

Abstract
Background:
Anxiety is a common preprocedural problem and during processing especially in interventional medical processes.
Aim:
Aim of this study was to assess the level of anxiety in patients who will undergo upper gastrointestinal endoscopy and coloscopy.
Methods:
Five hundred patients scheduled to undergo sedation for elective upper gastrointestinal endoscopy and colonoscopy were studied. Beck Anxiety Inventory (BAI) was administered to each patient before brought to the endoscopy room. Demographic data of patients were collected.
Results:
BAI scores and anxiety levels were significantly lower in; males compared to females, patients with no comorbidity compared to patients with comorbidity (both P values < 0.001). BAI scores were significantly lower in patients educational status university and upper compared to patients educational status primary-high school (p=0.026). There were no significant difference between BAI and anxiety levels compared to procedures (Respectively, P=0.144 P=0.054). There were no significant difference between BAI scores and anxiety levels compared to age groups (Respectively, P=0.301 P=0.214).
Conclusions:
We think that level of anxiety in patients who will undergo upper gastrointestinal endoscopy and colonoscopy was effected by presence of comorbidities and gender but was not effected by features such as age, procedure type and educational status.
Keywords: Anxiety, sedation, upper gastrointestinal endoscopy, colonoscopy
1. INTRODUCTION
However endoscopy is the golden standard of gastrointestinal system examination and treatment of gastrointestinal system diseases, painfulness and discomfort of procedure makes the process for both appliers and the ones who was applied (1, 2). As a result, acceptance of this procedure may cause major anxiety usually. Anxiety is a common problem in patients undergoing interventional medical procedures. Because of this reason, sedo-analgesia demand on endoscopic procedures has been increased. Sedation for upper gastrointestinal endoscopy and colonoscopy not only improves patient tolerance and satisfaction but also increases the willingness of patients to return for repeated procedures (3). Despite this, gastrointestinal endoscopy and colonoscopy are still accepted as invasive procedures with the potential for discomfort, embarrassment and disappointment related to unexpected findings. These concerns can result in anxiety that unfavorably decreases patient cooperation and satisfaction with the gastroscopic or colonoscopic procedure (4). It was reported that features such as age and gender may effect the anxiety (5). Different types of anxiety scales were preferred in patients who will undergo upper gastrointestinal endoscopy and colonoscopy. (6, 7). Beck Anxiety Inventory has a widespread use in this subject. Determination, alleviation and elimination of anxiety is important for not just unwanted and discomfortable conditions, it is also important that anxiety extends, complicate the procedure and increases complications (8). For the alleviation of anxiety, many techniques such as information and music playback before the various invasive procedures has been tried (9, 10). But, it is important for the efficiency of these techniques to determinate the anxiety levels and potential risk groups for anxiety.
Aim of this study was to assess the level of anxiety in patients who will undergo upper gastrointestinal endoscopy and colonscopy, and the relationship between anxiety and individual and social features of these patients.
2. PATIENTS AND METHODS
Institutional ethics committee approval and written consent from the patients were obtained for the study. Five hundred patients between the ages of 18-80 years, ASA physical status I, II and III, scheduled to undergo sedation for elective upper gastrointestinal endoscopy and colonoscopy were studied. Patients were excluded if they were declined conscious sedation or had previously undergone sedation for elective upper gastrointestinal endoscopy and colonoscopy. Other exclusion criteria included: patient age below 18 or above 80 years, physical inability to participate, hearing problems due to any cause, any overt or borderline psychiatric illnesses, senile dementia and treatment with anxiolytic medication in the last 72 hours prior to examination. Beck Anxiety Inventory (11) was administered to each patient before brought to the endoscopy room. This is a 21-item self-report questionnaire in which the respondent is asked to rate how much each symptom has bothered him/her over the week leading up to the procedures. The symptoms are rated on a four-point scale, ranging from ‘not at all’ [0] to ‘severely’ [3]. The values for each item are summed yielding a total score ranging between 0 and 63 points. A Beck score of 0-7 represents a minimal level of anxiety, 8-15 mild, 16-25 moderate and 26-63 severe anxiety. No sedative premedication was employed before the procedure. Demographic data of patients including age, gender, comorbidities, height, weight, body mass index and educational status, were collected. The procedure was also recorded.
Statistical analyses were performed with SPSS 15.0 software. Parametric data were tested with Student’s t test and One-way ANOVA presented as median, interquartile range (IQR) and range, accordingly. Categorical data were analyzed with the two-tailed Pearson’s x2 test and are given as numbers and proportions. A P-value less than 0.05 was considered statistically significant. If Bonferroni correction used P-value less than 0.01 was considered statistically significant.
