

Abstract
Critical appraisal of outcomes after burn shock resuscitation with albumin has previously been restricted to small relatively old randomized trials, some with high risk of bias. Extensive recent data from nonrandomized studies assessing the use of albumin can potentially reduce bias and add precision. The objective of this meta-analysis was to determine the effect of burn shock resuscitation with albumin on mortality and morbidity in adult patients. Randomized and nonrandomized controlled clinical studies evaluating mortality and morbidity in adult patients receiving albumin for burn shock resuscitation were identified by multiple methods, including computer database searches and examination of journal contents and reference lists. Extracted data were quantitatively combined by random-effects meta-analysis. Four randomized and four nonrandomized studies with 688 total adult patients were included. Treatment effects did not differ significantly between the included randomized and nonrandomized studies. Albumin infusion during the first 24 hours showed no significant overall effect on mortality. However, significant statistical heterogeneity was present, which could be abolished by excluding two studies at high risk of bias. After those exclusions, albumin infusion was associated with reduced mortality. The pooled odds ratio was 0.34 with a 95% confidence interval of 0.19 to 0.58 (P < .001). Albumin administration was also accompanied by decreased occurrence of compartment syndrome (pooled odds ratio, 0.19; 95% confidence interval, 0.07–0.50; P < .001). This meta-analysis suggests that albumin can improve outcomes of burn shock resuscitation. However, the scope and quality of current evidence are limited, and additional trials are needed.
Although fluid resuscitation is the foundation of acute burn care, the optimal type, timing, and amount of fluid for burn shock remains inadequately investigated. Early burn resuscitation formulas of the 1940s and 1950s incorporated colloids, usually in the form of albumin-containing blood products1,2 but also purified albumin.3 Unacceptably high rates of viral hepatitis transmission discouraged the continued use of plasma preparations available during that period, however.4 By contrast, no case of viral disease transmission has ever been identified for licensed albumin or albumin contained in other licensed products, according to the US Food and Drug Administration.5 In addition to concern about viral disease transmission, the subsequent introduction of crystalloid-only formulas was prompted by an increasing focus on the role of extravascular sodium deficiency in burn shock.6
The commonly used Parkland and modified Brooke formulas using crystalloid in the form of lactated Ringer’s solution have remained unchanged since their introduction in the 1970s.7 In the first 24 hours after a burn, the Parkland formula calls for 4 ml·kg−1 crystalloid per percent TBSA (%TBSA) burned and the modified Brooke formula for 2 ml·kg−1 per %TBSA.
An increasingly recognized concern is that many patients are found to receive considerably more resuscitation fluid than predicted by the formulas.8 This phenomenon was termed “fluid creep” by Pruitt in 2000, and excessive resuscitation has emerged as a significant problem in modern burn care.8,9 Numerous reports document that the majority of patients with major burns are exceeding the predicted amount of acute care resuscitation fluid.10–17 In a 2007 U.S. multicenter study of patients with major burns, fluid in excess of the predicted volume was accompanied by increased odds of pneumonia, with an odds ratio (OR) of 1.92, bloodstream infections (OR, 2.33), adult respiratory distress syndrome (OR, 1.55), multiorgan failure (OR, 1.49), and death (OR, 1.74).18
A major complication attributable to over-resuscitation in burn patients is compartment syndrome of the abdomen or extremities resulting from massive edema in both burned and unburned tissue.11,19–22 Large-volume fluid resuscitation in patients with major burns increases the risk of intraabdominal hypertension and consequent abdominal compartment syndrome (ACS). Generally, ACS is encountered in patients with extensive burns of approximately 50% TBSA or more, often with concomitant inhalation injury.23 ACS can significantly worsen the prognosis of burn patients.
The primary goal of resuscitation is to restore and preserve tissue perfusion. Colloids by virtue of their oncotic properties can better maintain intravascular volume than crystalloids, and thus reduce fluid volume demands. Yet, the question of whether colloids can improve outcomes of burn shock resuscitation remains unsettled. In an international survey of burn shock resuscitation practices, approximately half of respondents administered colloid during the first 24 hours.24 The colloids predominantly used were purified albumin and fresh frozen plasma (FFP). Present at a concentration of 4.09 g·dL−1, albumin is the predominant protein in FFP, accounting for more than 75% of its colloid osmotic pressure.25
Definitive large-scale randomized trials investigating the use of albumin for burn shock resuscitation have yet to be conducted. Meta-analysis can be of value in establishing the current state of knowledge and informing the design of future trials. While theoretically randomized trials should guarantee balance between treatment groups and minimize distortions arising from the placebo effect, the currently available randomized trials examining albumin infusion for burn shock resuscitation are few in number, small in size, and prone to bias, for instance, resulting from lack of blinding and imbalances in baseline risk. A series of larger and more recent nonrandomized controlled studies can potentially reduce bias and increase precision.26 As a general principle, the inclusion of both randomized and nonrandomized studies in meta-analyses has been advocated,27 and such an approach appears to be particularly appropriate in light of currently available evidence on albumin infusion for burn shock resuscitation. We here describe such a meta-analysis.
METHODS
Inclusion Criteria
Controlled clinical studies comparing purified human albumin with crystalloid for burn shock resuscitation of adult patients were eligible for inclusion. Studies of postresuscitation albumin supplementation for hypoalbuminemia were not considered. Data on mortality and/or morbidity must have been available. Safeguards against bias arising from imbalances in baseline risk of poor outcome must have been implemented either through random allocation to treatment or, in the case of nonrandomized studies, by adjustment for observed imbalances with multivariate statistical methods. No language or time period restrictions were imposed.
Search Techniques
Published and unpublished studies conforming to the above inclusion criteria were sought by a variety of methods, including computer searches of bibliographic databases (MEDLINE and EMBASE), the Cochrane Library, meeting abstract databases and other Internet-resident information resources. Online and hard copy journal contents were perused. Reference lists were examined.
Data Extraction
Two investigators independently extracted data from the reports of included studies. Differences in interpretation were resolved by discussion. Extracted data consisted of: study year, locale, and design; numbers of study centers, patients, deaths, and complications; resuscitation fluid regimens compared; age; %TBSA burned; inhalation injury; and imbalances in baseline risk factors.
Statistical Analysis
The primary outcome measure was the OR for mortality and particular types of complications. The pooled OR for included studies and its 95% confidence interval (CI) were computed under a random-effects model.28 Heterogeneity, that is, variability of effect size greater than expected for a homogeneous population of studies, was evaluated by Cochran Q test and the I2 statistic.29 Differences in effect between randomized and nonrandomized studies were determined by test of interaction.30 Publication bias was assessed by linear regression of standardized effect vs precision.31 Quality assessment of randomized studies included three validated criteria: randomization method, allocation concealment, and blinding.32
RESULTS
Included Studies
Through the search process 135 candidate study reports were identified (Figure 1). On screening of the abstracts, 31 of the reports were excluded, most often because they were review articles without original data. The full text of the other 104 articles was examined in detail. At that stage 96 additional reports were excluded, again most frequently because of lack of original data.
