeks in one patient. Newly designed metal stents, consisting of a fully covered 13-mm length and 15-mm diameter stent with double flanges, were used in our study. Different from traditional self-expandable metal stents, the double flanged metal stent is designed with bilateral anchor flanges. Using this type of metal stent, the incidence rate of displacement is decreased. Since March 2012, 17 patients underwent EUS-guided pseudocyst drainage using a fully covered double flanged metal stent in our endoscopy center. The mean time of stent removal is 11.2 weeks. Our case is the only stent migration that has occurred until now. Although migration of a double flanged metal stent is rare, it remains challenging for the endoscopist, as it is difficult to dislodge the stent using endoscopy. Hence, follow-up is important for patients with a double flanged metal stent, specifically with regards to postprocedural stent migration.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Talreja JP, Shami VM, Ku J, et al. Transenteric drainage of pancreatic-fluid collections with fully covered self-expanding metallic stents (with video) Gastrointest Endosc. 2008;68:1199–203. doi: 10.1016/j.gie.2008.06.015. [DOI] [PubMed] [Google Scholar]
- 2.Belle S, Collet P, Post S, et al. Temporary cystogastrostomy with self-expanding metallic stents for pancreatic necrosis. Endoscopy. 2010;42:493–5. doi: 10.1055/s-0029-1244021. [DOI] [PubMed] [Google Scholar]
- 3.Itoi T, Binmoeller KF, Shah J, et al. Clinical evaluation of a novel lumen-apposing metal stent for endosonography-guided pancreatic pseudocyst and gallbladder drainage (with videos) Gastrointest Endosc. 2012;75:870–6. doi: 10.1016/j.gie.2011.10.020. [DOI] [PubMed] [Google Scholar]