3. RESULTS
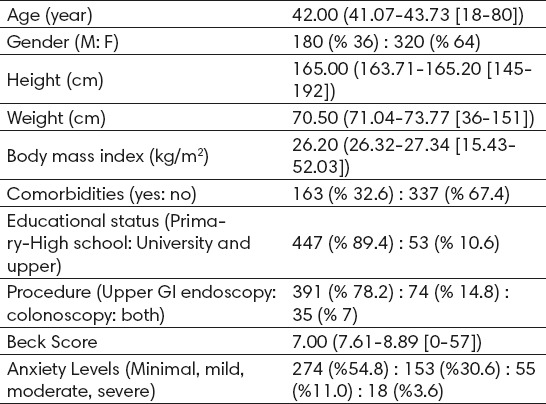
Data were collected for all 500 enrolled patients. Patients’ characteristics for 500 patients data are summarized in Table 1. Values are expressed as median (IQR [range]), number or number (proportion).
Table 1.
Patients’ characteristics for 500 patients. Values are as median (IQR [range]), number or number (proportion).
Comparison of Beck Anxiety Inventory scores and demographic data by gender are summarized in Table 2.
Table 2.
Comparison of anxiety scores and demographic data by gender. Values are as median (IQR [range]), number or number (proportion). *Minimal, mild, moderate, severe. ** Primary-High school: University and upper *** Upper GI endoscopy: colonoscopy: both
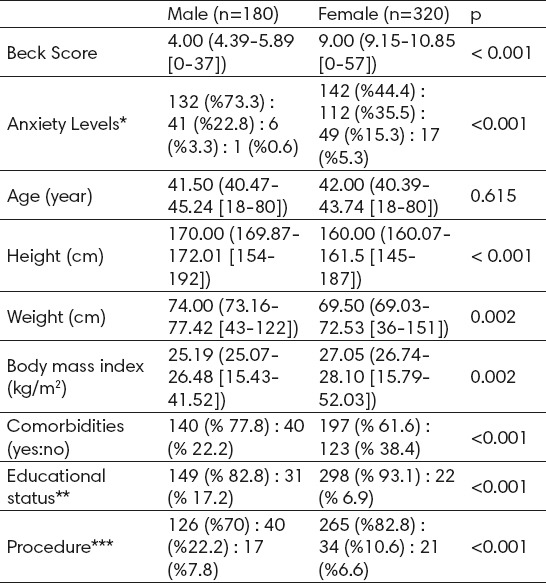
Beck Anxiety Inventory scores were significantly lower in males compared to females [Respectively, 4.00 (4.39-5.89 [0-37]), 9.00 (9.15-10.85 [0-57]) p<0.001]. Anxiety levels (minimal, mild, moderate, severe) were significantly lower in males compared to females too [Respectively, 132 (%73.3) : 41 (%22.8) : 6 (%3.3) : 1 (%0.6), 142 (%44.4) : 112 (%35.5) : 49 (%15.3) : 17 (%5.3) p<0.001]. Comparison of Beck Anxiety Inventory scores and demographic data by comorbidity are summarized in Table 3. Beck Anxiety Inventory scores were significantly lower in patients with no comorbidity compared to patients with comorbidity [Respectively, 6.00 (6.60-8.13 [0-57]), 9.00 (8.97-11.20 [0-32]) p<0.001]. Anxiety levels (minimal, mild, moderate, severe) were significantly lower in patients with no comorbidity compared to patients with comorbidity too [Respectively, 203 (%60.2) : 100 (%29.7): 23 (%6.8) : 11 (%3.3), 71 (%43.6) : 53 (%32.5) : 32 (%19.6): 7 (% 4.3) p<0.001]. Comparison of Beck Anxiety Inventory scores and demographic data by educational status are summarized in Table 4.
Table 3.