Figure 1.
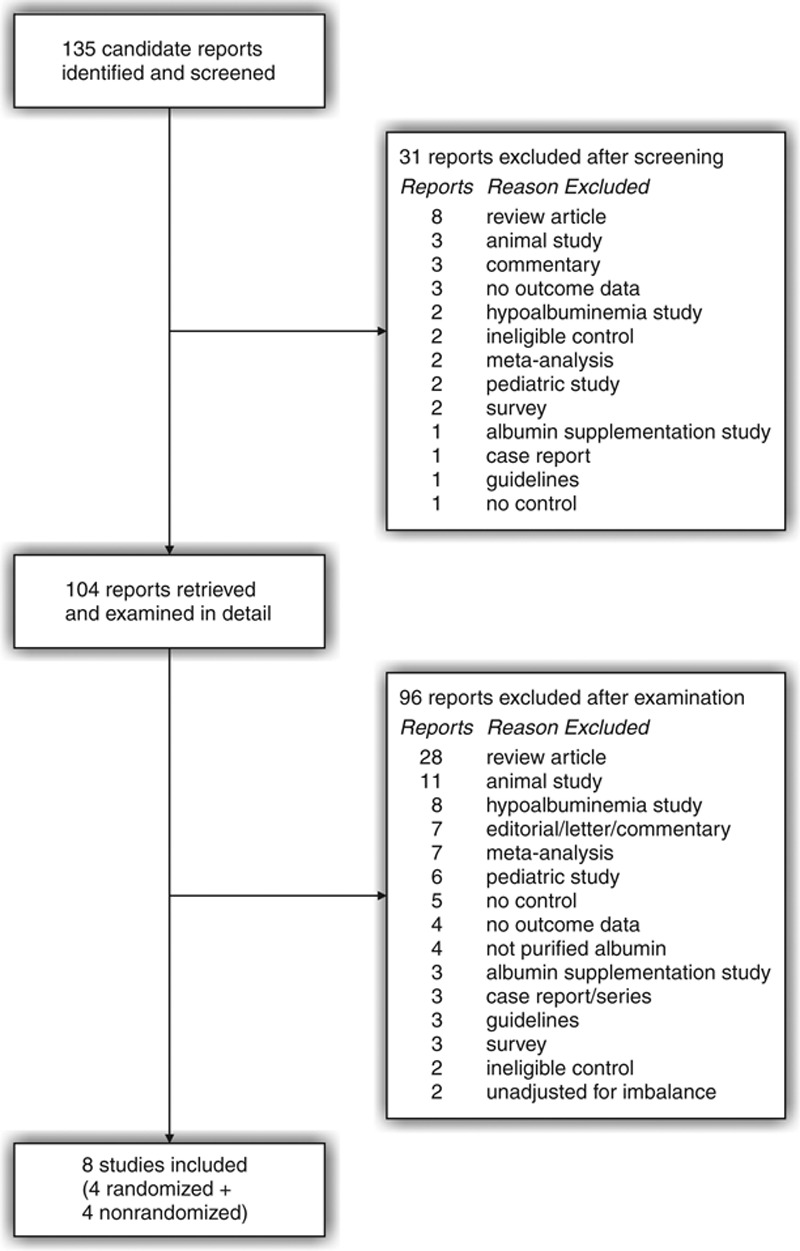
Study selection process.
The remaining eight studies, four randomized, and four nonrandomized, with a total of 688 patients were included.33–40 One randomized study involved both pediatric and adult patients,33 and only the data pertaining to the adults were extracted and analyzed. Another randomized study evaluated an echocardiographic protocol in 29 patients and a lung water protocol in 50 patients.35 Outcomes were reported exclusively for the lung water protocol, and only the data for those 50 patients were included in the meta-analysis.
Most of the studies were conducted in the United States (Table 1). The control fluid was lactated Ringer’s in all but one study.
Table 1.
Study characteristics
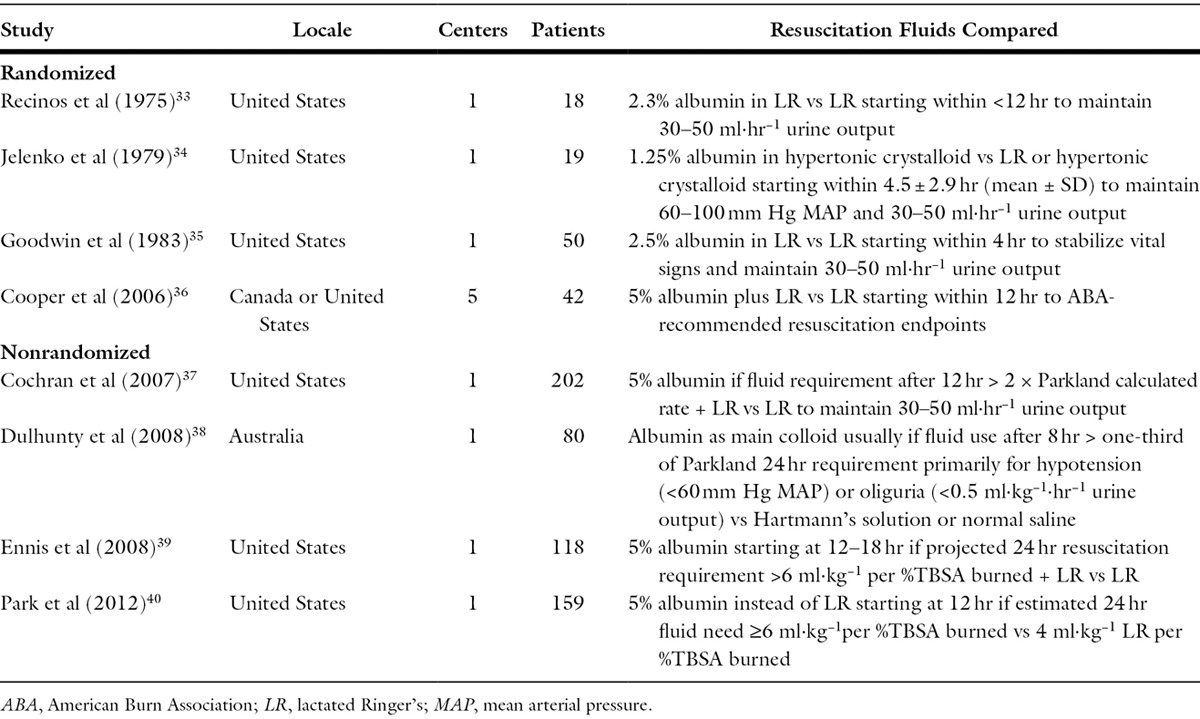
Fluid protocols differed according to study design. In the randomized studies, test fluids were administered early to every patient, in all cases within the first 12 hours. Among the nonrandomized studies, by contrast, albumin was commenced only after 8 to 12 hours as rescue therapy for the difficult cases with observed excessive fluid requirements.
