

INTRODUCTION
Superior mesenteric artery (SMA) syndrome or Wilkie's syndrome is a rare but potentially life threatening gastrointestinal condition. This syndrome is a clinical phenomenon believed to be caused by compression of the third part of the duodenum between the SMA and the aorta, leading to obstruction. Patients may present symptoms of gastrointestinal obstruction, such as with recurrent episodes vomiting, upper abdominal distension and epigastric tenderness8. Various etiology theories, clinical course and treatment options have hitherto been discussed5. An interdisciplinary teamwork provides the most beneficial diagnostic and therapeutic result in this often underestimated disease.
CASE REPORT
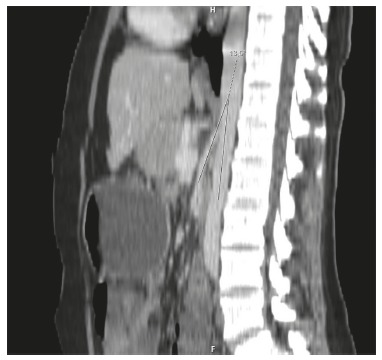
A 27 years old woman was referred to our hospital, with recurrent episodes of profuse vomiting and upper abdominal pain associated with loss of appetite and dyspepsia since two years. She had no other comorbidities. Had been treated at another hospital with proton pump inhibitors, analgesics and intravenous fluids. She had a history of chronic anorexia and progressive loss of weight along with recurrent episodes of vomiting and upper abdominal pain. Clinical examination revealed dehydration, asthenicity (body mass index 19,5 kg/m2, weight: 50 kg, length:160 cm), abdominal distension, epigastric tenderness. Laboratory investigations showed a total white cell count of 9 500 mm3 and hypokalaemia (serum potassium: 3 mEq/l). Plain radiograph of the abdomen revealed gastric dilation. Ultrasonography was unremarkable. Upper gastrointestinal endoscopy showed dilated stomach and duodenum. Contrast-enhanced computerized tomography scan revealed grossly distended stomach and duodenum proximal to the third part of the duodenum at the level of the origin of superior mesenteric artery with abrupt narrowing at this level, suggestive of Wilkie's syndrome. While, normally, the angle between the SMA and the aorta is 22° to 60°, in this case, the aortomesenteric angle was 13,5°(Figure 1). In this case, conservative management was inefficient, so surgical treatment aiming to bypass the obstruction by an anastomosis between the jejunum and the proximal duodenum (duodenojejunostomy) was successful.
FIGURE 1. - CT of the abdomen showing reduced angle between the superior mesenteric artery and the aorta, with compression of the duodenum.
DISCUSSION
Wilkie's syndrome occurs when the third portion of the duodenum is compressed between the SMA and the aorta. While, normally, the angle between the SMA and the aorta is 25° to 60°, it is narrowed in this syndrome7. The aortomesenteric angle may be narrowed because of congenital anomalies, significant weight loss, lumbar hyperlordosis, restorative proctocolectomy with ileal-anal anastomosis1 , 2 , 6. Clinical features of Wilkie's syndrome are entirely vague and non-specific. The most prominent symptoms are post-prandial abdominal pain (59%), nausea (40%), vomiting (50%), early satiety (32%), and anorexia (18%). These symptoms are aggravated by lying supine after eating and are relieved by assuming the left lateral decubitus, prone or knee-chest position3. These symptoms are compatible with more common conditions such as peptic ulcer disease, biliary colic, pancreatitis, and mesenteric ischemia. Physical examination generally reveals an asthenic body habitus.
The diagnosis of Wilkie's Syndrome requires a high degree of clinical suspicion confirmed by radiographic studies demonstrating compression of the third portion of the duodenum. CT of the abdomen typically shows gastric and duodenal dilation and narrowed aortomesenteric angle9. Wilkie's syndrome responds to conservative management in the form of adequate nutrition by enteral/parenteral feeding and proper positioning of the patient after feeds. Surgery is resorted to when conservative measures are ineffective or in patients with long history of progressive weight loss or pronounced duodenal dilatation with stasis and complications4.
Footnotes
Financial source: none
REFERENCES
- 1.Adson DE, Mitchell JE, Trenkner SW. The superior mesenteric artery syndrome and acute gastric dilatation in eating disorders: a report of two cases and a review of the literature. Int J Eat Disord. 1997;21:103–114. doi: 10.1002/(sici)1098-108x(199703)21:2<103::aid-eat1>3.0.co;2-p. [DOI] [PubMed] [Google Scholar]
- 2.Goitein D, Gagne DJ, Papasavas PK, Dallal R, Quebbemann B, Eichinger JK, Johnston D, Caushaj PF. Superior mesenteric artery syndrome after laparoscopic Roux-en-Y gastric bypass for morbid obesity. Obes Surg. 2004;14:1008–1011. doi: 10.1381/0960892041719626. [DOI] [PubMed] [Google Scholar]
- 3.Hines JR, Gore RM, Ballantyne GH. Superior mesenteric artery syndrome. Diagnostic criteria and therapeutic approaches. Am J Surg. 1984;148:630–632. doi: 10.1016/0002-9610(84)90339-8. [DOI] [PubMed] [Google Scholar]
- 4.Massoud WZ. Laparoscopic management of superior mesenteric artery syn-drome. Int Surg. 1995;80:322–327. [PubMed] [Google Scholar]
- 5.Mathenge N, Osiro S, Rodriguez II, Salib C, Tubbs RS, Loukas M. Superior mesenteric arterysyndrome and its associated gastrointestinal implications. Clin Anat. 2014;27(8):1244–1252. doi: 10.1002/ca.22249. [DOI] [PubMed] [Google Scholar]
- 6.Matheus Cde O, Waisberg J, Zewer MH, Godoy AC. Syndrome of duodenal compression by the superior mesenteric artery following restorative proctocolectomy: a case report and review of literature. Sao Paulo Med J. 2005;123:151–153. doi: 10.1590/S1516-31802005000300013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Neri S, Signorelli SS, Mondati E, Pulvirenti D, Campanile E, Di Pino L, Scuderi M, Giustolisi N, Di Prima P, Mauceri B, Abate G, Cilio D, Misseri M, Scuderi R. Ultrasound imaging in diagnosis of superior mesenteric artery syndrome. J Intern Med. 2005;257:346–351. doi: 10.1111/j.1365-2796.2005.01456.x. [DOI] [PubMed] [Google Scholar]
- 8.Shiu JR, Chao HC, Luo CC, Lai MW, Kong MS, Chen SY, Chen CC, Wang CJ. Clinical and nutritional outcomes in children with idiopathic superior mesenteric artery syndrome. J Pediatr Gastroenterol Nutr. 2010;51:177–182. doi: 10.1097/MPG.0b013e3181c7bdda. [DOI] [PubMed] [Google Scholar]
- 9.Unal B, Aktas A, Kemal G, Bilgili Y, Güliter S, Daphan C, Aydinuraz K. Superior mesenteric artery syndrome: CT and ultrasonography findings. Diagn Interv Radiol. 2005;11:90–95. [PubMed] [Google Scholar]