Comparison of anxiety scores and demographic data by comorbidity. Values are as median (IQR [range]), number or number (proportion). *Minimal, mild, moderate, severe. **Primary-High school: University and upper ***Upper GI endoscopy: colonoscopy: both
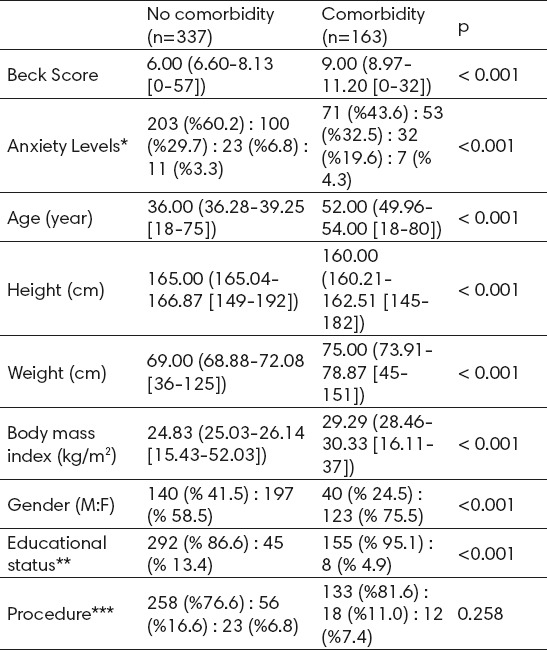
Table 4.
Comparison of anxiety scores and demographic data by educational status. Values are as median (IQR [range]), number or number (proportion). *Minimal, mild, moderate, severe. **Upper GI endoscopy: colonoscopy: both
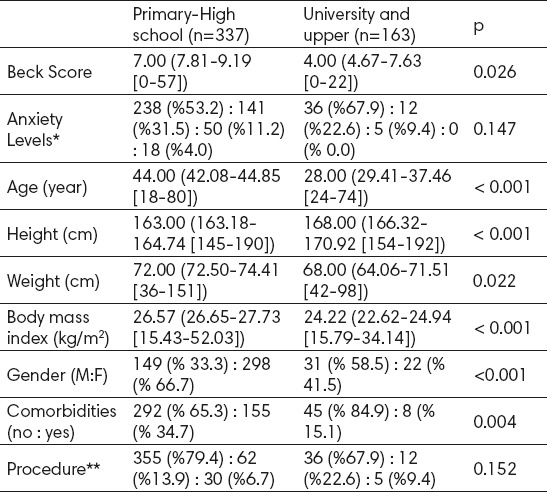
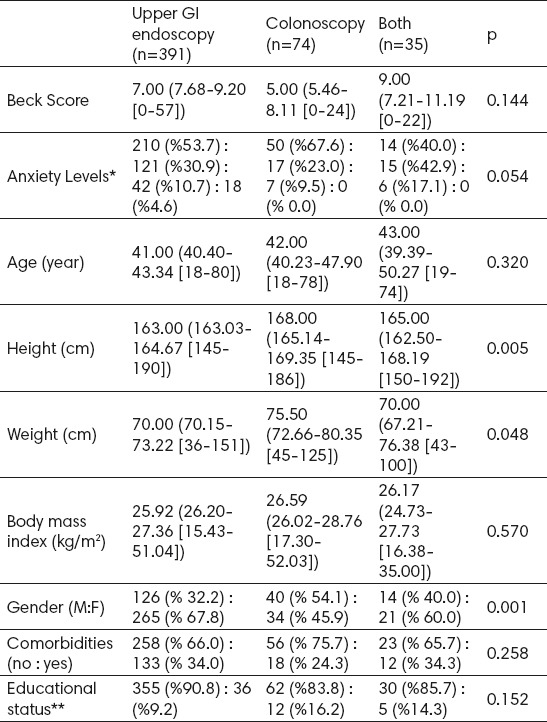
Beck Anxiety Inventory scores were significantly lower in patients educational status university and upper compared to patients educational status primary-high school [Respectively, 7.00 (7.81-9.19 [0-57]), 4.00 (4.67-7.63 [0-22]) p=0.026]. There were no significant difference between anxiety levels compared to educational status groups [Respectively, 238 (%53.2): 141 (%31.5): 50 (%11.2): 18 (%4.0), 36 (%67.9): 12 (%22.6): 5 (%9.4): 0 (% 0.0) p=147]. Comparison of Beck Anxiety Inventory scores and demographic data by procedure are summarized in Table 5. There were no significant difference between Anxiety Inventory scores compared to procedures [Respectively, 7.00 (7.68-9.20 [0-57]), 5.00 (5.46-8.11 [0-24]), 9.00 (7.21-11.19 [0-22]) p=0.144]. There were no significant difference between anxiety levels compared to procedures too [Respectively, 210 (%53.7): 121 (%30.9): 42 (%10.7): 18 (%4.6), 50 (%67.6): 17 (%23.0): 7 (%9.5): 0 (% 0.0), 14 (%40.0): 15 (%42.9): 6 (%17.1): 0 (% 0.0) p=0.054]. According to comparison of anxiety scores and demographic data by age groups there were no significant difference between Beck Anxiety Inventory scores compared to age groups [Respectively, 7.00 (7.81-9.19 [0-57]), 4.00 (4.67-7.63 [0-22]) p=0.301]. There were no significant difference between anxiety levels compared to age groups [Respectively, 139 (%58.9): 68 (%28.8): 20 (%8.5): 9 (%3.8), 135 (%51.1): 85 (%32.2): 35 (%13.3): 9 (% 3.4) p=0.214].