Randomized Study Quality
The quality of the randomized studies was generally poor. These were small, mostly old studies with a high risk of bias. The total numbers of patient in these four studies ranged from 18 to 50 (Table 1). Three of the four were published more than 30 years ago. Only one was conducted at more than one center.36
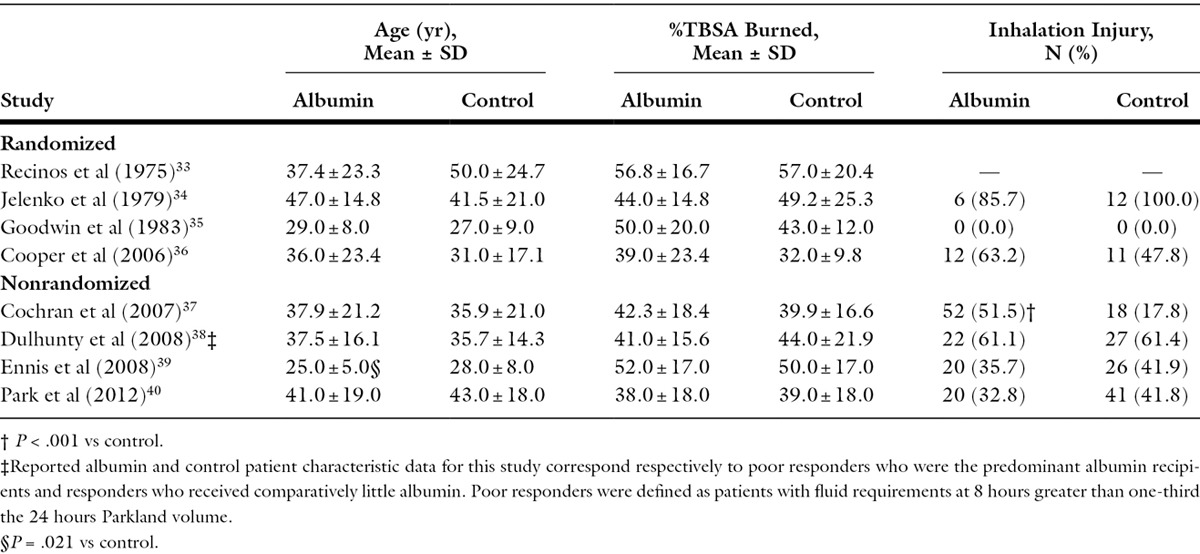
Small size rendered these studies more vulnerable to chance imbalances in baseline risk of poor outcome, despite randomization. In the one multicenter study,36 mean %TBSA burned and proportion of patients with inhalation injury were both higher in the albumin group (Table 2). While neither difference, taken singly, reached statistical significance, predicted mortality at baseline accounting for both %TBSA burned and inhalation injury41 was significantly higher in the albumin group (P = .011). No statistical adjustment was applied for this imbalance. In another study,35 mean %TBSA burned was 16.3% higher in the albumin than control group (Table 2); however, that difference was not statistically significant (P = .14).
Table 2.
Patient characteristics
In one each of the four included randomized studies, patients were assigned to treatment group by computer-generated randomization list,36 random number table,35 hospital number33, and an unspecified method.34 Allocation concealment was accomplished through the use of sequentially numbered sealed opaque envelopes in the multicenter study.36 Measures taken to ensure allocation concealment were unspecified for the remaining studies. The multicenter study was unblinded. The use of blinding, if any, was unspecified for the other studies.
Nonrandomized Study Quality
Published from 2007 to 2012, the four nonrandomized studies accounted for 81.2% of the total patients in the meta-analysis (Table 1). Thus, these studies were more recent and far larger than their randomized counterparts. They were, however, limited at least in part by retrospective design. Two were retrospective case–control studies.37,38 The other two compared patients before vs after the institution of a new fluid protocol calling for the use of 5% albumin in difficult-to-resuscitate patients.39,40 In one of those two, data were prospectively collected for consecutive patients after the switch to the new protocol.39 Otherwise the prospective vs retrospective design of the two before–after studies was unspecified.
Both retrospective case–control studies exhibited significant baseline risk imbalances. In one,37 inhalation injury was 2.9-fold more frequent in the albumin group (Table 2). In the other,38 baseline APACHE II score was higher in the albumin group. In both studies, results were adjusted for baseline imbalance using multivariate logistic regression. The groups differed slightly but significantly by age in one before–after study (Table 2).39
Mortality
Data on mortality were available for all four randomized studies and three of the four nonrandomized studies (Figure 2). Twenty-nine deaths occurred in the randomized studies and 90 in the nonrandomized studies. In one retrospective case–control study with nearly three times the frequency of inhalation injury among albumin as control patients,37 crude mortality was higher among albumin recipients. However, multivariate adjustment indicated a significant decrease in the odds of death associated with albumin administration for that study.
Figure 2.
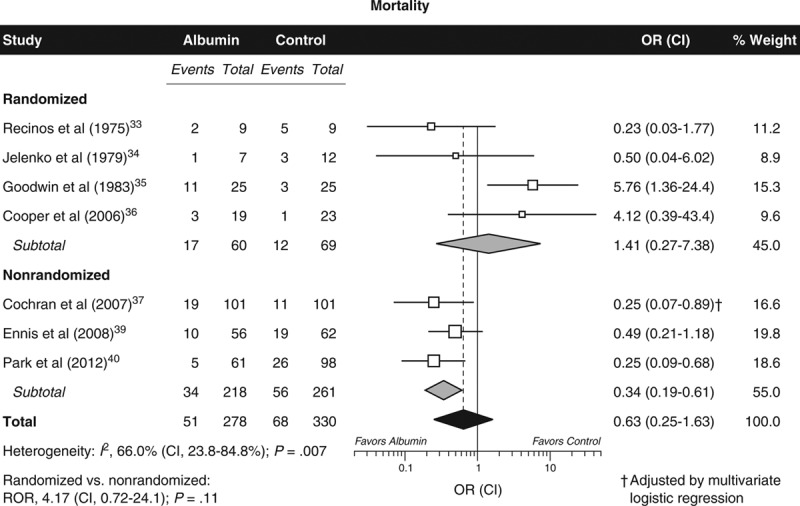
Mortality after burn shock resuscitation with albumin infusion. Data points for individual studies scaled in proportion to meta-analytic weight. Error bars depict CI. CI, 95% confidence interval; OR, odds ratio; ROR, ratio of odds ratios.
The pooled OR showed lower odds of death among albumin recipients across all seven studies (Figure 2), although the difference was not statistically significant. No publication bias could be detected (P = .47). There was, however, substantial and significant heterogeneity (Figure 2). The heterogeneity could not be attributed to study design per se, since the OR for mortality did not differ significantly between the randomized and nonrandomized studies (P = .11). Rather, the heterogeneity was confined exclusively to the randomized studies (I2, 62.0%; CI, 0.0–87.2%; P = .048) and was absent from the nonrandomized studies (I2, 0.0%; CI, 0.0–83.9%; P = 0.52).
One potential explanation for the heterogeneity was the above discussed evidence of unadjusted excess baseline risk among albumin recipients in two randomized studies.35,36 In both studies, the mortality of the albumin group was markedly elevated (OR, 4.12 and 5.76); whereas, in all five of the other studies mortality was lower in the albumin group, and quantitatively the OR for mortality fell within the narrow range of 0.23 to 0.50. In a sensitivity analysis, exclusion of the two imbalanced studies abolished overall heterogeneity (I2, 0.0%; CI, 0.0–45.5%; P = .82). Furthermore, in that sensitivity analysis encompassing two randomized and three nonrandomized studies, albumin administration was associated with significantly reduced mortality (pooled OR, 0.34; 0.19–0.58; P < .001).
Morbidity
The most frequently reported forms of morbidity were compartment syndrome of the abdomen or extremities (Figure 3), respiratory complications (Figure 4), and renal dysfunction (Figure 5). Thirty-eight total cases of compartment syndrome were reported among two randomized and three nonrandomized studies. The albumin group experienced a marked relative decrease of 81% in the odds of compartment syndrome (pooled OR, 0.19; P < .001). The magnitude of the effect did not differ between the randomized and nonrandomized studies (P = .71), and there was no evidence of heterogeneity (P = .29) or publication bias (P = .28).
Figure 3.
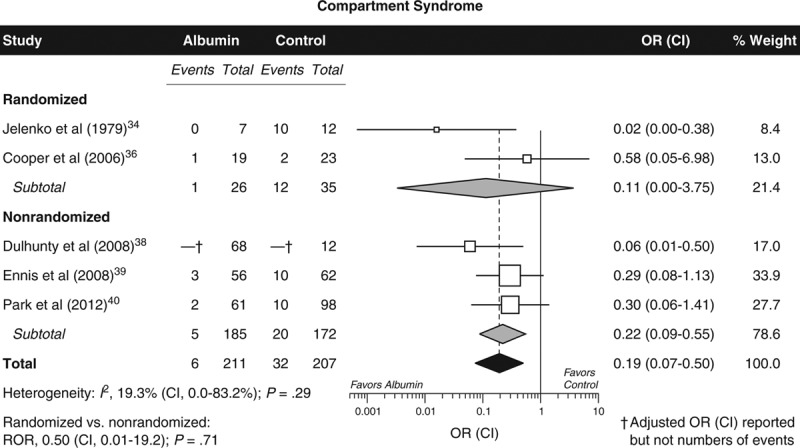
Compartment syndrome of the abdomen or extremities after burn shock resuscitation with albumin infusion. Graphic conventions as in Figure 2. CI, 95% confidence interval; OR, odds ratio; ROR, ratio of odds ratios.
Figure 4.

Respiratory complications after burn shock resuscitation with albumin infusion. Graphic conventions as in Figure 2. CI, 95% confidence interval; OR, odds ratio; ROR, ratio of odds ratios.
Figure 5.
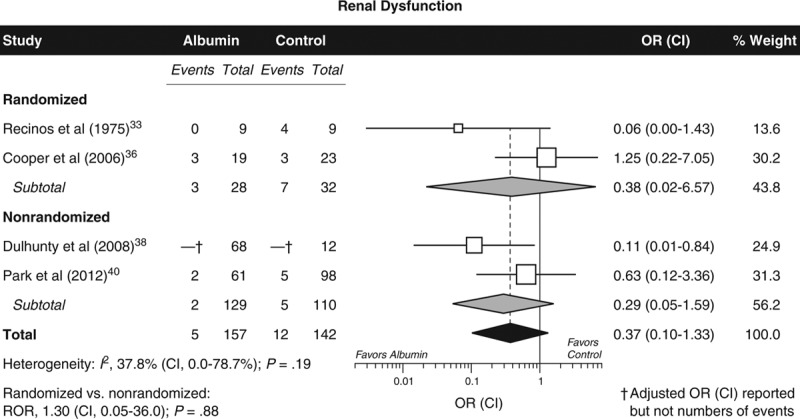
Renal dysfunction after burn shock resuscitation with albumin infusion. Graphic conventions as in Figure 2. CI, 95% confidence interval; OR, odds ratio; ROR, ratio of odds ratios.
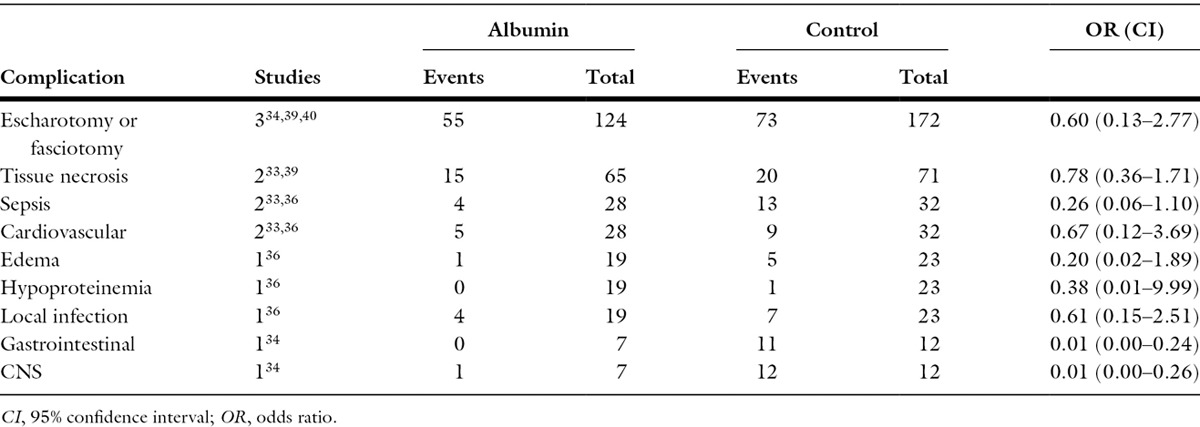
Albumin infusion was accompanied by reduced odds of respiratory complications, renal dysfunction, need for escharotomy or fasciotomy, tissue necrosis, sepsis, cardiovascular complications, edema, hypoproteinemia, local infection, and gastrointestinal and central nervous system complications (Figures 4 and 5; Table 3). In most instances, these differences were nevertheless not statistically significant. Only gastrointestinal and central nervous system complications, reported in a single randomized study, were significantly reduced by albumin.