Table 5.
Comparison of anxiety scores and demographic data by procedure. Values are as median (IQR [range]), number or number (proportion). *Minimal, mild, moderate, severe. **Primary-High school: University and upper
4. DISCUSSION
In the present study the effect of age, gender, comorbidity, education status and procedure type to preprocedural anxiety scores who will undergo elective upper gastrointestinal endoscopy and colonoscopy under sedation, were evaluated. While gender, comorbidity and education status effect the anxiety scores, procedure type and age were presented not effected the anxiety scores. When the results of the present study were evaluated, [Minimal (%54.8), mild (%30.6), moderate (%11.0), severe (%3.6)] anxiety levels are correlated to clinical study that was performed in 135 patients who underwent colonoscopy under sedation (12).
In a study which was performed in patients who underwent gastrointestinal endoscopy under sedation, higher anxiety scores were determined in younger patients than older (13). As reason of this state it was denoted that older subjects generally had a limited understanding of the procedure and showed less anxiety about the procedure. However mean age of older patients in our study were very high than this study, in our study there were no difference between young and old patients in anxiety scores adversely to the study. We think the detailed preprocedural information given by the endoscopist is the reason of this state. In an other study about this subject in literature, it was reported that preprocedural anxiety scores were not effected by age (14). Higher preprocedural anxiety scores have been exhibited in women than in men who will undergo upper gastrointestinal endoscopy vs colonoscopy (13, 15-17). The results of our study are consistent with those results.
The results of our study exhibited higher preprocedural anxiety scores in patients who has comorbidities. In literature there is no study or data about this subject that support or suggest otherwise, but it is acceptable that comorbidity also may cause anxiety who will not undergo any procedure too.
Education status is a possible reason for preprocedural anxiety. In a study which was performed in patients who underwent upper gastrointestinal endoscopy and colonoscopy under sedation, it was reported that there were no relationship between education status and preprocedural anxiety. In our study, however Beck Anxiety Inventory scores 7.00 (7.81-9.19 [0-57]) were statistically higher in Primary - High school group, these scores were not significant in clinically. Thus it was seen these scores are clinically insignificant by anxiety levels were not different when educational status were compared.
As similar with our study results there were no difference in preprocedural anxiety determined in studies which compared preprocedural anxiety scores in different types of procedures (upper gastrointestinal endoscopy and colonoscopy) (14-16, 18). Further more, there were 3 types of procedure performed in our study (upper gastrointestinal endoscopy, colonoscopy and both), not 2 types (upper gastrointestinal endoscopy and colonoscopy). There were no statistically difference detected in preprocedural anxiety scores and levels when these 3 types are compared.
5. CONCLUSION
Although sedation demand for upper gastrointestinal endoscopy and colonoscopy increased it was seen inadequate to reduce the preprocedural anxiety levels. Further, presence of comorbidity and gender must be considered, because to determine the factors that effect preprocedural anxiety and well assessment of these factors are important. However the effect of age, educational status and procedure type on preprocedural anxiety could not shown in our study, further studies are needed because inadequacy of literature.
Footnotes
• Conflict of interest: none declared.