Table 3.
Less frequently reported complications
DISCUSSION
This is the first meta-analysis focused solely on the effects of albumin for burn shock resuscitation, the first to investigate morbidity in addition to mortality, the first to include data from nonrandomized as well as randomized controlled studies, and the first to address potential biases. Among all included studies, albumin infusion was commenced within the first 24 hours after burn injury. The meta-analysis suggests that, based on the totality of currently available evidence, acute burn shock resuscitation with albumin may reduce mortality and compartment syndrome.
At the same time, the meta-analysis indicated important weaknesses in the existing evidence. The quality of available randomized studies is poor, and retrospective design is a limitation of some available nonrandomized studies. The numbers of patients with available data for other types of complications were far smaller than for compartment syndrome, and hence the meta-analysis may have been underpowered to detect additional effects on morbidity. It is noteworthy that the odds of all 11 types of complications evaluated besides compartment syndrome (Figures 4 and 5; Table 3) were lower in the albumin group, although the difference was only significant for two complication types based on data from a single study. All these weaknesses highlight the need for additional trials, a need that has previously been recognized.7,42
Among all seven studies with data no overall effect of albumin on mortality could be detected. That result needs to be interpreted with caution because of the presence of marked heterogeneity. On investigation that heterogeneity could be ascribed to disproportionate baseline risk in the albumin group of two randomized studies. Heterogeneity could be eliminated by excluding those two studies, with the result that albumin infusion was associated with a significant 64% relative decrease in the odds of death (OR, 0.34).
Baseline risk imbalances were also evident in two of the nonrandomized studies; however, the investigators used multivariate statistical analysis to adjust for imbalance. In one retrospective case–control study,37 the largest study of the meta-analysis, there was nearly three times the frequency of inhalation injury among albumin as control patients, and crude mortality was higher among albumin recipients. Inhalation injury is an important risk factor for mortality in burned patients.41,43,44 Adjustment for the imbalance revealed a 75% relative decrease in mortality odds for that study (OR, 0.25).
More than 80% of all patients were derived from the included nonrandomized studies, and so the meta-analysis borrowed major strength from those studies. Thus, there was a clear advantage to including nonrandomized studies. This advantage was not gained at the cost of heterogeneity, inasmuch as there was in no case any significant effect size difference between the randomized and nonrandomized studies (Figures 2–5). This finding is consistent with numerous large-scale empirical studies demonstrating agreement between randomized and nonrandomized studies.45–48
Mortality from burn injuries is now at historically low levels,8 and thus more attention is being focused on associated morbidity. The recent renewed interest in the use of albumin has been driven by the desire to reduce morbidity related to the large quantities of resuscitation fluid administered to burn patients in the first 24 hours. Aggressive fluid therapy can escalate the massive edema in both burned and nonburned tissue occurring after burn injury.49 Edema leads to tissue hypoxia and increased tissue pressure. Increased interstitial pressure in burned soft tissue compartments often necessitates escharotomy or even fasciotomy.49 ACS is an extreme example of massive edema, which can be life-threatening.50,51 Compartment syndrome can also occur in unburned limbs, requiring fasciotomies. In all five studies with data on either abdominal or extremity compartment syndrome, albumin use was consistently associated with a marked decrease in this complication. The overall pooled results showed an 81% relative odds decrease for compartment syndrome in the albumin group patients. This observation is in accord with a randomized trial of 31 severely burned patients comparing FFP and lactated Ringer’s as the resuscitation fluids.52 There was a significantly greater increase in intraabdominal pressure among patients assigned to the crystalloid protocol, and all but one patient of 15 in that group exceeded the 25-mm Hg pressure threshold associated with complications. By contrast, 14 of the 16 patients in the FFP group did not exceed the threshold.
A 1998 Cochrane meta-analysis exclusively of randomized trials suggested increased mortality attributable to albumin among critically injured patients, including those with burns.53 That meta-analysis was widely criticized by burn specialists54–57 and could not be reproduced, either with respect to critically injured patients generally or burn patients specifically, in a far larger subsequent meta-analysis.58 Importantly, no excess mortality related to albumin has been found in three subsequent large-scale randomized trials of critically injured patients.59–61
The explanation for the disparity was shown to be that the Cochrane meta-analysis was limited to a small, biased subset of eligible randomized trials.62 With regard to burns in particular, the latest 2011 update of the Cochrane meta-analysis includes four randomized studies with 205 total patients undergoing burn shock resuscitation or postburn albumin supplementation and continues to suggest an almost 3-fold increase in the odds of death among patients receiving albumin.63 However, the Cochrane investigators neglected to include two trials satisfying their eligibility criteria and showing either reduced mortality among albumin recipients33 or no effect.64 With inclusion of the two omitted trials a significant effect on mortality can no longer be demonstrated. Furthermore, no attempt was made in that meta-analysis to deal with the baseline risk imbalances favoring the control group in two of the included studies.35,36
In a recent Brazilian study of a hospital information system database, albumin was administered to 4% of 39,684 patients with moderate or major burns.65 Although an association between albumin usage and increased mortality was claimed, no assessment was reported on the comparative baseline %TBSA burned or frequency of inhalation injury between albumin recipients and nonrecipients. In large intensive care unit studies, albumin was reserved for the most severely injured patients,66,67 and the Brazilian study was likely subject to similar allocation bias. Accordingly, that study was excluded from the current meta-analysis.
A major issue regarding burn shock resuscitation with colloids is whether because of the early transient increase in capillary permeability their use could contribute to edema formation. In a comprehensive review of the burn edema process, Demling concluded that in virtually all experimental studies, using both protein and nonprotein colloids, there was a decrease in nonburned skin edema and no increase in burn wound edema.49 Increased vascular permeability appears to be only a phenomenon of the first few hours after a burn injury.68 Beginning about 8 to 12 hours postburn, decreased plasma oncotic pressure resulting from depleted plasma protein levels contributes to fluid movement into the tissues.
In the included nonrandomized studies, albumin was administered as rescue therapy for the most difficult-to-resuscitate patients, starting from 8 to 12 hours after the burn injury. Albumin use was begun even earlier in the included randomized studies. According to the most recent recommendations of the American Burn Association, one option is to administer colloid-containing fluids between 12 and 24 hours postinjury to decrease overall fluid requirements during acute burn shock resuscitation.69
Transient increase in vascular permeability during the first hours after thermal injury may provide a mechanistic basis for favoring a delay before albumin infusion until 8 to 12 hours.68 Nevertheless, that approach, as exemplified by the included nonrandomized studies, was not associated in this meta-analysis with superior outcomes as compared with the included randomized studies in which albumin administration was commenced earlier. The meta-analysis may have been underpowered to detect such a difference, and additional data would be needed to resolve this question.
Use of albumin in burned patients was first described more than 70 years ago among combat casualties of Pearl Harbor.70 Yet, despite clinical use in burns for decades, the optimal timing, dose, and patient population for albumin use remain unclear. As demonstrated in this meta-analysis, the current available evidence suggests that albumin can improve outcomes of burn shock resuscitation. However, the scope and quality of current evidence are limited, and new adequately powered, preferably multicenter clinical trials should be conducted.
ACKNOWLEDGMENTS
All authors contributed to the conception and design of the study and to revision of the article critically for important intellectual content and gave final approval of the version to be submitted. Additionally, Roberta J. Navickis and Mahlon M. Wilkes contributed to the acquisition, analysis and interpretation of data, and drafting of the article.
The funding source played no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Footnotes
This investigation was supported under an unrestricted research grant from CSL Behring, King of Prussia, Pennsylvania. Drs. Navickis and Wilkes have received past unrestricted research grant funding from Baxter, CSL Behring and Grifols. Dr. Greenhalgh has no possible conflicts of interest to disclose.
REFERENCES
- 1.Cope O, Moore FD. The redistribution of body water and the fluid therapy of the burned patient. Ann Surg. 1947;126:1010–45. doi: 10.1097/00000658-194712000-00013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Evans EI, Purnell OJ, Robinett PW, Batchelor A, Martin M. Fluid and electrolyte requirements in severe burns. Ann Surg. 1952;135:804–17. doi: 10.1097/00000658-195206000-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Janeway CA, Gibson ST, Woodruff LM, Heyl JT, Bailey OT, Newhouser LR. Chemical, clinical, and immunological studies on the products of human plasma fractionation. VII. Concentrated human serum albumin. J Clin Invest. 1944;23:465–90. doi: 10.1172/JCI101514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Reiss E, Stirmann JA, Artz CP, Davis JH, Amspacher WH. Fluid and electrolyte balance in burns. J Am Med Assoc. 1953;152:1309–13. doi: 10.1001/jama.1953.03690140017004. [DOI] [PubMed] [Google Scholar]
- 5.Food and Drug Administration. Guidance for industry: revised preventive measures to reduce the possible risk of transmission of Creutzfeldt-Jakob disease and variant Creutzfeldt-Jakob disease by blood and blood products. 2012. available from http://www.fda.gov/downloads/biologicsbloodvaccines/guidancecomplianceregulatoryinformation/guidances/blood/ucm307137.pdf; accessed 03 Aug. 2014. [Google Scholar]
- 6.Moyer CA, Margraf HW, Monafo WW., Jr Burn shock and extravascular sodium deficiency—treatment with Ringer’s solution with lactate. Arch Surg. 1965;90:799–811. doi: 10.1001/archsurg.1965.01320120001001. [DOI] [PubMed] [Google Scholar]
- 7.Greenhalgh DG. Burn resuscitation. J Burn Care Res. 2007;28:555–65. doi: 10.1097/bcr.0b013e318093df01. [DOI] [PubMed] [Google Scholar]
- 8.Saffle JI. The phenomenon of “fluid creep” in acute burn resuscitation. J Burn Care Res. 2007;28:382–95. doi: 10.1097/BCR.0B013E318053D3A1. [DOI] [PubMed] [Google Scholar]
- 9.Pruitt BA., Jr Protection from excessive resuscitation: “pushing the pendulum back”. J Trauma. 2000;49:567–8. doi: 10.1097/00005373-200009000-00030. [DOI] [PubMed] [Google Scholar]
- 10.Engrav LH, Colescott PL, Kemalyan N, et al. A biopsy of the use of the Baxter formula to resuscitate burns or do we do it like Charlie did it? J Burn Care Rehabil. 2000;21:91–5. doi: 10.1097/00004630-200021020-00002. [DOI] [PubMed] [Google Scholar]
- 11.Ivy ME, Atweh NA, Palmer J, Possenti PP, Pineau M, D’Aiuto M. Intra-abdominal hypertension and abdominal compartment syndrome in burn patients. J Trauma. 2000;49:387–91. doi: 10.1097/00005373-200009000-00001. [DOI] [PubMed] [Google Scholar]
- 12.Cartotto RC, Innes M, Musgrave MA, Gomez M, Cooper AB. How well does the Parkland formula estimate actual fluid resuscitation volumes? J Burn Care Rehabil. 2002;23:258–65. doi: 10.1097/00004630-200207000-00006. [DOI] [PubMed] [Google Scholar]
- 13.Cancio LC, Chávez S, Alvarado-Ortega M, et al. Predicting increased fluid requirements during the resuscitation of thermally injured patients. J Trauma. 2004;56:404–13; discussion 413–4. doi: 10.1097/01.TA.0000075341.43956.E4. [DOI] [PubMed] [Google Scholar]
- 14.Friedrich JB, Sullivan SR, Engrav LH, et al. Is supra-Baxter resuscitation in burn patients a new phenomenon? Burns. 2004;30:464–6. doi: 10.1016/j.burns.2004.01.021. [DOI] [PubMed] [Google Scholar]
- 15.Mitra B, Fitzgerald M, Cameron P, Cleland H. Fluid resuscitation in major burns. ANZ J Surg. 2006;76:35–8. doi: 10.1111/j.1445-2197.2006.03641.x. [DOI] [PubMed] [Google Scholar]