REFERENCES
- 1.Axon AT, Bell GD, Jones RH, Quine MA, McCloy RF. Guidelines on appropriate indications for upper gastrointestinal endoscop Working Party of the Joint Committee of the Royal College of Physicians of London, Royal College of Surgeons of England, Royal College of Anaesthetists, Association of Surgeons, the British Society of Gastroenterology, and the Thoracic Society of Great Britain. BMJ. 1995 Apr 1;310(6983):853–6. doi: 10.1136/bmj.310.6983.853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Yamada T. Endoscopy Handbook of Gastroenterology. USA: Lippincott Williams & Wilkins; 2002. pp. 667–80. [Google Scholar]
- 3.Weinman J, Johnston M. In: Topics in health psychology. Maes S, Spielberger CD, Defares P, Sarason I, editors. Chichester: John Wiley & Sons; 1988. [Google Scholar]
- 4.Rex DK, Khalfan HK. Sedation and the technical performance of colonoscopy. Gastrointestinal Endoscopy Clinics of North America. 2005;15:661–72. doi: 10.1016/j.giec.2005.08.003. [DOI] [PubMed] [Google Scholar]
- 5.Williams GL, Clarke P, Vellacott KD. Anxieties should not be forgotten when screening relatives of colorectal cancer patients by colonoscopy. Colorectal Dis. 2006;8:781–4. doi: 10.1111/j.1463-1318.2006.01092.x. [DOI] [PubMed] [Google Scholar]
- 6.Jones MP, Ebert CC, Sloan T, Spanier J, Bansal A, Howden CW, et al. Patient anxiety and elective gastrointestinal endoscopy. J Clin Gastroenterol. 2004 Jan;38(1):35–40. doi: 10.1097/00004836-200401000-00009. [DOI] [PubMed] [Google Scholar]
- 7.Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica. 1983;67:361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x. [DOI] [PubMed] [Google Scholar]
- 8.Essink-Bot ML, Kruijshaar ME, Bac DJ, Wismans PJ, ter Borg F, Steyerberg EW, et al. Different perceptions of the burden of upper GI endoscopy: an empirical study in three patient groups. Qual Life Res. 2007 Oct;16(8):1309–18. doi: 10.1007/s11136-007-9239-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Spielberger C. State-Trait Anxiety Inventory (Form Y) Palo Alto, California: Mind Garden; 1983. [Google Scholar]
- 10.Campo R, Brullet E, Montserrat A, Calvet X, Moix J, Rué M, et al. Identification of factors that influence tolerance of upper gastrointestinal endoscopy. Eur J Gastroenterol Hepatol. 1999 Feb;11(2):201–4. doi: 10.1097/00042737-199902000-00023. [DOI] [PubMed] [Google Scholar]
- 11.Rudin D. Frequently overlooked and rarely listened to: music therapy in gastrointestinal endoscopic procedures. World J Gastroenterol. 2007;13(33):4533. doi: 10.3748/wjg.v13.i33.4533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Salmore RG, Nelson JP. The effect of preprocedure teaching, relaxation instruction, and music on anxiety as measured by blood pressures in an outpatient gastrointestinal endoscopy laboratory. Gastroenterol Nurs. 2000;23:102–10. doi: 10.1097/00001610-200005000-00003. [DOI] [PubMed] [Google Scholar]
- 13.Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: psychometric properties. Journal of Consulting and Clinical Psychology. 1988;56:893–7. doi: 10.1037//0022-006x.56.6.893. [DOI] [PubMed] [Google Scholar]
- 14.Chung KC, Juang SE, Lee KC, Hu WH, Lu CC, Lu HF, et al. The effect of pre-procedure anxiety on sedative requirements for sedation during colonoscopy. Anaesthesia. 2013 Mar;68(3):253–9. doi: 10.1111/anae.12087. [DOI] [PubMed] [Google Scholar]
- 15.Lee SY, Son HJ, Lee JM, Bae MH, Kim JJ, Paik SW, et al. Identification of factors that influence conscious sedation in gastrointestinal endoscopy. J Korean Med Sci. 2004 Aug;19(4):536–40. doi: 10.3346/jkms.2004.19.4.536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.El-Hassan H, McKeown K, Muller AF. Clinical trial: music reduces anxiety levels in patients attending for endoscopy. Aliment Pharmacol Ther. 2009 Oct;30(7):718–24. doi: 10.1111/j.1365-2036.2009.04091.x. [DOI] [PubMed] [Google Scholar]
- 17.Ersöz F, Toros AB, Aydoğan G, Bektaş H, Ozcan O, Arikan S. Assessment of anxiety levels in patients during elective upper gastrointestinal endoscopy and colonoscopy. Turk J Gastroenterol. 2010 Mar;21(1):29–33. doi: 10.4318/tjg.2010.0044. [DOI] [PubMed] [Google Scholar]
- 18.Trevisani L, Sartori S, Putinati S, Gaudenzi P, Chiamenti CM, Gilli G, et al. Assessment of anxiety levels in patients during diagnostic endoscopy. Recenti Prog Med. 2002 Apr;93(4):240–4. [PubMed] [Google Scholar]
- 19.Muzzarelli L, Force M, Sebold M. Aromatherapy and reducing preprocedural anxiety: a controlled prospective study. Gastroenterol Nurs. 2006;29:466–71. doi: 10.1097/00001610-200611000-00005. [DOI] [PubMed] [Google Scholar]
- 20.Drossman DA, Brandt LJ, Sears C, Li Z, Nat J, Bozymski EM. A preliminary study of patients’concerns related to GI endoscopy. Am J Gastroenterol. 1996 Feb;91(2):287–91. [PubMed] [Google Scholar]