- 16.Blumetti J, Hunt JL, Arnoldo BD, Parks JK, Purdue GF. The Parkland formula under fire: is the criticism justified? J Burn Care Res. 2008;29:180–6. doi: 10.1097/BCR.0b013e31815f5a62. [DOI] [PubMed] [Google Scholar]
- 17.Cartotto R, Zhou A. Fluid creep: the pendulum hasn’t swung back yet! J Burn Care Res. 2010;31:551–8. doi: 10.1097/BCR.0b013e3181e4d732. [DOI] [PubMed] [Google Scholar]
- 18.Klein MB, Hayden D, Elson C, et al. The association between fluid administration and outcome following major burn: a multicenter study. Ann Surg. 2007;245:622–8. doi: 10.1097/01.sla.0000252572.50684.49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Greenhalgh DG, Warden GD. The importance of intra-abdominal pressure measurements in burned children. J Trauma. 1994;36:685–90. doi: 10.1097/00005373-199405000-00015. [DOI] [PubMed] [Google Scholar]
- 20.Ivy ME, Possenti PP, Kepros J, et al. Abdominal compartment syndrome in patients with burns. J Burn Care Rehabil. 1999;20:351–3. doi: 10.1097/00004630-199909000-00003. [DOI] [PubMed] [Google Scholar]
- 21.Oda J, Yamashita K, Inoue T, et al. Resuscitation fluid volume and abdominal compartment syndrome in patients with major burns. Burns. 2006;32:151–4. doi: 10.1016/j.burns.2005.08.011. [DOI] [PubMed] [Google Scholar]
- 22.Strang SG, Van Lieshout EM, Breederveld RS, Van Waes OJ. A systematic review on intra-abdominal pressure in severely burned patients. Burns. 2014;40:9–16. doi: 10.1016/j.burns.2013.07.001. [DOI] [PubMed] [Google Scholar]
- 23.Markell KW, Renz EM, White CE, et al. Abdominal complications after severe burns. J Am Coll Surg. 2009;208:940–7; discussion 947–9. doi: 10.1016/j.jamcollsurg.2008.12.023. [DOI] [PubMed] [Google Scholar]
- 24.Greenhalgh DG. Burn resuscitation: the results of the ISBI/ABA survey. Burns. 2010;36:176–82. doi: 10.1016/j.burns.2009.09.004. [DOI] [PubMed] [Google Scholar]
- 25.Greenhalgh DG, Housinger TA, Kagan RJ, et al. Maintenance of serum albumin levels in pediatric burn patients: a prospective, randomized trial. J Trauma. 1995;39:67–73; discussion 73–4. doi: 10.1097/00005373-199507000-00009. [DOI] [PubMed] [Google Scholar]
- 26.Kaizar EE. Estimating treatment effect via simple cross design synthesis. Stat Med. 2011;30:2986–3009. doi: 10.1002/sim.4339. [DOI] [PubMed] [Google Scholar]
- 27.Shrier I, Boivin JF, Steele RJ, et al. Should meta-analyses of interventions include observational studies in addition to randomized controlled trials? A critical examination of underlying principles. Am J Epidemiol. 2007;166:1203–9. doi: 10.1093/aje/kwm189. [DOI] [PubMed] [Google Scholar]
- 28.DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–88. doi: 10.1016/0197-2456(86)90046-2. [DOI] [PubMed] [Google Scholar]
- 29.Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21:1539–58. doi: 10.1002/sim.1186. [DOI] [PubMed] [Google Scholar]
- 30.Altman DG, Bland JM. Interaction revisited: the difference between two estimates. BMJ. 2003;326:219. doi: 10.1136/bmj.326.7382.219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34. doi: 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Jüni P, Altman DG, Egger M. Systematic reviews in health care: Assessing the quality of controlled clinical trials. BMJ. 2001;323:42–6. doi: 10.1136/bmj.323.7303.42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Recinos PR, Hartford CA, Ziffren SE. Fluid resuscitation of burn patients comparing a crystalloid with a colloid containing solution: a prospective study. J Iowa Med Soc. 1975;65:426–32. [PubMed] [Google Scholar]
- 34.Jelenko C, 3rd, Williams JB, Wheeler ML, et al. Studies in shock and resuscitation, I: use of a hypertonic, albumin-containing, fluid demand regimen (HALFD) in resuscitation. Crit Care Med. 1979;7:157–67. [PubMed] [Google Scholar]
- 35.Goodwin CW, Dorethy J, Lam V, Pruitt BA., Jr Randomized trial of efficacy of crystalloid and colloid resuscitation on hemodynamic response and lung water following thermal injury. Ann Surg. 1983;197:520–31. doi: 10.1097/00000658-198305000-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Cooper AB, Cohn SM, Zhang HS, Hanna K, Stewart TE, Slutsky AS ALBUR Investigators. Five percent albumin for adult burn shock resuscitation: lack of effect on daily multiple organ dysfunction score. Transfusion. 2006;46:80–9. doi: 10.1111/j.1537-2995.2005.00667.x. [DOI] [PubMed] [Google Scholar]
- 37.Cochran A, Morris SE, Edelman LS, Saffle JR. Burn patient characteristics and outcomes following resuscitation with albumin. Burns. 2007;33:25–30. doi: 10.1016/j.burns.2006.10.005. [DOI] [PubMed] [Google Scholar]
- 38.Dulhunty JM, Boots RJ, Rudd MJ, Muller MJ, Lipman J. Increased fluid resuscitation can lead to adverse outcomes in major-burn injured patients, but low mortality is achievable. Burns. 2008;34:1090–7. doi: 10.1016/j.burns.2008.01.011. [DOI] [PubMed] [Google Scholar]
- 39.Ennis JL, Chung KK, Renz EM, et al. Joint Theater Trauma System implementation of burn resuscitation guidelines improves outcomes in severely burned military casualties. J Trauma. 2008;64(2 Suppl):S146–51; discussion S151–2. doi: 10.1097/TA.0b013e318160b44c. [DOI] [PubMed] [Google Scholar]
- 40.Park SH, Hemmila MR, Wahl WL. Early albumin use improves mortality in difficult to resuscitate burn patients. J Trauma Acute Care Surg. 2012;73:1294–7. doi: 10.1097/TA.0b013e31827019b1. [DOI] [PubMed] [Google Scholar]
- 41.Ryan CM, Schoenfeld DA, Thorpe WP, Sheridan RL, Cassem EH, Tompkins RG. Objective estimates of the probability of death from burn injuries. N Engl J Med. 1998;338:362–6. doi: 10.1056/NEJM199802053380604. [DOI] [PubMed] [Google Scholar]
- 42.Cartotto R, Callum J. A review of the use of human albumin in burn patients. J Burn Care Res. 2012;33:702–17. doi: 10.1097/BCR.0b013e31825b1cf6. [DOI] [PubMed] [Google Scholar]
- 43.Shirani KZ, Pruitt BA, Jr, Mason AD., Jr The influence of inhalation injury and pneumonia on burn mortality. Ann Surg. 1987;205:82–7. doi: 10.1097/00000658-198701000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Smith DL, Cairns BA, Ramadan F, et al. Effect of inhalation injury, burn size, and age on mortality: a study of 1447 consecutive burn patients. J Trauma. 1994;37:655–9. doi: 10.1097/00005373-199410000-00021. [DOI] [PubMed] [Google Scholar]
- 45.Benson K, Hartz AJ. A comparison of observational studies and randomized, controlled trials. N Engl J Med. 2000;342:1878–86. doi: 10.1056/NEJM200006223422506. [DOI] [PubMed] [Google Scholar]
- 46.Concato J, Shah N, Horwitz RI. Randomized, controlled trials, observational studies, and the hierarchy of research designs. N Engl J Med. 2000;342:1887–92. doi: 10.1056/NEJM200006223422507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Ioannidis JP, Haidich AB, Pappa M, et al. Comparison of evidence of treatment effects in randomized and nonrandomized studies. JAMA. 2001;286:821–30. doi: 10.1001/jama.286.7.821. [DOI] [PubMed] [Google Scholar]
- 48.Wilkes MM, Navickis RJ, Chan WW, Lewiecki EM. Bisphosphonates and osteoporotic fractures: a cross-design synthesis of results among compliant/persistent postmenopausal women in clinical practice versus randomized controlled trials. Osteoporos Int. 2010;21:679–88. doi: 10.1007/s00198-009-0991-1. [DOI] [PubMed] [Google Scholar]
- 49.Demling RH. The burn edema process: current concepts. J Burn Care Rehabil. 2005;26:207–27. [PubMed] [Google Scholar]
- 50.Blinderman C, Lapid O, Shaked G. Abdominal compartment syndrome in a burn patient. Isr Med Assoc J. 2002;4:833–4. [PubMed] [Google Scholar]
- 51.Cheatham ML. Abdominal compartment syndrome: pathophysiology and definitions. Scand J Trauma Resusc Emerg Med. 2009;17:10. doi: 10.1186/1757-7241-17-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.O’Mara MS, Slater H, Goldfarb IW, Caushaj PF. A prospective, randomized evaluation of intra-abdominal pressures with crystalloid and colloid resuscitation in burn patients. J Trauma. 2005;58:1011–8. doi: 10.1097/01.ta.0000162732.39083.15. [DOI] [PubMed] [Google Scholar]
- 53.Cochrane Injuries Group Albumin Reviewers. Human albumin administration in critically ill patients: systematic review of randomised controlled trials. BMJ. 1998;317:235–40. doi: 10.1136/bmj.317.7153.235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Frame JD, Moiemem N. Human albumin administration in critically ill patients. Statisticians not trained in burns care should not evaluate data. BMJ. 1998;317:884–5. [PubMed] [Google Scholar]
- 55.Cole RP. The UK albumin debate. Burns. 1999;25:565–8. doi: 10.1016/s0305-4179(99)00119-9. [DOI] [PubMed] [Google Scholar]
- 56.Fogarty BJ, Khan K. More on albumin. Multicentre randomised controlled trail is needed before changing resuscitation formulas for major burns. BMJ. 1999;318:1215. [PubMed] [Google Scholar]
- 57.Judkins K. Burns resuscitation: what place albumin? Hosp Med. 2000;61:116–9. doi: 10.12968/hosp.2000.61.2.1276. [DOI] [PubMed] [Google Scholar]
- 58.Wilkes MM, Navickis RJ. Patient survival after human albumin administration. A meta-analysis of randomized, controlled trials. Ann Intern Med. 2001;135:149–64. doi: 10.7326/0003-4819-135-3-200108070-00007. [DOI] [PubMed] [Google Scholar]
- 59.SAFE Study Investigators. A comparison of albumin and saline for fluid resuscitation in the intensive care unit. N Engl J Med. 2004;350:2247–56. doi: 10.1056/NEJMoa040232. [DOI] [PubMed] [Google Scholar]
- 60.Charpentier J, Mira J-P. Efficacy and tolerance of hyperoncotic albumin administration in septic shock patients: the EARSS study. Intensive Care Med. 2011;37(Suppl 1):S115. [Google Scholar]
- 61.Caironi P, Tognoni G, Masson S, et al. ALBIOS Study Investigators. Albumin replacement in patients with severe sepsis or septic shock. N Engl J Med. 2014;370:1412–21. doi: 10.1056/NEJMoa1305727. [DOI] [PubMed] [Google Scholar]
- 62.Wilkes MM, Navickis RJ. Does albumin infusion affect survival? Review of meta-analytic findings. In: Vincent J-L, editor. In: 2002 yearbook of intensive care and emergency medicine. Berlin: Springer-Verlag; 2002. pp. 454–64. [Google Scholar]
- 63.Roberts I, Blackhall K, Alderson P, et al. Human albumin solution for resuscitation and volume expansion in critically ill patients. Cochrane Database Syst Rev. 2011;11:CD001208. doi: 10.1002/14651858.CD001208.pub4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Mohammadi AA, Hashemi-Nasab MJ, Ershadi R, et al. Parenteral albumin therapy in burn patients: a randomized controlled trial. Iran J Med Sci. 2010;35:95–100. [Google Scholar]
- 65.Caleman G, Morais JF, Puga ME, Riera R, Atallah AN. Use of albumin as a risk factor for hospital mortality among burn patients in Brazil: non-concurrent cohort study. Sao Paulo Med J. 2010;128:289–95. doi: 10.1590/S1516-31802010000500009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Vincent JL, Sakr Y, Reinhart K, Sprung CL, Gerlach H, Ranieri VM ‘Sepsis Occurrence in Acutely Ill Patients’ Investigators. Is albumin administration in the acutely ill associated with increased mortality? Results of the SOAP study. Crit Care. 2005;9:R745–54. doi: 10.1186/cc3895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Schortgen F, Girou E, Deye N, Brochard L CRYCO Study Group. The risk associated with hyperoncotic colloids in patients with shock. Intensive Care Med. 2008;34:2157–68. doi: 10.1007/s00134-008-1225-2. [DOI] [PubMed] [Google Scholar]
- 68.Vlachou E, Gosling P, Moiemen NS. Microalbuminuria: a marker of endothelial dysfunction in thermal injury. Burns. 2006;32:1009–16. doi: 10.1016/j.burns.2006.02.019. [DOI] [PubMed] [Google Scholar]
- 69.Pham TN, Cancio LC, Gibran NS American Burn Association. American Burn Association practice guidelines burn shock resuscitation. J Burn Care Res. 2008;29:257–66. doi: 10.1097/BCR.0b013e31815f3876. [DOI] [PubMed] [Google Scholar]
- 70.Saxl NT. Burns en masse. US Navy Med Bull. 1942;40:570–6. [Google Scholar]